
Abstract
Background
Extended-spectrum β-lactamase-producing Escherichia coli has become ubiquitous and has been reported in diverse ecosystems. We evaluated the potential impact of post-acute and long-term healthcare activities on the environment by quantifying ESBL-producing Enterobacteriaceae in wastewaters of a French geriatric hospital.
Methods
We collected wastewater specimens representative of one-day efflux immediately before the connection with the municipal sewer pipe. The sample was processed following two different methods: dilution-filtration method and concentration method and was screened for ESBL-producing Enterobacteriaceae using selective media. ESBL E. coli strains were quantified, screened for ESBL genes and compared with ESBL strains isolated from patients present in the building at the time of wastewater collection, using molecular methods.
Results
Six distinct environmental ESBL E. coli clusters were identified, two of them related to patient strains. The concentrations in hospital wastewater of these strains ranged from 2.5 × 104 to 106 UFC/L.
Conclusions
Our results demonstrate that the presence of ESBL E. coli patients leads to a dissemination of ESBL E. coli in the environment and highlights the need to improve excreta and wastewater policy in hospitals.
Similar content being viewed by others


Background
The first extended-spectrum β-lactamases (ESBLs) were isolated in the 1980’s [1, 2]. Since the early 2000’s, CTX-M-type ESBLs have spread worldwide among Escherichia coli strains in hospitals and in the community [3, 4]. ESBL-producing E. coli have been reported in diverse human communities, even in remote populations [5], pets [6, 7], farm animals [8–10], lakes and river [11], wildlife [12] and soils [10]. Presence of ESBL-producing E. coli has been demonstrated in hospital wastewater [13–17] however the link between the presence of ESBL-producing E. coli in hospital wastewater and patients infected or colonized with such bacteria remains unclear. In this study, we focused on a building of our hospital and quantified ESBL-producing Enterobacteriaceae in wastewaters discharged from this building.
Methods
Hospital setting
The study was conducted at the Charles Foix hospital, a 450-bed teaching medical institution located at Ivry-sur-Seine, suburb of Paris, France. We focused the study on the building Calmette et Guérin (CG, 126 beds) which is constituted of geriatric post-acute care (PAC), long-term care (LTC) units along with a little psychiatric unit.
Wastewater collection
From December 29th 2010 9.30 am until December 30th 2010 9.30 am, wastewater samples were collected at the sewer pipe that collects wastewaters from the CG building, immediately before the connection with the municipal sewer pipe. At this collection point, 140-mL samples were collected every 15 min within 24 h using an automatic refrigerated water sampler (Teledyne Isco, Lincoln, NE, USA). These samples were mixed to constitute a specimen representative of one-day efflux. Flow, pH and temperature were continuously monitored.
Wastewater processing
The sample was processed on the same day following two methods, i.e. the dilution-filtration method and the concentration method.
In the dilution-filtration method, the sample was diluted in sterile saline solution (10-2–7) and 2 volumes of 100 mL of each diluted suspensions were filtrated on 0.45 μm nitrocellulose membranes (Merck Millipore, Billerica, MA, USA). These membranes were deposited on two distinct selective agars: chromID® ESBL agar (bioMérieux, Marcy l’Etoile, France) and Drigalski agar supplemented with cefotaxime (0.5 mg/L) and ticarcillin (250 mg/L) (Drig-TC).
In the concentration method, 20 mL of the wastewater specimen were filtrated on a 0.4 μm polycarbonate Isopore® membrane (Merck Millipore, Billerica, MA, USA) and then suspended in 5 mL sterile saline solution using a sterile cell scraper. These suspensions were then diluted in sterile saline solution (10-1–6) and 100 μL of each diluted suspension were plated on both chromID® ESBL and Drig-TC agars.
Patients
The microbiological database was screened for patients present in the building at the time of wastewater collection and whose bacteriological specimens, taken either for clinical or bacteriological (i.e. rectal swab) were positive for ESBL-producing E. coli.
Bacterial strains and susceptibility assays
Environmental, epidemiological and clinical strains were identified by API 20E® system (bioMérieux, Marcy l’Etoile, France). Susceptibility to antimicrobial agents was assessed by disk diffusion method according to French guidelines (www.sfm-microbiologie.org) and ESBL production was screened by the double disk synergy test (DDST) [18].
Beta-lactamase characterization and screening of resistance genes
Each strain displaying a positive DDST was screened for the presence of for the bla TEM, bla SHV and bla CTX-M genes, using PCR amplification and sequencing as reported before [19].
Molecular typing
Wastewater and patient ESBL-producing strains of E. coli were compared using the semi-automated typing system DiversiLab® (bioMérieux, Marcy l’Etoile, France) as described elsewhere [20] using 95 % similarity threshold to consider fingerprints as similar.
When DiversiLab fingerprints were considered as similar, the corresponding strains were further studied by Pulsed-Field Gel Electrophoresis (PFGE) as reported before [21].
Results
At collection point, the flow was 39,270 m3 per day, the temperature ranged from 12 to 17.3 °C and the pH ranged from 6.2 to 8.9.
Each distinct colony that grew on selective agar plates (chromID® ESBL and Drig-TC) inoculated with wastewater processed by dilution-filtration or concentration method was identified and screened for ESBL production. A total of 389 colonies could be individualized and were studied. Most of them were non fermentative bacteria or cephalosporinase-producing enterobacteria. Twenty-five colonies were identified as ESBL-producing Enterobacteriaceae, including 23 E. coli and two Enterobacter cloacae. The concentrations of ESBL-producing E. coli in wastewater was estimated using the number of colonies, the dilution factor and the volume filtrated. This estimated concentrations ranged between 1 × 106 UFC/L based on the characteristics of the dilution-filtration method, and 2.5 × 105 UFC/L based on the characteristics of the concentration method.
Nine patients hospitalized in the CG building at the time of wastewater collection had been identified carrying ESBL E. coli. The 23 isolates from wastewater and 9 strains isolated from 9 carriers were submitted to genotyping and identification of ESBL-encoding genes.
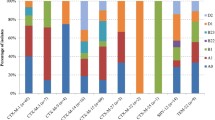
The 23 wastewater ESBL E. coli isolates belonged to 5 distinct DiversiLab® patterns: 14 to pattern 1, four to pattern 2, two to patterns 3 and 5, respectively, and one to pattern 4 (Table 1). The isolates belonging to the DiversiLab® profile 1 was subdivided into two pulsotypes 1a and 1b. PFGE 1a corresponded to isolates carrying the ESBL bla CTXM-14 and the broad-spectrum β-lactamase bla TEM-1 genes. PFGE 1b corresponded to ESBL CTX-M-27-producing isolates (Table 1). Other clusters produced CTX-M-1 or TEM-3.
Thus, a total of six distinct clusters of ESBL-producing E. coli clusters (WWCG1a to WWCG5) were identified in wastewater. The concentrations of each cluster was estimated using the number of colonies belonging to this cluster, the dilution factor and the volume filtrated. The estimated concentration ranged from 2.5 × 104 to 106 UFC/L (Table 1). Most of them (4/6) produced a CTX-M-type ESBL, the others producing TEM-3.
The genotyping results obtained for the 9 ESBL-producing E. coli strains from patients, showed that five of them were undistinguishable (Table 2). These five strains were also undistinguishable from the wastewater WWCG1b cluster defined above and carried the bla CTX-M-27 gene. These strains had been isolated from three patients hospitalized in the same post-acute care ward (PAC-Mong) (Table 2), from one patient hospitalized in the long-term care ward but who had been previously hospitalized in PAC-Mong unit at the same time as the above patients, and from one patient hospitalized in a distinct post-acute care ward (PAC-Nec) that shares nursing and medical staffs with PAC-Mong ward. One patient strain cluster belonged to DiversiLab® profile 1 and pulsotype 1a, carried bla CTXM-14 and bla TEM-1 genes and consequently was undistinguishable from wastewater cluster WWCG1a (Table 2).
The other three patients strains were distinct one from each other and also distinct from wastewater isolates.
Discussion
Enterobacteriaceae, particularly E. coli, are commensal bacteria present at about 108 colony-forming units per gram of human faeces. The faecal concentration of ESBL-producing E. coli may vary with the antibiotic treatment and it has been shown that the mean relative faecal abundance of ESBL-producing E. coli was 13-fold higher in women exposed to antimicrobials [22]. Even before ESBLs were first reported, hospitals were considered as sources of environmental pollution with multiresistant E. coli strains. Indeed, in 1973, Grabow et al. reported that the proportion of E. coli carrying multiresistant conjugative plasmids was higher (26 % vs 4 %) in hospital wastewater samples than in city sewage samples [23]. As hospital settings concentrate ESBL-producing E. coli carriers, they can be a source of environmental ESBL-type pollution.
Several studies have focused on hospital discharge of ESBL-producing Enterobacteriaceae [13–17]. However, in most cases, sewages were sampled by filling directly sterile bottles, i.e. by studying random specimens of wastewater. In our study, the sewage point was sampled using equipment allowing the collection of a specimen representative of a daily wastewater discharge, taking into account quantitative and qualitative variations of flow that can be observed within a single day.
Moreover, in most of the above studies, Enterobacteriaceae were enumerated but the presence of ESBL-producing strains was notified without the range quantification [13–16]. In our study, we estimated the concentration of ESBL-producing E. coli based on the specimen processing. Concentrations we have found are consistent with the concentration of cefotaxime-resistant E. coli strains reported by Galvin et al. in the effluents of an Irish hospital (estimation, 105 UFC/L) [15]. Most of the environmental ESBL E. coli isolates (20/23) found in our hospital wastewater produced a CTX-M-type ESBL belonging either to group 1 or to group 9 and few to TEM type. This predominance of CTX-M-type ESBLs is consistent with the relative distribution of ESBL enzymes among clinical ESBL E. coli in France [24].
Molecular typing of wastewater ESBL isolates allowed identifying and quantifying two clusters carried by patients present in the building at the time of wastewater collection.
To our knowledge, the present study is the first report of ESBL-producing E. coli quantification in sewage in direct relation with strains isolated from patients.
Conclusions
The present study demonstrates that the presence of ESBL-producing E. coli carriers in hospital may lead to a dissemination of ESBL-producing E. coli in the environment, with a quantification of ESBL-producing E. coli in sewage in direct relation with strains isolated from patients. In this matter, Healthcare settings play an important role in ESBL-producing bacteria spread, not only through cross-transmission and antibiotics consumption, but also through their wastes and should improve their disposal of human excreta in order to reduce their impact on the environment.
Abbreviations
- DDST:
-
double disk synergy test
- Drig-TC:
-
Drigalski agar supplemented with cefotaxime and ticarcillin
- ESBL:
-
extended-spectrum β-lactamase
- ESBL-E:
-
extended-spectrum β-lactamase-producing Enterobacteriaceae
- LTC:
-
long-term care
- MRSA:
-
methicillin-resistant Staphylococcus aureus
- PAC:
-
post-acute care
- PCR:
-
polymerase chain reaction
- PFGE:
-
pulsed-field gel electrophoresis
- UFC:
-
unit forming colony
- WWTP:
-
wastewater treatment plant
References
Brun-Buisson C, Legrand P, Philippon A, Montravers F, Ansquer M, Duval J. Transferable enzymatic resistance to third-generation cephalosporins during nosocomial outbreak of multiresistant Klebsiella pneumoniae. Lancet. 1987;2:302–6.
Sirot D, Sirot J, Labia R, Morand A, Courvalin P, Darfeuille-Michaud A, et al. Transferable resistance to third-generation cephalosporins in clinical isolates of Klebsiella pneumoniae: identification of CTX-1, a novel beta-lactamase. J Antimicrob Chemother. 1987;20:323–34.
Pitout JDD, Laupland KB. Extended-spectrum beta-lactamase-producing Enterobacteriaceae: an emerging public-health concern. Lancet Infect Dis. 2008;8:159–66.
Bush K, Fisher JF. Epidemiological expansion, structural studies, and clinical challenges of new β-lactamases from gram-negative bacteria. Annu Rev Microbiol. 2011;65:455–78.
Woerther PL, Angebault C, Lescat M, Ruppé E, Skurnik D, Mniai AE, et al. Emergence and dissemination of extended-spectrum beta-lactamase-producing Escherichia coli in the community: lessons from the study of a remote and controlled population. J Infect Dis. 2010;202:515–23.
Wieler LH, Ewers C, Guenther S, Walther B, Lübke-Becker A. Methicillin-resistant staphylococci (MRS) and extended-spectrum beta-lactamases (ESBL)-producing Enterobacteriaceae in companion animals: nosocomial infections as one reason for the rising prevalence of these potential zoonotic pathogens in clinical samples. Int J Med Microbiol. 2011;301:635–41.
Dahmen S, Haenni M, Châtre P, Madec J-Y. Characterization of blaCTX-M IncFII plasmids and clones of Escherichia coli from pets in France. J Antimicrob Chemother. 2013;68:2797–801.
Liebana E, Batchelor M, Hopkins KL, Clifton-Hadley FA, Teale CJ, Foster A, et al. Longitudinal farm study of extended-spectrum beta-lactamase-mediated resistance. J Clin Microbiol. 2006;44:1630–4.
Geser N, Stephan R, Hächler H. Occurrence and characteristics of extended-spectrum β-lactamase (ESBL) producing Enterobacteriaceae in food producing animals, minced meat and raw milk. BMC Vet Res. 2012;8:21.
Hartmann A, Locatelli A, Amoureux L, Depret G, Jolivet C, Gueneau E, et al. Occurrence of CTX-M Producing Escherichia coli in Soils, Cattle, and Farm Environment in France (Burgundy Region). Front Microbiol. 2012;3:83.
Zurfluh K, Hächler H, Nüesch-Inderbinen M, Stephan R. Characteristics of extended-spectrum β-lactamase- and carbapenemase-producing Enterobacteriaceae Isolates from rivers and lakes in Switzerland. Appl Environ Microbiol. 2013;79:3021–6.
Guenther S, Ewers C, Wieler LH. Extended-spectrum beta-lactamases producing E. coli in wildlife, yet another form of environmental pollution? Front Microbiol. 2011;2:246.
Prado T, Pereira WC, Silva DM, Seki LM, Carvalho APD, Asensi MD. Detection of extended-spectrum beta-lactamase-producing Klebsiella pneumoniae in effluents and sludge of a hospital sewage treatment plant. Lett Appl Microbiol. 2008;46:136–41.
Diwan V, Tamhankar AJ, Khandal RK, Sen S, Aggarwal M, Marothi Y, et al. Antibiotics and antibiotic-resistant bacteria in waters associated with a hospital in Ujjain, India. BMC Public Health. 2010;10:414.
Galvin S, Boyle F, Hickey P, Vellinga A, Morris D, Cormican M. Enumeration and characterization of antimicrobial-resistant Escherichia coli bacteria in effluent from municipal, hospital, and secondary treatment facility sources. Appl Environ Microbiol. 2010;76:4772–9.
Chagas TP, Seki LM, Cury JC, Oliveira JA, Dávila AM, Silva DM, et al. Multiresistance, beta-lactamase-encoding genes and bacterial diversity in hospital wastewater in Rio de Janeiro, Brazil. J Appl Microbiol. 2011;111:572–81.
Bréchet C, Plantin J, Sauget M, Thouverez M, Talon D, Cholley P, et al. Wastewater treatment plants release large amounts of extended-spectrum β-lactamase-producing Escherichia coli into the environment. Clin Infect Dis. 2014;58:1658–65.
Drieux L, Brossier F, Sougakoff W, Jarlier V. Phenotypic detection of extended-spectrum beta-lactamase production in Enterobacteriaceae: review and bench guide. Clin Microbiol Infect. 2008;14:90–103.
Garrec H, Drieux-Rouzet L, Golmard JL, Jarlier V, Robert J. Comparison of nine phenotypic methods for detection of extended-spectrum beta-lactamase production by Enterobacteriaceae. J Clin Microbiol. 2011;49:1048–57.
Brolund A, Haeggman S, Edquist PJ, Gezelius L, Olsson-Liljequist B, Wissel KT, et al. The DiversiLab system versus pulsed-field gel electrophoresis: characterisation of extended spectrum beta-lactamase producing Escherichia coli and Klebsiellla pneumoniae. J Microbiol Methods. 2010;83:224–30.
Drieux L, Brossier F, Duquesnoy O, Aubry A, Robert J, Sougakoff W, et al. Increase in hospital-acquired bloodstream infections caused by extended spectrum beta-lactamase-producing Escherichia coli in a large French teaching hospital. Eur J Clin Microbiol Infect Dis. 2009;28:491–8.
Ruppé E, Lixandru B, Cojocaru R, Büke C, Paramythiotou E, Angebault C, et al. Relative fecal abundance of extended-spectrum beta-lactamases-producing Escherichia coli and their occurrence in urinary-tract infections in women. Antimicrob Agents Chemother. 2013;57:4512–7.
Grabow WO, Prozesky OW. Drug resistance of coliform bacteria in hospital and city sewage. Antimicrob Agents Chemother. 1973;3:175–80.
Nicolas-Chanoine M-H, Jarlier V, Robert J, Arlet G, Drieux L, Leflon-Guibout V, et al. Patient’s Origin and Lifestyle Associated with CTX-M-Producing Escherichia coli: A Case–control-Control Study. PLoS One. 2012; doi:10.1371/journal.pone.0030498.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SH performed experimental work, analysed the study data and critically reviewed the manuscript. LD preformed experimental work, analysed the study data and drafted the manuscript. LM and VJ conceived the study, analysed the data and critically reviewed the manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Drieux, L., Haenn, S., Moulin, L. et al. Quantitative evaluation of extended-spectrum β-lactamase-producing Escherichia coli strains in the wastewater of a French teaching hospital and relation to patient strain. Antimicrob Resist Infect Control 5, 9 (2016). https://doi.org/10.1186/s13756-016-0108-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13756-016-0108-5