
Abstract
Background
Unintended pregnancy is a pregnancy either mistimed or unwanted. The main consequence of unintended pregnancy is inducing abortion. In Ethiopia, more than half of unintended pregnancies end up in abortion.
Objective
This study aims to measure the change in unintended pregnancy among women of reproductive age between survey years 2005 and 2016 and to identify the socio-demographic factors that most significantly contributed to the change.
Methods
Data from the two most recent Ethiopian Demographic and Health Surveys (EDHS) were analyzed. We quantified the contribution of socio-demographic factors in the change of unintended pregnancy, using Oaxaca-Blinder decomposition for non-linear regression models by applying the STATA command ‘mvdcmp’.
Result
Unintended pregnancy decreased from 37% in 2005 to 27% in 2016 in Ethiopia. Both changes in population characteristics and coefficient were the contributing elements to the observed change in unintended pregnancy. Among population characteristics factors, being a partial decision-maker and being a slum in the Somali region contributed 10 and 14% to the change of unintended pregnancy between the 2005 and 2016. Of the coefficient factors, knowledge of modern family planning, being a partial decision-maker, media exposure, distance to health facilities, and health facility visits contributed to the change by 93, 43, 17, and 10% respectively.
Conclusion
The majority of the change in unintended pregnancy from 2005 to 2016 survey was due to differences in coefficients (85%). The principal contributing factors to the change of unintended pregnancy were FP knowledge, decision making, media exposure and health facility visits. Therefore, an interventional plan will be efficient, better, and more effective if focused on the larger contributing factors.
Similar content being viewed by others

Introduction
As defined by the Centers for Disease Control and Prevention (CDC), unintended pregnancy is defined as a pregnancy that is either unwanted, or the pregnancy is mistimed, such as the pregnancy occurring earlier than desired [1].
Worldwide, the rate of pregnancy shows significant decrement, but the rate of unintended pregnancy remains high. From 1990 to 2015 the rate of unintended pregnancy declined 15 percentage points (i.e. from 79 to 64%) [2]. Globally, of the 208 million pregnancies that happened in 2008, 86 million (41%) were unintended and 40% of the total pregnancies in developing countries were unintended [3]. Similarly, Of these 85 million unintended pregnancies that occurred in 2012, 50% they resulted in abortion, 13% ended in miscarriage, and 38% resulted in an unplanned birth [4]. Nearly 40% of unintended pregnancies ended in abortion from 2015 to 2019 [2]. The burden of unintended pregnancy remains high in Africa. According to a study done using multiple sources of data to estimate unintended pregnancy, 35% of the total pregnancies in Africa were unintended.
Pocket Studies done in different portions of Ethiopia showed a high prevalence of unintended pregnancy. For instance, a study conducted in the central portion of the country revealed that the prevalence of unintended pregnancy was 41.5% [5]. Other studies also reached a similar conclusion were; Gelan District (55%) [6] Hadiya zone(36%) [7], Gondar city (47%) [8], and Harari (33%) [9]. The consequences of unintended pregnancy are eclampsia, preeclampsia, and hemorrhage after birth, relative to planned pregnancy [10]. But, the most unpleasant outcome of unintended pregnancy is unsafe abortion [11, 12]. In Ethiopia, more than 50% of unintended pregnancies end up in induced abortion [9].
Much kind research revealed that socio-demographic factors such as; maternal age [5, 13, 14], level of education [13, 15,16,17], religion [18,19,20], marital status [5, 21, 22], distance from the nearest health facilities, parity [5, 13, 16, 18], household size [22, 23], wealth status [20], knowledge on ovulation cycle, knowledge on family planning [16], ever had terminated pregnancy [5, 14, 24] residence [16, 18, 20] and region [13, 23] were the main factors associated with unintended pregnancy. Therefore, to close the huge gap in this country, major contributing factors to the decrease or increase of unintended pregnancy need to be identified using nonlinear regression methods.
There hasn’t been any study that used broadly representative data to identify the contributing factors to the Change in unintended pregnancy. In Ethiopia, prior studies were mainly focused on the prevalence and determinant factors of unintended pregnancy using a dataset of a single survey. The factors which contributed to the change of unintended pregnancy remained untouched. Therefore, this study is aimed to address the contributing factors for the changes in unintended pregnancy through multivariable decomposition analysis based on the 2005 and 2016 EDHS.
This study applied multivariable decomposition analysis to identify which socio-demographic predictors are strongly correlated with the change in unintended pregnancy among reproductive-age women (15–49 years) in Ethiopia. We hypothesized that the change of unintended pregnancy changed in Ethiopia between the two survey periods and different factors contributed to the change of unintended pregnancy.
Method and materials
Study design and sampling procedures
The data utilized for this study were retrieved from 2005 and 2016 EDHS. These surveys were carried out using a stratified two-stage random sampling method. In the first stage, 540 Enumeration Areas (EAs) in EDHS 2005 and 645 EAs in EDHS 2016 were randomly selected proportional to their EA size and, on average, 27 to 32 households per EAs were selected in the second stage.
A weighted sample of 14,890 (7300 in survey 2005 and 7590 in survey 2016) reproductive-age women were incorporated in this study. Sample weighting was applied to correct for the under or over-sampling of different strata during sampling. If weights had been used, all calculations would have been biased towards the levels and relationships in the over-sampled strata. Therefore, weighting the sample helps in restoring the representativeness of the survey and in getting reliable statistical estimates. Detailed information about sampling procedures was showcased in the EDHS reports [25, 26].
Study variables outcome variable
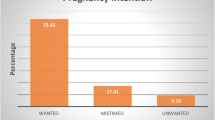
The outcome variable was unintended pregnancy, which is defined as either unwanted or mistimed pregnancy. Unwanted pregnancy is a pregnancy that took place when no longer child is required by the woman. Mistimed pregnancy is a pregnancy that came earlier than expected time [1]. The outcome variable was dichotomized as “unintended” if women had encountered either unwanted or mistimed last pregnancy were coded 1 otherwise “wanted” code 0.
Independent variables
The independent variables regarded in this study were: age, educational status, religion, marital status, place of residence, women working status, household wealth status, media exposure, ever termination of pregnancy, knowledge of family planning, history of visiting health facilities in the last 12 months, history of a visit by field workers in the last 12 months, perceived distance from home to proximate health facilities, age at first marriage, parity, sex of household head, region of residency, and desired number of children.
Operational definition
Media exposure
Created by combining whether a respondent reads the newspaper, listens to the radio, or watches television. If the woman was exposed to at least one of the three Media she was considered as “exposed” and otherwise “not exposed” coded “0”. This is done to overcome the reduction of sample size when the three media exposure is used as independent variable separately. For example, only educated women are eligible for the question “do you read a newspaper?” and this will exclude uneducated women. The same is true for watching television, that only women who have access to electricity are suited for this question.
Statistical analysis
Important variables were extracted from the Individual Record (IR) datasets. Data were weighted using the “svyset” STATA command, and it was applied for descriptive analysis. The variables required for the “svyset” are the weight variable (v005), primary sampling unit (v021), and strata (v023).
Non-linear multivariable decomposition analysis
Logit-based multivariable decomposition analysis for a non-linear response model was calibrated to analyze the change in unwanted pregnancy between the two surveys. This model was applied to identify the source of variations of unintended pregnancy between the two surveys (i.e.2005 and 2016). The Logit-based multivariable decomposition analysis utilizes the output from the logistic regression model to assign the observed change in unintended pregnancy over time into different components.
Using the Stata command “append,” the 2016 EDHS dataset was appended to the 2005 EDHS dataset for analysis. Moreover, the Logit-based multivariable decomposition analysis was calibrated using the “mvdcmp” STATA command. The change in unintended pregnancy can be explained by the compositional difference (i.e. the difference in characteristics) and/or the difference in effects of explanatory variables (i.e. the difference in the coefficients) between the surveys. For logistic regression, the Logit or log-odd of unintended pregnancy is taken as:
[27].
X indicates independent variables (unintended pregnancy).
β denotes that, the regression coefficient of each selected explanatory variables.
The E component refers to the part of the differential owing to differences in endowments or characteristics. The C component refers to that part of the differential attributable to differences in coefficients or effects.
Ethical approval and consent
Since the study was a secondary data analysis of publicly available survey data from the MEASURE DHS program, ethical approval and participant consent were not necessary for such kind of study. We requested DHS Program, and authorization was awarded to download and use the data for advance analysis from the website http://www.dhsprogram.com.
Result
Characteristics of the study population
Nearly half of the study participants in 2005 (46.4%) and 2016 (50.4%) were aged between 25 and 34 years. The percent of none educated women decreased by 15% from 2005 to 2016 (Table 1).
Change of unintended pregnancy
The magnitude of unintended pregnancy decreased from 37% in 2005 to 27% in 2016 surveys (Table 1).
Decomposition analysis
Variables with a p-value less than 0.2 from the bi-variable decomposition analysis were selected as candidate variable for multivariable decomposition analysis. Because there is a greater amount of missing value, the variable parity is dropped entirely. Additionally, the variable region, religion, and place of residence had a p-value of 0.2 in the bivariable analysis, they were not transferred to a multivariable analysis. The multivariable decomposition regression models found that 85.2% of the decline in unintended pregnancy from 2005 (37%) to 2016 (27%) was attributed to changes in the coefficients (mother’s characteristics) and only 14.8% of the decline was due to changes in the population characteristics (population dynamics) (Table 2).
Non-linear decomposition analysis
The multivariable decomposition comparison showed that the combined effect of all changes in the distribution of population characteristics (endowments) changed the prevalence of unintended pregnancy rate by 1.6% points (a 14.8% decrease = − 0.016033/− 0.10831). The combined effect of all coefficients would have been to decrease unintended pregnancy by 9.3% points (85.2% decrease) due to behavioral effects (Table 2). This finding can be alternatively interpreted as if the composition of the women population composition had remained the same for the 2005 and 2016 surveys, the rate of unintended pregnancy would have increased by 14.8%. Besides, if the effect of the coefficient of each variable had not changed, the rate of unintended pregnancy would have been elevated by 85.2%.
Difference due to characteristics (Endowment)
Keeping the effect of change in the coefficient of each variable constant, 15% of changes in unintended pregnancy was due to dissimilarity in the composition of women between 2005 and 2016 surveys. Being in the age group of 15–24 years, being a partial decision maker, being a resident of Afar, being a resident of Amhara, being the resident of Oromia region, and being the resident of SNNP all significantly contributed to the change in magnitude of unintended pregnancy. Being a resident of the Somali region and being a partial decision-maker are among the most influential compositional factors.
If women in 2005 had the same behavioral response (i.e., residency in Somalia & partial decision maker) as women in 2016, the prevalence of unintended pregnancy is expected to increase by 14 and 10% percent respectively keeping all other compositional and coefficient factors constant (Table 3).
Difference due to effects of the coefficient
Keeping the effect of change in compositional characteristics stationary, 85% of changes in unintended pregnancy was attributable to the difference in the effect of coefficient (Table 3). This means 85% of the change in unintended pregnancy among reproductive-age women was explained by differences in coefficient across the two surveys. Change of the effect of educational status (secondary and above), autonomy in decision making (partial maker), media exposure (being exposed), perceived distance to nearby health facilities (perceived as a big problem), is not working, being knowledgeable on family planning method, and region of residency (being a resident of Oromia, Somali, Benishangul, SNNPR, Gambela, Harari) were the main explanatory variables for the change of unintended pregnancy over the last 11 years (Table 3).
Knowledge of family planning, being a partial decision-maker, media exposure (exposed), visiting health facilities, and perceived distance to health facilities were factors with the most influential coefficients.
If the influence of the coefficient of knowledge of family planning remained identical between 2005 and 2016, the magnitude of unintended pregnancy would have elevated by 93% in 2016. Similarly, the prevalence of unintended pregnancy would have increased by 43.5%, if the coefficient of partial autonomy in decision making remained the same for the last 11 years. Additionally, the prevalence of unintended pregnancy would have been reduced by 5.3%, if the effect coefficient of being educated to secondary school and above was brought the same in the 2005 and 2016 surveys (Table 3). Therefore, equalizing the differential effects of educational status alone could reduce the risk of unintended pregnancy by 5.3%.
Discussion
This study identified and evaluated contributions of differences in measurable characteristics and effects of coefficients on change of unintended pregnancy from 2005 to 2016 surveys in Ethiopia. Besides, a considerable reduction in unintended pregnancies was observed between those survey periods (reduced from 37 to 27%). This finding is coherent with other DHS trend analysis carried out in Nigeria, which pointed out that unintended pregnancy reduced from 16.3% in 2003 to 10.6% in 2013 [15]. The increased utilization of modern family planning uptake [28], increased involvement of donor support, elevated public-private partnerships, and the expansion of health extension programs, all of which may have boosted the reduction of unintended pregnancy in Ethiopia [29, 30].
The major portion of change of unintended pregnancy was shared by dissimilarity in the effect of coefficients of explanatory variables across the two surveys. More than 93% of the change in unintended pregnancy was imputable to changes in women who are knowledgeable on modern family planning holding other variables’ coefficient effect constant, a finding in line with other studies from Jamaica [31]. This may be due to women who have good knowledge on modern family planning are more likely to uptake family planning services compared to less those knowledgeable, which prevent unplanned pregnancy [32]. Therefore, we call for health services providers to play a significant role in mothers’ understanding of modern family planning and to approach women based on their knowledge of status.
Change in the coefficient effect of being women partial decision-maker, shifted the number of unintended pregnancies by 43%. This finding is consistent with the study done in Bangladesh [33] and Ghana [34], which declared that as the autonomy scale of women in decision making increases the prevalence of unintended pregnancy decreases. This is because of women having autonomy in health decision especially decision making related to family planning are more likely to utilize modern family planning and in return drives to halt unintended pregnancy [7].
Unequal distribution of the effect of coefficient of distance from health facilities (perceived as not a big problem) contributed positively (i.e., 10% rise) to the prevalence of unintended pregnancy. This finding is supported by studies carried out in Ethiopia [35,36,37]. This might be justified through, women who reported the distance to proximate health facilities as not big problem are expected to have easy access to family planning and to have good knowledge of other reproductive health-related counseling services [38]. Other studies revealed that as the distance to proximate health facilities increases, the probability of visiting to get services decreases [39,40,41]. Having a long-distance from facility to residency also decay the probability of visiting facilities through increasing cost of transport and rising issues delaying productive activities [42, 43].
Visit health facilities was one of the reasons for the reduction of unintended pregnancy by 10%.this finding is consistent with the fact that women who visit health facilities have good opportunities to access family planning services to nullify unintended pregnancy [44] as the biggest reason for unintended pregnancies is not using family planning (either not using consistently or appropriately) [45, 46]. This finding has important implications in that equalizing the distribution of women who perceived the distance as not a big problem in 2016 with 2005 would have decreased the prevalence of unintended pregnancy by 10%.
The main strength of this study the authors utilized a large and representative datasets to compare the magnitude of unintended pregnancy between two surveys. Besides, advanced statistical model to address the main contributing factors to the change of unintended pregnancy in Ethiopia. Even though we compared two large datasets to show the change and contributing factors to the change of unintended pregnancy, we were unable to consider other significant contributing variables (cultural, clinical, and other factors) which were not collected by the EDHS program. The fact that the women were asked about the state of their socio-demographic characteristics throughout the previous 5 years prior to the study during the survey period means that this research is not free from recall bias.
Finally, we recommend the upcoming researchers better to do studies that includes the, missed cultural, clinical and other pertinent factors to get good statistical power. As the change in the magnitude of unintended pregnancy in Ethiopia is not satisfactory, deep understanding and knowledge is required through conducting qualitative research methods. For Ethiopian women, we recommend to follow Medias, to know the modern family planning and get awareness about the consequences of unintended pregnancy.
Conclusion
The present study provide evidence on sources of change in unintended pregnancy between the 2005 and 2016 EDHS. The principal contributing factors to the change of unintended pregnancy were FP knowledge, decision making, media exposure and health facility visits. We conclude that interventional activities better to prioritize women having poor understanding of modern family planning, women having poor participation decision making and women having not satisfactory visits to health facilities.
Availability of data and materials
The datasets and materials are available at www.dhsprogram.com. Additional data and materials utilized in this study can be obtained from corresponding author for a reasonable request.
Abbreviations
- EDHS:
-
Ethiopian Demographic Health Surveys
- EAs:
-
Enumeration areas
- FP:
-
Family planning
- SNNP:
-
South nations and nationalities people
References
CDC. reproductive health 2021 [updated June 28, 2021; cited 2021 jan 22/2022]. Available from: https://www.cdc.gov/reproductivehealth/contraception/unintendedpregnancy/index.htm.
Guttmacher insatitute. Unintended pregnancy and abortion worldwide Global and Regional estimates of unintended pregnancy and abortion 2022 [cited 2022 August 8]. Available from: https://www.guttmacher.org/fact-sheet/induced-abortion-worldwide#..
Singh S, Sedgh G, Hussain R. Unintended pregnancy: worldwide levels, trends, and outcomes. Stud Fam Plan. 2010;41(4):241–50.
Sedgh G, Singh S, Hussain R. Intended and unintended pregnancies worldwide in 2012 and recent trends. Stud Fam Plan. 2014;45(3):301–14.
Fite RO, Mohammedamin A, Abebe TW. Unintended pregnancy and associated factors among pregnant women in Arsi Negele Woreda, West Arsi Zone. Ethiopia BMC Res Notes. 2018;11(1):1–7.
Yohannes E, Balis B. Unintended Pregnancy and Associated Factors among Women Who Live in Ilu Gelan District, Western Ethiopia, 2021. Int J Reprod Med. 2022;2022:8646724.
Abame DE, Abera M, Tesfay A, Yohannes Y, Ermias D, Markos T, et al. Relationship between unintended pregnancy and antenatal care use during pregnancy in Hadiya Zone, Southern Ethiopia. J Reprod Infertility. 2019;20(1):42.
Asratie MH. Unintended pregnancy during COVID-19 pandemic among women attending antenatal care in Northwest Ethiopia: magnitude and associated factors. Int J Women’s Health. 2021;13:461.
Worku S, Fantahun M. Unintended pregnancy and induced abortion in a town with accessible family planning services: the case of Harar in eastern Ethiopia. Ethiop J Health Dev. 2006;20(2):79–83.
Gerdts C, Dobkin L, Foster DG, Schwarz EB. Side effects, physical health consequences, and mortality associated with abortion and birth after an unwanted pregnancy. Womens Health Issues. 2016;26(1):55–9.
Brown SS, Eisenberg L. The best intentions: Unintended pregnancy and the well-being of children and families; 1995.
Yazdkhasti M, Pourreza A, Pirak A, Abdi F. Unintended pregnancy and its adverse social and economic consequences on health system: a narrative review article. Iran J Public Health. 2015;44(1):12.
Nyarko SH. Unintended pregnancy among pregnant women in Ghana: prevalence and predictors. J Pregnancy. 2019;2019:2920491.
Tsegaye AT, Mengistu M, Shimeka A. Prevalence of unintended pregnancy and associated factors among married women in west Belessa Woreda, Northwest Ethiopia, 2016. Reprod Health. 2018;15(1):1–8.
Yaya S, Amouzou A, Uthman OA, Ekholuenetale M, Bishwajit G, Udenigwe O, et al. Prevalence and determinants of terminated and unintended pregnancies among married women: analysis of pooled cross-sectional surveys in Nigeria. BMJ Glob Health. 2018;3(2):e000707.
Habib MA, Raynes-Greenow C, Nausheen S, Soofi SB, Sajid M, Bhutta ZA, et al. Prevalence and determinants of unintended pregnancies amongst women attending antenatal clinics in Pakistan. BMC Pregnancy Childbirth. 2017;17(1):1–10.
Wellings K, Jones KG, Mercer CH, Tanton C, Clifton S, Datta J, et al. The prevalence of unplanned pregnancy and associated factors in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Lancet. 2013;382(9907):1807–16.
Goshu YA, Yitayew AE. Prevalence and determinant factors of unintended pregnancy among pregnant women attending antenatal clinics of Addis Zemen hospital. PLoS One. 2019;14(1):e0210206.
Getachew FD. Level of unintended pregnancy and its associated factors among currently pregnant women in Duguna Fango district, Wolaita zone, southern Ethiopia. Malaysian J Med Biol Res. 2016;3(1):11–24.
Ameyaw EK. Prevalence and correlates of unintended pregnancy in Ghana: Analysis of 2014 Ghana Demographic and Health Survey. Matern Health Neonatol Perinatol. 2018;4(1):1–6.
Kassahun EA, Zeleke LB, Dessie AA, Gersa BG, Oumer HI, Derseh HA, et al. Factors associated with unintended pregnancy among women attending antenatal care in Maichew Town, Northern Ethiopia, 2017. BMC Res Notes. 2019;12(1):1–6.
Yenealem F, Niberet G. Prevalence and associated factors of unintended pregnancy among pregnant woman in Gondar town, North west Ethiopia, 2014. BMC Res Notes. 2019;12(1):1–5.
Tebekaw Y, Aemro B, Teller C. Prevalence and determinants of unintended childbirth in Ethiopia. BMC Pregnancy Childbirth. 2014;14(1):1–9.
Rizvi F, Williams J, Hoban E. Factors influencing unintended pregnancies amongst adolescent girls and young women in Cambodia. Int J Environ Res Public Health. 2019;16(20):4006.
Demographic E. Health Survey. Addis Ababa and Calverton: Central Statistical Agency and ORC Macro; 2006.
Csa I. Central statistical agency (CSA)[Ethiopia] and ICF. Addis Ababa and Calverton: Ethiopia Demographic and Health Survey; 2016.
Powers DA, Yoshioka H, Yun M-S. mvdcmp: Multivariate decomposition for nonlinear response models. Stata J. 2011;11(4):556–76.
Fekadu GA, Omigbodun AO, Roberts OA, Yalew AW. Determinants of change in long-acting or permanent contraceptives use in Ethiopia; A multivariate decomposition analysis of data from the Ethiopian demographic and health survey. PLoS One. 2020;15(1):e0227218.
Yalew SA, Zeleke BM, Teferra AS. Demand for long acting contraceptive methods and associated factors among family planning service users, Northwest Ethiopia: a health facility based cross sectional study. BMC Res Notes. 2015;8(1):1–10.
USAID A. Three successful Sub-Saharan Africa family planning programs: lessons for meeting the MDGs. Washington DC: USAID; 2012.
Hylton-Kong T, Bailey A, Steiner MJ, Gallo MF. Contraceptive knowledge among women at risk of unintended pregnancy in Kingston, Jamaica. Women Health. 2021;61(3):294–302.
Duze MC, Mohammed IZ. Male knowledge, attitude, and family planning practices in Northern Nigeria. Afr J Reprod Health. 2006;10(3):53–65.
Rahman M. Women’s autonomy and unintended pregnancy among currently pregnant women in Bangladesh. Matern Child Health J. 2012;16(6):1206–14.
Bain LE, Muftugil-Yalcin S, Amoakoh-Coleman M, Zweekhorst M, Becquet R, de Cock BT. Decision-making preferences and risk factors regarding early adolescent pregnancy in Ghana: stakeholders’ and adolescents’ perspectives from a vignette-based qualitative study. Reprod Health. 2020;17(1):1–12.
Bekele YA, Fekadu GA. Factors associated with unintended pregnancy in Ethiopia; further analysis of the 2016 Ethiopian demographic health survey data. BMC Pregnancy Childbirth. 2021;21(1):1–7.
Getu Melese K, Gebrie MH, Berta Badi M, Fekadu MW. Unintended Pregnancy in Ethiopia: Community Based Cross-Sectional Study. Obstet Gynecol Int. 2016;2016:4374791.
Kassa N, Berhane Y, Worku A. Predictors of unintended pregnancy in Kersa, Eastern Ethiopia, 2010. Reprod Health. 2012;9(1):1–7.
Gonie A, Wudneh A, Nigatu D, Dendir Z. Determinants of family planning use among married women in bale eco-region, Southeast Ethiopia: a community based study. BMC Womens Health. 2018;18(1):1–10.
Feikin DR, Nguyen LM, Adazu K, Ombok M, Audi A, Slutsker L, et al. The impact of distance of residence from a peripheral health facility on pediatric health utilisation in rural western Kenya. Tropical Med Int Health. 2009;14(1):54–61.
Adazu K, Lindblade KA, Rosen DH, Odhiambo F, Ofware P, Kwach J, et al. Health and demographic surveillance in rural western Kenya: a platform for evaluating interventions to reduce morbidity and mortality from infectious diseases. 2005.
Mwaniki P, Kabiru E, Mbugua G. Utilisation of antenatal and maternity services by mothers seeking child welfare services in Mbeere District, Eastern Province, Kenya. East Afr Med J. 2002;79(4):184–7.
Awoyemi T, Obayelu O, Opaluwa H. Effect of distance on utilization of health care services in rural Kogi State, Nigeria. J Human Ecol. 2011;35(1):1–9.
Girma F, Jira C, Girma B. Health services utilization and associated factors in jimma zone, South west ethiopia. Ethiop J Health Sci. 2011;21(Suppl 1):85–94.
Curtis C, Huber D, Moss-Knight T. Postabortion family planning: addressing the cycle of repeat unintended pregnancy and abortion. Int Perspect Sex Reprod Health. 2010;36(1):44–8.
Bellizzi S, Mannava P, Nagai M, Sobel H. Reasons for discontinuation of contraception among women with a current unintended pregnancy in 36 low and middle-income countries. Contraception. 2020;101(1):26–33.
Centers for diseses control and prevention c. Reproductive Health: CDC; 2021 [updated June 28, 2021; cited 2022 2/26/2022]. Available from: https://www.cdc.gov/reproductivehealth/contraception/unintendedpregnancy/index.htm.
Funding
The authors received no specific funding for this work.
The authors have not received a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
AAT: Conceptualization, Formal analysis, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. EBE: Conceptualization, Formal analysis, Methodology, Resources, Software, Validation, Writing – original draft, Writing – review & editing. ATD: Formal analysis, Methodology, Software, Writing – review & editing. AWS: Resources, Visualization, Software, Writing – review & editing. MDK: Investigation, Methodology, Validation, Writing – review & editing. HBE: Formal analysis, Software, Writing – original draft, Writing – review & editing. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Permission to access data was obtained from major demographic and health surveys through requesting online to the website http://www.dhsprogram.com. The data used for this study were publicly available with no personal identifier. Our study was based on secondary data from Ethiopian Demographic and Health surveys and we have secured the permission letter from the major Demographic Health and surveys website.
Consent for publication
Not applicable.
Competing interests
The authors have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tareke, A.A., Enyew, E.B., Dubale, A.T. et al. Determinants of change in unintended pregnancy in Ethiopia using the 2005 and 2016 EDHS: non-linear multivariable decomposition analysis. Arch Public Health 80, 232 (2022). https://doi.org/10.1186/s13690-022-00984-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13690-022-00984-2