
Abstract
Background
Upper limb (UL) disabilities have attracted worldwide attention due to the high economic costs of health care and the negative effects on the quality of life of patients with these disabilities. Telerehabilitation technologies are one of the most important ways to reduce rehabilitation costs and increase the quality of life of patients. Therefore, the aim of this study was to investigate the role of telerehabilitation in improving the health status of patients with upper limb disabilities.
Methods
This scoping review was conducted by searching the Web of Science, PubMed, and Scopus until July 30, 2021. We used a data extraction form with 18 fields to extract data from primary studies. The selection of articles and data extraction was made by four researchers using a data collection form based on inclusion and exclusion criteria. Disagreements were resolved through consultation with the fifth and sixth researchers.Inclusion criteria were studies published in English, studies on upper limb disability, and telerehabilitation based on any technology (synchronous telerehabilitation, asynchronous, or both). Exclusion criteria were articles that did not focus on telerehabilitation and upper limb disabilities. Also, books, book chapters, letters to the editor, and conference abstracts were also removed.
Results
A total of 458 articles were retrieved, and after removing irrelevant and duplicate articles, 29 articles were finally included in this review. Most telerehabilitation was performed for patients with stroke (65%). Among the 15 different services provided with telerehabilitation technologies, "Evaluation of exercises and also a musculoskeletal function of patients by the therapist","Recording of patients' rehabilitation exercises and sending them to the therapist” and "Prescribing new rehabilitation exercises by the therapist" were the most widely used services, respectively. Virtual reality technologies, smart wearables, and robots were used to provide telerehabilitation services. Among the 13 types of evaluation used for telerehabilitation systems, “Evaluation and measurement of upper limb function” was the most used evaluation in the studies. "Improvement in musculoskeletal functions”, "Increasing patients' interest and motivation to perform rehabilitation exercises", and "Increasing adherence to rehabilitation exercises and greater participation in treatment processes" were the most important outcomes, respectively.
Conclusion
Our findings indicate that telerehabilitation provides individuals with equitable access to rehabilitation services, improves musculoskeletal function, and empowers individuals by providing a variety of rehabilitation capabilities.
Similar content being viewed by others

Background
Upper limb (UL) disability is a common health problem in the general population [1]. Upper limb disabilities have attracted worldwide attention due to the high economic costs of their health care and negative effects on the individuals’ quality of life [1]. Patients with these disabilities, on the other hand, have a shorter period of illness and are discharged from hospitals sooner than in the past. This is mainly due to the time limits and economic considerations that health organizations are facing. However, many of these patients still need rehabilitation services to fully recover from the disease. In addition, such services are often costly and patients sometimes have to make several travels to a rehabilitation center during the treatment process [2].
Technology advancements have enabled new approaches to rehabilitate upper limb disabilities. Internet access and video conferencing have grown in popularity over the last decade, allowing for remote training for people with upper limb disabilities [3]. Telerehabilitation, as an emerging field of telemedicine, is defined as a set of tools, procedures, and protocols for providing rehabilitative processes remotely [4]. Telerehabilitation has the potential to provide rehabilitation services that go beyond conventional treatment and address the current functional needs of patients with chronic upper extremity injuries [3]. The technology improves service quality by monitoring patients on-site, mainly in communities far from urban centers. This technology is also expected to improve the cost-effectiveness of interventions [5]. Previous systematic studies evaluated the feasibility, effectiveness, and cost issues of telerehabilitation for individuals with a variety of health conditions. The results of these studies showed that remote rehabilitation is an effective alternative to face-to-face interventions [6, 7].
To our knowledge, no comprehensive review has been published on the telerehabilitation of upper limb disabilities as yet. As a result, the purpose of this scoping review is to identify the functions and outcomes of telerehabilitation intervention in the recovery of upper limb functions. In addition, we identified various evaluation methods for telerehabilitation systems in this study.
Material and methods
The current study is a scoping review on the functions and outcomes of telerehabilitation in the improvement of upper limb disabilities. Scoping reviews are an effective and useful method for determining the scope or coverage of a body of literature on a specific topic, as well as providing a clear indication of the volume of literature and studies available, and an overview (broad or detailed) of its focus [8]. It should be noted that we used the PRISMA scoping reviews checklist for selecting studies and reporting the results [9].
Information sources and search strategy
To find articles about telerehabilitation for upper limb disabilities, three databases were searched: PubMed, Web of Science, and Scopus until January 3, 2022. The keywords upper limb disability and telerehabilitation were used to conduct the search process. The search strategy was developed by three researchers (KB, AH, and ASH) and finally approved by KHM and ASH. The keywords and search strategies used in each database are listed in Additional file 1: Appendix A. In January 2022, the search was carried out across all three databases. Furthermore, we did not impose any restrictions on the database search's starting point. It should be noted that in order to access articles that we did not have full-text access to, we emailed the corresponding author and requested that they send them to us.
Eligibility criteria
In this study, articles focusing on telerehabilitation and upper limb disability were included. Inclusion criteria included articles published in English, research on upper limb disability due to any disease or injury, telerehabilitation based on any technology (robotics, smart wearables, and virtual reality), and synchronous telerehabilitation (real-time or live video) and asynchronous (stored-and-forward). Exclusion criteria also included articles that did not focus on telerehabilitation and upper limb disabilities. Books, book chapters, letters to the editor, and conference abstracts were also removed.
Selection of sources of evidence
First, abstracts of all retrieved articles were entered into EndNote software and duplicate articles were excluded by KHM. Then, according to the inclusion and exclusion criteria, title and abstract of the articles, related studies were selected by AH, MGH, and MSH. All valid articles included in the study were reviewed by KB and KHM (authors reviewed an article together) and finally approved by ASH. In case of disagreement, the final decision on each article would be decided by discussion between the authors. After the final approval of the articles, their full texts were reviewed by KHM and ASH to extract the required data.
Data charting process and data items
We used a data extraction form to extract data from primary studies. The validity of this form was confirmed by two medical informatics and health information management specialists. Data extraction form includes fields such as country, publication year, the purpose of study, disease leading to upper limb disability, upper limb part involved in the disability (Table 1 and more details in Additional file 1: appendix B), functions and services of telerehabilitation, services provided with telerehabilitation systems (Table 2 and more details in Additional file 1: appendix B), hardware equipment used in providing telerehabilitation services (Additional file 1: appendix B), assistive technologies to provide telerehabilitation services, types of services (synchronous and asynchronous, synchronous or asynchronous) (Table 3 and more details in Additional file 1: appendix B), equipment used to build the robot, use of smart wearables devices type of smart wearable devices, equipment used to make the smart wearable devices (Additional file 1: appendix B), duration of use of the telerehabilitation systems (Additional file 1: appendix C), evaluation and type of evaluation, samples size ( Table 4 and more details in Additional file 1: appendix C), outcomes and results ( Table 5 and more details in Additional file 1: appendix C).
Data collation process
After the final approval of the articles in the previous steps, in order to extract the required information, their full text was read separately by KB, KHM, and ASH. Necessary information was extracted from the articles and recorded in the above-mentioned data extraction form (KB, KHM and ASH). Then, the information extracted from the articles was re-examined separately by MGH and MSH and confirmed by AH. When there was disagreement about the information extracted, the members of the research team met to make a final decision. It should be noted that for articles with missing information, we emailed the corresponding author and asked them to send us the missing information. Finally, the extracted information was entered into an Excel spreadsheet.
Synthesis of results
After entering the extracted data into an Excel file, we qualitatively classified the various telerehabilitation applications in patients with upper limb disabilities and reported their results and frequency. To synthesize data, the authors used the advancement scoping method recommended by Levac et al. [10]. One author (KHM) refined the data (e.g., spell check, cell formatting) to ensure that Excel performed procedures, calculations, and analyses correctly and adequately (e.g., making axis tables, and charts). Because scoping reviews do not seek to summarize or weigh evidence from various studies [10, 11], only descriptive analyses (e.g., frequencies, percentages) were performed on the extracted data to describe the findings of the included studies [12]. The descriptive data and findings from the included articles were organized into tables and figures based on themes to provide the review's findings, which guided the study objectives (by KB, KHM, and ASH). If the authors disagreed, the final decision on each figure or table was reached through discussion.
Ethical considerations
The protocol of this study was approved by the ethical committee of Kerman University of Medical Sciences (IR.KMU.REC.1400.606).
Results
Selection of sources of evidence
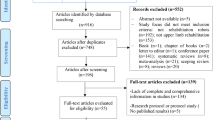
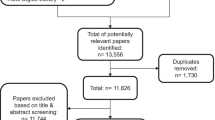
In total, 458 articles were retrieved. After removing duplicates, the remaining 387 studies were carefully reviewed and assessed based on inclusion and exclusion criteria. Finally, 29 articles were included in the study. The results of the search and study selection are presented in Fig. 1.

Study selection process
Characteristics of the included studies
An overview of selected studies is presented in Table 1.
As shown in Fig. 2, telerehabilitation technologies are used to rehabilitate upper limb disabilities since 2002. Most articles were published in 2014 [25,26,27], 2016 [30,31,32] and 2019 [37,38,39](n = 3). No studies were published in 2003 or 2008. (More details in Table 1).

Distribution of the studies in terms of publication year
The majority of studies were conducted in the United States (n = 12, 41%) [3, 13,14,15,16, 18, 21, 22, 26, 29, 37, 40]. Also, 6.88% of studies were carried out in Australia (n = 2) [23, 33]. South Korea, China, Taiwan, and Japan are the only Asian countries to conduct telerehabilitation studies for upper limb disabilities limb (see Table 1 for more details).
As shown in Fig. 3, telerehabilitation was performed for eight categories of diseases or complications leading to upper limb disabilities. Most telerehabilitation was performed for patients with stroke (n = 19 (65%) [3, 13,14,15,16,17,18,19,20,21,22, 24, 28, 31, 32, 36, 38,39,40]. The frequencies and percentages of other diseases are shown in Fig. 3.

The distribution of the studies based on diseases and injuries leading to upper limb disabilities
Functions and services of telerehabilitation
A total of 15 different functions and services were identified for telerehabilitation systems. "Evaluation of exercises and also a musculoskeletal function of the patient by the therapist” (n = 19), "Recording of patients' rehabilitation exercises and sending them to the therapist" (n = 16), and "Prescribing new rehabilitation exercises by the therapist "(n = 16) were the most widely used functions and services of telerehabilitation systems for rehabilitation of upper limb disabilities, respectively. (Table 2, more details in Additional file 1: Appendix B).
Methods of providing telerehabilitation services and exercises
According to Table 3, virtual reality technologies, smart wearable devices, and robots were used to provide telerehabilitation services. Virtual reality was the most widely used technology. Different types of rehabilitation services were provided to patients in three forms: synchronous, asynchronous, and a combination of synchronous and asynchronous. Combined synchronous and asynchronous services were the most common type of services. (More details in Additional file 1: Appendix B).
Evaluations in telerehabilitation systems for upper limb disabilities
The number of participants in the evaluation of telerehabilitation systems varied from one to 85 people. Also, the minimum and maximum duration of the evaluation processes were 20 min [37] to 14 months [22], respectively. According to Table 4, thirteen different types of evaluations were performed for telerehabilitation systems in upper limb rehabilitation. “Evaluation and measurement of upper limb function” was the most common type of evaluation (n = 21). “Fugl-Meyer Upper Extremity score (FMA-UE)” was the most widely used evaluation method in the measurement of upper limb function (n = 9). Evaluation of “Range and motor skills and functional strength of the hand” was in the next rank (n = 7). As shown in Table 4, 8 different evaluation methods were used. After "Range and motor skills and functional strength of the hand", “Lab-based clinical and kinematic “ and “Patient satisfaction” were the most used evaluation methods (n = 5). Questionnaires and interviews were used to assess patient satisfaction. Questionnaire (n = 3) was used more than interview (n = 1). (More details in Additional file 1: Appendix C).
Outcomes of using telerehabilitation systems for upper limb disabilities
The most important outcomes of using telerehabilitation systems were, in order, "improvement in musculoskeletal functions," “increasing patients' interest and motivation to perform rehabilitation exercises", and "increasing adherence to rehabilitation exercises and greater participation in treatment processes." Table 5 shows the other outcomes. (More information can be found in Additional file 1: Appendix C.)
It should be noted that “Increasing the total exercise time" was the only negative outcome reported in one of the 29 studies included in our study [16].
Discussion
The functions and outcomes of telerehabilitation technology for the upper limbs were investigated in this study. In addition, in this study, we identified different methods for evaluating telerehabilitation. "Evaluation of exercises and musculoskeletal function of the patient by the therapist" was the most widely used function/service provided by telerehabilitation. Three technologies of virtual reality, smart wearables, and robots were used to provide telerehabilitation services. Among the 13 different evaluations of telerehabilitation systems, "Evaluation and measurement of upper limb function" was the most widely used. Researchers reported a variety of outcomes of telerehabilitation systems for upper limb disabilities. These outcomes are described below.
-
Improvement in musculoskeletal functions
One of the most important findings of the studies reviewed in this study was improving musculoskeletal functions through telerehabilitation. When compared to usual and traditional care, these findings highlight the potential for telerehabilitation to be an alternative model of care. As a result, while telerehabilitation may not be superior to traditional models of care, it may provide additional benefits in clinical settings (such as increased access to health care for patients and improved efficiency for health professionals). However, to increase the effectiveness of telerehabilitation in improving musculoskeletal functions, a person-centered approach to treatment should be employed to encourage greater participation in exercise [41]. Different studies [42, 43] suggest that patients prefer individualized, supervised exercise programs with a therapist's opinion. In addition to web-based software, the development of mobile-based telerehabilitation applications can provide patients with personalized and supervised exercise programs and input from therapists [44]. There is evidence that using mobile apps with therapist input, particularly the ability to set and monitor the quality of exercise completion [33], leads to higher adherence rates and thus improves musculoskeletal functions than traditional paper handouts. This success could be attributed to a variety of factors, including the ability of applications to send alerts, motivating messages, or reminders. Furthermore, patients may prefer to access their home exercise programs (HEPs) via a mobile phone or another portable device rather than a paper handout [33]. Patients' adherence, on the other hand, maybe positively affected if they are aware that their therapist can remotely monitor and provide feedback via an application [45].
In a systematic review, Sarfo et al., [46] concluded that telerehabilitation interventions significantly improved motor deficits, higher cortical dysfunction, and people with upper limb. However, Some studies have reported that telerehabilitation systems may not improve upper limb mobility and function in the short term, and the long-term effectiveness of these systems may be apparent to patients [19]. Long-term maintenance of motor gains or improvement in musculoskeletal functions includes continued adherence to exercises (after the end of telerehabilitation) and maintaining motivation in the absence of external factors (e.g., clinician encouragement) [47]. Musculoskeletal functions and upper limb range of motion can be improved in these systems by incorporating games and virtual reality technology [38]. By controlling movement, increasing the number of repetitions of exercises, and motivating patients, video games can improve musculoskeletal function and range of motion [38]. According to these studies, it can be said that the therapeutic effects of these systems are not less than traditional systems, but the effectiveness of these telerehabilitation systems may not be apparent in the short term. On the other hand, with the use of video games based on virtual reality technologies and mobile-based applications, the therapeutic effects of these systems will increase.
-
Increased patients’ interest and motivation to perform rehabilitation exercises
Other findings of our study showed that telerehabilitation will increase patients' interest and motivation to perform therapeutic exercises. Aguilera-Rubio et al. [48] demonstrated that motivation has an effect on motor and functional outcomes in people with orthopedic and neurological disorders. Some of studies [49] show that a lack of motivation is a barrier to physical activity and training following a disability. Sucar et al. [19], also reviewed the Gesture Therapy (GT) telerehabilitation system versus traditional rehabilitation. They concluded that there was a greater motivation and dependence on treatment for patients using GT. They also noted that motivation and long-term rehabilitation exercises are key factors in improving upper limb function. Low levels of motivation have a negative effect on the type and extent of use of rehabilitation exercises [19]. Therefore, motivation factors should be considered in rehabilitation services [40]. Video game exercises are one of the most important reasons for strengthening and motivating participants to do rehabilitation exercises [38, 40]. Visual feedback provided through games increases the patients’ awareness of their progress and increases their motivation and their continuity in treatment. In addition, visual biofeedback (for example, tools like Kinect) promotes higher levels of active participation [38]. Patients who use virtual environment video games are more motivated, rely more on rehabilitative exercises [50, 51], enjoy treatment more, work harder to heal themselves, and ultimately have better upper limb function [19, 52]. Some studies [48, 53] have also shown that VR-based games can provide effective sensory feedback and place subjects in a virtual environment to watch their body’s movements. On the other hand, the virtual and gaming environment should be designed in such a way that the patient has a sense of presence in a real environment. Considering other elements such as the background, avatar design, and the scene’s realism are very important in designing virtual reality and game environments [47]. Personalization of rehabilitation programs and games by actively involving the patient in setting rehabilitation goals may thus directly increase the patient’s sense of independence and in turn, their motivation, as suggested by Jansson et al. [54].
-
Increased adherence to rehabilitation exercises and greater participation in treatment processes
Of the 29 studies, seven studies showed that telerehabilitation increased adherence to rehabilitation exercises and increased patient participation in their treatment processes. The results of the study by Lambert et al. [33] showed that participants who received their rehabilitation exercises through telerehabilitation were more adherent to treatment and their performances were improved more than participants who received paper handouts. Cramer et al., [55] also examined the effectiveness of home-based telerehabilitation versus traditional in-clinic for adults with stroke. The patients in the telerehabilitation group had 35.4 (98.3%) of the 36 assigned treatments, and the patients in the clinical group had 33.6 (93.3%) of the 36 assigned treatments. At the same time, poor adherence to home exercise programs and treatment plans may affect treatment outcomes and symptom recurrence [56]. Non-adherence to a home exercise program may be due to patient-related reasons, including pain, lack of motivation, poor self-efficacy, limited exercise experience, and reduced social support. Furthermore, patients may not immediately recognize the benefits of a home exercise program [33]. Some authors [57, 58] have suggested that adherence to a home exercise program could be enhanced if therapists increase face-to-face time with patients, but this is costly and rarely feasible given limited resources. Therefore, the other effective factors in increasing adherence should be better understood and strategies should be provided to stimulate long-run exercises. Palazzo et al., [56] presented the physical exercise program (number, power, complexity, and weight of exercising), health care trip (breakdown between monitored meetings and home practice, lack of follow-up, and problems contacting care providers), diseased person representations (unwellness and representation of exercise, discouragement, natural depression, and lack of motivation), and the environment (attitudes of others, exercise planning problem) as the most important barriers to adherence to rehabilitation exercises that must be considered when designing and implementing telerehabilitation systems. Apart from environmental and exercise-related factors, various aspects of technology will also affect adherence to treatment and rehabilitation exercises. Qiu et al. [40] believe that adherence to rehabilitation provided through technology has a complex structure because technical problems can be a major obstacle to increase adherence. Therefore, in designing technology, factors related to clinical-demographic characteristics of patients such as age, housing state, and level of computer expertise or degree of damage should be considered. In addition, an algorithm program operating in the background can dynamically change the difficulty level of games based on people's performance to limit frustration and increase their motivation [40]. Also, adherence to treatment processes can be increased if the system is easy for patients to use and has an attractive user interface [59]. Dodakian and et al. [59], believed that the best rehabilitation-treatment program is of little help to patients if they do not adhere to it, so telerehabilitation programs were designed to increase compliance. A key feature of this is the use of virtual reality gaming to drive therapy, a known way of maximizing desirability and accessibility and promoting patient engagement.
-
Improved user satisfaction
In this review, we observed that telerehabilitation can improve user satisfaction. In the study by Lambert et al. [33], approximately 90% of the people in the intervention group (who received their rehabilitation exercises through the website) expressed their satisfaction with healthcare service-support and healthcare service-delivery of more than 95%. In addition, a number of studies [60,61,62] found that telerehabilitation services are useful and effective both for children and adults with disabilities, and therapists have also reported high levels of satisfaction and acceptance of telerehabilitation services. Based on the findings of these studies and the study of Tousignant et al., [63] it can be said that satisfaction is an important indicator of the degree of efficiency and effectiveness, and its high level increases patient motivation and improves compliance with treatment. Satisfaction conceptualization defines both one's legitimate expectation of having demands met and one's perception of the actual experience [64]. Dislike some disagreements [65, 66], satisfaction is often used as one of the important factors in healthcare quality, as it can both influence adherence to treatment plans and improve clinical outcomes [67]. However, the concept of satisfaction is complex and is related to different aspects of healthcare such as accessibility of resources, qualification of healthcare professionals, the patient-therapist relationship, and the overall care organization [64].
Moreover, we believe that patient satisfaction with a health technology will not be easy; for high satisfaction, a number of factors must always be considered. Patients’trust in telerehabilitation, quality of the patient-therapist relationship, quality of rehabilitation sessions, quality and performance of the technological platform, and user-friendliness of equipment are among the factors that can affect patients’ satisfaction with telerehabilitation systems [63, 68]. Reducing disconnection problems, ease of use of telerehabilitation, absence of adverse events, adequacy of audio/video quality, and increased adherence to exercise training can also have a significant impact on improving patient satisfaction [69]. If the patient's satisfaction with a system such as telerehabilitation systems increases, its continuity and use increases, and the patient's' adherence to treatment processes and rehabilitation exercises will increase, resulting in the development of the system and its acceptance by users will be easy. Therefore, patient satisfaction with the designed systems should always be considered a basic principle of system development processes.
-
No adverse effects on patients
The studies examined also pointed out that telerehabilitation systems have no negative effect on patients. Qiu et al. [40] used the Virtual Rehabilitation System (HoVRS) to rehabilitate 15 patients with stroke. The results of this study showed that after 13.5 h of using the system, all 15 patients completed the rehabilitation process without any side effects. Results of a systematic review by Vieira et al. [70] showed that telerehabilitation improved functional capacity, performance, and physical factors of quality of life, and indeed significantly reduced side effects. In some other studies, Kinect2Scratch game-based training and therapist-based training were compared [38]. The results indicated that Kinect2Scratch game-based training did not cause any serious side effects for patients with upper extremity disabilities. Also, none of the patients needed further treatment [38]. Although in our study, studies reported no exercise-related adverse events in the telerehabilitation groups, other studies reported similar adverse events in the telerehabilitation system. Adverse events in a minority of participants included new-onset arrhythmias (including supraventricular contractions, atrial fibrillation, and premature ventricular contractions), hypertension, angina [71, 72], and worsening of chronic obstructive pulmonary disease (COPD) [73]. This may indicate that more monitoring is used at home than exercise. On the other hand, patients who experience side effects, in addition to their reluctance to use the technology, discontinue treatment or receive lower doses, both of which lead to an increase in the overall treatment dose [74]. Therefore, telerehabilitation systems should be designed in such a way that they can minimize side effects for patients and ensure the absence of side effects for patients before using the system so that they can use these systems safely.
-
Telerehabilitation systems feasibility for remote monitoring and control of patients
According to the findings of the studies, we found that the use of telerehabilitation systems for remote monitoring and control of patients with upper limb disabilities is feasible. Some studies [55, 59] have suggested that telerehabilitation for patients with stroke and upper limb disabilities are feasible and as effective as in-person therapy. Reinkensmeyer et al. [14] analyzed data from home-based use related to a stroke patient. The results of this analysis demonstrate that it is possible, useful, and effective to use the system to direct a medical care platform, mechanically assist movement, and track progress in movement power. This is while evidence demonstrates that the feasibility of telerehabilitation systems is not easy; Factors such as costs associated with purchasing, maintaining and insuring hardware, as well as logistics related to equipment provision, monitoring, and return, can affect the viability of a telerehabilitation system [75]. Computer training is another factor that can affect the feasibility of telerehabilitation systems [75]. Evidence indicates that computer training can significantly reduce computer anxiety while also increasing computer interest and performance in older adults [76]. This means that providing education and training to patients on relevant technologies can increase the use of telerehabilitation systems. In addition, access to computers at home and the age of individuals are both strongly related to individuals' feelings about the acceptance and feasibility of technology and telerehabilitation [75]. Access to a computer at home seems to be one of the strongest predictors of feasibility and acceptance. The study by Nelson et al. [75] showed that patients with access to computers were more interested in exercising learning, more confident in the technology, less likely to avoid technology, and more likely to engage and feel safe and secure in telerehabilitation system. Furthermore, this study showed that patients over the age of 65 were less likely to use a telerehabilitation system compared to patients under the age of 66 [75]. Their reluctance to use telerehabilitation systems is more likely because they are more worried, concerned, and less confident than their younger peers. As a result, in order for telerehabilitation systems to be feasible, this age group should not be excluded from consideration. To maximize the uptake of telerehabilitation systems, healthcare providers looking to implement telerehabilitation and the designers of these systems should consider patients' age, access to technology at home, training and education requirements, and technology preferences.
-
Reduced or relieved pain
In our review, some studies showed that telerehabilitation had an effect on reducing or relieving pain. The results of the study by Van Straaten et al [29] showed that after using the telerehabilitation system, the pain of patients decreased, the function of different parts of their upper limbs improved and the isometric power evaluation of the anterior serratus and scapular retractors increased. In the study by Tousignant et al. [27], the pain was assessed using the SF-MPQ test. The results of this study showed that the pain diminished essentially between face-to-face evaluations before (T1) and immediately after (T2) as demonstrated by the SF-MPQ score and the VAS. The illustrated pain reduction was more noteworthy than the negligible clinically significant contrast. In the study of Sucar et al. [19], the effect of using telerehabilitation and conventional occupational therapy systems in reducing pressure and pain was reported to be equal. In other studies [77, 78], aggressive rehabilitation programs have been shown to improve joint function and reduce pain, increase strength, walking speed, and self-efficacy, and reduce the risk of other chronic conditions. Both home-based exercise and aerobic walking reduce pain and disability [79].
But what is important is that we know that the pain does not reduce or alleviate itself by using telerehabilitation systems and that a number of indicators alongside these systems must always be considered. Osteras et al., [80] believed that high-repetition doses reduced pain more than lower doses. As a result, when considering the dose aspect of the dose-response relationship for telerehabilitation, we must consider items such as "number and duration of repetitions in one set," "number and duration of sets of an exercise," "number and duration of exercises in one treatment," "number and duration of treatments during a week (s)," and "total number and duration of treatments" [80]. While all of these indicators affect patients' treatment preferences, therapist contact mode proved a key driver of preference for chronic pain rehabilitation, with patients who have a high preference for face-to-face contact with some therapists. Treatment scenarios that include some remote therapist video communication are usually preferred over scenarios that only include remote video communication. This decision could be influenced by the psychosocial nature of chronic pain treatment [81]. In the treatment of chronic pain especially, patient-therapist communication plays an important role, as pain should be defined as a subjective phenomenon in the discussion and both empathy and emotional support are considered necessary [82]. Although touch is not essential to convey empathy and create a therapeutic bond per se [83], a qualitative study in patients with chronic pain has shown that some patients associated remote patient-therapist counseling with a loss of personal attention [84]. Therefore, it seems that in order to allow patients to recover faster and increase their satisfaction and use of telerehabilitation systems, the two rules of patient-therapist communication and empathy and emotional support should always be considered in these systems.
-
Reliability of telerehabilitation systems
According to our other findings, some of the included studies proved the reliability of telerehabilitation in the treatment of patients. By conducting a series of clinical trials on three patients with upper limb disability, Song et al. [32] demonstrated the efficiency and good reliability of telerehabilitation techniques in movement therapy at home or in nursing homes. movement Also, this technology is able to improve the efficiency of rehabilitation training and solve the problems of lack of therapists [32]. Furthermore, Sampson et al. [24] assessed the BUiLT + VR system on hemiparesis patients with upper limb disability and discovered that treatment with this system was reliable and could be safely prescribed. The system can also measure isometric power, FMA-UE, and IMI through its positive trend. A prerequisite for reliability is that we evaluate a system to ensure that it performs its intended function over a period of runtime without any failure [85]. Some studies have shown that telerehabilitation-based intervention is somewhat related to concurrent validity and reliability of the outcome standards. So, evaluating and making the concurrent validity and reliability of outcome standards via telerehabilitation prior to adoption in the scheduled clinical practice has been considered imperative [86].On the other hand, to maximize reliability, we must minimize the faults of the systems. Although the definition of failure is different for different systems and different states, a failure is always a part of the system that exists and can be eliminated by correcting the wrong part of the system [87]. Reliability is defined as failure-free operation over time. This definition in health care is linked to several of the IOM's goals for the healthcare system, including "effectiveness (where the failure can result from not applying evidence)," "timeliness (where the failure results from not taking action in the required time")," and "patient-centeredness (where failure results from not complying with patients' values and preferences)" [88]. Therefore, before a rehabilitation system is provided to patients, its reliability must be ensured from different dimensions, leading problems must be prevented, and various reasons or factors that may affect reliability must be considered at all times. The major factors that affect reliability are improper maintenance or installation, operating statuses including the working environment, the operators' effects, the operative duty referring to the ranges of operating stress imposed, the education of the staff involved in use and maintenance, and a lack of adequate supervision [89].
-
Improved quality of life
Other findings of our study showed that telerehabilitation could improve the quality of life of patients with upper limb. These findings approve the results of two single-center studies [90, 91], which showed that telerehabilitation significantly improved overall quality of life indices. The results of the study by Cikajlo et al. [35] indicated that telerehabilitation both improved UL function in people with Parkinson's disease and improved the quality of life of these patients. Some studies have also shown that short-term improvements in motor function (BBT, UPDRS III) and daily activities lead to improved cognitive function and quality of life in participants with PD without changes in diet, medication, or lifestyle. After analyzing the data obtained from the Stroke Impact Scale (SIS) questionnaire and patient interviews in the study of Pickett et al. [17], it is proved that the use of the Tele-CIMT rehabilitation system reduced patients’ travel to rehabilitation centers, reduced patients' feelings of isolation and improved their quality of life. It is important for us to know that quality of life is not just a dimension that can be easily improved and enhanced. Quality of life, defined as the quality of life affected by the disease, is a multidimensional measure that includes physical, social, and emotional health [92]. Therefore, these three dimensions should be considered when using telerehabilitation. Also, Some studies have shown that upper limb function, mental health, and participation in leisure activities are key variables that affect and enhance the quality of life [92]. Therefore, if we use special interventions such as game-based virtual reality and robot-assisted therapy along with telerehabilitation, the upper limb function, mental health, and participation in leisure activities can be improved [92, 93]. Game-based virtual reality and robot-assisted therapy technologies can increase patients' motivation and desire to perform therapeutic exercises [32, 94, 95], perform repetitive and long exercises easily [96], reduce the time required to perform therapeutic exercises [97], increase the patient's independence in performing therapeutic exercises [97,98,99], and increase adherence to rehabilitation exercises [100]. Finally, these technologies can help improve the quality of life of patients with upper extremity disabilities. Levy et al. [101] evaluated functional outcomes, health-related quality of life (HRQoL), and satisfaction in a group of veterans through a home video-based telerehabilitation program. Assessments showed significant improvements in functional independence, Montreal Cognitive Assessment (MOCA), two-minute walk test, Veterans RAND 12-ItemHealth Survey (VR-12), and HRQoL. In addition to providing rehabilitation exercises through the telerehabilitation system, the therapist should be able to provide teleconsultation services to patients to improve the mental health status of the patient. Larson et al. [102] also believe that increasing patients' access to symptom management and emotional support services may lead to patients taking a more active role in their healthcare and could improve patient outcomes, including overall quality of life. Larson et al [102] Moreover, the patient’s sensation of control may be strengthened if the patient is invited to participate in setting realistic goals for outcomes in rehabilitation. This suggests that working with patients to set goals for recovery and self-care may improve adherence to these goals over time and improve quality of life. Failure to adhere to lifestyle changes and desired goals at the end of a rehabilitation program is a well-known problem in rehabilitation [103]. Another important issue worth pointing out is that the cultural and religious factors could significantly affect the level of quality of life, so both factors must be considered in telerehabilitation systems to improve the quality of life [104].
“Increasing the total exercise time” was the only negative outcome identified in our study [16]. This outcome is discussed below.
-
Increasing the total exercise time
A study by Kuttuva et al. [16] showed that the use of telerehabilitation increased total exercise time (up 28%). In this study, a 56-year-old male with right hemi-paresis underwent telerehabilitation for 3 days/week for 12 sessions. It seems that if this study had been performed with larger sample size and longer intervention time, another result might have been obtained. Tabak et al. [105] argued that if sample size and intervention time were not sufficient in a telerehabilitation study, the main effect of the intervention might not be properly apparent. For example, they believed that four weeks of intervention and 30 participants were not enough to estimate the duration of exercise, establish changes in activity behavior, investigate the treatment effects, or detect exacerbations. Therefore, future studies are proposed with a larger sample size and long intervention time, which analyze treatment effects and compliance on both the short- and long-term. The effects of the telerehabilitation systems maybe be various in the long-term follow-up [106]. As a result, evidence of health benefits from long-term patient follow-up is significant enough to be included in the total exercise increase time with telerehabilitation.
Limitations of the study
There were a few limitations in this review. In this study, only studies in English were reviewed; if a study was published in a language other than English, we did not review it. However, the present study is the first scoping review to examine the outcomes of telerehabilitation for upper limb disabilities; therefore, the results of this study can serve as a basis for further studies. Also, to find related studies, we searched three scientific databases, Scopus, PubMed, and Web of Science. As a result, future studies should be conducted on a larger number of databases in order to obtain more comprehensive results. Furthermore, we did not perform a critical appraisal of individual sources of evidence in this study; this limitation should be considered in future studies.
Conclusion
According to this review, telerehabilitation technology is a valuable treatment option in the recovery process for upper limb disabilities, and it has the potential to become a quality rehabilitation services delivery model. Furthermore, this technology is a viable alternative rehabilitation approach for upper limb disabilities, as well as a potentially effective tool for increasing positive behavioral change in upper limb disabilities toward a more physically active lifestyle. It should also be noted that the different aspects of telerehabilitation technology identified in this study can be used to design and implement telerehabilitation systems for other disabilities.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- UL:
-
Upper limb
- CIMT:
-
Clinic-based Constraint-Induced Movement Therapy
- TBI:
-
Traumatic Brain Injury
- SCI:
-
Spinal Cord Injury
- CVA:
-
Cerebrovascular Accident
- BUiLT:
-
Bilateral Upper Limb Coach
- SSc:
-
Systemic Sclerosis
- ABI:
-
Acquired Brain Injury
- PD:
-
Parkinson’s Disease
- VR:
-
Virtual Rehabilitation
- MCITE:
-
Modified Constraint-Induced Therapy Extension
- HoVRS:
-
Home based Virtual Rehabilitation System
- FMA-UE:
-
Fugl-Meyer Upper Extremity score
- WMFT:
-
Wolf Motor Function
- MAL:
-
Motor Activity Log
- ROM:
-
Range Of Motion
- BBT:
-
Box and Block Test
- PDQ-39:
-
Parkinson’s Disease Questionnaire
- WUSPI:
-
Wheelchair User’s Shoulder Pain Index
- IMI:
-
Intrinsic Motivation Inventory
- SRQ:
-
Shoulder Rating Questionnaire
- UPDRS:
-
Unified Parkinson’s Disease Rating Scale
- SIS:
-
Stroke Impact Scale
- DASH:
-
Disabilities of Arm, Shoulder, and Hand
- QOM:
-
Point Quality of Movement
- DXA:
-
Dual energy X-ray Absorptiometry
- pQCT:
-
Peripheral quantitative Computed Tomography
- CT:
-
Computed Tomography
- SF-MPQ:
-
Short-Form McGill Pain Questionnaire
- SUS:
-
System Usability Scale
- FIM:
-
Functional Independence Measure
- ReWiiRe:
-
Wii Rehabilitation
- HEPs:
-
Home Exercise Programs
- HoVRS:
-
Virtual Rehabilitation System
- HAMIS:
-
Hand Mobility in Scleroderma
- FIHOA:
-
Functional Index of Hand Osteoarthritis
- JTHFT:
-
Jebsen-Taylor Hand Function Test
- AAUT:
-
Actual Amount of Use Test
- 9HPT:
-
Nine-Hole Peg Hole Test
- SIS:
-
Stroke Impact Scale
- HRQoL:
-
Health Related Quality of Life
- MOCA:
-
Montreal Cognitive Assessment
References
Almomani F, Alghwiri AA, Alghadir AH, Al-Momani A, Iqbal A. Prevalence of upper limb pain and disability and its correlates with demographic and personal factors. J Pain Res. 2019;12:2691–700.
Hosseiniravandi M, Kahlaee AH, Karim H, Ghamkhar L, Safdari R. Home-based telerehabilitation software systems for remote supervising: a systematic review. Int J Technol Assess Health Care. 2020;36(2):113–25.
Langan J, Delave K, Phillips L, Pangilinan P, Brown SH. Home-based telerehabilitation shows improved upper limb function in adults with chronic stroke: a pilot study. J Rehabil Med. 2013;45(2):217–20.
Rogante M, Kairy D, Giacomozzi C, Grigioni M. A quality assessment of systematic reviews on telerehabilitation: what does the evidence tell us? Annali dell’Istituto superiore di sanita. 2015;51(1):11–8.
Dias JF, Oliveira VC, Borges PRT, Dutra FCMS, Mancini MC, Kirkwood RN, Resende RA, Sampaio RF. Effectiveness of exercises by telerehabilitation on pain, physical function and quality of life in people with physical disabilities: a systematic review of randomised controlled trials with GRADE recommendations. Br J Sports Med. 2021;55(3):155–62.
Agostini M, Moja L, Banzi R, Pistotti V, Tonin P, Venneri A, Turolla A. Telerehabilitation and recovery of motor function: a systematic review and meta-analysis. J Telemed Telecare. 2015;21(4):202–13.
Kairy D, Lehoux P, Vincent C, Visintin M. A systematic review of clinical outcomes, clinical process, healthcare utilization and costs associated with telerehabilitation. Disabil Rehabil. 2009;31(6):427–47.
Munn Z, Peters MD, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):1–7.
PRISMA for Scoping Reviews [https://prisma-statement.org/Extensions/ScopingReviews]
Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implementation Sci. 2010;5(69):1–10.
Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Murrell JE, Pisegna JL, Juckett LA. Implementation strategies and outcomes for occupational therapy in adult stroke rehabilitation: a scoping review. Implementation Sci. 2021;16(1):1–26.
Piron L, Tonin P, Trivello E, Battistin L, Dam M. Motor tele-rehabilitation in post-stroke patients. Med Inform Internet Med. 2004;29(2):119–25.
Reinkensmeyer DJ, Pang CT, Nessler JA, Painter CC. Web-based telerehabilitation for the upper extremity after stroke. IEEE Trans Neural Syst Rehabil Eng. 2002;10(2):102–8.
Feng X, Winters JM. UniTherapy: A computer-assisted motivating neurorehabilitation platform for teleassessment and remote therapy. In: 2005 Ieee 9th International Conference on Rehabilitation Robotics. IEEE; 2005 June 28 - July 1, Chicago, IL, USA;2005:349–52.
Kuttuva M, Boian R, Merians A, Burdea G, Bouzit M, Lewis J, Fensterheim D. The Rutgers Arm, a rehabilitation system in virtual reality: a pilot study. Cycberpsychol Behav. 2006;9(2):148–51.
Pickett TC, Davis SB, Fritz SL, Malcolm MP, Ketterson TU, Light KE, Glueckauf RL. Telehealth and Constraint-Induced Movement Therapy (CIMT): An Intensive Case Study Approach. Clin Gerontol. 2007;31(1):5–20.
Page SJ, Levine P. Modified constraint-induced therapy extension: using remote technologies to improve function. Arch Phys Med Rehabil. 2007;88(7):922–7.
Sucar LE, Leder R, Hernandez J, Sanchez I, Azcarate G. Clinical Evaluation of a Low Cost Alternative for Stroke Rehabilitation. In: 2009 Ieee 11th International Conference on Rehabilitation Robotics, Vols 1 and 2. IEEE; 2009: 1006-+.
Sucar LE, Luis R, Leder R, Hernandez J, Sanchez I. Gesture Therapy: A Vision-Based System for Upper Extremity Stroke Rehabilitation. In: 2010 Annual International Conference of the Ieee Engineering in Medicine and Biology Society. IEEE; 2010: 3690–3693.
Golomb MR, McDonald BC, Warden SJ, Yonkman J, Saykin AJ, Shirley B, Huber M, Rabin B, Abdelbaky M, Nwosu ME, et al. In-home virtual reality videogame telerehabilitation in adolescents with hemiplegic cerebral palsy. Arch Phys Med Rehabil. 2010;91(1):1-8.e1.
Golomb MR, Warden SJ, Fess E, Rabin B, Yonkman J, Shirley B, Burdea GC. Maintained hand function and forearm bone health 14 months after an in-home virtual-reality videogame hand telerehabilitation intervention in an adolescent with hemiplegic cerebral palsy. J Child Neurol. 2011;26(3):389–93.
Aung YM, Al-Jumaily A. AR based Upper Limb Rehabilitation System. In: Desai JP, Jay LPS, Zollo L, editors. 2012 4th Ieee Ras & Embs International Conference on Biomedical Robotics and Biomechatronics. 2012. p. 213–8.
Sampson M, Shau YW, King MJ. Bilateral upper limb trainer with virtual reality for post-stroke rehabilitation: case series report. Disabil Rehabil Assist Technol. 2012;7(1):55–62.
Piga M, Tradori I, Pani D, Barabino G, Dessì A, Raffo L, Mathieu A. Telemedicine applied to kinesiotherapy for hand dysfunction in patients with systemic sclerosis and rheumatoid arthritis: recovery of movement and telemonitoring technology. J Rheumatol. 2014;41(7):1324–33.
Langan J, Kern KL, Hurvitz EA, Brown SH. Upper-limb position sense deficits in adults with cerebral palsy. Am J Phys Med Rehabil. 2014;93(9):774–81.
Tousignant M, Giguère AM, Morin M, Pelletier J, Sheehy A, Cabana F. In-home telerehabilitation for proximal humerus fractures: a pilot study. Int J Telerehabil. 2014;6(2):31–7.
Kato N, Tanaka T, Sugihara S, Shimizu K. Development and evaluation of a new telerehabilitation system based on VR technology using multisensory feedback for patients with stroke. J Phys Ther Sci. 2015;27(10):3185–90.
Van Straaten MG, Cloud BA, Morrow MM, Ludewig PM, Zhao KD. Effectiveness of home exercise on pain, function, and strength of manual wheelchair users with spinal cord injury: a high-dose shoulder program with telerehabilitation. Arch Phys Med Rehabil. 2014;95(10):1810-1817.e1812.
Cabana F, Pagé C, Svotelis A, Langlois-Michaud S, Tousignant M. Is an in-home telerehabilitation program for people with proximal humerus fracture as effective as a conventional face-to face rehabilitation program? A study protocol for a noninferiority randomized clinical trial. BMC Sports Sci Med Rehabil. 2016;8(1):27.
Tsekleves E, Paraskevopoulos IT, Warland A, Kilbride C. Development and preliminary evaluation of a novel low cost VR-based upper limb stroke rehabilitation platform using Wii technology. Disabil Rehabil Assist Technol. 2016;11(5):413–22.
Song A, Wu C, Ni D, Li H, Qin H. One-Therapist to Three-Patient Telerehabilitation Robot System for the Upper Limb after Stroke. Int J Soc Robot. 2016;8(2):319–29.
Lambert TE, Harvey LA, Avdalis C, Chen LW, Jeyalingam S, Pratt CA, Tatum HJ, Bowden JL, Lucas BR. An app with remote support achieves better adherence to home exercise programs than paper handouts in people with musculoskeletal conditions: a randomised trial. J Physiother. 2017;63(3):161–7.
Kizony R, Weiss PL, Harel S, Feldman Y, Obuhov A, Zeilig G, Shani M. Tele-rehabilitation service delivery journey from prototype to robust in-home use. Disabil Rehabil. 2017;39(15):1532–40.
Cikajlo I, Hukić A, Dolinšek I, Zajc D, Vesel M, Krizmanič T, Blažica B, Biasizzo A, Novak F, Peterlin Potisk K. Can telerehabilitation games lead to functional improvement of upper extremities in individuals with Parkinson’s disease? Int J Rehabil Res. 2018;41(3):230–8.
Kim WS, Cho S, Park SH, Lee JY, Kwon S, Paik NJ. A low cost kinect-based virtual rehabilitation system for inpatient rehabilitation of the upper limb in patients with subacute stroke A randomized, double-blind, sham-controlled pilot trial. Medicine. 2018;97(25):e11173.
Cabrera-Martos I, Ortiz-Rubio A, Torres-Sánchez I, López-López L, Rodríguez-Torres J, Carmen Valenza M. Agreement Between Face-to-Face and Tele-assessment of Upper Limb Functioning in Patients with Parkinson Disease. PM R. 2019;11(6):590–6.
Hung JW, Chou CX, Chang YJ, Wu CY, Chang KC, Wu WC, Howell S. Comparison of Kinect2Scratch game-based training and therapist-based training for the improvement of upper extremity functions of patients with chronic stroke: a randomized controlled single-blinded trial. Eur J Phys Rehabil Med. 2019;55(5):542–50.
Agyeman MO, Al-Mahmood A. Design and implementation of a wearable device for motivating patients with upper and/or lower limb disability via gaming and home rehabilitation. In: 2019 4th International Conference on Fog and Mobile Edge Computing, FMEC 2019. 2019. p. 247–52.
Qiu Q, Cronce A, Patel J, Fluet GG, Mont AJ, Merians AS, Adamovich SV. Development of the Home based Virtual Rehabilitation System (HoVRS) to remotely deliver an intense and customized upper extremity training. J Neuroeng Rehabil. 2020;17(1):155.
Macedo LG, Bostick GP, Maher CG. Exercise for prevention of recurrences of nonspecific low back pain. Phys Ther. 2013;93(12):1587–91.
Saner J, Bergman EM, de Bie RA, Sieben JM. Low back pain patients’ perspectives on long-term adherence to home-based exercise programmes in physiotherapy. Musculoskeletal Sci Pract. 2018;38:77–82.
Bennell KL, Marshall CJ, Dobson F, Kasza J, Lonsdale C, Hinman RS. Does a Web-Based Exercise Programming System Improve Home Exercise Adherence for People With Musculoskeletal Conditions?: A Randomized Controlled Trial. Am J Phys Med Rehabil. 2019;98(10):850–8.
Agnew JMR, Hanratty CE, McVeigh JG, Nugent C, Kerr DP. An Investigation Into the Use of mHealth in Musculoskeletal Physiotherapy: Scoping Review. JMIR Rehabil Assist Technol. 2022;9(1):e33609–e33609.
Jordan JL, Holden MA, Mason EE, Foster NE. Interventions to improve adherence to exercise for chronic musculoskeletal pain in adults. Cochrane Database Syst Rev. 2010;2010(1):CD005956–CD005956.
Sarfo FS, Ulasavets U, Opare-Sem OK, Ovbiagele B. Tele-Rehabilitation after Stroke: An Updated Systematic Review of the Literature. J Stroke Cerebrovasc Dis. 2018;27(9):2306–18.
Allegue DR, Kairy D, Higgins J, Archambault PS, Michaud F, Miller WC, Sweet SN, Tousignant M. A Personalized Home-Based Rehabilitation Program Using Exergames Combined With a Telerehabilitation App in a Chronic Stroke Survivor: Mixed Methods Case Study. JMIR serious games. 2021;9(3):e26153–e26153.
Aguilera-Rubio Á, Cuesta-Gómez A, Mallo-López A, Jardón-Huete A, Oña-Simbaña ED, Alguacil-Diego IM. Feasibility and Efficacy of a Virtual Reality Game-Based Upper Extremity Motor Function Rehabilitation Therapy in Patients with Chronic Stroke: A Pilot Study. Int J Environ Res Public Health. 2022;19(6):3381.
Montoya D, Barria P, Cifuentes CA, Aycardi LF, Morís A, Aguilar R, Azorín JM, Múnera M. Biomechanical Assessment of Post-Stroke Patients’ Upper Limb before and after Rehabilitation Therapy Based on FES and VR. Sensors (Basel). 2022;22(7):2693.
Hatem SM, Saussez G, Della Faille M, Prist V, Zhang X, Dispa D, Bleyenheuft Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front Hum Neurosci. 2016;10:442.
Mihelj M, Novak D, Milavec M, Ziherl J, Olenšek A, Munih M. Virtual rehabilitation environment using principles of intrinsic motivation and game design. Presence Teleoperators Virtual Environ. 2012;21(1):1–15.
Flores E, Tobon G, Cavallaro E, Perry JC, Keller T. Improving patient motivation in game development for motor deficit rehabilitation. In: Proceedings of the 2008 international conference on advances in computer entertainment technology: 2008. 2018. p. 381–4.
Oujamaa L, Relave I, Froger J, Mottet D, Pelissier JY. Rehabilitation of arm function after stroke. Literature review. Ann Phys Rehabil Med. 2009;52(3):269–93.
Jansson I, Fors A, Ekman I, Ulin K. Documentation of person-centred health plans for patients with acute coronary syndrome. Eur J Cardiovasc Nurs. 2018;17(2):114–22.
Cramer SC, Dodakian L, Le V, See J, Augsburger R, McKenzie A, Zhou RJ, Chiu NL, Heckhausen J, Cassidy JM, et al. Efficacy of Home-Based Telerehabilitation vs In-Clinic Therapy for Adults After Stroke: A Randomized Clinical Trial. JAMA Neurol. 2019;76(9):1079–87.
Palazzo C, Klinger E, Dorner V, Kadri A, Thierry O, Boumenir Y, Martin W, Poiraudeau S, Ville I. Barriers to home-based exercise program adherence with chronic low back pain: Patient expectations regarding new technologies. Ann Phys Rehabil Med. 2016;59(2):107–13.
Sluijs EM, Kok GJ, Van der Zee J. Correlates of exercise compliance in physical therapy. Phys Ther. 1993;73(11):771–82.
Reilly K, Lovejoy B, Williams R, Roth H. Differences between Supervised and Independent Strength and Conditioning Program with Chronic Low Back Syndromes. J Occup Med. 1989;31:547–50.
Dodakian L, McKenzie AL, Le V, See J, Pearson-Fuhrhop K, Burke Quinlan E, Zhou RJ, Augsberger R, Tran XA, Friedman N, et al. A Home-Based Telerehabilitation Program for Patients With Stroke. Neurorehabil Neural Repair. 2017;31(10–11):923–33.
Caprì T, Fabio RA, Iannizzotto G, Nucita A. The TCTRS Project: A Holistic Approach for Telerehabilitation in Rett Syndrome. 2020;9(3):491–9.
Golomb MR, McDonald BC, Warden SJ, Yonkman J, Saykin AJ, Shirley B, Huber M, Rabin B, AbdelBaky M, Nwosu M, et al. In-home virtual reality videogame telerehabilitation in adolescents with hemiplegic cerebral palsy. Arch Phys Med Rehabil. 2010;91(1):1–81.
Huber M, Rabin B, Docan C, Burdea G, Nwosu ME, Abdelbaky M, Golomb MR: PlayStation 3-based tele-rehabilitation for children with hemiplegia. In: 2008 Virtual Rehabilitation: 2008: IEEE; 2008: 105–112.
Tousignant M, Boissy P, Moffet H, Corriveau H, Cabana F, Marquis F, Simard J. Patients’ satisfaction of healthcare services and perception with in-home telerehabilitation and physiotherapists’ satisfaction toward technology for post-knee arthroplasty: an embedded study in a randomized trial. Telemed J E Health. 2011;17(5):376–82.
Moffet H, Tousignant M, Nadeau S, Mérette C, Boissy P, Corriveau H, Marquis F, Cabana F, Belzile ÉL, Ranger PJT, et al. Patient satisfaction with in-home telerehabilitation after total knee arthroplasty: results from a randomized controlled trial. Telemed J E Health. 2017;23(2):80–7.
Fenton JJ, Jerant AF, Bertakis KD, Franks P. The cost of satisfaction: a national study of patient satisfaction, health care utilization, expenditures, and mortality. Arch Intern Med. 2012;172(5):405–11.
Chang JT, Hays RD, Shekelle PG, MacLean CH, Solomon DH, Reuben DB, Roth CP, Kamberg CJ, Adams J. Young RT Patients’ global ratings of their health care are not associated with the technical quality of their care. Ann Intern Med. 2006;144(9):665–72.
Shirley ED, Sanders JO. Patient satisfaction: implications and predictors of success. J Bone Joint Surg Am. 2013;95(10):e69.
Russell TG, Buttrum P, Wootton R, Jull GA. Rehabilitation after total knee replacement via low-bandwidth telemedicine: the patient and therapist experience. J Telemed Telecare. 2004;10(1_suppl):85–7.
Marquis N, Larivée P, Saey D, Dubois M-F, Tousignant MJ. In-home pulmonary telerehabilitation for patients with chronic obstructive pulmonary disease: a pre-experimental study on effectiveness, satisfaction, and adherence. Telemed J E Health. 2015;21(11):870–9.
Vieira AGdS, Pinto ACPN, Garcia BMSP, Eid RAC, Mól CG, Nawa RK. Telerehabilitation improves physical function and reduces dyspnoea in people with COVID-19 and post-COVID-19 conditions: a systematic review. J physiotherapy. 2022;68(2):90–8.
Sparks K, Shaw D, Eddy D, Hanigosky P, Vantrese J. Alternatives for cardiac rehabilitation patients unable to return to a hospital-based program. Heart Lung. 1993;22(4):298–303.
Squires RW, Miller TD, Harn T, Micheels TA, Palma TA. Transtelephonic electrocardiographic monitoring of cardiac rehabilitation exercise sessions in coronary artery disease. Am J Cardiol. 1991;67(11):962–4.
Maltais F, Bourbeau J, Shapiro S, Lacasse Y, Perrault H, Baltzan M, Hernandez P, Rouleau M, Julien M, Parenteau SJAoim: Effects of home-based pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: a randomized trial. 2008;149(12):869–78.
Grutters JP, Govers T, Nijboer J, Tummers M, Van Der Wilt GJ, Rovers MM. Problems and promises of health technologies: the role of early health economic modeling. Int J Health Policy Manag. 2019;8(10):575.
Nelson MJ, Crossley KM, Bourke MG, Russell TG. Telerehabilitation Feasibility in Total Joint Replacement. Int J Telerehabil. 2017;9(2):31–8.
Xie B. Bugg JM Public library computer training for older adults to access high-quality Internet health information. Libr Inf Sci Res. 2009;31(3):155–62.
Foley A, Halbert J, Hewitt T, Crotty M. Does hydrotherapy improve strength and physical function in patients with osteoarthritis–a randomised controlled trial comparing a gym based and a hydrotherapy based strengthening programme. Ann Rheum Dis. 2003;62(12):1162–7.
van Dulmen S, Sluijs E, van Dijk L, de Ridder D, Heerdink R, Bensing J. Patient adherence to medical treatment: a review of reviews. BMC Health Serv Res. 2007;7:55.
Roddy E, Zhang W, Doherty M. Aerobic walking or strengthening exercise for osteoarthritis of the knee? A systematic review. Ann Rheum Dis. 2005;64(4):544–8.
Østerås H, Torstensen TA, Østerås B. High-dosage medical exercise therapy in patients with long-term subacromial shoulder pain: a randomized controlled trial. Physiother Res Int. 2010;15(4):232–42.
Cranen K, Groothuis-Oudshoorn CG, Vollenbroek-Hutten MM, IJzerman MJ. Toward patient-centered telerehabilitation design: understanding chronic pain patients’ preferences for web-based exercise telerehabilitation using a discrete choice experiment. J Med Internet Res. 2017;19(1):1–14.
Matthias MS, Bair MJJPM: The patient–provider relationship in chronic pain management: Where do we go from here? In: Blackwell Publishing Inc Malden, USA; 2010:11(11);1747–9.
Kairy D, Tousignant M, Leclerc N, Côté A-M, Levasseur M. The patient’s perspective of in-home telerehabilitation physiotherapy services following total knee arthroplasty. Int J Environ Res Public Health. 2013;10(9):3998–4011.
Cranen K, Drossaert CH, Brinkman ES, Braakman-Jansen AL, IJzerman MJ, Vollenbroek-Hutten MM. An exploration of chronic pain patients’ perceptions of home telerehabilitation services. Health Expect. 2012;15(4):339–50.
Zaitseva E: Reliability analysis methods for healthcare system. In: 3rd international conference on human system interaction: 2010: IEEE; 2010: 211–216.
Mani S, Sharma S, Singh DK. Concurrent validity and reliability of telerehabilitation-based physiotherapy assessment of cervical spine in adults with non-specific neck pain. J Telemed Telecare. 2021;27(2):88–97.
Zio EJRe, safety s: Reliability engineering: Old problems and new challenges. 2009, 94(2):125–141.
Nolan T, Resar R, Griffin F, Gordon AB: Improving the reliability of health care. Institute for Healthcare Improvement; 2004.
Karanikas N. Using reliability indicators to explore human factors issues in maintenance databases. 2013;30(2):116–28.
Piotrowicz E, Baranowski R, Bilinska M, Stepnowska M, Piotrowska M, Wójcik A, Korewicki J, Chojnowska L, Malek LA, Klopotowski M. A new model of home-based telemonitored cardiac rehabilitation in patients with heart failure: effectiveness, quality of life, and adherence. Eur J Heart Fail. 2010;12(2):164–71.
Piotrowicz E, Zieliński T, Bodalski R, Rywik T, Dobraszkiewicz-Wasilewska B, Sobieszczańska-Małek M, Stepnowska M, Przybylski A, Browarek A, Szumowski Ł. Home-based telemonitored Nordic walking training is well accepted, safe, effective and has high adherence among heart failure patients, including those with cardiovascular implantable electronic devices: a randomised controlled study. Eur J Prev Cardiol. 2015;22(11):1368–77.
Shin J-H, Park SB, Jang SH. Effects of game-based virtual reality on health-related quality of life in chronic stroke patients: a randomized, controlled study. Comput Biol Med. 2015;63:92–8.
Pulman J, Buckley E. Assessing the efficacy of different upper limb hemiparesis interventions on improving health-related quality of life in stroke patients: a systematic review. Top Stroke Rehabil. 2013;20(2):171–88.
Vanmulken D, Spooren AIF, Bongers HMH, Seelen HAM. Robot-assisted task-oriented upper extremity skill training in cervical spinal cord injury: a feasibility study. Spinal Cord. 2015;53(7):547–51.
Gilliaux M, Renders A, Dispa D, Holvoet D, Sapin J, Dehez B, Detrembleur C, Lejeune TM, Stoquart G. Upper Limb Robot-Assisted Therapy in Cerebral Palsy: A Single-Blind Randomized Controlled Trial. Neurorehabil Neural Repair. 2015;29(2):183–92.
Housley SN, Wu D, Richards K, Belagaje S, Ghovanloo M, Butler AJ. Improving Upper Extremity Function and Quality of Life with a Tongue Driven Exoskeleton: A Pilot Study Quantifying Stroke Rehabilitation. Stroke Res Treat. 2017;2017:3603860.
Palermo E, Hayes DR, Russo EF, Calabro RS, Pacilli A, Filoni S. Translational effects of robot-mediated therapy in subacute stroke patients: an experimental evaluation of upper limb motor recovery. Peerj. 2018;6:e5544.
Hung CS, Lin KC, Chang WY, Huang WC, Chang YJ, Chen CL, Grace Yao K, Lee YY. Unilateral vs Bilateral Hybrid Approaches for Upper Limb Rehabilitation in Chronic Stroke: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2019;100(12):2225–32.
Tartamella F, Chillura A, Pisano MF, Cacioppo A, Licari S, Caradonna D, Portaro S, Calabr RS, Bramanti P, Naro A. A case report on intensive, robot-assisted rehabilitation program for brainstem radionecrosis. Medicine. 2020;99(10):e19517.
Flynn N, Froude E, Cooke D, Dennis J, Kuys S. The sustainability of upper limb robotic therapy for stroke survivors in an inpatient rehabilitation setting. Disabil Rehabil. 2021;2(1):1–6.
Levy CE, Silverman E, Jia H, Geiss M, Omura D. Effects of physical therapy delivery via home video telerehabilitation on functional and health-related quality of life outcomes. J Rehabil Res Dev. 2015;52(3):361–70.
Larson JL, Rosen AB, Wilson FA. The effect of telehealth interventions on quality of life of cancer patients: a systematic review and meta-analysis. Telemed J E Health. 2018;24(6):397–405.
Spindler H, Leerskov K, Joensson K, Nielsen G, Andreasen JJ, Dinesen B. Conventional Rehabilitation Therapy Versus Telerehabilitation in Cardiac Patients: A Comparison of Motivation, Psychological Distress, and Quality of Life. Int J Environ Res Public Health. 2019;16(3):512.
Piotrowicz E, Mierzynska A, Pencina M, Opolski G, Zareba W, Banach M, Kowalik I, Orzechowski P, Szalewska D, Pluta SJEHJ: Quality of life in heart failure patients undergoing hybrid comprehensive telerehabilitation versus usual care results of TELEREH-HF randomized clinical trial. 2020, 41(Supplement_2):ehaa946. 3109.
Tabak M, Vollenbroek-Hutten MM, van der Valk PD, van der Palen J, Hermens HJ. A telerehabilitation intervention for patients with Chronic Obstructive Pulmonary Disease: a randomized controlled pilot trial. Clin Rehabil. 2014;28(6):582–91.
Fatoye F, Gebrye T, Fatoye C, Mbada CE, Olaoye MI, Odole AC, Dada O. The clinical and cost-effectiveness of telerehabilitation for people with nonspecific chronic low back pain: randomized controlled trial. JMIR Mhealth Uhealth. 2020;8(6):1–10.
Acknowledgements
The authors thank the Central Library and Documentation Center of Kerman University of Medical Sciences for providing access to knowledge base references required for this study.
Funding
This study was supported by Medical Informatics Research Center of Kerman University of Medical Sciences (Code: 99001139). The funder had no roles in study design, data gathering and analysis.
Author information
Authors and Affiliations
Contributions
KM, KB and ASH have designed the study, finalized the search strategy and implemented the thematic analysis, AH and MSH have searched and screened the articles and extracted the initial codes for data charting. MGH has supervised the whole review process, KM has contributed in revising the finalizing data analysis and KB and ASH have technically edited and finalized the article. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol of this study was approved by ethical committee of Kerman University of Medical Sciences (IR.KMU.REC.1400.606).
Consent for publication
Not applicable.
Competing interests
Authors declare that there are no conflicts of interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix A.
The keywords and searchstrategies used in the PubMed and Web of Science databases are listed in Table1. Table1. Keywords and searchstrategy. Appendix B. Overview of the functionalities and facilitiesof telerehabilitation systems presented in the studies. Appendix C. Evaluationsand a summary of reported outcomes in the included studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Moulaei, K., Sheikhtaheri, A., Nezhad, M.S. et al. Telerehabilitation for upper limb disabilities: a scoping review on functions, outcomes, and evaluation methods. Arch Public Health 80, 196 (2022). https://doi.org/10.1186/s13690-022-00952-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13690-022-00952-w