
Abstract
Background
Low back pain is a disability that occurs worldwide. It is a heterogeneous disorder that affects patients with dominant nociceptive, neuropathic, and central sensitization pain. An important pathophysiology of low back pain involves pain sensitization. Various nonoperative interventions are available for treatment, but there is inconclusive evidence on the effectiveness of these interventions for pain sensitization, leading to arbitrary nonoperative treatments for low back pain.
Methods
We will conduct a systematic review of RCTs evaluating the effectiveness and safety of nonoperative treatment for pain sensitization in patients with low back pain. The primary outcomes will be static quantitative sensory testing, dynamic quantitative sensory testing, and pain algometry. The secondary outcome will be adverse events. We will search the PubMed, Embase, Scopus, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Controlled Trials (CENTRAL), and Cochrane Library databases. Two independent authors will screen the titles and abstracts, review full texts, extract data, assess the risk of bias, and evaluate the quality of evidence. We will qualitatively and quantitatively synthesize the results using a random effects model for meta-analysis.
Discussion
This systematic review aims to provide evidence regarding which treatment, if any, provides the greatest benefit for pain sensitization and safety among patients with low back pain. Evidence synthesized from this systematic review will inform clinical practice and further research. Since there is still a small amount of research, additional studies might need to be conducted in the future.
Systematic review registration
Submitted to PROSPERO on March 20, 2021, CRD42021244054
Similar content being viewed by others


Background
Description of the condition
Low back pain (LBP) is defined as pain or discomfort localized below the costal margin and above the gluteal crease, with or without referred leg pain [1]. Nonspecific LBP is the most common type of LBP and is defined as LBP without any known specific cause or pathology (e.g., infection, cancer, osteoporosis, inflammation, cauda equina syndrome or fractures) [2]. LBP can be classified into three groups based on the duration of symptoms: acute LBP persists for less than 6 weeks, subacute LBP persists between 6 and 12 weeks, and chronic LBP persists for 12 weeks or more [3, 4].
Low back pain is a major health problem among the global population. There are substantiate numbers of populations suffering from low back pain, with an estimated 33% point prevalence, 65% 1-year prevalence, and 84% lifetime prevalence [5]. LBP is an important cause of global disability [6], leading to considerable health and socioeconomic burdens [7]. While low back pain is usually resolved within 6 weeks after onset, some patients still suffer from chronic low back pain [8], which accounts for approximately 40% of LBP patients [9].
Even with the high prevalence and high incidence of LBP, evidence regarding the causes of LBP is still inconclusive. Degenerative changes seen in spinal imaging do not explain the symptoms of LBP, as they are also seen in subjects without low back pain [10], and there is a weak correlation between symptoms of LBP and imaging [11]. An explicit pathological mechanism cannot be identified for 85% of LBP patients; hence, these patients are considered to have nonspecific LBP.
In nonspecific LBP, central sensitization (CS) is described by the International Association for the Study of Pain (IASP) as “Increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input” [12]. Abnormal pain processing in the central nervous system (CNS) rather than from actual damage and/or injury to bodily anatomic structures may lead to increased neuronal response and central sensitization (CS) [13], and this may manifest as mechanical hyperalgesia, allodynia, and/or referred pain, which are important in chronic pain syndromes [14]. While pain hypersensitivity measured by quantitative sensory testing might show no significant association with pain intensity or disability in patients with spinal pain [15], approximately one fourth of nonspecific LBP patients experience pain mainly originating from pain sensitization [16]. Moreover, a recent study revealed the difference in pain sensitization measured by mechanical quantitative sensory testing at the lower back between nonspecific chronic patients with low back pain and healthy controls [17].
Description of the intervention
Various nonoperative interventions are available for nonspecific low back pain treatment, in which lifestyle modification, education, superficial heat, and some nonpharmacological therapy, including exercise and cognitive behavioral therapy, are considered the first-line treatment, while other nonpharmacological therapy and pharmacological therapy, both oral and systemic, are used as second-line or adjunctive treatments [18]. There are several nonpharmacological therapies with promising outcomes for nonspecific low back pain, such as massage [19], acupuncture [20, 21], yoga [22], and interdisciplinary rehabilitation, including biopsychosocial rehabilitation [23, 24], combined chiropractic [25], therapeutic ultrasound [26], radiofrequency denervation [27], neuroreflexotherapy [28], extracorporeal shockwave therapy [29,30,31], laser therapy [32,33,34], and neuromodulation [35,36,37]. For pharmacological therapies, nonsteroidal anti-inflammatory drugs (NSAIDs) [38,39,40], muscle relaxants [41], intra-articular facet joint injection [42], and herbal medicine, including C. frutescens (Cayenne), H. procumbens, S. alba, S. officinale L., S. chilensis, and lavender essential oil, have shown significant benefits for nonspecific LBP [43]. Ultrasound-guided injection and fluoroscopic-guided injection with promising outcomes have also been reviewed [44]. However, there is still a lack of relevant research, and additional studies need to be performed in the future.
Mechanisms through which nonoperative treatment may improve pain sensitization
Pain sensitization is an important pain mechanism in patients with low back pain that relates to increasing pain intensity and disease progression while decreasing quality of life [45, 46]. Clinically, pain sensitization can be indirectly measured by quantitative sensory testing (QST) [47, 48]. Recently, there have been an increasing number of intervention studies on patients with low back pain presenting positive results on pain sensitization outcomes measured by the QST, particularly for pain pressure threshold (PPT) [49,50,51].
Patients with low back pain have decreased mechanical reception [52], decreased endogenous pain inhibition [53], decreased proprioception [54], and increased hyperalgesia [55]. Patients with low back pain can be classified by latent class analysis into pain “sensitized” and “not sensitized,” which might be an important factor of nonoperative treatment effectiveness on pain sensitization. The mechanisms of improving pain sensitization are different between patients with low back pain with high generalized pain sensitivity and those with increased local pain sensitivity [51]. Moreover, nociceptive input inhibition is a promising mechanism by which nonoperative treatment can improve pain sensitization [50].
Why it is important to do this review
There are systematic reviews on observation studies comparing pain sensitization in patients with low back pain and healthy controls [17] and the association of pain sensitization and low back pain outcomes [56]. However, there is no systematic review on how nonoperative treatments affect pain sensitization in patients with low back pain. The systematic literature search and the review methods followed the current edition of the Cochrane Handbook for Systematic Reviews of Interventions [57] and recommendations from the Cochrane Back and Neck group [3].
Objective
The objective is to evaluate the effectiveness of nonoperative treatment for pain sensitization measured by quantitative sensory testing in patients with nonspecific low back pain through a systematic review and meta-analysis.
Methods
We have submitted the systematic review with the International Prospective Register of Systematic Reviews (PROSPERO) on March 20, 2021, and have followed the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement [58]. We used the PRISMA-P 2015 checklist to establish the quality of the protocol (see Additional file 1).
Criteria for considering studies for this review
Types of studies
We will include only original peer-reviewed articles of RCTs of nonoperative interventions. Nonrandomized intervention studies, observational studies, case series, case reports, review articles, letters to editors, commentaries, protocols, and guidelines will be excluded.
Type of participants
We will include RCTs of adult subjects defined as aged 18 years or older who have acute, subacute, or chronic nonspecific low back pain with or without sciatica. We will include RCTs that include participants of any gender and race/ethnicity, any duration of illness, and any previous treatment. We will exclude RCTs that include patients with specific low back pain caused by pathological entities such as infection, neoplasm, metastasis, osteoporosis, rheumatoid arthritis, cauda equina syndrome, or fractures. We will also exclude RCTs with pregnant or postpartum subjects.
Type of interventions
We will include RCTs with any type of nonoperative treatments (i.e., education, self-care, nonpharmacological therapy, pharmacological therapy, or interventional therapy) [18] administered by any route with or without the combination of other treatments as defined by the authors. The comparison intervention will be placebo, other nonoperative treatments, or surgical interventions.
Type of outcome measures
RCTs on this topic have various timing with respect to outcome measurements: immediate (postintervention to up to 7 days post-randomization), short-term (from the eighth day to less than 3 months post-randomization), intermediate-term (from 3 months to less than 6 months post-randomization), and long-term (6 months post-randomization or more). Therefore, we will examine each outcome described below at four time points: immediately, short-term, intermediate-term, and long-term. If there is more than one follow-up time point within each period, we will select the outcome measurement at the longest follow-up time point (i.e., if an RCT reports the outcomes at 1 week, 2 weeks, 1 month, 2 months, 3 months, 6 months, and 1 year, we will analyze the result at two months for the short-term outcome, three months for the intermediate-term outcome and one year for the long-term outcome).
Primary outcomes
-
Mean change in static quantitative sensory testing, including but not limited to chemical, electrical, mechanical (pressure, punctate/brush, vibratory), and thermal (heat, cold), from the baseline.
-
Mean change in dynamic quantitative sensory testing, including but not limited to temporal summation and conditioned pain modulation, from the baseline.
-
Mean change in pressure pain threshold measured by pain algometry from baseline.
Secondary outcomes
-
Proportion of patients who have intervention-related adverse events.
Search methods for the identification of studies
Electronics searches
We will work with an information specialist to design an appropriate search strategy. The PubMed, Embase, Scopus, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Cochrane Central Register of Controlled Trials (CENTRAL) databases will be searched for peer-reviewed studies with no restrictions on publication date or language. In addition, the reference lists of included articles will be searched, as well as related citations from other journals via Google Scholar and Web of Science. Additional file 2 shows the detailed search strategies.
Data collection and analysis
Selection of studies
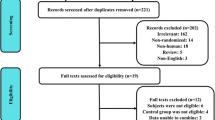
We will use a systematic review management software (Covidence) to manage all citations identified from the systematic search [59]. After removing duplicate studies, two review authors will screen the titles and abstracts of potential studies independently. We will record each article as relevant or not relevant for full-text review. Two review authors will thoroughly read the full texts of relevant RCTs and use the inclusion and exclusion criteria to select RCTs for further data extraction. For each article excluded in the full-text screening, we will report the reason for exclusion. We will generate a study selection flow diagram to describe the workflow and identify the included RCTs. Discrepancies between two review authors in each stage of article screening will be resolved by consensus.
Data extraction and management
We will use Covidence to manage data extraction. We will prospectively design a data extraction form. The data extraction form will be pilot tested and refined. Two independent authors will extract the following data: (1) study information (authors, year of publication, study type, journal, contact, country, and funding), (2) characteristics of the participants (sample size, age, gender, ethnicity, comorbidities, current disease duration, presence of absence of sciatica), (3) intervention detail (type of intervention, duration of treatment, dosage, intervention compliance), (4) comparator detail (type of comparator, duration of treatment, dosage, comparator compliance), and (5) outcomes described under the “type of outcome measures” subheading (complete list of the names of all measured outcomes, unit of measurement, follow-up time point, missing data). All relevant text, tables, and figures will be examined for data extraction. Discrepancies between two independent authors will be resolved by consensus. We will contact the RCT authors to request incompletely reported data. If the RCT authors do not respond for 14 days, we will conduct analyses using available data. Multiple reports from the same study will be identified using authors’ names, funding sponsor, country, trial registration number, specific details of participants, and interventions. Then, we will collect data from each report and link the data together into one study.
Assessment of risk of bias in included studies
Two independent authors will assess the risk of bias in the included trials using the Cochrane Risk of Bias tool 2.0 for randomized control trial study [60]. We will assess each of the following domains:
-
Bias arising from the randomization process.
-
Bias due to deviations from intended intervention.
-
Bias due to missing outcome data*.
-
Bias in the measurement of the outcome*.
-
Bias in the selection of the reported result.
*Domain will be assessed by the outcome.
We will assign each domain as having a low risk of bias, some concerns and a high risk of bias. We will contact the RCT authors if there is not enough information to assess. If the trial authors do not respond for 14 days, we will conduct an assessment using available data. We will resolve the disagreement through discussion. We will present our risk of bias assessment in the “Risk of bias” summary tables.
Assessment of reporting bias
We will search for trial protocols and trial registration. We will then compare the intended outcome measures and analyses specified in protocols and registration with those in the published articles. Reporting bias will be suspected when there is any change in primary outcomes, secondary outcomes, or statistical analysis plan.
Measure of treatment effect
For continuous outcomes, we will present the results as the mean difference with 95% confidence intervals (CIs), while we will present the results as the relative risk with 95% CIs for dichotomous outcomes.
Assessment of heterogeneity
We will assess statistical heterogeneity using the I2 and X2 statistics. We will categorize the level of heterogeneity for the I2 statistic as defined in chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions: 0 to 40% might not be important, 30 to 60% may represent moderate heterogeneity, 50 to 90% may represent substantial heterogeneity, and 75 to 100% may represent considerable heterogeneity [57]. For the X2 test, we will assess the included trials for statistical heterogeneity with a P value of less than 0.10 (statistically significant).
Data synthesis
We will provide qualitative analysis of trials and their results following standard 4.2 and conduct a qualitative synthesis, chapter 4 of Finding What Works in Health Care: Standards for Systematic Reviews [61]. If there is no considerable clinical, methodological, and statistical heterogeneity, we will use random effects meta-analysis by the DerSimonian and Laird method. The meta-analysis will be performed using Review Manager version 5.3 [62]. We will summarize the three primary outcome measures (mean change in static quantitative sensory testing from baseline; mean change in dynamic quantitative sensory testing from baseline; mean change in pressure pain threshold measured by pain algometry from baseline) at two specific time points, including short-term and intermediate-term time points along with adverse event outcome measures, in the “Summary of findings” table.
Quality of evidence
We will use the Grading of Recommendation Assessment, Development and Evaluation (GRADE) approach to assess the quality of evidence for the primary outcome (i.e., mean change in static quantitative sensory testing from the baseline; mean change in dynamic quantitative sensory testing from the baseline; mean change in pressure pain threshold measure by pain algometry). We will use the five GRADE considerations, including risk of bias, imprecision, inconsistency, indirectness, and publication bias. We will then classify each outcome as follows [63]:
-
High quality was defined as “we are very confident that the true effect lies close to that of the estimate of the effect.”
-
Moderate quality is defined as “we are moderately confident in the effect estimate: the true effect is likely to be close to estimate of the effect, but there is a possibility that it is substantially different.”
-
Low quality, defined as “our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.”
-
Very low quality defined as “we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
Subgroup analysis and investigation of heterogeneity
We will undertake a subgroup analysis by type of intervention, duration of intervention (immediate, short-term, intermediate-term, and long-term), type of comparator, presence or absence of sciatica, and disease duration (acute and chronic).
Sensitivity analysis
We will exclude RCTs with a high risk of overall bias to assess the robustness of the results. We will conduct additional sensitivity analyses to determine the impact of any post hoc decisions, if any, during the review process.
Availability of data and materials
Data will be available as supplementary files.
Abbreviations
- CENTRAL:
-
Cochrane Central Register of Controlled Trials
- CIs:
-
Confidence intervals
- GRADE:
-
Grading of Recommendation Assessment, Development and Evaluation
- LBP:
-
Low back pain
- PRISMA-P:
-
Preferred Reporting Items for Systematic review and Meta-analysis Protocols
- QST:
-
Quantitative sensory testing
- RCTs:
-
Randomized controlled trials
- US:
-
United States
References
Airaksinen O, Brox J, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion A, Reis S, Staal J, Ursin H, Zanoli G. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006;15(Suppl 2):S192–300. https://doi.org/10.1007/s00586-006-1072-1.
Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379(9814):482–91. https://doi.org/10.1016/S0140-6736(11)60610-7.
Furlan AD, Malmivaara A, Chou R, Maher CG, Deyo RA, Schoene M, Bronfort G, van Tulder MW. Editorial Board of the Cochrane Back, Neck Group. 2015 Updated Method Guideline for Systematic Reviews in the Cochrane Back and Neck Group. Spine (Phila Pa 1976). 2015;40(21):1660–73. https://doi.org/10.1097/BRS.0000000000001061.
Krismer M, van Tulder M. Low Back Pain Group of the Bone and Joint Health Strategies for Europe Project. Strategies for prevention and management of musculoskeletal conditions. Low back pain (non-specific). Best Pract Res Clin Rheumatol. 2007;21(1):77–91. https://doi.org/10.1016/j.berh.2006.08.004.
Henschke N, Kamper SJ, Maher CG. The epidemiology and economic consequences of pain. Mayo Clin Proc. 2015;90(1):139–47. https://doi.org/10.1016/j.mayocp.2014.09.010.
Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743–800. https://doi.org/10.1016/S0140-6736(15)60692-4.
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–47. https://doi.org/10.1016/S0140-6736(16)30970-9.
da C Menezes Costa L, Maher CG, Hancock MJ, McAuley JH, Herbert RD, Costa LO. The prognosis of acute and persistent low-back pain: a meta-analysis. CMAJ. 2012;184(11):E613–24. https://doi.org/10.1503/cmaj.111271.
Costa Lda C, Maher CG, McAuley JH, Hancock MJ, Herbert RD, Refshauge KM, Henschke N. Prognosis for patients with chronic low back pain: inception cohort study. BMJ. 2009;339:b3829. https://doi.org/10.1136/bmj.b3829.
Steffens D, Hancock MJ, Pereira LS, Kent PM, Latimer J, Maher CG. Do MRI findings identify patients with low back pain or sciatica who respond better to particular interventions? A systematic review. Eur Spine J. 2016;25(4):1170–87. https://doi.org/10.1007/s00586-015-4195-4.
van Tulder M, Becker A, Bekkering T, Breen A, del Real MT, Hutchinson A, Koes B, Laerum E, Malmivaara A; COST B13 Working Group on Guidelines for the Management of Acute Low Back Pain in Primary Care. Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. Eur Spine J. 2006;15(Suppl 2):S169–91. https://doi.org/10.1007/s00586-006-1071-2.
Loeser JD, Treede RD. The Kyoto protocol of IASP Basic Pain Terminology. Pain. 2008;137(3):473–477. https://doi.org/10.1016/j.pain.2008.04.025.
Baranauskas G, Nistri A. Sensitization of pain pathways in the spinal cord: cellular mechanisms. Prog Neurobiol. 1998;54(3):349–65. https://doi.org/10.1016/s0301-0082(97)00067-1.
Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2–S15. https://doi.org/10.1016/j.pain.2010.09.030.
Hübscher M, Moloney N, Leaver A, Rebbeck T, McAuley JH, Refshauge KM. Relationship between quantitative sensory testing and pain or disability in people with spinal pain-a systematic review and meta-analysis. Pain. 2013;154(9):1497–1504. https://doi.org/10.1016/j.pain.2013.05.031.
Roussel NA, Nijs J, Meeus M, Mylius V, Fayt C, Oostendorp R. Central sensitization and altered central pain processing in chronic low back pain: fact or myth? Clin J Pain. 2013;29(7):625–38. https://doi.org/10.1097/AJP.0b013e31826f9a71.
den Bandt HL, Paulis WD, Beckwée D, Ickmans K, Nijs J, Voogt L. Pain Mechanisms in Low Back Pain: A Systematic Review With Meta-analysis of Mechanical Quantitative Sensory Testing Outcomes in People With Nonspecific Low Back Pain. J Orthop Sports Phys Ther. 2019;49(10):698–715. https://doi.org/10.2519/jospt.2019.8876.
Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, Ferreira PH, Fritz JM, Koes BW, Peul W, Turner JA, Maher CG; Lancet Low Back Pain Series Working Group. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–83. https://doi.org/10.1016/S0140-6736(18)30489-6.
Furlan AD, Giraldo M, Baskwill A, Irvin E, Imamura M. Massage for low-back pain. Cochrane Database Syst Rev. 2015(9):CD001929. https://doi.org/10.1002/14651858.CD001929.
Mu J, Furlan AD, Lam WY, Hsu MY, Ning Z, Lao L. Acupuncture for chronic nonspecific low back pain. Cochrane Database Syst Rev. 2020;12(12):CD013814. https://doi.org/10.1002/14651858.CD013814.
Furlan AD, van Tulder MW, Cherkin DC, Tsukayama H, Lao L, Koes BW, Berman BM. Acupuncture and dry-needling for low back pain. Cochrane Database Syst Rev. 2005:CD001351. https://doi.org/10.1002/14651858.CD001351.
Wieland LS, Skoetz N, Pilkington K, Vempati R, D'Adamo CR, Berman BM. Yoga treatment for chronic non-specific low back pain. Cochrane Database Syst Rev. 2017;1(1):CD010671. https://doi.org/10.1002/14651858.CD010671.
Marin TJ, Van Eerd D, Irvin E, Couban R, Koes BW, Malmivaara A, van Tulder MW, Kamper SJ. Multidisciplinary biopsychosocial rehabilitation for subacute low back pain. Cochrane Database Syst Rev. 2017;6(6):CD002193. https://doi.org/10.1002/14651858.CD002193.
Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJ, Ostelo RW, Guzman J, van Tulder MW. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ. 2015;350:h444. https://doi.org/10.1136/bmj.h444.
Walker BF, French SD, Grant W, Green S. Combined chiropractic interventions for low-back pain. Cochrane Database Syst Rev. 2010;2010(4):CD005427. https://doi.org/10.1002/14651858.CD005427.
Ebadi S, Henschke N, Forogh B, Nakhostin Ansari N, van Tulder MW, Babaei-Ghazani A, Fallah E. Therapeutic ultrasound for chronic low back pain. Cochrane Database Syst Rev. 2020;7(7):CD009169. https://doi.org/10.1002/14651858.CD009169.
Maas ET, Ostelo RW, Niemisto L, Jousimaa J, Hurri H, Malmivaara A, van Tulder MW. Radiofrequency denervation for chronic low back pain. Cochrane Database Syst Rev. 2015:CD008572. https://doi.org/10.1002/14651858.CD008572.
Urrútia G, Burton AK, Morral A, Bonfill X, Zanoli G. Neuroreflexotherapy for non-specific low-back pain. Cochrane Database Syst Rev. 2004:CD003009. https://doi.org/10.1002/14651858.CD003009.
Király M, Bender T, Hodosi K. Comparative study of shockwave therapy and low-level laser therapy effects in patients with myofascial pain syndrome of the trapezius. Rheumatol Int. 2018;38(11):2045–2052. https://doi.org/10.1007/s00296-018-4134-x.
Wei W, Tang HY, Li YZ, Wang TS. Effectiveness of extracorporeal shock wave for low back pain: A protocol of systematic review. Medicine (Baltimore). 2019;98(7):e14511. https://doi.org/10.1097/MD.0000000000014511.
Walewicz K, Taradaj J, Rajfur K, Ptaszkowski K, Kuszewski MT, Sopel M, Dymarek R. The Effectiveness Of Radial Extracorporeal Shock Wave Therapy In Patients With Chronic Low Back Pain: A Prospective, Randomized, Single-Blinded Pilot Study. Clin Interv Aging. 2019;14:1859–69. https://doi.org/10.2147/CIA.S224001.
Glazov G, Yelland M, Emery J. Low-dose laser acupuncture for non-specific chronic low back pain: a double-blind randomised controlled trial. Acupunct Med. 2014;32(2):116–23. https://doi.org/10.1136/acupmed-2013-010456.
AAbdelbasset WK, Nambi G, Alsubaie SF, Abodonya AM, Saleh AK, Ataalla NN, Ibrahim AA, Tantawy SA, Kamel DM, Verma A, Moawd SA. A Randomized Comparative Study between High-Intensity and Low-Level Laser Therapy in the Treatment of Chronic Nonspecific Low Back Pain. Evid Based Complement Alternat Med. 2020;2020:1350281. https://doi.org/10.1155/2020/1350281.
Abdelbasset WK, Nambi G, Elsayed SH, Alrawaili SM, Ataalla NN, Abodonya AM, Saleh AK, Moawd SA. Short-term clinical efficacy of the pulsed Nd: YAG laser therapy on chronic nonspecific low back pain: A randomized controlled study. Medicine (Baltimore). 2020;99(36):e22098. https://doi.org/10.1097/MD.0000000000022098.
Røe C. Transcranial magnetic stimulation, paravertebral muscles training, and postural control in chronic low back pain. Scand J Pain. 2016;12:60–61. https://doi.org/10.1016/j.sjpain.2016.04.004.
Shafiee S, Hasanzadeh Kiabi F, Shafizad M, Emami Zeydi A. Repetitive transcranial magnetic stimulation: a potential therapeutic modality for chronic low back pain. Korean J Pain. 2017;30(1):71–72. https://doi.org/10.3344/kjp.2017.30.1.71.
Ng SK, Urquhart DM, Fitzgerald PB, Cicuttini FM, Hussain SM, Fitzgibbon BM. The Relationship Between Structural and Functional Brain Changes and Altered Emotion and Cognition in Chronic Low Back Pain Brain Changes: A Systematic Review of MRI and fMRI Studies. Clin J Pain. 2018;34(3):237–261. https://doi.org/10.1097/AJP.0000000000000534.
Enthoven WT, Roelofs PD, Deyo RA, van Tulder MW, Koes BW. Non-steroidal anti-inflammatory drugs for chronic low back pain. Cochrane Database Syst Rev. 2016;2(2):CD012087. https://doi.org/10.1002/14651858.CD012087.
Roelofs PD, Deyo RA, Koes BW, Scholten RJ, van Tulder MW. Nonsteroidal anti-inflammatory drugs for low back pain: an updated Cochrane review. Spine (Phila Pa 1976). 2008;33(16):1766–74. https://doi.org/10.1097/BRS.0b013e31817e69d3.
van der Gaag WH, Roelofs PD, Enthoven WT, van Tulder MW, Koes BW. Non-steroidal anti-inflammatory drugs for acute low back pain. Cochrane Database Syst Rev. 2020;4(4):CD013581. https://doi.org/10.1002/14651858.CD013581.
van Tulder MW, Touray T, Furlan AD, Solway S, Bouter LM. Muscle relaxants for non-specific low back pain. Cochrane Database Syst Rev. 2003:CD004252. https://doi.org/10.1002/14651858.CD004252.
Nopsopon T, Pongpirul K, Rittiphairoj T, Lertparinyaphorn I, Suputtitada A. The therapeutic effect of intra-articular facet joint injection with normal saline as a comparator for chronic low back pain: a systematic review and meta-analysis. MedRxiv. 2021; https://doi.org/10.1101/2021.01.27.21250595.
Oltean H, Robbins C, van Tulder MW, Berman BM, Bombardier C, Gagnier JJ. Herbal medicine for low-back pain. Cochrane Database Syst Rev. 2014:CD004504. https://doi.org/10.1002/14651858.CD004504.
Wu T, Zhao WH, Dong Y, Song HX, Li JH. Effectiveness of Ultrasound-Guided Versus Fluoroscopy or Computed Tomography Scanning Guidance in Lumbar Facet Joint Injections in Adults With Facet Joint Syndrome: A Meta-Analysis of Controlled Trials. Arch Phys Med Rehabil. 2016;97(9):1558–63. https://doi.org/10.1016/j.apmr.2015.11.013.
Smart KM, Blake C, Staines A, Doody C. The Discriminative validity of "nociceptive," "peripheral neuropathic," and "central sensitization" as mechanisms-based classifications of musculoskeletal pain. Clin J Pain. 2011;27(8):655–63. https://doi.org/10.1097/AJP.0b013e318215f16a.
Smart KM, Blake C, Staines A, Thacker M, Doody C. Mechanisms-based classifications of musculoskeletal pain: part 1 of 3: symptoms and signs of central sensitisation in patients with low back (± leg) pain. Man Ther. 2012;17(4):336–44. https://doi.org/10.1016/j.math.2012.03.013.
Blumenstiel K, Gerhardt A, Rolke R, Bieber C, Tesarz J, Friederich HC, Eich W, Treede RD. Quantitative sensory testing profiles in chronic back pain are distinct from those in fibromyalgia. Clin J Pain. 2011;27(8):682–90. https://doi.org/10.1097/AJP.0b013e3182177654.
Arendt-Nielsen L, Morlion B, Perrot S, Dahan A, Dickenson A, Kress HG, Wells C, Bouhassira D, Drewes AM. Assessment and manifestation of central sensitisation across different chronic pain conditions. Eur J Pain. 2018;22(2):216–41. https://doi.org/10.1002/ejp.1140.
Aspinall SL, Jacques A, Leboeuf-Yde C, Etherington SJ, Walker BF. Pressure pain threshold and temporal summation in adults with episodic and persistent low back pain trajectories: a secondary analysis at baseline and after lumbar manipulation or sham. Chiropr Man Therap. 2020;28(1):36. https://doi.org/10.1186/s12998-020-00326-5.
Chapman KB, van Roosendaal BK, Yousef TA, Vissers KC, van Helmond N. Dorsal Root Ganglion Stimulation Normalizes Measures of Pain Processing in Patients with Chronic Low-Back Pain: A Prospective Pilot Study using Quantitative Sensory Testing. Pain Pract. 2021;21(5):568–577. https://doi.org/10.1111/papr.12992.
Nim CG, Weber KA, Kawchuk GN, O'Neill S. Spinal manipulation and modulation of pain sensitivity in persistent low back pain: a secondary cluster analysis of a randomized trial. Chiropr Man Therap. 2021;29(1):10. https://doi.org/10.1186/s12998-021-00367-.
Luomajoki H, Moseley GL. Tactile acuity and lumbopelvic motor control in patients with back pain and healthy controls. Br J Sports Med. 2011;45(5):437–40. https://doi.org/10.1136/bjsm.2009.060731.
Corrêa JB, Costa LO, de Oliveira NT, Sluka KA, Liebano RE. Central sensitization and changes in conditioned pain modulation in people with chronic nonspecific low back pain: a case-control study. Exp Brain Res. 2015;233(8):2391–9. https://doi.org/10.1007/s00221-015-4309-6.
Brumagne S, Cordo P, Verschueren S. Proprioceptive weighting changes in persons with low back pain and elderly persons during upright standing. Neurosci Lett. 2004;366(1):63–6. https://doi.org/10.1016/j.neulet.2004.05.013.
O'Neill S, Manniche C, Graven-Nielsen T, Arendt-Nielsen L. Generalized deep-tissue hyperalgesia in patients with chronic low-back pain. Eur J Pain. 2007;11(4):415–20. https://doi.org/10.1016/j.ejpain.2006.05.009.
Marcuzzi A, Dean C, Wrigley P, Chakiath R, Hush J. Prognostic value of quantitative sensory testing in low back pain: a systematic review of the literature. J Pain Res. 2016;9:599–607.
Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, Thomas J. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019:ED000142. https://doi.org/10.1002/14651858.ED000142.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350:g7647. https://doi.org/10.1136/bmj.g7647.
Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org. Accessed on 29 Mar 2022.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. https://doi.org/10.1136/bmj.l4898.
Institute of Medicine (US) Committee on Standards for Systematic Reviews of Comparative Effectiveness Research. Finding What Works in Health Care: Standards for Systematic Reviews. Eden J, Levit L, Berg A, Morton S, editors. Washington (DC): National Academies Press (US); 2011.
Review Manager 5 (RevMan 5) [Computer program]. Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration; 2014. Available from https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman/revman-5-download. Accessed 29 Mar 2022.
Schünemann H, Brożek J, Guyatt G, Oxman A. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. GRADE Working Group; 2013. Available from https://training.cochrane.org/resource/grade-handbook. Accessed 29 Mar 2022.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
TN and AS contributed to writing the manuscript. TN, AS, and KP contributed to the conception and design. TN, AS, IL, and KP contributed to the critical revision of manuscript. All authors read and approved the final manuscript. AS is the guarantor of the review.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA-P 2015 Checklist.
Additional file 2.
Details of search strategies for each database.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nopsopon, T., Suputtitada, A., Lertparinyaphorn, I. et al. Nonoperative treatment for pain sensitization in patients with low back pain: protocol for a systematic review. Syst Rev 11, 59 (2022). https://doi.org/10.1186/s13643-022-01927-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-022-01927-2