
Abstract
Background
Midwives’ practices during the second stage of labour vary nationally and internationally. We aim to retrieve evidence that supports high-quality intrapartum care by conducting a systematic review of the literature.
Methods
Electronic bibliographic databases including PubMed, EMBASE.com, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Maternity and Infant Care Database (through MIDIRS), and The Cochrane Library will be searched to identify studies that meet the inclusion criteria. No language or publication date constraints will be applied. Articles that pass the two-stage screening process will then be assessed for risk of bias and have their reference lists hand searched.
Discussion
A midwife’s practice can be influenced by education and cultural practices but ultimately it should be informed by up-to-date research evidence. By analysing and synthesising the results of the studies, this systematic review will provide valuable insight into high-quality evidence-based midwifery care, which can inform practice, education and future research.
Systematic review registration
PROSPERO CRD42018088300
Similar content being viewed by others

Background
Labour and birth constitute significant and memorable life events for a woman and her wider family. How a woman experiences birth has both short- and long-term effects on health and wellbeing for both herself and her baby [2, 4, 5, 9, 10, 14]. Experiencing a physiological labour and birth may contribute to positive outcomes: “The health and well-being of a mother and child at birth largely determines the future health and wellness of the entire family” [15].
As far back as 1997, the WHO defined physiological birth as spontaneous onset, low risk at the commencement of labour and continuing so for the remainder of labour and birth. The infant is born spontaneously, between 37 and 42 weeks of pregnancy with a cephalic presentation. Following birth, both mother and infant are in good condition (World Health Organization, 1997). Labour can be divided into three stages: the first, second and the third stage of labour. The WHO (2018) have recently defined the first stage of labour as the time period characterised by regular painful uterine contractions until full dilatation of the cervix and the second stage of labour as the time period between full dilatation of the cervix and the birth of the baby, whilst the woman is experiencing an involuntary urge to bear down, due to expulsive uterine contractions. The third stage is recognised as the period after the birth of the baby ending with the birth of the placenta and fetal membranes [1].
Midwives can facilitate the process of physiological labour and birth by enabling the interplay of reproductive hormonal and neuro-hormonal mechanisms by their kind and respectful caring practices, which promote oxytocin release for effective uterine contractions during labour and the relaxation of the birth canal [12, 13]. However, there is little explanation or description of the variety of physical and emotional actions the midwife does when “being with” a woman during birth of the baby, in particular, how they facilitate this physiological process. Furthermore, Kennedy et al. emphasised the priority of research that “identifies and describes aspects of care that optimise, and those that disturb, the biological/physiological processes for healthy childbearing women and fetus/newborn infants and those who experience complications” ([8] p e777).
Therefore, we plan to undertake a systematic review to identify pertinent evidence related to intrapartum midwifery care, focusing specifically on care during the second stage of labour.
This leads to our structured research questions which were formulated using the PICO (Patient or Population, Intervention, Comparison, Outcome) framework for quantitative research and the PEO (Population, Exposure, Outcomes) question format for qualitative research questions: “How do midwives facilitate women to give birth during physiological second stage of labour?” and “What evidence supports good quality intrapartum care during the second stage of labour?”
The aim of the systematic review is to collate, analyse and synthesise the international evidence that supports high-quality intrapartum care during the second stage, which will inform midwifery practice, education and future research and positively influence this aspect of midwifery care for women.
Methods
We will undertake a systematic literature search based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (www.prisma-statement.org) (see Additional file 1). The Peer Review of Electronic Search Strategies (PRESS) 2015 Guideline Statement will be used to enhance the quality and comprehensiveness of the electronic literature search [11]. We will use the PICO framework for quantitative research—P: women in second stage of labour, I: intrapartum intervention by midwives, C: standard care, O: spontaneous physiological birth. For qualitative research, we will use PEO framework—P: women in second stage of labour, E: midwives practices in the second stage of labour, O: spontaneous physiological birth. Systematic searches will identify all pertinent publications, in relevant bibliographic databases: PubMed, EMBASE.com, CINAHL (via Ebsco), PsycINFO (via Ebsco) and The Cochrane Library (via Wiley) from inception, i.e. no publication date restrictions will be applied. An additional search will be performed in the Maternity and Infant Care Database (through MIDIRS). The search strategy will include the Boolean terms OR and AND, the search terms will include controlled terms (for example, MeSH terms in PubMed and Emtree in Embase) as well as free text terms and truncations (*). We will use free text terms only in The Cochrane Library and synonyms and variations of the keywords in all databases (see Fig. 1). The search terms include the following: Labor, Obstetric"[Mesh] OR "Parturition"[Mesh] OR "Delivery, Obstetric"[Mesh] OR labor [tiab] OR labour [tiab] OR birth*[tiab] OR childbirth*[tiab] OR parturition*[tiab] OR deliver*[tiab] Labor, Stage, Second"[Mesh]. All languages will be accepted, as the COST Action network for this study includes individuals who can translate most languages. Animal studies will be excluded. This protocol is registered in the International Prospective Register of Systematic Reviews (PROSPERO; Registration CRD42018088300).

Search terms
Study identification and selection
Criteria for considering studies for review
Inclusion criteria
All studies describing midwives’ care or practice during second stage of physiological birth or normal birth will be included. Both relevant quantitative and qualitative studies will be eligible for review.
Exclusion criteria
Studies examining midwifery practice of women that focused only on care during the first or third stage of labour are not eligible. Those studies which include women with an epidural, spinal or instrumental/operative vaginal birth or caesarean section birth will not be included. Furthermore, studies that include women who have not reached full-term pregnancy, have had their pregnancy induced or labour augmented with intravenous oxytocin will not be eligible.
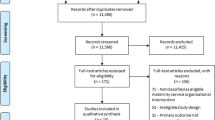
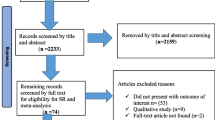
Studies will be selected for inclusion following a two-stage process using Covidence. Covidence is a web-based software platform that streamlines the production of systematic reviews, including Cochrane reviews. All available studies, irrespective of language will be included to decrease bias [6]. Within the first stage, each study will have its title and abstract screened by pairs of two independent reviewers (CV, DS, VN, MH). Studies will be excluded if both reviewers consider that a study does not meet eligibility criteria. Full-text manuscripts of all citations that are likely to meet the selection criteria will be retrieved. The final inclusion or exclusion decisions will be made on examination of the full-text manuscripts. Two reviewers will then independently select the studies, which meet the predefined criteria. All disagreements will be discussed and resolved by a senior review author (CV or MH). We will report the reasons for exclusion for each study, and a flow chart (Fig. 2) will be used to present the process of screening and inclusion of the studies in this review. Articles that pass the two-stage screening process will then be assessed for risk of bias and have their reference lists hand searched.

Flow chart
Study quality assessment
Study quality assessment will be performed by two reviewers independently. The tool utilised to assess the quality of evidence will depend on each study’s methodological approach. To assess the risk of bias in randomised controlled trials, the Cochrane Collaboration’s tool for assessing risk of bias will be used [7]. For all other study types, the Critical Appraisal Skills Programme (CASP) criteria will be used [3]. The Grading of Recommendations Assessment, Development and Evaluation (GRADE), Cochrane’s recommended approach for grading the body of evidence, will be used for quantitative studies. Confidence in the Evidence from Reviews of Qualitative research (CERQual) will be used for grading the confidence in the evidence of qualitative studies.
Analysis
Depending on the findings, a meta-analysis and/or a meta-synthesis will be undertaken.
Discussion
A midwife’s practice can be influenced by education and cultural practices, but ultimately it should be informed by up-to-date research evidence. This systematic review will comprehensively collate, analyse and synthesise the available evidence relating to what midwives do to facilitate physiological birth. This will help to formulate midwifery practice, education and future research recommendations that support high-quality intrapartum care during the second stage of labour.
Abbreviations
- CERQual:
-
Confidence in the Evidence from Reviews of Qualitative research
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
- PEO:
-
Population, Exposure, Outcomes
- PICO:
-
Patient or Population, Intervention, Comparison, Outcome
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- WHO:
-
World Health Organization
References
Begley CM, Gyte GM, Devane D, McGuire W, Weeks A. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2015;3:CD007412 DOI: 10.1002/14651858.CD007412.pub4. Review.
Creedy DK, Shochet IM, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth. 2000;27(2):104–11.
Critical Appraisal Skills Programme 2018. CASP Checklists. Available at https://casp-uk.net/casp-tools-checklists/.
Czarnocka J, Slade P. Prevalence and predictors of post-traumatic stress symptoms following childbirth. Br J Clin Psychol. 2000 Mar;39(Pt 1):35–51.
Dahlen HG, Dowling H, Tracy M, Schmied V, Tracy S. Maternal and perinatal outcomes amongst low risk women giving birth in water compared to six birth positions on land. A descriptive cross sectional study in a birth centre over 12 years. Midwifery. 2013;29(7):759–64. https://doi.org/10.1016/j.midw.2012.07.002.
Egger M, Zellweger-Zahner T, et al. Language bias in randomised controlled trials published in English and German. Lancet. 1997;350:326–9. https://doi.org/10.1016/S0140-6736(97)02419-7.
Higgins JPT. In: Green S, editor. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration; 2011. Available from www.handbook.cochrane.org.
Kennedy HP, Yoshida S, Costello A, Declercq E, Dias MA, Duff E, Gherissi A, Kaufman K, McConville F, McFadden A, Michel-Schuldt M, Moyo NT, Schuiling K, Speciale AM, Renfrew MJ. Asking different questions: research priorities to improve the quality of care for every woman, every child. Lancet Glob Health. 2016;4(11):e777–9. https://doi.org/10.1016/S2214-109X(16)30183-8 Epub 2016 Sep 20.
Lemola S, Stadlmayr W, Grob A. Maternal adjustment five months after birth: the impact of the subjective experience of childbirth and emotional support from the partner. J. Reprod. Infant Psychol. 2007;25(3):190–202 doi.org/10.1080/02646830701467231.
Lundgren I, et al. Long-term memories and experiences of childbirth in a Nordic context—a secondary analysis. Int J Qual Stud Health Well Being. 2009;4(2):115–28.
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40–6 doi: 10.1016.
Uvnäs-Moberg K. The hormone of closeness: the role of oxytocin in relationships. London: Pinter & Martin Ltd; 2012.
Uvnäs-Moberg K. How kindness, warmth, empathy and support promote the progress of labour: a physiological perspective. In: Byrom S, Downe S, editors. The Roar Behind the Silence. London: Pinter & Martin Ltd; 2015.
Waldenström U, Schytt E. A longitudinal study of women’s memory of labour pain—from 2 months to 5 years after the birth. BJOG Int J Obstet Gynaecol. 2009;116(4):577–83.
World Health Organization. World health report 2005: make every mother and child count. Geneva: WHO; 2005.
Acknowledgements
This article is based upon work from COST Action IS1405 BIRTH: “Building Intrapartum Research Through Health - an interdisciplinary whole system approach to understanding and contextualising physiological labour and birth” (https://www.cost.eu/actions/IS1405/#tabs|Name:overview), supported by COST (European Cooperation in Science and Technology).
The authors gratefully thank Mary Dharmachandran (subject librarian at the Royal College of Midwives, UK) for her valuable contribution to this systematic review.
Finally, they thank the School of Nursing and Midwifery, Queen’s University Belfast, who funded access to Covidence, the web-based systematic review software package recommended by Cochrane.
Funding
This systematic review will be conducted as part of the COST Action IS1405 “Building Intrapartum Research Through Health (BIRTH) – an interdisciplinary whole system approach to understanding and contextualising physiological labour and birth”. Furthermore, the School of Nursing and Midwifery, Queen’s University Belfast, funded access to Covidence, the web-based systematic review software package recommended by Cochrane.
Availability of data and materials
Not applicable.
Author information
Authors and Affiliations
Contributions
CV and MH designed the study. All authors (CV, DS, VN, RO and MH) contributed in writing the manuscript and critically revised earlier drafts of the paper. All authors read and approved the final manuscript. As the guarantor of the review, MH accepts official responsibility for the overall integrity of the manuscript (including ethics, data handling, reporting of results and study conduct).
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This is a protocol for a systematic review which utilises published data, and as such, ethical approval is not required for this study. Wide dissemination of the findings of this study will be undertaken via peer-reviewed publications and conference presentations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
The PRISMA-P 2015 Checklist (PDF 373 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Verhoeven, C.J., Spence, D., Nyman, V. et al. How do midwives facilitate women to give birth during physiological second stage of labour? A protocol for a systematic review. Syst Rev 8, 1 (2019). https://doi.org/10.1186/s13643-018-0916-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-018-0916-1