
Abstract
Background
Sperm motility is a critical factor in male fertility. Low motility can be caused by a variety factors including abnormal spermatogenesis, oxidative damage, or depletion of intracellular ATP. Recent findings indicate that hydrogen molecule (H2) selectively reduces toxic reactive oxygen species. In this study, we investigated the effects of H2 on human sperm motility in vitro.
Methods
Experimentally damaged sperm suspensions from patients left at room temperature for > 5 days or frozen immediately after ejaculation were used. After exposure with H2, their forward motility was measured with a counting chamber. A time-lapse movie was recorded to analyze sperm swimming speed. Mitochondria were stained with a membrane potential-sensitive dye.
Results
H2 treatment significantly improved the rate of forward motility, whereas treatment with nitrogen gas did not. While treatment for 30 min was sufficient to improve motility, it did not affect sperm swimming speed. After 24 h, retreatment with H2 increased the motility again. H2 treatment also increased mitochondrial membrane potential. Forward motility of low motile frozen-thawed sperm from patients significantly improved with cleavage medium containing H2.
Conclusions
Our results illustrated that H2 treatment stimulates low sperm motility. H2 is a new promising tool for male infertility treatments.
Similar content being viewed by others

Introduction
Several factors are present in infertile males with sperm function defects caused by asthenozoospermia [1]. Gene defects, including DNMT3B and MTHFR, have been well documented to correlate with this phenotype [2]. Mitochondria DNA haplogroups may affect sperm motility [3]. Systemic disorders such as polycystic kidney disease [4] also affect fertility and cause asthenozoospermia. Sperms are highly vulnerable to oxidative stress because they contain high concentrations of free unsaturated fatty acids, lack intracellular antioxidant enzymes, and have a limited capacity for DNA repair [5]. The precise mechanisms of motility loss in the sperm, the ability of this cell to fuse with the oocyte under oxidative stress, and the subsequent initiation of lipid peroxidation are not known [6]; however, both oxidative damage to the axoneme and depletion of intracellular ATP appear to be involved [7]. While mitochondria are crucial for ATP production, they are also the main source of reactive oxygen species (ROS), notably via the formation of superoxide in the electron transport chain. Nevertheless, low levels of ROS are essential and act as second messengers for the regulation of sperm functions [8].
Previous studies have examined the effects of seminal plasma levels or oral administration of zinc, aspartic acid or coenzyme Q10 on semen quality, and their effects in vitro [9-11]. Especially, myoinositol and xanthine derivates have turned out to be an effective tool in stimulation of sperm motility [12,13]. We reported previously that the hydrogen molecule (H2) dose-dependently reduces the hydroxyl radical (•OH) in vitro, whereas H2 is too weak to reduce physiologically important ROS such as NO• and superoxide [14]. H2, the smallest molecule in the universe, has the unique ability of rapidly diffusing across membranes; it can react with cytotoxic •OH in all organelles, including mitochondria and the nucleus, and thus effectively protect cells against oxidative damage. Indeed, H2 prevented a decrease in the cellular levels of ATP synthesized in mitochondria [14]. Many studies reported previously that H2 suppressed oxidative stress-induced injury in several organs, reduced ischemia-reperfusion injury in the brain, heart, liver, and retina [14-17], protected against nephrotoxicity [18], and suppressed radiation-induced acute injury in the lung [19]. In the present study, we used experimentally damaged sperm suspensions, and investigated whether H2 treatment exerts protective effects on human sperm. We further demonstrated the practical application of H2 treatment of frozen-thawed sperm from patients.
Methods
Preparation of sperm suspensions
Human sperm suspensions from donors were used in this study. This study was approved by the Institutional Review Board of Yamashita Shonan Yume Clinic with consent from patients receiving in vitro fertilization (IVF) treatment at the Yamashita Shonan Yume Clinic. All patients needed IVF and/or intracytoplasmic sperm injection (ICSI) because they showed seminal defects such as hypospermia, oligozoospermia and asthenozoospermia. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and its later amendments. Informed consent was obtained from all patients for being included in the study.
Semen suspensions from patients, who were asked to respect an ejaculatory abstinence period of 3–5 days, were collected by masturbation. A part of them were immediately frozen by the method described below. Sperm parameters were assessed according to World Health Organization criteria (2010) [20]. Collected samples were prepared by washing semen in cleavage medium (SAGE cleavage medium; CooperSurgical, CT, USA) supplemented with 10% plasma protein fraction (PPF; Baxter Healthcare, IL, USA) to remove seminal plasma, centrifuging through a two-layer Percoll® density gradient at 600 × g for 15 min, concentrating by centrifugation at 400 × g for 5 min, and resuspending sperm in cleavage medium with 10% PPF [21].
Treatment of experimentally damaged sperm with hydrogen molecule
After IVF using sperm from patients, remaining sperms for discard were used. Each experimentally damaged sperm suspension left in room air at room temperature for > 5 days was divided into three groups as follows: untreated (i.e., control), H2-treated, and N2-treated. During experiments, sperm suspensions were kept in approximately atmospheric O2 concentration to enhance oxidative damage. A sperm suspension of 100 μL on a culture dish was placed into an exposure chamber (volume, approximately 5 L) with H2-mixed gases (5% CO2, 20% O2, 50% H2, and 25% N2) or N2-mixed gases (5% CO2, 20% O2, and 75% N2). After closing the exposure chamber tightly, these concentrations of mixed gases (1 L/min flow rate) were reached within approximately 5 min. To confirm saturation of the sperm suspensions with mixed gases, we monitored H2 and O2 concentrations with needle-type sensors (Unisense, Aarhus N, Denmark). After exposure to mixed gases, each sperm suspension was mixed well by pipetting and a 5–10 μL drop was placed in a counting chamber [22]. The sperm concentration, forward motility sperm rate, non-forward motility sperm rate, and immobility sperm rate were measured visually three times for each sperm suspension.
To evaluate the velocities of motile sperm, a drop of the suspension was placed in a counting chamber and time-lapse movies of sperm movement were recoded using a microscope (Olympus, Tokyo, Japan) for 10 s. Moving images were processed with ImageJ and the CASA (computer assisted sperm analysis) plugin [23]. Forward motility sperm were selected to calculate the velocity.
Treatment of frozen-thawed sperm with hydrogen molecule
Equal amount of freshly prepared sperm suspension from 21 patients in cleavage medium and TEST-yolk buffer (Irvine Scientific, CA, USA) were mixed and dispended into cryotubes. After exposing to nitrogen steam for 5 minutes, cryotubes were stocked in liquid nitrogen [24]. To thaw frozen sperm solution, cryotubes were warmed at 37°C for 5 min, and then each frozen-thawed sperm suspension was dispensed into 4 vials. To prepare the sperm-wash medium containing H2, a 50, 75 or 100% of cleavage medium saturated with H2 was mixed with the medium equilibrated with 5% CO2. Sperm suspensions were washed for 5 minutes with them, and measured their motility.
Fluorescent staining of sperm mitochondria
Mitochondria were co-stained with MitoTracker Green (MTG, 2 μM; Life Technologies, CA, USA) and tetramethylrhodamine methyl ester (TMRM, 2 μM; Life Technologies) for 30 min. MTG fluorescence was independent of the membrane potential; however, TMRM fluorescence was dependent on the membrane potential. MTG and TMRM were visualized with excitation at 488 and 543 nm, and emission at 510 and 565 nm with a laser-scanning confocal microscope (Leica, Wetzlar, Germany). Images were analyzed for the membrane potential of individual sperm using TMRM fluorescence intensity values [25]. Sperm viability was assessed by staining with propidium iodine (PI, 10 μM; Dojindo, Kumamoto, Japan) and Hoechst 33342 (10 μM; Dojindo). Stained sperm were visualized with excitation at 535 and 350 nm, and emission at 617 and 461 nm with a laser-scanning confocal microscope, respectively.
Statistical analysis
All statistical analyses were conducted with JMP (SAS, NC, USA) and essentially performed using one-way ANOVA followed by a post hoc Dunnett's test and two-way ANOVA. Comparison of forward motility before and after treatment of each sperm solution was performed using the paired t-test. Differences between data were considered significant for P-values < 0.05.
Results
Improvement of experimentally damaged sperm motility by treatment with hydrogen molecule
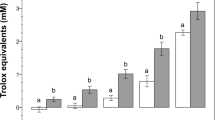
To assess the effect of H2 on sperm motility, we first prepared highly damaged sperms in vitro. Sperm suspensions from patients were left at room temperature for > 5 days, which enhanced oxidative stress and reduced sperm motility. The average of forward motility rate in 35 suspensions was 3.6% [90% confidence interval (CI): 0.6-6.7%]. We then treated the sperm suspensions with mixed gases containing 50% H2 gas (H2-mixed gases) for 40 min and found that the forward motility rate increased significantly (16.8%, 90% CI: 13.8-19.9%) (Figure 1a). On the other hand, the rate did not change (7.7%, 90% CI: 4.6-10.8%) after the sperm suspensions were treated with N2-mixed gases (without H2 gas). At that time, pH was almost equal between suspensions treated with N2- and H2-mixed gases (pH7.3 ± 0.1). Next, we examined the effect of treatment duration using other suspensions with relatively higher motility (n = 12). Both 30 and 60 min treatments with H2-mixed gas significantly improved sperm motility, whereas the 5 min treatment did not (Figure 1b), indicating that H2 treatment for 30 min is sufficient to improve motility.

Effect of H 2 treatment on human sperm motility. Damaged sperm suspensions (n = 35) were untreated or treated with H2- or N2-mixed gases for 40 min (a). Another sperm suspensions (n = 12) were treated with H2-mixed gases for the indicated times (b). Data are represented as means ± standard deviation (SD). ***P < 0.001, versus the untreated sperm suspension.
Effect of the sperm survival rate on H2 treatment
The survival rate of sperm is different in each patient and affects the mobility [26]. We selected other sperm suspensions from 30 patients and examined survival by staining sperm with PI. The average percentage of PI-negative, viable sperm in all suspensions was \( {18.6}_{-18.6}^{+35.0}\% \). We then divided them into two groups based on the percentage of viable sperm: high > 20% (n = 17, \( {35.6}_{-12.0}^{+20.0}\% \)) and low < 20% (n = 13, \( {3.7}_{-3.7}^{+9.3}\% \)). In low-viability group, sperm were immobile before and after treatment with mixed gases. However, we found that H2 treatment stimulated a very sluggish motility of several sperms with pendular movement of their heads around the axis of forward motility in 3 out of 13 suspensions, indicating that almost immobile sperm remaining a weak ability of movement may be activated by H2 treatment. We further investigated the effects of H2 treatment on sperm in high-viability group, in which the average forward motility was 3.0% (90.0% CI: 0.0-10.4%). After treatment with H2-mixed gas, we found that the forward motility in 16 suspensions significantly increased (Figure 2). Sperm motility in 4 suspensions improved with both H2- and N2-mixed gases, except for one suspension, which was not activated by both mixed gases. The average forward motilities in sperm suspensions after treatment with H2- and N2-mixed gases were 11.0% (90% CI: 2.7-20.0%) and 3.6% (90% CI: 0.0-17.6%), respectively. Thus, H2 treatment effectively and significantly improved sperm motility in suspensions with a higher survival rate.

Effect of H 2 treatment on human sperm motility in each suspension. Seventeen sperm suspensions with a sperm viability rate > 20% were used. Sperm motility was determined before and after treatment with H2- or N2-mixed gases for 30 min. Sperm motility in 12 suspensions (dark blue) improved only with H2-mixed gas, in 4 suspensions (light blue) improved with both H2- and N2-mixed gases and in one suspension (pink) was not activated by both mixed gases. P-values were determined using paired t-test.
Effect of H2 treatment on sperm swimming speed
To examine the effect of H2 treatment on sperm swimming speed, we used time-lapse microscopy and analyzed images with sperm analysis computer software, CASA. Ten sperm suspensions, which were randomly selected from 17 suspensions with a higher survival rate used in Figure 2, were treated with mixed gases for 30 min, and traveling distances of only moving sperm were measured for 10 s (Figure 3). No significant difference was observed between control and treated groups, indicating that H2 treatment does not affect sperm swimming speed.

Effect of H 2 treatment on human sperm velocity. Ten sperm suspensions were treated with H2- or N2-mixed gases for 30 min, and time-lapse movies of sperm motility were recorded with a microscope for 10 s. No significant difference was observed between control and treated groups. Data are represented as means ± standard deviation (SD).
Retention time of H2 treatment on sperm motility
The retention time of motile sperm treated with H2 is an important indicator of IVF and ICSI success. After treatment with H2- or N2-mixed gases for 30 min, 10 sperm suspensions were kept at 25°C in room air. After 2.5 h, we found that forward motility in H2 treated suspension was still higher than that before treatment (Figure 4). It is noteworthy that H2 quickly diffuses. Approximately 10 min after placing an aliquot of the H2-treated sperm suspension in room air, the dissolved H2 concentration reached < 0.1% of its saturated concentration, indicating that the higher sperm motility enhanced by H2 treatment can be maintained without H2 for at least 2.5 h.

Retention time of sperm suspensions with improved motility following H 2 treatment. Twelve sperm suspensions were treated with H2- or N2-mixed gases for 30 min (first treatment) and then retreated after 24 h, (second treatment), as indicated by hatching. Before and after the treatment, the suspension was kept at 25°C in room air. The average % of motile sperm per 1 mL of sperm suspension at the indicated times was calculated. Data represent means ± standard deviation (SD). ***P < 0.001; versus suspensions just before treatment (time = 0).
After the first H2 treatment, we further kept a sperm suspension at 25°C in room air for 24 h and found that its motility still remained a level approximately 36% of that of the first treatment (Figure 4). However, it was not significantly higher than that before treatment. We then treated this sperm suspension with H2 for 30 min (second treatment) and kept it at 25°C in room air for 30 min, and found that sperm motility increased again, reaching a level approximately 67% of that of the first treatment.
Enhancement of mitochondrial membrane potential by H2 treatment
Since sperm motility is dependent on ATP content, we hypothesized that the improvement of sperm motility by H2 treatment might be due to changes in mitochondrial function. Therefore, after treatment with H2- or N2-mixed gases for 30 min by the same method described in Figures 1, 2 and 3, we stained sperm with TMRM, a mitochondrial membrane potential-dependent dye, and found that TMRM fluorescence increased (Figure 5), suggesting that H2 treatment may enhance mitochondrial function and sperm motility.

Increase of mitochondrial membrane potential in sperm suspensions by H 2 treatment. Six sperm suspensions were either untreated (a), or treated with H2- or N2-mixed gases (b and c, respectively), and stained with MitoTracker Green (MTG) and TMRM mitochondria- and mitochondrial membrane potential-sensitive fluorescent dyes. Differential interference contrast (DIC) images are also shown. Bars = 10 μm. The fluorescence intensity of each TMRM-stained sperm was semi-quantitatively analyzed by ImageJ (d). Data represent means ± SD. ***P < 0.001, versus the untreated sperm suspension.
Improvement in frozen-thawed sperm motility by treatment with hydrogen molecule
To demonstrate the practical application of H2, we prepared frozen-thawed sperm suspension from each patient, which could be used for infertility treatment. The average forward motility of total 21 suspensions was 37.1% (95%CI: 28.7-45.6). Asthenozoospermia was defined according to the WHO guideline as samples with < 50% progressive sperm motility [20]. Therefore, we divided them into two groups, higher (forward motility ≥ 50%, n = 6) and lower (<50%, n = 15) suspensions, of which the average forward motilities before H2-treatment were 61.3% (95% CI: 50.8-71.8%) and 27.5% (95% CI: 21.7-33.2%), respectively. All suspensions were treated with sperm-wash media containing different concentrations (50, 75, and 100%) of H2. Dunnett's t-test for unpaired values indicated that the motility in suspensions of lower motile, asthenozoospermic sperms significantly increased after treatment with sperm-wash media containing 50% of H2, whereas treatment with 75% and 100% of H2 did not (Figure 6a). H2-treatment did not show any dose-dependency. The motility both in total and suspensions of higher motile, normozoospermic sperms did not significantly increase after H2-treatment. Next, we compared the forward motility before and after treatment of each sperm suspension by using the paired t-test. The forward motility in suspensions of higher motile sperms moderately increased after H2-treatment (Figure 6b). Treatments with 75% of H2 significantly improved the motility of suspensions, whereas treatments with 50% and 100% of H2 did not. On the other hand, we found that the forward motility in suspensions of lower motile sperms apparently increased after treatment with sperm-wash medium containing both 50% and 75% of H2 (Figure 6c), whereas treatment with 100% of H2 did not. These results indicated that H2-treatment effectively and significantly improved the motility of frozen-thawed sperms, especially low motile, asthenozoospermic ones.

Effect of H 2 treatment on human frozen-thawed sperm motility in each suspension. Total frozen-thawed sperm suspensions (n = 21) were divided into 2 groups, those with higher (forward motility ≥ 50%, normozoospermic, n = 6) or lower (<50%, asthenozoospermic, n = 15) motility. Sperm motility was determined before and after treatment with sperm-wash medium containing 50%, 75% and 100% of H2 for 30 min. Data represent means ± SD. *P < 0.05, versus the untreated sperm suspension (a). Comparison of forward motility before and after treatment of each sperm suspension with higher (b) or lower (c) motility. P-values were determined using paired t-test.
Discussion
Since previous studies have shown the balance between ROS and antioxidants to be unequivocally important for a variety of functions in the male reproductive system, we hypothesized that H2 treatment may be protective as a weak scavenger of ROS and may improve sperm motility in vitro. There are two reasons why sperm suspensions left at room temperature for > 5 days were used. Firstly, ejaculated sperm must be kept for 3 days at our clinic for infertility treatments, and remaining sperms for discard were used. Secondly, H2 is stable and must be coaxed with strong catalysts to enter into chemical reactions, and has been treated as an inactive gas in our body, indicating the possibility that the effects of H2 on sperm are not strong. Then, we expected that the using of highly damaged sperms was more sensitive to easily assess the effect of H2 on sperm motility.
The rate of forward motility increased from 3.6% to 16.8% (Figure 1a). The change in motility by H2 treatment was higher than or similar to results previously reported, e.g., 17.95% to 25.1% for treatment with platelet-activating factor [27] and a 21% increase for exogenous pyruvate treatment [28]. Because the increase of forward motility was observed within only 30 min, H2 treatment may stimulate cell signaling and activate mitochondria, but not transcription and translation in sperm. However, it remains to be elucidated whether the stimulatory effects are dependent on a property of H2 as a reductant. Furthermore, H2, but not N2, stimulated sperm motility, indicating that the effect of H2 did not rely on mechanical stimuli.
Effects were evident in almost all sperm suspensions (16 out of 17) with higher survival rates in which an increase of forward motility was observed with H2 treatment (Figure 2). Slight increase of the motility treated with N2 may due to the effect of mixing and shaking of sperm suspension during experimental manipulation [29]. The samples used in this study were collected from various patients with different physiological conditions and genetic backgrounds; therefore, it is possible that the effects of H2 rely on the character of each sperm suspension. The lack of response in forward motility in sperm suspensions with low survival rates indicated that H2 treatment was less effective on complete or nearly complete necrozoospermia. However, we found that H2 treatment stimulated a very sluggish motility of several sperms in 3 out of 13 suspensions with low survival rates, further indicating that H2 is beneficially effective on movement of sperms with both high and low survival rates. The differential effects of H2 treatment may be dependent on various conditions of sperm.
H2 did not enhance the sperm swimming speed (Figure 3), indicating that H2 did not hyperactivate sperm. Hyperactivation is characterized by a more energetic and less symmetric beat of sperm flagella and can be achieved in vitro by seminal plasma removal and incubation of sperm in capacitating medium. However, several reagents, including caffeine, which can stimulate sperm movement, have no effect on sperm velocity [30]. On the other hand, exogenous pyruvate accelerates glycolysis, and stimulates motility and hyperactivation with an increase in intracellular ATP levels [28]. It has been reported that glucose-derived ATP during capacitation involves hyperactivation [31], indicating that H2 treatment does not affect glycolysis.
We found that the higher sperm motility induced by H2 treatment was maintained for 2.5 h, even in the absence of H2 (Figure 4), which is clinically enough time for IVF and ICSI. The decrease in motility after H2 treatment is due to several reasons, including the reduction of intracellular ATP, and oxidative stress of oxygen in the room air [32]. Nevertheless, the motility increased the following day after a second H2 treatment. The increase of motility with second treatment of H2 was still higher than that of N2, indicating that the repeated increase was due to H2, but not mechanical stimuli. The repeated stimulation of sperm is likely to be useful in a clinical setting. Higher variation of the mobility in H2-treated sperm in Figure 4 may be dependent on its higher mobility, because the difference of coefficients of variation between the mobility of H2-treated sperm (0.26 to 0.59%) and that of N2 (0.48 to 0.98%) was very low.
A functional relationship among sperm mitochondrial membrane potential, sperm motility, and fertility potential has been proposed [33]. We found that H2 treatment enhanced mitochondrial membrane potential (Figure 5). Since sperm motility is dependent on ATP content, we speculate that H2 treatment enhances mitochondrial function, promotes ATP production, and then stimulates sperm motility. Indeed, we observed previously that H2 prevented a decrease in cellular levels of ATP synthesized in mitochondria [14]. Precise measurements of both ATP and calcium in sperm are needed before and after treatment with H2.
Finally, we used frozen-thawed sperm suspensions to validate the effects of H2 treatment on the motility of damaged sperm. Frozen sperm suspension is used routinely in assisted reproduction treatment. However, freezing has been reported to cause changes in sperm morphology, including damage to mitochondria. Sperm motility is particularly sensitive to freezing damage [34,35]. Effects were evident in 13 out of 15 suspensions of low motile frozen-thawed sperm (86.7%) in which an increase of forward motility was observed with sperm-wash medium containing 50% of H2 (Figure 6b), indicating that H2 treatment is clinically a potential approach to activate low motility sperm. However, treatment with medium containing higher concentration, 100%, of H2 was not effective, indicating the possibility that very low concentration of O2 in the medium might repress the sperm motility [36]. Further study is needed to elucidate a dose-dependency of H2-treatment.
The fertilization rates after IVF and ICSI using normal sperm are approximately 60% and 70%, respectively [37]. In general, the decision to perform either IVF or ICSI is dependent on sperm quality [38], which is determined by the total number of motile sperm [39]. While the concentration and morphology of ejaculated sperm do not affect ICSI results, the injection of a completely immotile spermatozoon is likely to have a negative effect on fertilization and the pregnancy rate [21,40]. Currently, there is no efficient therapy for asthenozoospermia.
Conclusion
The findings of this study strongly indicate that H2 treatment activates low motility sperms. Importantly, recent studies demonstrated that H2 might have potential for wide use in medical applications as a novel, safe, effective antioxidant with minimal side effects [14-19]. We propose here that H2 is a new promising agent for male infertility treatment. However, to make practical use of H2 treatment, we further need to examine the effects of H2-treated sperm on fertilizing ability, embryonic development and safety for IVF and ICSI in future studies.
Abbreviations
- CI:
-
Confidence interval
- ICSI:
-
Intracytoplasmic sperm injection
- IVF:
-
In vitro fertilization
- MTG:
-
MitoTracker Green
- PPF:
-
Plasma protein fraction
- ROS:
-
Reactive oxygen species
- SD:
-
Standard deviation
- TMRM:
-
Tetramethylrhodamine methyl ester
References
Matzuk MM, Lamb DJ. The biology of infertility: research advances and clinical challenges. Nat Med. 2008;14:1197–213.
Dhillon VS, Shahid M, Husain SA. Associations of MTHFR DNMT3b 4977 bp deletion in mtDNA and GSTM1 deletion, and aberrant CpG island hypermethylation of GSTM1 in non-obstructive infertility in Indian men. Mol Hum Reprod. 2007;13:213–22.
Ruiz-Pesini E, Lapeña AC, Díez-Sánchez C, Pérez-Martos A, Montoya J, Alvarez E, et al. Human mtDNA haplogroups associated with high or reduced spermatozoa motility. Am J Hum Genet. 2000;67:682–96.
Torra R, Sarquella J, Calabia J, Martí J, Ars E, Fernández-Llama P, et al. Prevalence of cysts in seminal tract and abnormal semen parameters in patients with autosomal dominant polycystic kidney disease. Clin J Am Soc Nephrol. 2008;3:790–3.
Gharagozloo P, Aitken RJ. The role of sperm oxidative stress in male infertility and the significance of oral antioxidant therapy. Hum Reprod. 2011;26:1628–40.
Delbarco-Trillo J, Roldan ER. Effects of metabolic rate and sperm competition on the fatty-acid composition of mammalian sperm. J Evol Biol. 2013. doi:10.1111/jeb.12275.
El-Taieb MA, Herwig R, Nada EA, Greilberger J, Marberger M. Oxidative stress and epididymal sperm transport, motility and morphological defects. Eur J Obstet Gynecol Reprod Biol. 2009;144 Suppl 1:S199–203.
Sousa MI, Amaral S, Tavares RS, Paiva C, Ramalho-Santos J. Concentration-dependent Sildenafil citrate (Viagra) effects on ROS production, energy status, and human sperm function. Syst Biol Reprod Med. 2014;60:72–9.
Eskenazi B, Kidd SA, Marks AR, Sloter E, Block G, Wyrobek AJ. Antioxidant intake is associated with semen quality in healthy men. Hum Reprod. 2005;20:1006–12.
Schmid TE, Eskenazi B, Marchetti F, Young S, Weldon RH, Baumgartner A, et al. Micronutrients intake is associated with improved sperm DNA quality in older men. Fertil Steril. 2012;98:1130–7.
Talevi R, Barbato V, Fiorentino I, Braun S, Longobardi S, Gualtieri R. Protective effects of in vitro treatment with zinc, d-aspartate and coenzyme q10 on human sperm motility, lipid peroxidation and DNA fragmentation. Reprod Biol Endocrinol. 2013;11:81.
Condorelli RA, La Vignera S, Bellanca S, Vicari E, Calogero AE. Myoinositol: does it improve sperm mitochondrial function and sperm motility? Urology. 2012;79:1290–5.
Ebner T, Tews G, Mayer RB, Ziehr S, Arzt W, Costamoling W, et al. Pharmacological stimulation of sperm motility in frozen and thawed testicular sperm using the dimethylxanthine theophylline. Fertil Steril. 2011;96:1331–6.
Ohsawa I, Ishikawa M, Takahashi K, Watanabe M, Nishimaki K, Yamagata K, et al. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat Med. 2007;13:688–94.
Hayashida K, Sano M, Ohsawa I, Shinmura K, Tamaki K, Kimura K, et al. Inhalation of hydrogen gas reduces infarct size in the rat model of myocardial ischemia-reperfusion injury. Biochem Biophys Res Commun. 2008;373:30–5.
Fukuda K, Asoh S, Ishikawa M, Yamamoto Y, Ohsawa I, Ohta S. Inhalation of hydrogen gas suppresses hepatic injury caused by ischemia/reperfusion through reducing oxidative stress. Biochem Biophys Res Commun. 2007;361:670–4.
Oharazawa H, Igarashi T, Yokota T, Fujii H, Suzuki H, Machide M, et al. Protection of the retina by rapid diffusion of hydrogen: administration of hydrogen-loaded eye drops in retinal ischemia-reperfusion injury. Invest Ophthalmol Vis Sci. 2010;51:487–92.
Cardinal JS, Zhan J, Wang Y, Sugimoto R, Tsung A, McCurry KR, et al. Oral hydrogen water prevents chronic allograft nephropathy in rats. Kidney Int. 2010;77:101–9.
Terasaki Y, Ohsawa I, Terasaki M, Takahashi M, Kunugi S, Dedong K, et al. Hydrogen therapy attenuates irradiation-induced lung damage by reducing oxidative stress. Am J Physiol Lung Cell Mol Physiol. 2011;301:L415–26.
World Health Organization. WHO laboratory manual for the examination and processing of human semen. 5th ed. Geneva: WHO Press; 2010.
Liu J, Nagy Z, Joris H, Tournaye H, Devroey P, Van Steirteghem AC. Intracytoplasmic sperm injection does not require special treatment of the spermatozoa. Hum Reprod. 1994;9:1127–30.
Makler A. The improved 10 mic. chamber for rapid sperm count and motility evaluation. Fertil Steril. 1980;33:337–8.
ESHRE Andrology Special Interest Group. Guidelines on the application of CASA technology in the analysis of spermatozoa. Hum Reprod. 1998;13:142–5.
Zavos PM, Sofikitis N, Toda T, Miyagawa I. Improvements in qualitative characteristics of cryopreserved human spermatozoa following recovery via the SpermPrep II filtration method. Tohoku J Exp Med. 1991;165:283–90.
Marchetti C, Jouy N, Leroy-Martin B, Defossez A, Formstecher P, Marchetti P. Comparison of four fluorochromes for the detection of the inner mitochondrial membrane potential in human spermatozoa and their correlation with sperm motility. Hum Reprod. 2004;19:2267–76.
Angelopoulou R, Lavranos G, Manolakou P. ROS in the aging male: model diseases with ROS-related pathophysiology. Reprod Toxicol. 2009;28:167–71.
Esmaeilpour T, Zarei MR, Bahmanpour S, Aliabadi E, Hosseini A, Jaberipour M. Effect of follicular fluid and platelet-activating factor on lactate dehydrogenase C expression in human asthenozoospermic samples. Iran J Med Sci. 2014;39:20–8.
Hereng TH, Elgstøen KB, Cederkvist FH, Eide L, Jahnsen T, Skålhegg BS, et al. Exogenous pyruvate accelerates glycolysis and promotes capacitation in human spermatozoa. Hum Reprod. 2011;26:3249–63.
Makler A, Jakobi P. Effects of shaking and centrifugation on human sperm motility. Arch Androl. 1981;7:21–6.
Moussa MM. Caffeine and sperm motility. Fertil Steril. 1983;39:845–8.
Williams AC, Ford WC. The role of glucose in supporting motility and capacitation in human spermatozoa. J Androl. 2001;22:680–95.
Luconi M, Forti G, Baldi E. Pathophysiology of sperm motility. Front Biosci. 2006;11:1433–47.
Kasai T, Ogawa K, Mizuno K, Nagai S, Uchida Y, Ohta S, et al. Relationship between sperm mitochondrial membrane potential, sperm motility, and fertility potential. Asian J Androl. 2002;4:97–103.
O'Connell M, McClure N, Lewis SE. The effects of cryopreservation on sperm morphology, motility and mitochondrial function. Hum Reprod. 2002;17:704–9.
Boitrelle F, Albert M, Theillac C, Ferfouri F, Bergere M, Vialard F, et al. Cryopreservation of human spermatozoa decreases the number of motile normal spermatozoa, induces nuclear vacuolization and chromatin decondensation. J Androl. 2012;33:1371–8.
NEVO AC. Dependence of sperm motility and respiration on oxygen concentration. J Reprod Fertil. 1965;9:103–7.
Check JH, Bollendorf A, Wilson C, Summers-Chase D, Horwath D, Yuan W. A retrospective comparison of pregnancy outcome following conventional oocyte insemination vs intracytoplasmic sperm injection for isolated abnormalities in sperm morphology using strict criteria. J Androl. 2007;28:607–12.
Vellani E, Colasante A, Mamazza L, Minasi MG, Greco E, Bevilacqua A. Association of state and trait anxiety to semen quality of in vitro fertilization patients: a controlled study. Fertil Steril. 2013;99:1565–72.
Stalf T, Mehnert C, Hajimohammad A, Manolopoulos K, Shen Y, Schuppe HC, et al. Influence of motility and vitality in intracytoplasmic sperm injection with ejaculated and testicular sperm. Andrologia. 2005;37:125–30.
Liu J, Nagy Z, Joris H, Tournaye H, Smitz J, Camus M, et al. Analysis of 76 total fertilization failure cycles out of 2732 intracytoplasmic sperm injection cycles. Hum Reprod. 1995;10:2630–6.
Acknowledgments
The work was funded by research funding (KAKENHI 30343586) from the Ministry of Education, Culture, Sports, Science and Technology (MEXT) of Japan. We are greatful to Naoki Nakayama, Kayoko Ikegami, Aya Nakanishi, Mutsumi Abe, and Hitomi Watanabe (Yamashita Shonan Yume Clinic) for collection of samples.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KN involved in conceiving and designing the study, analyzing and interpreting the data; NY in provision of materials, patients and resources; YN in technical support; IO in organization of this study and writing the article. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Nakata, K., Yamashita, N., Noda, Y. et al. Stimulation of human damaged sperm motility with hydrogen molecule. Med Gas Res 5, 2 (2015). https://doi.org/10.1186/s13618-014-0023-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13618-014-0023-x