
Abstract
Background
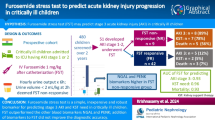
Furosemide responsiveness (FR) is determined by urine output after furosemide administration and has recently been evaluated as a furosemide stress test (FST) for predicting severe acute kidney injury (AKI) progression. Although a standardized furosemide dose is required for FST, variable dosing is typically employed based on illness severity, including renal dysfunction in the clinical setting. This study aimed to evaluate whether FR with different furosemide doses can predict AKI progression. We further evaluated the combination of an AKI biomarker, plasma neutrophil gelatinase-associated lipocalin (NGAL), and FR for predicting AKI progression.
Results
We retrospectively analyzed 95 patients who were treated with bolus furosemide in our medical–surgical intensive care unit. Patients who had already developed AKI stage 3 were excluded. A total of 18 patients developed AKI stage 3 within 1 week. Receiver operating curve analysis revealed that the area under the curve (AUC) values of FR and plasma NGAL were 0.87 (0.73–0.94) and 0.80 (0.67–0.88) for AKI progression, respectively. When plasma NGAL level was < 142 ng/mL, only one patient developed stage 3 AKI, indicating that plasma NGAL measurements were sufficient to predict AKI progression. We further evaluated the performance of FR in 51 patients with plasma NGAL levels > 142 ng/mL. FR was associated with AUC of 0.84 (0.67–0.94) for AKI progression in this population with high NGAL levels.
Conclusions
Although different variable doses of furosemide were administered, FR revealed favorable efficacy for predicting AKI progression even in patients with high plasma NGAL levels. This suggests that a combination of FR and biomarkers can stratify the risk of AKI progression in a clinical setting.
Similar content being viewed by others

Background
Acute kidney injury (AKI) is highly prevalent in an intensive care unit (ICU) and is associated with significant morbidity and mortality [1,2,3]. Severe AKI has an unacceptably high mortality, especially when renal replacement therapy (RRT) is required [4,5,6]. Prediction of AKI progression from a mild to severe form is clinically important for several reasons. First, the early initiation of RRT can be supported for highly possible AKI progression, although there is currently no consensus regarding the timing of initiating RRT [7, 8]. Second, AKI diagnosis is based on the changes of serum creatinine concentration, but it is well known that changes in serum creatinine levels are delayed. Although the Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guideline for Acute Kidney Injury suggests considering an invasive diagnostic workup (stage 1) along with ICU admission (stage 2) for AKI management based on AKI severity determined by serum creatinine [9], establishing a triage decision for management and prevention of AKI progression is difficult with a late marker of serum creatinine. Finally, identifying possible AKI progressors may contribute to the development of novel drugs for AKI by reducing inappropriate enrollment of patients with mild AKI who recover spontaneously.
To date, multiple biomarkers, such as plasma neutrophil gelatinase-associated lipocalin (NGAL), L-type fatty acid binding protein (L-FABP), interleukin (IL)-18, and tissue inhibitor of metalloproteinases (TIMP-2)/insulin-like growth factor-binding protein 7 (IGFBP7), have been developed [10,11,12,13,14]. Moreover, urinary NGAL and L-FABP can reportedly discriminate between prerenal and renal AKI [15,16,17] and TIMP-2/IGFBP7 can predict AKI progression [18, 19].
Furosemide is excreted from the blood into the urine through the proximal tubules by the human organic anion transporter and inhibits luminal sodium transporters in the loop of Henle from the urinal lumen [20]. If furosemide administration increases the urine output, it could be assumed that the tubules are functional. Koyner et al. [21] recently demonstrated that the 2-h urine output after a standardized high-dose intravenous furosemide injection (furosemide stress test; FST) was sensitive in predicting AKI progression to stage 3 in patients with early AKI.
To better stratify the risk of AKI progression, a combination of renal functional and damage biomarkers is recommended [22]. However, there are no reports in the literature that have examined the combination of functional and damage biomarkers for predicting AKI progression. In this study, we retrospectively evaluated the combination of AKI biomarkers and urine output in response to the administration of bolus furosemide for stratifying the risk of AKI progression in critically ill patients.
Methods
Definition
Furosemide responsiveness (FR) is newly defined as total urine output in 2 h (mL) divided by the dose of bolus furosemide (mg) administered. A previous study reported that the urine output within the first 2 h after a standardized dose of furosemide administration provided the highest prediction of the development of severe AKI [23]. We reviewed furosemide dose and hourly urine output using ICU medical charts and determined FR of each patient. The timing and dose of furosemide administration were determined by the physician involved. In our regular clinical practice, furosemide dose was decided based on body weight, volume status, cardiac function, serum creatinine concentration at the time of furosemide administration, and presence of complications of chronic kidney disease (CKD). All patients finally enrolled in this study had an indwelling catheter, and hourly urine output could be accurately measured.
Study design
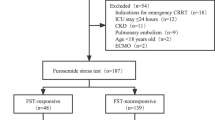
This study is a subanalysis of our prospective observational studies [24,25,26]. The cohort in this study was selected from these previous prospective observational studies conducted in the medical–surgical mixed ICU at the University of Tokyo Hospital. In previous studies, we measured the AKI biomarkers of plasma NGAL, urinary L-FABP, and urinary N-acetyl-β-d-glucosaminidase (NAG) and evaluated the association with AKI biomarkers and AKI progression within 1 week. Among 523 adult critically ill patients enrolled, 153 were retrospectively identified to have received furosemide on the same day that the above-mentioned AKI biomarkers were measured. Finally, 95 patients were eligible for analysis after excluding 33 patients who were administered continuous intravenous furosemide infusion instead of a bolus and 25 patients who had already progressed to AKI stage 3 at the time of ICU admission (Fig. 1). Volume depletion was evaluated by the clinical context, physical signs, and findings on cardiac ultrasound examination in all 95 patients. The study protocol was approved by the institutional review board of the University of Tokyo and adhered to the Declaration of Helsinki. Patient informed consent was obtained at the time of ICU admission. The following clinical variables during the ICU and hospital stay were evaluated: age, sex, weight, causes of ICU admission, acute physiology and chronic health evaluation II score [27], and the length of ICU and hospital stay.

Study flow diagram
Assessment of kidney function
Baseline serum creatinine level was defined as the last outpatient value within 6 months prior to ICU admission. If the creatinine level prior to admission was not known, the baseline value was defined as the lowest among creatinine values in hospital but prior to ICU admission, the last level before hospital discharge, and the estimated value using the Modification of Diet in Renal Disease equation at the lower end of the normal range [28]. The definition and classification of AKI were made according to the KDIGO Clinical Practice Guideline for Acute Kidney Injury [29].
Measurement of AKI biomarkers
Urine and plasma samples were collected at the time of ICU admission and were frozen at − 80 °C within 1 h of collection. As urine output was measured hourly by an indwelling catheter, we could obtain a fresh urine sample that was collected within 1 h previously. The plasma NGAL level was determined using the Triage NGAL Device (AlereMedical, San Diego, CA, USA). Urinary L-FABP level was measured using commercially available enzyme-linked immunosorbent assay kits (Human L-FABP Assay Kit; CMIC Co. Ltd., Tokyo, Japan). Urinary NAG level was measured at the University of Tokyo Hospital Clinical Laboratory using the 4-HP-NAG substrate method (L-Type NAG; Wako Pure Chemical Industries Ltd., Osaka, Japan). Urinary L-FABP and NAG level measurements were evaluated by adjusting with urine creatinine concentration [11, 30].
Statistical analyses
Data are presented as median (interquartile range). Continuous variables were compared using Wilcoxon rank-sum tests if they were non-normally distributed. Categorical variables were compared using the Pearson Chi-square or Fisher exact test. The urinary and plasma biomarker performance was ascertained using a receiver operating characteristic (ROC) curve analysis. The optimal cutoff values were acquired using the Youden index (sensitivity + specificity − 1), which is a common summary measure of the ROC curve representing the maximum potential effectiveness of a marker [31]. Comparisons of the ROC curves were performed as previously reported [30, 32]. All analyses were performed using a statistical analysis software (JMP ver. 11.2; SAS Institute Inc., Cary, NC). A conventional criterion of an α level of 0.05 was used to assess statistical significance.
Results
Patient characteristics and AKI progression to AKI stage 3
Characteristics of all 95 patients studied are presented in Table 1. Among these, 51 patients (54%) were diagnosed with AKI at the time of furosemide administration; 34 were diagnosed with AKI stage 1 (36%) and 17 with AKI stage 2 (18%). Within 1 week following furosemide administration, 18 patients progressed to AKI stage 3 (Fig. 1). Among this, 10 patients had progressed from AKI stage 1 and four patients from stage 2. Four patients did not have AKI at the time of furosemide administration.
Biomarkers, FR, and AKI stages at 1 week
First, the association between progression to AKI stage 3 after 1 week with FR and AKI biomarkers was evaluated. FR and plasma NGAL level showed significant differences between the AKI progression group (from any stage to stage 3) and the non-progression group (Fig. 2). When weight-adjusted FR is defined as the total urine output in 2 h divided by furosemide dose per kilogram body weight (mg/kg), weight-adjusted FR showed a significant difference between the groups (Additional file 1: Figure S1). Measurement of urinary L-FABP and NAG levels could not significantly differentiate AKI progression to stage 3. The ROC analysis demonstrated that FR, weight-adjusted FR, and plasma NGAL could significantly predict AKI progression to stage 3; in contrast, urinary L-FABP and NAG levels could not predict AKI progression (Table 2). Similar results were obtained when a composite outcome of AKI stage 3 or death within 1 week after furosemide administration was used (Table 2; Figs. 2, 3; Additional file 1: Figure S2).

Biomarkers and furosemide responsiveness (FR) in AKI progression. The boxplots show the differences in the AKI biomarkers and FR between patients a without and with the progression to AKI stage 3 and b without and with the progression to AKI stage 3 or death within 1 week. *p < 0.01

Prediction of AKI progression by biomarkers and furosemide responsiveness (FR). Receiver operating characteristic curves (ROC) in a progression to AKI stage 3 and b progression to AKI stage 3 or death at 1 week. NGAL, neutrophil gelatinase-associated lipocalin; L-FABP, L-type fatty acid binding protein; NAG, N-acetyl-β-d-glucosaminidase; FR, furosemide responsiveness
FR for the prediction of AKI progression in the population with high NGAL levels
Among the 95 enrolled patients, 51 were diagnosed with AKI of different stages at the time of furosemide administration. For predicting AKI progression to stage 3, the plasma NGAL level measured at the time of furosemide administration showed a good AUC in the ROC analysis, 0.79 (0.68–0.86) with a cutoff value of 142 ng/mL, as determined by the Youden index (sensitivity, 72.1%; specificity, 79.4%). When the plasma NGAL level was < 142 ng/mL, only one patient progressed to AKI stage 3, indicating that plasma NGAL level alone was sufficient to predict AKI progression to stage 3. Therefore, we further evaluated the efficacy of FR in predicting AKI progression in patients with plasma NGAL levels > 142 ng/mL. Among the 51 patients with plasma NGAL levels > 142 ng/mL at the time of furosemide administration, 17 progressed to AKI stage 3 (eight patients required RRT) and four died (Fig. 4). FR was associated with AUCs of 0.84 (0.67–0.94) and 0.88 (0.70–0.96) to predict the development of AKI stage 3 and the composite outcome of AKI stage 3 progression or death. Cutoff values of FR for both AKI progression to stage 3 and the composite outcome as determined by Youden index were 3.9 mL/mg/2 h.

Distribution of ICU patients determined by the plasma NGAL level. NGAL, neutrophil gelatinase-associated lipocalin
The characteristics of the population with higher NGAL levels divided by FR positive (n = 36) or FR negative (n = 15) with the cutoff value of 3.9 mL/mg/2 h described above are shown in Table 3. The serum creatinine levels at the time of hospitalization and furosemide administration were higher in the FR-positive patients compared with the FR-negative patients. The proportion of patients at each stage of AKI at the time of ICU admission and furosemide administration, as well as the plasma NGAL level measured at the time of furosemide administration, were not significantly different. A higher dose of furosemide was administered to patients who were FR negative than to those who were FR positive. Among the 15 patients who were FR negative, 13 (86.7%) progressed to AKI stage 3, while six (40%) required RRT. On the other hand, among 36 patients who were FR positive, only four (11%) progressed to AKI stage 3 and two (5.6%) required RRT (Table 4).
Discussion
AKI progression frequently occurs in ICU in the context of multiple organ failure [33] and is significantly associated with high mortality in different cohorts of ICU and in patients who have undergone cardiac surgery and those with cardiorenal syndrome [10, 34, 35]. The identification of the potential AKI progression may allow us to initiate early interventions (e.g., more invasive monitoring and RRT) before the development of life-threatening complications. In addition, with the likely development of novel therapies for AKI, an accurate prediction of AKI progression may help to determine patients at the highest risk and those most likely to benefit from such treatment. Several emerging AKI biomarkers, including TIMP-2/IGFBP-7, IL-18, and plasma NGAL, have been demonstrated to predict AKI progression [10, 34]. In particular, TIMP-2/IGFBP-7 was validated for early AKI risk stratification in critically ill patients in multicenter studies [18, 36, 37]. These cell-cycle arrest biomarkers are expected to help in the early detection of patients at risk of AKI in various clinical settings. Recently, FST was suggested to be a significant predictor of progression to AKI stage 3 in patients with AKI stage 1 or 2 [23]. Moreover, Koyner et al. [21] reported a superior efficacy of FST than urinary AKI biomarkers for the prediction of AKI progression. This study demonstrates that both FR and plasma NGAL levels could successfully predict AKI progression as shown by previous studies described above. The novel findings of this study are as follows: (1) FST, as described originally, requires a standardized intravenous furosemide dose of 1 mg/kg. However, this study demonstrated that response to a variable dose of frusemide could also predict AKI progression under actual clinical conditions, when different doses of furosemide were chosen based on patient condition; (2) FR could predict AKI progression in patients with high plasma NGAL levels, while few patients with low plasma NGAL levels exhibited AKI progression. These results indicate that both functional (furosemide response) and structural evaluations (plasma NGAL level) in AKI may be helpful for the prediction of AKI progression.
As described above, FR (mL/mg/2 h) in this study was determined by the 2-h total urine output (mL) following furosemide administration divided by the dose of furosemide (mg). It is well known that the effect of loop diuretics is dose dependent [38]. The delivery of furosemide to the thick ascending limb of the loop of Henle depends on the secretion from the proximal tubular epithelial cells. Because the rate of delivery to the site of action is the most important determining factor for natriuresis induced by furosemide administration, FR in this study might reflect the proximal tubule function even with variable furosemide doses. In the studies involving normal healthy subjects, 10 mg furosemide produced diuresis and 40 mg intravenously administered was associated with the maximal effect. In oliguric AKI, the dose with the maximum effect of furosemide is assumed to be as high as 500 mg [39]. In this study, the furosemide dose ranged from 10 to 340 mg. Our findings provide useful information to clinicians as FR calculated with different doses of furosemide can be used to predict AKI progression. This is because furosemide dosing should be individually determined based on patient condition in a clinical setting.
Another important issue regarding the physiology of furosemide is serum albumin concentration. Hypoalbuminemia results in lower oncotic pressure and fluid shift to the interstitial compartment, which may depress fluid excretion by the kidneys. Previously, colloid infusion with loop diuretics was shown to increase urine output and lower net fluid balance in critically ill patients with hypoalbuminemia and fluid overload [40, 41]. In contrast, despite a possible role of albumin in furosemide-induced diuresis, serum albumin levels were not different between the FR-positive and FR-negative patients in the population with high NGAL levels. Thus, serum albumin levels seemed to have little impact on the response to furosemide.
An ideal AKI biomarker should aid in determining the degree of damage and functional changes in the kidney and help to adequately manage AKI and initiate RRT when needed [22]. Emerging AKI biomarkers, including NGAL, L-FABP, IL-18, and TIMP-2/IGFBP7, are reported to be useful for the early detection of AKI and prediction of progression because AKI impacts the metabolism and excretion of these biomarkers that are produced, excreted, or reabsorbed in the renal tubules [14, 18, 37, 42,43,44,45,46,47]. However, these biomarkers may be insufficient for the measurement of residual function of the kidney because they monitor damage but not severity of impairment of kidney function [48]. Therefore, we suggest a two-step approach for the prediction of AKI progression: (1) the evaluation of structural damage by plasma NGAL and (2) the subsequent functional assessment by FR (Fig. 5).

Algorithm of plasma NGAL level and furosemide responsiveness for AKI progression
This study has several limitations. First, this was a retrospective observational study and the number of patients included in this single-center study was small. Among 523 patients, only 153 were analyzed because furosemide administration was determined based on the clinical situation. In addition, plasma NGAL levels had to be measured on the same day as furosemide administration for study enrollment. Although we showed the significance of FR for predicting severe AKI progression, unmeasured factors could have biased our results. Therefore, inherent bias should be carefully considered while interpreting this study. However, it should be stated that the preliminary findings of this study may suggest that a novel approach combining structural damage makers and functional evaluation may be useful for predicting AKI progression. Future multicenter prospective studies with larger cohorts should be conducted to validate our strategy and findings. Second, the plasma NGAL cutoff level in this study was retrospectively determined and could not be extrapolated in other cohorts. A prospective cohort analysis is required to confirm our results. Third, furosemide was administered based on clinician judgment and criteria for administration depended on clinicians’ decision and the criteria to administer furosemide were vague. Although 1 mg/kg furosemide was used in the original paper for FST [21, 23], furosemide dose administered in our study was different in each patient and was determined by the physician based on the patient’s condition. Again, a prospective study with a predefined furosemide administration protocol is necessary. Finally, we did not evaluate the long-term outcomes in this study. Recent clinical reports demonstrate that AKI has a significant impact on mortality and the progression of kidney disease (e.g., chronic kidney disease or end-stage kidney disease) [49,50,51]. Further investigation is necessary to determine whether the combination of FR and AKI biomarkers is significant for predicting long-term AKI-related outcomes.
Conclusions
This retrospective study demonstrated that FR and plasma NGAL may be significant predictors of severe AKI progression in general ICU patients. In addition, FR could predict AKI progression even in patients with high NGAL values, indicating that the sequential evaluation with FR and plasma NGAL could identify patients at a high risk for the development of severe AKI. Of note, identifying high-risk patients may enable to decrease potential adverse effects of furosemide. Finally, careful consideration is necessary before applying the findings of this small retrospective study to clinical practice.
Abbreviations
- AKI:
-
acute kidney injury
- AUC:
-
area under the curve
- FR:
-
furosemide responsiveness
- FST:
-
furosemide stress test
- ICU:
-
intensive care unit
- IGFBP7:
-
insulin-like growth factor-binding protein 7
- IL-18:
-
interleukin 18
- KDIGO:
-
Kidney Disease: Improving Global Outcomes
- L-FABP:
-
L-type fatty acid binding protein
- NAG:
-
N-acetyl-β-d-glucosaminidase
- NGAL:
-
neutrophil gelatinase-associated lipocalin
- ROC:
-
receiver operating characteristic
- RRT:
-
renal replacement therapy
- TIMP-2:
-
tissue inhibitor of metalloproteinases
References
Bellomo R, Kellum JA, Ronco C. Acute kidney injury. Lancet. 2012;380:756–66.
Rewa O, Bagshaw SM. Acute kidney injury-epidemiology, outcomes and economics. Nat Rev Nephrol. 2014;10:193–207.
Singbartl K, Kellum JA. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int. 2012;81:819–25.
Iwagami M, Yasunaga H, Noiri E, Horiguchi H, Fushimi K, Matsubara T, et al. Current state of continuous renal replacement therapy for acute kidney injury in Japanese intensive care units in 2011: analysis of a national administrative database. Nephrol Dial Transplant. 2015;30:988–95.
Vesconi S, Cruz DN, Fumagalli R, Kindgen-Milles D, Monti G, Marinho A, et al. Delivered dose of renal replacement therapy and mortality in critically ill patients with acute kidney injury. Crit Care. 2009;13:R57.
RENAL Replacement Therapy Study Investigators, Bellomo R, Cass A, Cole L, Finfer S, Gallagher M, et al. Intensity of continuous renal-replacement therapy in critically ill patients. N Engl J Med. 2009;361:1627–38.
Gibney N, Hoste E, Burdmann EA, Bunchman T, Kher V, Viswanathan R, et al. Timing of initiation and discontinuation of renal replacement therapy in AKI: unanswered key questions. Clin J Am Soc Nephrol. 2008;3:876–80.
Vaara ST, Reinikainen M, Wald R, Bagshaw SM, Pettila V. Timing of RRT based on the presence of conventional indications. Clin J Am Soc Nephrol. 2014;9:1577–85.
Kidney Disease: Improving Global Outcomes (KDIGO) Work Group. KDIGO clinical practice guideline for acute kidney injury. Dialysis interventions for treatment of AKI. Section 3. Prevention and treatment of AKI. Kidney Int Suppl. 2012;2:37–68.
Koyner JL, Garg AX, Coca SG, Sint K, Thiessen-Philbrook H, Patel UD, et al. Biomarkers predict progression of acute kidney injury after cardiac surgery. J Am Soc Nephrol. 2012;23:905–14.
Koyner JL, Parikh CR. Clinical utility of biomarkers of AKI in cardiac surgery and critical illness. Clin J Am Soc Nephrol. 2013;8:1034–42.
Arthur JM, Hill EG, Alge JL, Lewis EC, Neely BA, Janech MG, et al. Evaluation of 32 urine biomarkers to predict the progression of acute kidney injury after cardiac surgery. Kidney Int. 2014;85:431–8.
Parikh CR, Thiessen-Philbrook H, Garg AX, Kadiyala D, Shlipak MG, Koyner JL, et al. Performance of kidney injury molecule-1 and liver fatty acid-binding protein and combined biomarkers of AKI after cardiac surgery. Clin J Am Soc Nephrol. 2013;8:1079–88.
Charlton JR, Portilla D, Okusa MD. A basic science view of acute kidney injury biomarkers. Nephrol Dial Transplant. 2014;29:1301–11.
Doi K, Katagiri D, Negishi K, Hasegawa S, Hamasaki Y, Fujita T, et al. Mild elevation of urinary biomarkers in prerenal acute kidney injury. Kidney Int. 2012;82:1114–20.
Singer E, Elger A, Elitok S, Kettritz R, Nickolas TL, Barasch J, et al. Urinary neutrophil gelatinase-associated lipocalin distinguishes pre-renal from intrinsic renal failure and predicts outcomes. Kidney Int. 2011;80:405–14.
Nejat M, Pickering JW, Devarajan P, Bonventre JV, Edelstein CL, Walker RJ, et al. Some biomarkers of acute kidney injury are increased in pre-renal acute injury. Kidney Int. 2012;81:1254–62.
Kashani K, Al-Khafaji A, Ardiles T, Artigas A, Bagshaw SM, Bell M, et al. Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Crit Care. 2013;17:R25.
Vijayan A, Faubel S, Askenazi DJ, Cerda J, Fissell WH, Heung M, et al. Clinical use of the urine biomarker [TIMP-2] × [IGFBP7] for acute kidney injury risk assessment. Am J Kidney Dis. 2016;68:19–28.
Huang X, Dorhout Mees EJ, Vos PF, Hamza S, Braam B. Everything we always wanted to know about furosemide but were afraid to ask. Am J Physiol Renal Physiol. 2016. https://doi.org/10.1152/ajprenal.00476.2015.
Koyner JL, Davison DL, Brasha-Mitchell E, Chalikonda DM, Arthur JM, Shaw AD, et al. Furosemide stress test and biomarkers for the prediction of AKI severity. J Am Soc Nephrol. 2015;26:2023–31.
Murray PT, Mehta RL, Shaw A, Ronco C, Endre Z, Kellum JA, et al. Potential use of biomarkers in acute kidney injury: report and summary of recommendations from the 10th Acute Dialysis Quality Initiative consensus conference. Kidney Int. 2014;85:513–21.
Chawla LS, Davison DL, Brasha-Mitchell E, Koyner JL, Arthur JM, Shaw AD, et al. Development and standardization of a furosemide stress test to predict the severity of acute kidney injury. Crit Care. 2013;17:R207.
Isshiki R, Asada T, Sato D, Sumida M, Hamasaki Y, Inokuchi R, et al. Association of urinary neutrophil gelatinase-associated lipocalin with long-term renal outcomes in ICU survivors: a retrospective observational cohort study. Shock. 2016;46:44–51.
Hayase N, Yamamoto M, Asada T, Isshiki R, Yahagi N, Doi K. Association of heart rate with N-terminal pro-B-type natriuretic peptide in septic patients: a prospective observational cohort study. Shock. 2016;46:642–8.
Asada T, Aoki Y, Sugiyama T, Yamamoto M, Ishii T, Kitsuta Y, et al. Organ system network disruption in nonsurvivors of critically ill patients. Crit Care Med. 2016;44:83–90.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13:818–29.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
The Kidney Disease: Improving Global Outcomes (KDIGO) Work Group. KDIGO clinical practice guideline for acute kidney injury. Dialysis interventions for treatment of AKI. Section 2. AKI Definition. Kidney Int Supple. 2012;2:19–36.
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–45.
Ruopp MD, Perkins NJ, Whitcomb BW, Schisterman EF. Youden Index and optimal cut-point estimated from observations affected by a lower limit of detection. Biom J. 2008;50:419–30.
Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148:839–43.
Russell JA, Singer J, Bernard GR, Wheeler A, Fulkerson W, Hudson L, et al. Changing pattern of organ dysfunction in early human sepsis is related to mortality. Crit Care Med. 2000;28:3405–11.
Doi K, Noiri E, Nangaku M, Yahagi N, Jayakumar C, Ramesh G. Repulsive guidance cue semaphorin 3A in urine predicts the progression of acute kidney injury in adult patients from a mixed intensive care unit. Nephrol Dial Transplant. 2014;29:73–80.
Chen C, Yang X, Lei Y, Zha Y, Liu H, Ma C, et al. Urinary biomarkers at the time of AKI diagnosis as predictors of progression of AKI among patients with acute cardiorenal syndrome. Clin J Am Soc Nephrol. 2016;11:1536–44.
Hoste EA, McCullough PA, Kashani K, Chawla LS, Joannidis M, Shaw AD, et al. Derivation and validation of cutoffs for clinical use of cell cycle arrest biomarkers. Nephrol Dial Transplant. 2014;29:2054–61.
Bihorac A, Chawla LS, Shaw AD, Al-Khafaji A, Davison DL, Demuth GE, et al. Validation of cell-cycle arrest biomarkers for acute kidney injury using clinical adjudication. Am J Respir Crit Care Med. 2014;189:932–9.
Brater DC, Day B, Burdette A, Anderson S. Bumetanide and furosemide in heart failure. Kidney Int. 1984;26:183–9.
Brater D, Voelker J. Use of diuretics in patients with renal disease. New York: Churchill Livingstone; 1987.
Martin GS, Moss M, Wheeler AP, Mealer M, Morris JA, Bernard GR. A randomized, controlled trial of furosemide with or without albumin in hypoproteinemic patients with acute lung injury. Crit Care Med. 2005;33:1681–7.
Cordemans C, De Laet I, Van Regenmortel N, Schoonheydt K, Dits H, Martin G, et al. Aiming for a negative fluid balance in patients with acute lung injury and increased intra-abdominal pressure: a pilot study looking at the effects of PAL-treatment. Ann Intensive Care. 2012;2:S15.
Waring WS, Moonie A. Earlier recognition of nephrotoxicity using novel biomarkers of acute kidney injury. Clin Toxicol. 2011;49:720–8.
Goetz DH, Willie ST, Armen RS, Bratt T, Borregaard N, Strong RK. Ligand preference inferred from the structure of neutrophil gelatinase associated lipocalin. Biochemistry. 2000;39:1935–41.
Cai L, Rubin J, Han W, Venge P, Xu S. The origin of multiple molecular forms in urine of HNL/NGAL. Clin J Am Soc Nephrol. 2010;5:2229–35.
Yamamoto T, Noiri E, Ono Y, Doi K, Negishi K, Kamijo A, et al. Renal L-type fatty acid-binding protein in acute ischemic injury. J Am Soc Nephrol. 2007;18:2894–902.
Doi K, Noiri E, Maeda-Mamiya R, Ishii T, Negishi K, Hamasaki Y, et al. Urinary L-type fatty acid-binding protein as a new biomarker of sepsis complicated with acute kidney injury. Crit Care Med. 2010;38:2037–42.
Kuwabara T, Mori K, Mukoyama M, Kasahara M, Yokoi H, Saito Y, et al. Urinary neutrophil gelatinase-associated lipocalin levels reflect damage to glomeruli, proximal tubules, and distal nephrons. Kidney Int. 2009;75:285–94.
Mehta RL. Biomarker explorations in acute kidney injury: the journey continues. Kidney Int. 2011;80:332–4.
Cohen SD, Kimmel PL. Long-term sequelae of acute kidney injury in the ICU. Curr Opin Crit Care. 2012;18:623–8.
Lo LJ, Go AS, Chertow GM, McCulloch CE, Fan D, Ordonez JD, et al. Dialysis-requiring acute renal failure increases the risk of progressive chronic kidney disease. Kidney Int. 2009;76:893–9.
Bucaloiu ID, Kirchner HL, Norfolk ER, Hartle JE, Perkins RM. Increased risk of death and de novo chronic kidney disease following reversible acute kidney injury. Kidney Int. 2012;81:477–85.
Authors’ contributions
RM and KD conceived the study, participated in its design and coordination, conducted sample collection, measured biomarkers, analyzed the data, and drafted the manuscript. YK, YM, TY, KY, RI, KM, and TY participated in the study design and coordination, analyzed the data, and drafted the manuscript. MN, EN, and NM conceived the study, participated in its design and coordination, analyzed the data, and drafted the manuscript. All authors read and approved the final manuscript.
Acknowledgements
This study was partly supported by grants from the Tokyo Society of Medical Sciences (KD). Alere Medical Co Ltd. (Tokyo, Japan) partly supported blood sample collection and testing but did not contribute to the study design, data analysis, or preparation of the manuscript.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Consent for publication
Patient informed consent was obtained at the time of ICU admission.
Ethics approval and consent to participate
The study protocol was approved by the institutional review board of The University of Tokyo.
Funding
This work was supported by a grant by the Tokyo Society of Medical Sciences.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
Figure S1. Weight-adjusted FR in AKI progression. The boxplots show the differences in weight-adjusted FR between patients (a) without and with the progression to AKI stage 3 and (b) without and with the progression to AKI stage 3 or death within one week. *, p < 0.01. Figure S2. prediction of AKI progression by weight-adjusted FR. Receiver operating characteristic curves (ROC) in (a) progression to AKI stage 3 and (b) progression to AKI stage 3 or death at one week.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Matsuura, R., Komaru, Y., Miyamoto, Y. et al. Response to different furosemide doses predicts AKI progression in ICU patients with elevated plasma NGAL levels. Ann. Intensive Care 8, 8 (2018). https://doi.org/10.1186/s13613-018-0355-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13613-018-0355-0