
Abstract
Aim
This descriptive review aimed to assess the characteristics and methodological quality of economic evaluations of cardiac rehabilitation (CR) programs according to updated economic guidelines for healthcare interventions. Recommendations will be made to inform future research addressing the impact of a physical exercise component on cost-effectiveness.
Methods
Electronic databases were searched for economic evaluations of exercise-based CR programs published in English between 2000 and 2014. The Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement was used to review the methodological quality of included economic evaluations.
Results
Fifteen economic evaluations met the review inclusion criteria. Assessed study characteristics exhibited wide variability, particularly in their economic perspective, time horizon, setting, comparators and included costs, with significant heterogeneity in exercise dose across interventions. Ten evaluations were based on randomised controlled trials (RCTs) spanning 6–24 months but often with weak or inconclusive results; two were modelling studies; and the final three utilised longer time horizons of 3.5–5 years from which findings suggest that long-term exercise-based CR results in lower costs, reduced hospitalisations and a longer cumulative patient lifetime. None of the 15 articles met all the CHEERS quality criteria, with the majority either fully or partially meeting a selection of the assessed variables.
Conclusion
Evidence exists supporting the cost-effectiveness of exercise-based CR for cardiovascular disease patients. However, variability in CR program delivery and weak consistency between study perspective and design limits study comparability and therefore the accumulation of evidence in support of a particular exercise regime. The generalisability of study findings was limited due to the exclusion of patients with comorbidities as would typically be found in a real-world setting. The use of longer time-horizons would be more comparable with a chronic condition and enable economic assessments of the long-term effects of CR. As none of the articles met recent reporting standards for the economic assessment of healthcare interventions, it is recommended that future studies adhere to such guidelines.
Similar content being viewed by others
Introduction
The global individual and economic burden of cardiovascular disease demands continual innovation of prevention and treatment strategies for effective patient management [1, 2]. Competition between interventions is accentuated by increasing financial constraints on healthcare resources [2]. Economic evaluations provide a useful comparative approach for effective and efficient policy and decision-making considering both costs and consequences on patient outcomes [3, 4].
Cardiac rehabilitation (CR) programs are a standard part of cardiac patient care [5]. Exercise is recognised as a core component of CR and is provided alone, or within a multidisciplinary program combining risk factor management, behaviour modification and psychosocial support [6, 7].
For cardiac patients, the cost-effectiveness of CR compared to standard care has been estimated to cost between USD$2000–$28,000 per life-year gained or leading to increased health-related quality of life (HRQL) at a cost of USD$700–$16,000 per quality-adjusted life-year (QALY) gained [3].
With new CR service-delivery models emerging and healthcare resources becoming more limited, it is timely to reassess the cost-effectiveness of CR-services. Also with the recent development of updated standards for economic evaluations of healthcare interventions, it is necessary to bring the findings of previous reviews [3, 5] into context with these guidelines as to provide a platform for future studies looking at the cost-effectiveness of CR services to build upon. With that in mind, this systematic review aims to understand how economic evaluations of exercise-based CR are conducted with the following objectives: (i) to review the characteristics of published economic evaluations of exercise-based CR with exercise as the primary outcome of interest; (ii) to evaluate the methodological quality of these CR economic evaluations using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist [8] and (iii) to make recommendations for future economic evaluations of CR services. This descriptive study will inform the quality of future research addressing the cost-effectiveness of exercise rehabilitation interventions.
Methods
Economic evaluation
Economic evaluations consist of partial or full analyses [3]. Partial evaluations assess either costs or consequences of multiple interventions or both costs and consequences of a single intervention. Full evaluations examine both costs and consequences of multiple interventions [3]. This review includes all forms of full economic evaluations, i.e. cost-effectiveness, cost-benefit or cost-utility analyses.
Literature search strategy
The “PICO” statement was used to define the search criteria for the review and identify the specifics of the patient population, intervention and the types of studies to be evaluated. Electronic databases (Medline, Embase, HTA, DARE, NHS EED and the Cochrane Library) were searched for all (UK and worldwide) full economic evaluations of CR published in English between 2000 and 2014. The following text-word terms and MeSH headings were used: cost, cost analysis, cost benefit, cost effectiveness, cost minimisation, cost utility, economic assessment, economic evaluation, health economics and cardiac rehabilitation (Appendix 1). Hand searches of bibliographies identified additional publications of which any date was included. Hand searching references of rejected publications also ensured that significant publications of relevance to the field were not missed. Grey literature was not included, but this is unlikely to have any significant effects on publication bias as most economic evaluations are published or cited in scientific or economic journals and will have been picked up through the extensive online literature search.
Selection criteria
A study was considered if it met all the following inclusion criteria:
-
(1)
Adult patients with heart disease/failure who have undergone myocardial infarction (MI) or revascularisation (percutaneous transluminal coronary angioplasty (PTCA) or coronary artery bypass grafting (CABG)) and participated in a CR program
-
(2)
Intervention includes an exercise-based CR program with follow-up
-
(3)
A full-economic evaluation
Data extraction
Two reviewers (KE and RPV) independently selected eligible publications. Disagreement between reviewers was resolved through direct consultation. Data extraction was carried out by a single reviewer (KE) and checked by RPV. Data was extracted from eligible publications on the following items from CHEERS [8]: target population and subgroups, setting and location, study perspective, comparators, time horizon, choice of health outcomes, measurement of effectiveness, measurement and valuation of preference-based outcomes, estimating resources and costs, choice of model, currency, price date and conversion, characterising uncertainty and characterising heterogeneity. Additional data was extracted on study design, sample demographics, exercise dose, frequency and duration of follow-up, included costs, chronic multimorbidity and findings.
Quality assessment
The methodological quality of included evaluations was assessed using CHEERS guidelines for each of the data items extracted [8]. In addition to reporting whether individual studies meet the criteria for each of the data items, their subsequent effects on the study results (such as uncertainty) are examined. The guideline criteria assess specific design elements of economic evaluations for healthcare interventions. CHEERS is not known to have previously been used to assess economic evaluations of exercise-based CR interventions.
Results
Synthesis of evidence
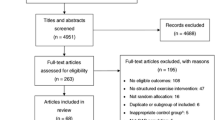
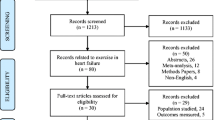
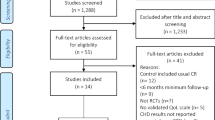
The search strategy retrieved 716 citations, 23 qualified for full-text review and eight were further excluded. Excluded were two literature reviews, one abstract, two which only reported on study designs, one reporting on an already included study, and two which were not full-economic evaluations. Southard et al. [9] is not designed as a full-economic evaluation and structured as a descriptive assessment, but it was included as it examines both health outcomes and costs between two CR interventions. Figure 1 illustrates the review selection process.

Flow of Review Selection Process
Descriptive analysis
Descriptive characteristics of the 15 included economic evaluations are provided in Appendix 2.
Dates, study design, perspective, time horizon and location
The 15 included articles were published between 1991 and 2008, with twelve (80%) being based in the USA or in Europe. Ten studies (67%) were based on randomised clinical trials (RCTs) with time horizons ranging from 6 to 24 months. Twelve (80%) of the studies adopted a cost-effectiveness or cost-utility approach, with the remaining three taking the cost-benefit approach. Eight (53%) of the included studies evaluated costs from the perspective of the healthcare system, with three of those additionally considering patient-borne costs (Table 1).
Program setting, comparators and target population
The comparisons assessed by the selected studies varied greatly. They were undertaken based on various features of the intervention such as where the CR program took place, how exercise was incorporated into the program, or even how the exercise component was delivered.
Taylor et al. [10] and Jolly et al. [11] compared hospital- vs. home- exercise-based CR. Five studies compared hospital-based CR interventions including exercise: Briffa et al. [12] against conventional care where it is unclear if exercise is a component; Levin et al. [13] with standard care and no provision of regular exercise; Dendale et al. [14] with no CR; Hall et al. [15] with no formal CR but provision of a home-walking program; and Ades et al. [16] devised a model based primarily on hospital CR programs that were compared to light/no exercise.
Four studies were at a rehabilitation facility: Papadakis et al. [2] and Reid et al. [17] were based on the same trial and evaluated service-delivery differences between a 3 and 12-month exercise-based CR program, whilst Carlson et al. [18] compared a traditional exercise-based program to one with tapered exercise sessions, and Yu et al. [19] compared an exercise-based CR program to conventional therapy without exercise.
Southard et al. [9] compared a home-based internet program for monitoring patient exercise to usual care, where it is unclear if exercise is a component.
In three studies, the setting of the exercise was unclear: the modelling study by Spronk et al. [20] compared three exercise-based CR strategies; Huang et al. [21] exercise-based CR to no-CR; and Oldridge et al. [4] exercise-based CR against usual care, but did not specify if exercise was a component of that care. Table 2 compares the interventions of each study according to program setting and exercise duration.
In twelve studies the target population included MI patients, one included only PCI patients [14], another only CABG patients [21], and one specified only low-risk cardiac patients who experienced cardiovascular surgery or an event (MI, PCI or CABG) [18].
Sample demographics, Subgroups and Comorbidities
Excluding the two modelling studies, the cohort study employed the largest sample at 4324 patients [21]. In the remaining trials, sample size ranged from 80 to 525 patients at initial recruitment; the majority were males who in most cases accounted for over 72% of the overall sample, with mean age ranging from 53 to 65 years.
Two studies conducted subgroup analyses, each looking at different variables (e.g. age, sex, BMI, cardiac risk, reason for referral) and extent of, if any, their effect on costs [2, 21].
Nine studies made no reference to comorbidities. Three excluded patients with major [10], life threatening or symptomatic comorbidities [14], or where program participation was prevented [11]. Two documented comorbidities, one reporting only cardiovascular-related comorbidities [12, 21]. One reported addressing co-morbidities but provided no details [17]. No study reported analysing data using comorbidities to stratify patients.
Dose of exercise
Excluding the two modelling studies [16, 20] and the cohort study [21], the exercise dose of interventions was assessed using FITT (frequency, intensity, time and type). Southard et al. [9] is classified as patient-dependent for all variables due to the intervention being home-based. Appendix 3 offers a detailed description of exercise dose by intervention within each selected study.
Frequency
The remaining 11 evaluations reported patient exercise frequency, with one referencing the original publication [4, 22]. The frequency of provision for supervised exercise sessions ranged from once-weekly [10] up to four-times weekly [15], with the majority providing twice-weekly sessions [2, 4, 13, 17, 19]. One combined data from three hospital-based CR programs where the frequency of exercise sessions was once-weekly, twice-weekly and tapered [11].
Intensity
Eight studies reported patient exercise intensity, five directly [11, 14, 17,18,19] and three through original trial publications [2, 4, 13, 22, 23]. The threshold for exercise intensity varied between these studies with the majority aiming for between 60 and 85% maximum heart rate capacity [4, 11, 18, 19]. Three did not report patient exercise intensity [10, 12, 15].
Time
Seven evaluations directly reported the duration of patient supervised exercise [11,12,13,14, 17,18,19], while two referred to original trial publications [2, 4, 22]. In these studies, exercise duration ranged from 30 to 120 min. Two did not report exercise duration on their respective CR programs [10, 15].
Type
Nine evaluations directly reported, with varying detail, on the type of exercise undertaken by CR program patients [4, 11,12,13,14,15, 17,18,19], while two referred to original trial publications [2, 10, 24]. The majority involved aerobic exercise training with some specifying the activities involved (e.g. running, cycling, rowing, and circuits). Two stated only that it was a low-level exercise program [4, 15], and one that exercise was ‘consistent with guidelines for patients with CAD’ (coronary artery disease) [17].
Health outcomes and measures of effectiveness
Included studies assessed a variety of health outcomes: (i) HRQL, (ii) cardiovascular health, and (iii) survival. Three were cost-benefit analyses and assessed the monetary equivalent of cardiovascular events [9, 14] or total cost over the study period [13]. Eight evaluated HRQL outcomes: seven using the QALY as an effectiveness measure and either the EQ-5D (using the UK value set tariff) [10, 11], time-trade off scores [3, 4, 19, 20], or UBQ-H scores [12] as preference-based outcomes, while one used a Quality-of-Life score derived from the Health Measurement Questionnaire as an effectiveness measure with no preference-based outcome [15]. Two evaluations assessed cardiovascular health outcomes using factors including peak oxygen consumption, cholesterol levels or kilojoules of activity-related energy as measures of effectiveness [17, 18]. Two looked at survival, with Years-of-Life-Saved (YLS) as the effectiveness measure with no preference-based outcome [16, 21] (Appendix 4).
Economic analysis
The following section reports on features of the health economic analyses. Details are provided in Appendix 5.
Costs
All evaluations considered direct medical costs relating to CR service-provision. Seven considered patient costs, including direct expenses [12], travel [4, 10, 11, 15, 20], time [4, 13, 20], equipment [4, 10] or childcare expenses [4]. One also considered costs associated with employee productivity loss from sick leave or early retirement [13].
Source of costs
Selected studies estimated costs from a combination of sources, including hospital-derived data [2, 15, 20], local/national publications [2, 12, 19], or health insurance companies [13, 17, 21]. One used published data from results of previous RCTs [16]. One did not report the source of their cost data [18].
Currency, price date and conversion
The majority of studies reported costs in United States dollars (USD$), with three having converted from Canadian dollars (CAN$) using a set exchange rate [2, 4, 17]. Two reported costs in British Pounds (£) [10, 11], two in Australian dollars (AUD$) [12, 15], one in Euros (€) [14], and one in Swedish Kroner (SEK) [13]. Two present costs in unspecified dollars, assumed to be USD$ based on the authors’ affiliations [9].
Uncertainty
Nine evaluations characterised the uncertainty around their results: three applied one-way sensitivity analysis [11, 13, 16], Spronk et al. [20] used a combination of one-way, two-way, multi-way and probabilistic sensitivity analyses, and both Briffa et al. [12] and Taylor et al. [10] combined sensitivity analysis and bootstrapping methods. Huang et al. [21] used bootstrapping methods alone, Papadakis et al. [2] combined this technique with a cost-effectiveness acceptability curve (CEAC), and Oldridge et al. [4] used scenario analysis to calculate the plausible range of costs using the minimal, mean and maximum estimates of direct medical costs per patient.
Heterogeneity
Only two evaluations performed subgroup analysis allowing the presentation of results by patient subgroups: Huang et al. [21] reported Medicare expenditure and survival by age, sex, race, number of cardiovascular conditions, diagnosis of chronic obstructive pulmonary disease (COPD), Medicare coverage, higher serum albumin, primary diagnosis of diabetes, AMI before CABG and propensity for receiving CR, while Papadakis et al. [2] provided mean incremental costs, QALYS gained and incremental cost-effectiveness ratio (ICER) by cardiac risk level, risk of disease progression, reason for referral and sex.
Choice of model
The review included two modelling studies: Spronk et al. [20] employed a Markov model to compare the cost-effectiveness of three exercise-based CR strategies, and Ades et al. [16] devised a statistical model to calculate cost-effectiveness in Years-of-Life-Saved.
Findings
Hospital-based CR
Five evaluations compared hospital-based exercise interventions: one to ‘standard’ care [13], one to ‘conventional’ care [12], two with no-CR [14, 15], and one to light/no exercise [16]. Against standard care, hospital-based CR was highly cost-saving over 5 years, with lower direct healthcare costs (3910SEK/€409), fewer cardiovascular-related rehospitalisation’s (0.6 events/patient, non-significant) and less time receiving in-hospital treatment (5.4 days, p < 0.05) [13]. Compared to conventional care, survival advantages are reported for hospital-CR patients where rehabilitation costs of AUD$631(€471)/patient were offset by reduced follow-up costs of AUD$236(€156)/patient and a non-significant gain in quality-of-life up to a year [12]. Against no-CR, one study found hospital-based CR cost €636 less/patient with a reduced number of cardiovascular-related events (0.59 events/patient) [14]. Another estimated CR program cost at AUD$300(€198) but, with non-significant differences between costs and health outcomes compared to no-CR patients, suggests savings may be made by targeting rehabilitation to high-risk individuals [15]. Over 15-years, hospital-based CR is reportedly highly cost-effective and compares favourably to alternative treatments (e.g. thrombolytic therapy, cholesterol-lowering drugs) with a net incremental cost of USD$430 ($1280 vs $850)/€357 (€1063 vs €706), a discounted incremental life expectancy of 0.202 years and an ICER of USD$4950(€4111)/YLS [16].
Home-based CR
One study used a home-based internet intervention to monitor patient activity and as a platform for guidance and interaction [9]. Over usual care, this had net cost-savings of USD$965(€801)/patient and an 11.6% reduction in major cardiovascular events [9].
Hospital- versus home-based CR
Two evaluations examined cost-effectiveness between hospital and home-based CR programs including exercise [10, 11]. Neither found significant differences for costs or health outcomes between patient groups. Taylor et al. [10] found home-based CR had a lower mean cost/patient due to reduced personnel costs (UK£30, 95% CI -£45 to -£12/€32, 95% CI -€48 to -€13), but was associated with greater healthcare costs (UK£78, 95% CI, −£1102 to £1191/€84, 95% CI -€1185 to €1281). Jolly et al. [11] found home-based CR had higher direct rehabilitation costs to the health service (UK£41, 95% CI £26 to £55/€44, 95% CI €28 to €59), even after including patient costs to the hospital-based arm. Each found a non-significantly worse difference in health outcomes for home-based patients with mean QALY differences of −0.022 (95% CI -0.072 to −0.028) [11] or −0.06 (SD, −0.15 to 0.02) [10] between interventions.
Centre-based CR
Four studies were based at a rehabilitation facility: two compared 3 and 12-month exercise-based interventions [2, 17], one a 6-month exercise program to one with tapered sessions [18], and another exercise-based CR to conventional care without exercise [19]. A 3-month CR program cost USD$135(€112) less than a 12-month program, with non-significant differences for exercise-related variables, cardiac risk factors and HRQL [17]. With the same trial, another study showed the 3-month program had an incremental gain of 0.009 QALYs (95% CI 0.004–0.013) and no significant cost differences to a 12-month program [2]. Sub-group analysis showed the 3-month program was dominant for patients with high-risk of disease progression while the 12-month program was preferential for PCI patients, suggesting triaging patients may improve cost-effectiveness [2]. Another study showed 6-month hospital-based CR with tapered exercise sessions was USD$738(€612)/patient cheaper than one with consistent thrice-weekly sessions, but with no significant differences between groups in outcome measures [18]. Against conventional care without exercise, CR was USD$416(€345)/patient cheaper with a 0.6 QALY gain after 2-years, but non-significantly [19].
Three studies do not explicitly report exercise setting. One compared three exercise-based CR strategies (CR only, diagnostic work up for revascularisation before CR or after CR failure), of which the latter was the most favourable with a non-significant gain of 0.03 QALYs and an ICER of USD$44,251(€36,728)/QALY over a patient lifetime compared to CR only [20]. Another study compared exercise-based CR to no-CR finding over 3.5-years finding CR highly cost-effective, associated with a longer cumulative lifetime (76 days, 95% CI 22–129 days) and ICER of USD$13,887(€11,526)/YLS [21]. The remaining study concluded exercise-based CR was an efficient use of healthcare resources with a best incremental cost of USD$480(€398) and mean QALY gain of 0.052 leading to an expected ICER of USD$9200(€7638)/QALY (range USD$2300 to $182,800/€1910 to €151,769) over usual care [4].
Quality assessment
None of the 15 articles met all the CHEERS criteria for included variables (Table 3). All 15 met the reporting recommendations for study perspective and measure of effectiveness. A mixture of studies fully or partially met criteria for reporting target population, setting/location, comparators, estimating resources and costs, and currency. Nine studies characterised the uncertainty of their results, of which only seven fully met the criteria. Two studies fully met the criteria for reporting choice of health outcomes as others did not specify the relevance of those chosen [2, 10]. Two studies performed sub-group analysis, with only one reporting between group variation for incremental costs, QALYs and ICER values [2, 21]. None fully met the criteria for time horizon, as none stated why that used was appropriate. CHEERS assessment was based on the content of individual articles only and not in conjunction with overlapping publications which may have contained relevant information.
Discussion
This review assessed how economic evaluations of exercise-based CR programs are conducted and evaluated their methodological quality against the recently published CHEERS guidelines for healthcare interventions [8]. Exercise was the primary outcome of interest in this review as it has proven health benefits [25] and is a principal component of CR services; other aspects of CR including psychological or educational interventions were not evaluated.
An extensive literature search identified 15 economic evaluations of exercise-based CR services. In consensus with previous reviews we identified wide variability amongst CR programs and service delivery [3, 5]. In this review, such variability was particularly evident in study perspective, time horizon, setting, comparators, included costs, and in exercise dose (FITT) between interventions. We critically appraised included evaluations against recently expanded and updated economic guidance, finding that none fully met the reporting criteria; while included studies predated development of this guidance, future studies may wish to adhere to these up-to-date standards [8].
As most evaluations (10) were RCTs, their meticulous patient selection process will question the wider generalisability of their findings. Comparatively other study types report higher proportions of males (60–89%) and greater CR uptake (64–72%). [25]. Patients in these RCTs were also younger than the average age distribution for CR participants (67 for men and 70 for women) [25]. The use of short time horizons (6–24 months) also seems incompatible with a chronic condition. Given the likelihood that patients registering with a controlled trial may be more inclined to adhere to exercise requirements, these elements suggest economic evaluations of exercise-based CR programs using RCT’s risk providing non-generalizable results.
Compared to RCT’s reporting non-conclusive or weak results, evaluations utilising studies with longer time horizons (3.5 – 5 years) suggest a long-term exercise-based CR program results in lower costs [13, 14], reduced hospitalisations [13, 14], and longer cumulative lifetime [21]. Longer follow-up times may allow for more benefits of the intervention to be accrued and suggest that interventions should be carried out with a long-expanding time horizon.
Despite a reported 60–70% of cardiac patients accessing CR services having comorbidities, these patients were largely absent from included studies. This has been recognised and it is estimated that 48% are deemed inappropriate for rehabilitation by their referrer [25]. In this review most studies failed to report co-morbidities or simply excluded such patients [11, 12]. The likely presence of comorbidities in the population, particularly in older individuals, questions generalisability of findings, and reflects a missed opportunity for their management.
This review identified extensive heterogeneity between studies in exercise dose (FITT) [25]. Session frequency ranged from once to four times weekly, exercise intensity was patient dependent or categorised in broad groups (low, moderate or high intensity), and exercise type often involved combinations of aerobic activity (e.g. walking, running, cycling, rowing, arm cranking, dumbbell or weight training). This reflects a lack of knowledge and absence of guidance on the most effective CR exercise program. Standardising CR would allow more accurate economic assessments, although risk eliminating the potential for more cost-effective results to be obtained from patient-dependent CR exercise regimes [18]. Alternatively, harmonising physical exercise dose into a common standard unit, such as the metabolic equivalent of tasks (METs), would allow for an effective comparison of the very diverse interventions found in the literature [26, 27].
Generic quality-of-life measures (i.e. QALY) allow a common measure across health conditions to facilitate healthcare resource allocation, but their broad scope fails to capture other health-related benefits outside the dimensions of the questionnaire (mobility, self-care, usual activities, pain/discomfort and anxiety/depression in the EQ-5D). The difficulty associated with measuring exercise is a challenge for such interventions and its effects has been captured elsewhere [28]. Exercise is known to have far-reaching benefits proven effective at reducing the disease burden of diabetes, osteoarthritis and cancer [25], however generic HRQL instruments (e.g. EQ-5D and the SF-36) are likely to be insensitive to detecting change brought about by exercise-based CR [25]. Using more specific outcome measures, such as the change in physical activity level or evaluating the psychology of exercise behaviour (e.g. BREQ questionnaire), will provide a more complete picture of the benefits produced by the interventions and avoid producing inaccurate and misleading cost-effectiveness results. Given many studies found non-significant differences in costs between interventions, differences in health outcomes have the capacity to be the main drivers of cost-effectiveness. Appropriate criteria to detect and measure health impact according to the specific study design must be applied. [29,30,31].
All studies incorporated direct CR medical costs into their evaluations, but lacked consistency in the types of costs included and would likely result in two evaluations of the same clinical study reporting different cost-effectiveness results. Use of standardised cost categories consistent with the study aims, perspective and nature of exercise is recommended. For exercise-based CR, the cost-savings attributable to reduced cardiovascular events and potential reduction of general healthcare resource use should be reported. Given that several studies found a non-significant difference in health outcomes between interventions, costs are a potential driving force behind cost-effectiveness.
Few studies reported statistically significant evidence in both costs and effects for CR (Table 2). These were predominantly cost-benefit analyses comparing exercise-based CR to no exercise or where the use of exercise was unclear [21]. Consequently, exercise-based CR was considered cost-saving compared to CR without exercise, and an effective secondary prevention strategy in reducing subsequent cardiac events and re-admissions, and increased survival [21]. Comparatively, other studies did not find significant evidence identifying any interventions as conclusively cost-effective, and this is likely due to inappropriate use of time horizons, perspective, choice of health outcomes, or cost categories.
Nevertheless, cost-effectiveness results can accurately be non-conclusive. Only two evaluations performed subgroup analysis, finding that interventions were more cost-effective depending on gender and risk of disease progression [2]. Given expected differences in cost and health effects for patients of different gender, ages, disease severity, and comorbidities, subgroup analysis is recommended to explore heterogeneity of results between relevant patient groups.
When analysing cost-effectiveness estimates for CR evaluations, it is key to consider input uncertainty on results, and observe whether statistical significance or minimally important differences are achieved. Presenting only deterministic results can be misleading and may show the intervention to be highly cost-effective, yet closer scrutiny of the confidence intervals in some cases reveals very limited certainty around the result [4]. Findings should therefore be reported showing deterministic results of the base case as well as subgroup analyses and measures of uncertainty such as confidence intervals and/or (probabilistic) sensitivity analyses. These will provide a fair representation of findings, statistical significance, achievement of MID, and the potential effect of unknowns on the decision to be made.
These findings provide the basis for the following recommendations for future economic evaluations of CR programs:
-
(1)
Include comorbid patients.
-
(2)
Use of longer time-horizons (ideally lifetime) to capture the long-term health and cost-related outcomes of exercise-based CR for chronic cardiovascular-related conditions.
-
(3)
Develop an effective standardised exercise-based CR program to enhance comparability of health outcomes between studies.
-
(4)
Develop standardised cost categories consistent with the study perspective to enhance comparability of economic findings between studies, potentially including relevant non-health care costs such as productivity loss.
-
(5)
Adhere to up-to-date standards for economic evaluations of healthcare interventions.
-
(6)
Use subgroup analysis to capture the effects of exercise-based CR on different patient groups.
-
(7)
Use standardised reporting guidelines (e.g. CHEERS) to enhance study comparability.
-
(8)
Report confidence intervals, outcome measures and MIDs to enhance the quality of methodological reporting.
Crucially, following the above recommendations will allow carers and providers to make better-informed choices about the CR programs most suitable for their specific patient groups or setting, as the particulars of each will bring specific value weights to the various elements of the costs and outcomes associated to specific modalities of CR programs.
Limitations of this review include incomplete retrieval of all economic evaluations of exercise-based CR-services, which may have arisen from the exclusion of some electronic or grey literature sources. As most economic evaluations are published or cited in economic and scientific journals, it is likely these effects will be minimal following an extensive literature search of several online databases.
Conclusion
Evidence exists supporting the cost-effectiveness of exercise-based CR for cardiovascular disease patients. Variability between studies in study perspective, time horizon, setting, comparators, included costs and interventions makes it difficult to compare and assess cost-effectiveness between alternative strategies. Future studies may wish to consider the implications of an exercise-based CR program for patients with comorbidities and employ longer time-horizons. This will allow the long-term effects of CR services to be better understood and in a majority patient group that presents to this pathway. Standardisation of CR service and delivery will enable greater comparability between studies on a clinical and cost level, with the program providing maximum patient-provider benefit to be identified. Future economic evaluations of exercise-based CR should adhere to current guidelines for the reporting of healthcare interventions. The methodology of cost-effectiveness evaluations could be further improved to accommodate different standards and processes between countries.
References
Nichols M, Townsend N, Luengo-Fernandez R, Leal J, Gray A, Scarborough P, and Rayner M. European Cardiovascular Disease Statistics 2012. European Heart Network, Brussels, European Society of Cardiology, Sophia Antipolis.
Papadakis S, Reid RD, Coyle D, Beaton L, Angus D, Oldridge N. Cost-effectiveness of cardiac rehabilitation program delivery models in patients at varying cardiac risk, reason for referral, and sex. Eur J Cardiovasc Prev Rehabil. 2008;15:347–53.
Papadakis S, Oldridge N, Coyle D, Mayhew A, Reid RD, Beaton L, Dafoe WA, Angus D. Economic evaluation of cardiac rehabilitation: a systematic review. Eur J Cardiovasc Prev Rehabil. 2005;12:513–20.
Oldridge N, Furlong W, Feeny D, Torrance G, Guyatt G, Crowe J, Jones N. Economic evaluation of cardiac rehabilitation soon after acute myocardial infarction. Am J Cardiol. 1993;72:154–61.
Wong WP, Feng J, Pwee KH, Lim JA. systematic review of economic evaluations of cardiac rehabilitation. BMC Health Serv Res. 2012;12:243.
Balady GJ, Williams MA, Ades PA, Bittner V, Comoss P, Foody JM, Franklin B, Sanderson B, Southard D. Core Components of Cardiac Rehabilitation/Secondary Prevention Programs: 2007 Update: A Scientific Statement From the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2007;115:2675–82.
NICE. Secondary prevention in primary and secondary care for patients following a myocardial infarction. National Institute for Health and Care Excellence. 2003. www.nice.org.uk/cg172.
Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, Augustovski F, Briggs AH, Mauskopf J, Loder E. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)--explanation and elaboration: a report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health. 2003;16:231–50.
Southard BH, Southard DR, Nuckolls J. Clinical trial of an Internet-based case management system for secondary prevention of heart disease. J Cardpulm Rehabil. 2003;23:341–8.
Taylor RS, Watt A, Dalal HM, Evans PH, Campbell JL, Read KLQ, Mourant AJ, Wingham J, Thompson DR, Pereira Gray DJ. Home-based cardiac rehabilitation versus hospital-based rehabilitation: a cost effectiveness analysis. Int J Cardiol. 2007;119:196–201.
Jolly K, Taylor R, Lip GYH, Greenfield S, Raftery J, Mant J, Lane D, Jones M, Lee KW, Stevens A. The Birmingham Rehabilitation Uptake Maximisation Study (BRUM). Home-based compared with hospital-based cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient adherence. Health Technol Assess. 2007;11:1–118.
Briffa TG, Eckermann SD, Griffiths AD, Harris PJ, Heath MR, Freedman SB, Donaldson LT, Briffa NK, Keech AC. Cost-effectiveness of rehabilitation after an acute coronary event: a randomised controlled trial. MJA. 2005;183:450–5.
Levin L, Perk AJ, Hedback B. Cardiac rehabilitation--a cost analysis. J Intern Med. 1991;230:427–34.
Dendale P, Hansen D, Berger J, Lamotte M. Long-term cost-benefit ratio of cardiac rehabilitation after percutaneous coronary intervention. Acta Cardiol. 2008;63:451–6.
Hall JP, Wiseman VL, King MT, Ross DL, Kovoor P, Zecchin RP, Moir FM, Robert Denniss A. Economic evaluation of a randomised trial of early return to normal activities versus cardiac rehabilitation after acute myocardial infarction. Heart Lung Circ. 2002;11:10–8.
Ades PA, Pashkow FJ, Nestor JR. Cost-effectiveness of cardiac rehabilitation after myocardial infarction. J Cardpulm Rehabil. 1997;17:222–31.
Reid RD, Dafoe WA, Morrin L, Mayhew A, Papadakis S, Beaton L, Oldridge NB, Coyle D, Wells GA. Impact of program duration and contact frequency on efficacy and cost of cardiac rehabilitation: results of a randomized trial. Am Heart J. 2005;149:862–8.
Carlson JJ, Johnson JA, Franklin BA, VanderLaan RL. Program participation, exercise adherence, cardiovascular outcomes, and program cost of traditional versus modified cardiac rehabilitation. Am J Cardiol. 2000;86:17–23.
CM Y, Lau CP, Chau J, McGhee S, Kong SL, Cheung BM, Li LSA. short course of cardiac rehabilitation program is highly cost effective in improving long-term quality of life in patients with recent myocardial infarction or percutaneous coronary intervention. Arch Phys Med Rehabil. 2004;85:1915–22.
Spronk S, Bosch JL, Ryjewski C, Rosenblum J, Kaandorp GC, White JV, Hunink MG. Cost-effectiveness of new cardiac and vascular rehabilitation strategies for patients with coronary artery disease. PLoS One. 2008;3:e3883.
Huang Y, Zhang R, Culler SD, Kutner NG. Costs and effectiveness of cardiac rehabilitation for dialysis patients following coronary bypass. Kidney Int. 2008;74:1079–84.
Oldridge N, Guyatt G, Jones N, Crowe J, Singer J, Feeny D, McKelvie R, Runions J, Streiner D, Torrance G. Effects on quality of life with comprehensive rehabilitation after acute myocardial infarction. Am J Cardiol. 1991;67:1084–9.
Hedback B, Perk J. 5-year results of a comprehensive rehabilitation programme after myocardial infarction. Eur Heart J. 1987;8:234–42.
Dalal HM, Evans PH, Campbell JL, Taylor RS, Watt A, Read KLQ, Mourant AJ, Wingham J, Thompson DR, Pereira Gray DJ. Home-based versus hospital-based rehabilitation after myocardial infarction: A randomized trial with preference arms — Cornwall Heart Attack Rehabilitation Management Study (CHARMS). Int J Cardiol. 2007;119:202–11.
BHF. National Audit of Cardiac Rehabilitation: Annual Statistical Report 2014. British Heart Foundation, London. 2014.
Jette M, Sidney K, Blumchen G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin Cardiol. 1990;13:555–65.
Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O'Brien WL, Bassett DR Jr, Schmitz KH, Emplaincourt PO, Jacobs DR Jr, and Leon AS. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 2000, 32: S498-S504.
Gates LS, Leyland KM, Sheard S, Jackson K, Kelly P, Callahan LF, Pate R, Roos EM, Ainsworth B, Cooper C, Foster C, Newton JL, Batt ME, Arden NK. Physical Activity and Osteoarthritis: A consensus study to harmonise self-reporting methods of physical activity across international cohorts. Rheumatol Int (In press). 2017;37(4):469–78.
Berger ML, Dreyer N, Anderson F, Towse A, Sedrakyan A, Normand SL. Prospective observational studies to assess comparative effectiveness: the ISPOR good research practices task force report. Value Health. 2012;15:217–30.
Ramsey SD, Willke RJ, Glick H, Reed SD, Augustovski F, Jonsson B, Briggs A, Sullivan SD. Cost-effectiveness analysis alongside clinical trials II-An ISPOR Good Research Practices Task Force report. Value Health. 2015;18:161–72.
Caro JJ, Briggs AH, Siebert U, Kuntz KM. Modeling Good Research Practices - Overview: A Report of the ISPOR-SMDM Modeling Good Research Practices Task Force-1. Value Health. 2012;15:796–803.
Acknowledgements
This project was supported by a donation from Health Education East Midlands.
Funding
This project was supported by a donation from Health Education East Midlands, who played no role in the design, conduct, or decision to publish the results from the study.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article and its additional files.
Author information
Authors and Affiliations
Contributions
NJ, JN, CF, AJ, KJ, NKA and RPV conceived the study and contributed to the study design. KE and RPV conducted the review, including extracting and screening all papers for inclusion, scoring and critically reviewing the content of included papers. RPV supervised all stages of the study, including drafting the paper for publication. All authors critically reviewed the academic content and participated in producing the final draft. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
Associate Professor Andrew Judge reports personal fees from SERVIER, UK RENAL REGISTRY, OXFORD CRANIOFACIAL UNIT, FRESHFIELDS, BRUCKHAUS DERINGER, ANTHERA PHARMACEUTICALS and other from IDIAP JORDI GOL and ROCHE, outside the submitted work. Professor Nigel K Arden reports personal fees from FLEXION, LILY, MERICK, Q-MED, ROCHE, SMITH & NEPHEW and FRESHFIELDS, outside the submitted work. Dr. Rafael Pinedo-Villanueva reports personal fees from FRESHFIELDS, outside the submitted work. The remaining authors have no conflicts of interest to declare.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1
Electronic search strategy: MEDLINE (OVID)
-
1
cost
-
2
costs
-
3
cost analysis
-
4
cost-analysis
-
5
cost analyses
-
6
cost-analyses
-
7
cost benefit
-
8
cost-benefit
-
9
cost benefit analysis
-
10
cost-benefit analysis
-
11
cost benefit analyses
-
12
cost-benefit analyses
-
13
cost effective
-
14
cost-effective
-
15
cost effectiveness
-
16
cost-effectiveness
-
17
cost effectiveness analysis
-
18
cost-effectiveness analysis
-
19
cost effectiveness analyses
-
20
cost-effectiveness analyses
-
21
cost minimisation
-
22
cost-minimisation
-
23
cost minimization
-
24
cost-minimization
-
25
cost minimisation analysis
-
26
cost-minimisation analysis
-
27
cost minimisation analyses
-
28
cost-minimisation analyses
-
29
cost minimization analysis
-
30
cost-minimization analysis
-
31
cost minimization analyses
-
32
cost-minimization analyses
-
33
cost utility
-
34
cost-utility
-
35
cost utility analysis
-
36
cost-utility analysis
-
37
cost utility analyses
-
38
cost-utility analyses
-
39
economic evaluation
-
40
economic assessment
-
41
health economics
-
42
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41
-
43
cardiac rehabilitation
-
44
42 and 43
Appendix 2
Appendix 3
Appendix 4
Appendix 5
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Edwards, K., Jones, N., Newton, J. et al. The cost-effectiveness of exercise-based cardiac rehabilitation: a systematic review of the characteristics and methodological quality of published literature. Health Econ Rev 7, 37 (2017). https://doi.org/10.1186/s13561-017-0173-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13561-017-0173-3