
Abstract
Purpose
Checkpoint inhibition therapy using monoclonal antibodies against programmed cell death protein 1 (PD-1) or its ligand (PD-L1) is now standard management of non-small cell lung cancer (NSCLC). PD-L1 expression is a validated and approved prognostic and predictive biomarker for anti-PD-1/PD-L1 therapy. Technetium-99 m [99mTc]-labelled anti-PD-L1 single-domain antibody (NM-01) SPECT/CT quantification correlates with PD-L1 expression in NSCLC, presenting an opportunity for non-invasive assessment. The aim of this study was to determine the inter- and intraobserver agreement of the quantitative assessment of [99mTc]NM-01 SPECT/CT in NSCLC.
Methods
[99mTc]NM-01 SPECT/CT studies of 21 consecutive NSCLC participants imaged for the evaluation of PD-L1 expression were analysed. Three independent observers measured maximum counts in a tumour region of interest (ROImax) of primary lung, metastatic lesions and normal tissue references of both 1 and 2 h post-injection (n = 42) anonymised studies using a manual technique. Intraclass correlation coefficients (ICC) were calculated, and Bland–Altman plot analysis was performed to determine inter- and intraobserver agreement.
Results
Intraclass correlation of primary lung tumour-to-blood pool (T:BP; ICC 0.83, 95% CI 0.73–0.90) and lymph node metastasis-to-blood pool (LN:BP; ICC 0.87, 0.81–0.92) measures of [99mTc]NM-01 uptake was good to excellent between observers. Freehand ROImax of T (ICC 0.94), LN (ICC 0.97), liver (ICC 0.97) and BP (ICC 0.90) reference tissues also demonstrated excellent interobserver agreement. ROImax scoring of healthy lung demonstrated moderate to excellent interobserver agreement (ICC 0.84) and improved when measured consistently at the level of the aortic arch (ICC 0.89). Manual ROImax re-scoring of T, LN, T:BP and LN:BP using [99mTc]NM-01 SPECT/CT following a 42-day interval was consistent with excellent intraobserver agreement (ICC range 0.95–0.97).
Conclusion
Good to excellent inter- and intraobserver agreement of the quantitative assessment of [99mTc]NM-01 SPECT/CT in NSCLC was demonstrated in this study, including T:BP which has been shown to correlate with PD-L1 status. [99mTc]NM-01 SPECT/CT has the potential to reliably and non-invasively assess PD-L1 expression.
Clinical trial registration
ClinicalTrials.gov identifier no. NCT02978196. Registered 30th November 2016.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Lung cancer is the most commonly diagnosed cancer globally and a leading cause of mortality with over 1.7 million deaths in 2018 alone [1]. Therapeutic molecular-targeting agents have resulted in significant improvements in progression-free and overall survival in advanced non-small cell lung cancer (NSCLC); however, targetable genetic aberrations represent only a small proportion of cases [2]. The introduction of monoclonal antibodies targeting immune checkpoint molecules including programmed cell death protein 1 (PD-1) and its ligand (PD-L1) has revolutionised the treatment paradigm of NSCLC. An important mechanism of immune escape involves the upregulation of co-inhibitory molecule PD-L1 by tumour cells, which on interaction with PD-1, expressed by effector T cells, lead to their dysfunction. Anti-PD-1/PD-L1 therapy improves median overall survival in advanced NSCLC in both first- and second-line settings compared to standard cytotoxic chemotherapy, with durable responses seen in around 20% [3,4,5,6].
PD-L1 expression determined by immunohistochemistry (IHC) is a widely validated biomarker correlating with anti-PD-1/PD-L1 therapeutic response and survival [4,5,6,7]. Despite this correlation, up to 10% of patients deemed ‘non-expressers’ by IHC respond to anti-PD-1/PD-L1 therapy [4]. Heterogeneity of PD-L1 expression both within and between tumours is well reported, as are changes over time particularly following exposure to anti-cancer therapies [8, 9]. Considering that multiple or serial biopsies are impractical and associated with increased risk to individual patients, this temporospatial heterogeneity presents a particular challenge as needle biopsy only samples a small area of the tumour. Additionally, there are multiple PD-L1 assays available which may assess PD-L1 expression on tumour or infiltrative immune cells alone or in combination [10]. Considering a potential for false negative results with IHC and the limitations described, non-invasive imaging techniques present a potential solution and opportunity to improve the predictive value of PD-L1 assessment.
NM-01 is a camelid single-domain antibody against PD-L1 that when radiolabelled with technetium-99 m ([99mTc]) can be detected by single-photon emission computed tomography (SPECT). Recently, we have reported results from a first-in-human study of [99mTc]NM-01 that demonstrated both safety and acceptable dosimetry in the first 16 recruited participants with NSCLC [11]. SPECT/computed tomography (CT) scans were obtained 1 and 2 h following [99mTc]NM-01 injection with primary tumour-to-blood pool ratio (T:BP) assessment correlating with PD-L1 expression determined by IHC. Additionally, uptake was demonstrated in nodal and bone metastases with heterogeneity of expression in 30% of cases. This novel single-domain antibody presents an opportunity for the non-invasive total tumoural assessment of PD-L1 that could help clinicians better stratify patients to receive the most appropriate anti-cancer therapy at the right time in their disease course. Our hypothesis was that quantitative measurement of PD-L1 expression using [99mTc]NM-01 SPECT/CT is consistent and reproducible between and within observers. The aim of this study was to determine the reproducibility of and agreement between experienced and less experienced observers within a cohort of patients with NSCLC.
Methods
Participants aged between 18 and 75 years with histologically confirmed, untreated NSCLC and an Eastern Cooperative Oncology Group (ECOG) performance score of 1 or less were eligible to participate and undergo [99mTc]NM-01 SPECT/CT. Exclusion criteria included pregnant or lactating females, severe infection and inability to provide biopsy sample for assessment of PD-L1. The study was registered with ClinicalTrials.gov identifier no. NCT02978196. Ethics approval was obtained from Shanghai General Hospital Ethics Committee (approval no. 2016KY220), and all enrolled participants provided written informed consent [11].
SPECT/CT protocol
SPECT/CT examinations were performed on a GE Discovery NM670 SPECT/CT scanner (GE Healthcare; NY, USA). Participants were administered an intravenous bolus of [99mTc]NM-01 (3.8–8.4 MBq/kg) equivalent to 100 μg (n = 18; 1.65 ± 0.46 μg/kg; range 1.19–2.11 μg/kg) and (9.1–10.4 MBq/kg) equivalent to 400 μg (n = 3; 5.81 ± 0.25 μg/kg; range 5.56–6.06 μg/kg). Participants were asked to drink 300–500 mL water post-injection and void bladder prior to imaging. Following an uptake time of 60 min, a low-dose CT was performed for anatomical correlation and attenuation correction. SPECT imaging, focusing on primary tumour (thorax) and site(s) of suspected metastases, was performed with the patient supine at 1 and 2 h post-injection at 10 cm/slice/min. Scans were performed as previously described using low-energy high-resolution collimators with a ± 10% energy window centred around 140 keV in a 64 × 64 matrix for tomographic images [11]. A 10% energy window centred at 120 keV was also used for tomographic image acquisition for scatter correction. SPECT was performed over 360° in 60 frames per rotation with 20-s acquisition per frame. Images were reconstructed using OSEM iterative reconstruction (2 iterations, 10 subsets) at a matrix size of 128 × 128 using scatter correction.
Image analysis
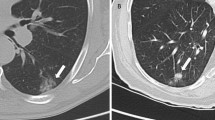
Images were reviewed by three independent observers blinded to patient details and each other’s assessments using Hermes GOLD™ (Hermes Medical Solutions; Stockholm, Sweden). The observers included one nuclear medicine physician, one nuclear medicine clinical fellow in training and one oncology clinical fellow PhD student with 30, 3 and 1 years of experience in nuclear medicine image analysis, respectively. Regions of interest including primary tumour and metastatic lesions, including lymph nodes and normal tissue references (lung, liver and blood pool), were identified with CT correlation. Using a freehand manual technique, the maximum count for regions of interest (ROImax) was recorded from 1- and 2-h SPECT images (n = 42) for each patient. ROImax was chosen as ROImean could be affected by differences in the manual segmentation and is more likely to be affected by the partial volume effect. In addition, the method using ROImax was previously shown to correlate with IHC [11]. Freehand ROImax was recorded for normal lung in the right upper lobe (or contralateral upper lobe if pathology present) for calculation of tumour-to-lung (T:L) ratio and for blood pool within the aortic arch for calculation of tumour-to-blood pool (T:BP) ratio. To evaluate if rule-based approaches improved consistency of scoring of normal tissue references, ROImax was also recorded using a standardised 3-cm-diameter sphere for normal lung at the level of the aortic arch and carina, and the liver at the level of the gastroesophageal junction (GOJ) on axial view. Examples of image analysis are provided in Fig. 1. To determine intraobserver agreement, the two independent observers with least experience (one nuclear medicine and one oncology clinical fellow) repeated their calculations for all measured regions blind to their initial measurements following a 42-day period.

Image analysis using ROImax scoring of [99mTc]NM-01 SPECT/CT of: primary left lower lobe tumour, IHC PD-L1 65% (a), freehand; unaffected lung tissue freehand (b) and using a 3-cm sphere at level of the aortic arch (c); blood pool reference tissue (d); liver reference tissue freehand (e) and using a 3-cm sphere at the axial level of the gastroesophageal junction (f)
Statistical analysis
Intraclass correlation coefficient (ICC) is a reliability index that represents both the degree of correlation but also the agreement between measurements. A full description of their application and formulae is described in the literature [12]. ICC and their 95% confidence intervals (CIs) were calculated using a two-way random consistent model, to determine interobserver agreement between all three observers. ICC and their 95% CI were calculated using a two-way mixed effects absolute agreement model, to determine intraobserver agreement for two observers. ICC values range from 0 to 1, where the values less than 0.5 indicate poor agreement, 0.5–0.75 moderate, 0.75–0.9 good, and greater than 0.9, i.e. close to 1, represent excellent agreement [12]. As the ICC obtained is an estimated value of the true ICC, the levels of agreements are defined by their 95% confidence intervals. Bland–Altman plots and their 95% limits of agreement were used to determine the agreement between observers and their repeat measurements for logarithm-transformed T:BP and LN:BP scores. Linear regression of Bland–Altman plots was performed to determine the β coefficient of the mean difference and demonstrate any proportional bias (where p < 0.05 is significant). Statistical analysis was performed using IBM SPSS Statistics for Windows, version 26.0 (Armonk, NY: IBM Corp.).
Results
Participant characteristics
Participants were recruited to the study between March 2018 and April 2019 (n = 21). The median age was 65 years (range 36–75 years); all were of Asian ethnicity. All had a histologically confirmed diagnosis of NSCLC (adenocarcinoma n = 10, squamous cell carcinoma n = 11) with 9 of 21 participants having metastatic disease. A full summary of participant characteristics is provided in Table 1.
Interobserver agreement
There was excellent agreement of manual freehand ROImax scoring between all three observers of primary lung tumour (T; ICC 0.94; 95% CI 0.9–0.97), lymph node metastases (LN; ICC 0.97; 0.95–0.98) and blood pool healthy reference tissue (BP; ICC 0.9; 0.84–0.94) using [99mTc]NM-01 SPECT/CT (Table 2). T:BP (ICC 0.83; 0.73–0.90) and LN:BP (ICC 0.87; 0.81–0.92) ratios, which provide a quantitative measure of [99mTc]NM-01 uptake for primary lung tumour and lymph node metastases on SPECT/CT, respectively, both demonstrated good interobserver agreement. Bland–Altman plot analysis demonstrated interobserver agreement with no proportional bias on linear regression for T:BP scores (Fig. 2). Bland–Altman analysis for LN:BP scores (Fig. 2) did, however, demonstrate proportional bias for observer B compared with both observer A (β = 0.11, p = 0.047) and observer C (β = -0.17, p = 0.02). There was acceptable agreement and no proportional bias for LN:BP scores between observers A and C (β = 0.06, p = 0.448).

Interobserver Bland–Altman level of agreement plots for log10 T:BP (a–c) and log10 LN:BP (d–f) scores. Upper and lower 95% limits of agreement represented by dashed lines. Solid horizontal lines represent between-observer mean difference. a T:BP scores observer A versus B (β = 0.13, p = 0.117); b T:BP scores observer A versus C (β = 0.07, p = 0.375); c T:BP scores observer B versus C (β = -0.06, p = 0.410); d LN:BP scores observer A versus B (β = 0.11, p = 0.047); e LN:BP scores observer A versus C (β = -0.06, p = 0.448); f LN:BP scores observer B versus C (β = -0.17, p = 0.020)
Freehand ROImax scoring of non-affected lung background reference tissue demonstrated moderate to excellent interobserver agreement (ICC 0.84; 0.75–0.90). The ICC was improved with good to excellent agreement when either rule-based approach was applied, measuring ROImax at the level of the aortic arch (ICC 0.89; 0.82–0.93) or the carina (ICC 0.88; 0.81–0.93). Calculated T:L ratios, when measuring healthy lung ROImax at the level of the aortic arch, were also improved to good to excellent (ICC 0.85; 0.77–0.91) compared to moderate to excellent agreement demonstrated with freehand (ICC 0.79; 0.68–0.88) and carina rule-based (ICC 0.80; 0.69–0.88) approaches.
Excellent interobserver agreement (ICC 0.97; 0.95–0.98) was also demonstrated of freehand ROImax scores for healthy reference tissue liver. Applying a consistent rule-based approach to score the liver at the level of the gastroesophageal junction did not improve agreement further (ICC 0.95; 0.92–0.97).
Using a T:BP score of ≥ 2.32 to represent a PD-L1 of ≥ 1%, the interobserver mean sensitivity was 61% and specificity 73% for this cohort (Table 3). Discrepant cases were reviewed, and a consensus was made between the three observers defining the T:BP as either < or ≥ 2.32 (Table 4). Five cases with PD-L1 expression between 1 and 10% on IHC remained discordant, four of which were considered negative PD-L1 by T:BP score of [99mTc]NM-01 SPECT/CT but positive (≥ 1%) by IHC.
Intraobserver agreement
Manual ROImax scoring of primary lung tumour, lymph node metastases and blood pool reference tissue using [99mTc]NM-01 SPECT/CT following a 42-day interval was consistent for the two observers analysed (Table 5). The intraobserver ICC for primary lung tumour ROImax scores for observer B (ICC 0.96; 95% CI 0.93–0.98) and observer C (ICC 0.95; 0.91–0.97) demonstrated excellent agreement. Scoring of lymph node metastases also demonstrated excellent agreement (observer B ICC 0.97; observer C ICC 0.97, see Table 5 for 95% CIs). The intraobserver ICC for freehand ROImax scores for reference tissue blood pool (observer B ICC 0.98; observer C ICC 0.97) confirmed excellent agreement. Excellent intraobserver agreement of both T:BP and LN:BP ratios for both observer B (ICC 0.96 and 0.95, respectively) and observer C (ICC 0.95 and 0.95) were also demonstrated. Bland–Altman plot analysis demonstrated intraobserver agreement with no proportional bias on linear regression for both T:BP and LN:BP scores (Fig. 3).

Intraobserver Bland–Altman level of agreement plots for log10 T:BP (a, b) and log10 LN:BP (c, d) scores. Upper and lower 95% limits of agreement represented by dashed lines. Solid horizontal lines represent between-timepoints mean difference. a T:BP scores observer B, time 1 versus time 2 (β = 0.01, p = 0.781); b T:BP scores observer C, time 1 versus time 2 (β = -0.04, p = 0.462); c LN:BP scores observer B, time 1 versus time 2 (β = -0.08, p = 0.183); d LN:BP scores observer C, time 1 versus time 2 (β = 0.09, p = 0.080)
The intraobserver ICC for freehand ROImax scores for healthy lung (observer B ICC 0.87; observer C ICC 0.91) and liver (observer B ICC 0.98; observer C ICC 0.99) demonstrated good to excellent agreement. A trend towards improved intraobserver agreement with rule-based approaches for healthy lung scoring was demonstrated, but no overall difference in the level of agreement was seen. Calculated T:L ratios demonstrated good or excellent intraobserver agreement (ICCs 0.84 to 0.92) irrespective of the healthy lung tissue scoring applied.
Discussion
Our study demonstrates that the quantitative assessment of [99mTc]NM-01 using SPECT/CT is both reliable and reproducible within and between independent observers. Interobserver agreement was demonstrated for both T:BP (ICC 0.83) and LN:BP (ICC 0.87). In addition, excellent intraobserver agreement was shown (T:BP ICC 0.95–0.96; LN:BP ICC 0.95). This provides further evidence that [99mTc]NM-01 has significant potential and clinical utility as a diagnostic agent for the measurement of PD-L1. Non-invasive assessment of PD-L1 is an attractive possibility considering the dynamic nature and heterogeneity of its expression. [99mTc]NM-01 uptake measured by T:BP on SPECT/CT has already been shown to correlate with PD-L1 expression measured by IHC (r = 0.68, p = 0.014) [11]. This study, which confirms good to excellent inter- and intraobserver agreement of the quantitative assessment of [99mTc]NM-01 SPECT/CT, supports its potential to provide reliable assessment of PD-L1 expression. It remains unclear whether temporal changes in PD-L1 expression and response assessment using [99mTc]NM-01 SPECT/CT following anti-PD-1/PD-L1 therapy will be demonstrated and of clinical utility. This will be further explored in a phase II clinical trial, PECan [NCT04436406], which will also compare changes in PD-L1 expression and response to parameters on [18F]FDG PET/CT in both NSCLC and malignant melanoma.
This study is the first to assess the agreement of SPECT/CT in measuring PD-L1 expression in cancer. Several other radionuclides are currently being developed specifically for imaging the PD-1/PD-L1 axis. 18F-BMS-986192 (18Fluor-labelled anti-PD-L1 Adnectin) uptake on positron emission tomography (PET) has been shown to correlate with PD-L1 expression in NSCLC, as has 89Zirconium-nivolumab for PD-1 expression, both in early phase clinical trials [13]. In both cases, inter- and intra-tumoural heterogeneity was demonstrated, consistent with the findings described in the early phase trial of [99mTc]NM-01 SPECT/CT. An important characteristic of [99mTc]NM-01 is that it is a small (14.3 kDa) antigen-binding fragment radiotracer with rapid blood clearance, with optimal SPECT/CT imaging performed at just 2 h following administration. As [99mTc]NM-01 does not directly block the PD-L1 binding site, it does not interfere with the PD-1/PD-L1 axis and thus has the potential to assess whole-body PD-L1 status before, during and after anti-PD-L1 therapy. Whilst PET/CT provides a higher degree of spatial resolution, there are some notable benefits to SPECT/CT imaging. [99mTc] radioisotope and SPECT imaging are both more widely available and relatively inexpensive. Concerns regarding the non-standardised quantification techniques for SPECT/CT may not be fully justified if quantification techniques are reproducible and reliable. Applying simple rules to ROImax scoring may improve both inter- and intraobserver agreement, as demonstrated in this study where applying a set 3-cm sphere to score the unaffected lung at the level of the aortic arch improved the interobserver ICC. Whilst we did not show any significant improvement in agreement applying a similar rule to the liver, both inter- and intraobserver ICC remained excellent, suggesting that simple rule-based approaches may be used to standardise and simplify image interpretation without significant impact on quantification.
There are some limitations to this study. Firstly, it is limited by its sample size; nevertheless, the relatively narrow confidence intervals suggest a good estimate of the agreement. Despite good to excellent interobserver agreement, the mean sensitivity and specificity were relatively poor with some discrepant cases resulting in a PD-L1 assessment determined by T:BP of [99mTc]NM-01 discordant with that found on IHC. This is not unexpected considering that heterogeneity of PD-L1 measured by IHC is widely reported in the literature and was demonstrated on [99mTc]NM-01 assessment in our previous study [11]. In addition, the cut-off value of T:BP ≥ 2.32 correlating with a PD-L1 of ≥ 1% on IHC was determined on a small sample size and requires further validation in larger cohorts [11]. It is also important to note that the patient cohort was relatively heterogenous with regards to tumour staging. Due to the low number of measurable extra-nodal (lung and bone) metastases in the cohort (n = 8), statistical analysis using ICC of the quantitative assessment of [99mTc]NM-01 in these lesions was not possible. With further understanding of the relationship between PD-L1 expression by IHC and [99mTc]NM-01 SPECT/CT, it may be possible for both quantitative (as described in this study) and qualitative assessments to be made by observers blind to IHC PD-L1 expression, and their agreement evaluated. SPECT is a highly sensitive imaging modality but has relatively poor resolution; further optimisation with iterative reconstruction methods along with CT attenuation and scatter corrections have the potential to further improve and standardise quantification [14]. Novel SPECT reconstruction techniques that enable standardised quantification will be employed in forthcoming PECan and PELICAN studies [EudraCT 2020-002809-26] to further investigate and validate [99mTc]NM-01 SPECT/CT clinically. This would also enable quantitative comparison with other PD-L1 PET radionuclides, for example the aforementioned 18F-BMS-986192 [13].
Conclusion
Overall, good to excellent inter- and intraobserver agreement of the quantitative assessment of [99mTc]NM-01 SPECT/CT in NSCLC was demonstrated in this study. With correlation between PD-L1 expression determined by [99mTc]NM-01 SPECT/CT and by immunohistochemistry previously demonstrated, there is considerable potential for [99mTc]NM-01 SPECT/CT to reliably assess PD-L1 expression, with further analysis in subsequent clinical trials now being conducted.
Availability of data and materials
The data sets used and analysed during the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
Change history
12 October 2021
This article has been retracted. Please see the Retraction Notice for more detail: https://doi.org/10.1186/s13550-021-00851-1
Abbreviations
- BP:
-
Blood pool
- CI:
-
Confidence interval
- CT:
-
Computed tomography
- ECOG:
-
Eastern Cooperative Oncology Group
- [18F]FDG:
-
2-Deoxy-2-[fluorine-18]fluoro-D-glucose
- GOJ:
-
Gastroesophageal junction
- ICC:
-
Intraclass correlation coefficient
- IHC:
-
Immunohistochemistry
- L:
-
Lung
- LN:
-
Lymph node
- LN:BP:
-
Lymph node-to-blood pool ratio
- NSCLC:
-
Non-small cell lung cancer
- PD-1:
-
Programmed cell death protein 1
- PD-L1:
-
Programmed death-ligand 1
- PET:
-
Positron emission tomography
- ROImax :
-
Maximum region of interest
- SPECT:
-
Single-photon emission computed tomography
- T:
-
Tumour
- T:BP:
-
Primary tumour-to-blood pool ratio
- [99mTc]:
-
Technetium-99 m
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. https://doi.org/10.3322/caac.21492.
Yuan M, Huang L-L, Chen J-H, Wu J, Xu Q. The emerging treatment landscape of targeted therapy in non-small-cell lung cancer. Signal Transduct Target Therapy. 2019;4(1):10. https://doi.org/10.1038/s41392-019-0099-9.
Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Updated Analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol. 2019;37(7):537–46. https://doi.org/10.1200/jco.18.00149.
Rittmeyer A, Barlesi F, Waterkamp D, Park K, Ciardiello F, Von Pawel J, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389(10066):255–65. https://doi.org/10.1016/s0140-6736(16)32517-x.
Vokes EE, Ready N, Felip E, Horn L, Burgio MA, Antonia SJ, et al. Nivolumab versus docetaxel in previously treated advanced non-small-cell lung cancer (CheckMate 017 and CheckMate 057): 3-year update and outcomes in patients with liver metastases. Ann Oncol. 2018;29(4):959–65. https://doi.org/10.1093/annonc/mdy041.
Fehrenbacher L, Spira A, Ballinger M, Kowanetz M, Vansteenkiste J, Mazieres J, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet. 2016;387(10030):1837–46. https://doi.org/10.1016/s0140-6736(16)00587-0.
Herbst RS, Baas P, Kim D-W, Felip E, Pérez-Gracia JL, Han J-Y, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016;387(10027):1540–50. https://doi.org/10.1016/S0140-6736(15)01281-7.
McLaughlin J, Han G, Schalper KA, Carvajal-Hausdorf D, Pelekanou V, Rehman J, et al. Quantitative assessment of the heterogeneity of pd-l1 expression in non-small-cell lung cancer. JAMA Oncol. 2016;2(1):46–54. https://doi.org/10.1001/jamaoncol.2015.3638.
Kim T-J, Hong SA, Kim O, Kim SJ, Yang J-H, Joung EK, et al. Changes in PD-L1 expression according to tumor infiltrating lymphocytes of acquired EGFR-TKI resistant EGFR-mutant non-small-cell lung cancer. Oncotarget. 2017. https://doi.org/10.18632/oncotarget.22582.
Udall M, Rizzo M, Kenny J, Doherty J, Dahm S, Robbins P, et al. PD-L1 diagnostic tests: a systematic literature review of scoring algorithms and test-validation metrics. Diagn Pathol. 2018. https://doi.org/10.1186/s13000-018-0689-9.
Xing Y, Chand G, Liu C, Cook GJR, O’Doherty J, Zhao L, et al. Early phase I study of a 99mTc-Labeled anti-programmed death ligand-1 (PD-L1) single-domain antibody in SPECT/CT assessment of PD-L1 expression in non-small cell lung cancer. J Nucl Med. 2019;60(9):1213–20. https://doi.org/10.2967/jnumed.118.224170.
Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–63. https://doi.org/10.1016/j.jcm.2016.02.012.
Niemeijer AN, Leung D, Huisman MC, Bahce I, Hoekstra OS, Van Dongen GAMS, et al. Whole body PD-1 and PD-L1 positron emission tomography in patients with non-small-cell lung cancer. Nat Commun. 2018. https://doi.org/10.1038/s41467-018-07131-y.
Dickson J, Ross J, Vöö S. Quantitative SPECT: the time is now. EJNMMI Phys. 2019. https://doi.org/10.1186/s40658-019-0241-3.
Acknowledgements
The authors would like to thank all the participants and staff involved in this study. Additionally, the authors acknowledge colleagues at Shanghai General Hospital, China, King’s College London, Guy’s and St Thomas’ PET Centre and the Guy’s Comprehensive Cancer Centre, London, UK, for their contributions.
Funding
This research was supported by NanoMab Technology Limited. The authors acknowledge financial support from the Wellcome Trust EPSRC Centre for Medical Engineering at King’s College London (WT203148/Z/16/Z), and UK Research & Innovation London Medical Imaging and Artificial Intelligence Centre.
Author information
Authors and Affiliations
Contributions
DJH, GC, VG and GJRC were responsible for study concept and design, data analysis and interpretation, writing, reviewing and editing the manuscript. DJH, GC and GJRC were responsible for observer rating. DJH and GJRC made the final decision to approve and submit the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Institutional ethics approval for this study was obtained from Shanghai General Hospital Ethics Committee (2016KY220). Participants enrolled in the study provided written informed consent to participate.
Consent for publication
Not applicable.
Competing interests
DJH has received honoraria from Novartis and research funding from NanoMab Technology Limited. GC provides consultancy for NanoMab Technology Limited. VG has received research support from Siemens Healthcare. GJRC has received research support from NanoMab Technology Ltd., Theragnostics Ltd. and Serac Healthcare Ltd. and provides consultancy for GE Healthcare and NanoMab Technology Ltd.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article has been retracted. Please see the retraction notice for more detail:https://doi.org/10.1186/s13550-021-00851-1
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hughes, D.J., Chand, G., Goh, V. et al. RETRACTED ARTICLE: Inter- and intraobserver agreement of the quantitative assessment of [99mTc]-labelled anti-programmed death-ligand 1 (PD-L1) SPECT/CT in non-small cell lung cancer. EJNMMI Res 10, 145 (2020). https://doi.org/10.1186/s13550-020-00734-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13550-020-00734-x