
Abstract
Purpose
We aimed to compare different methods for semi-quantitative analysis of cardiac retention of bone tracers in patients with cardiac transthyretin amyloidosis (ATTR).
Methods
Data from 67 patients with ATTR who underwent both conventional whole-body scan and a CZT myocardial SPECT (DSPECT, Spectrum Dynamics) 3 h after injection of 99mTc-labeled bone tracer were analyzed. Visual scoring of cardiac retention was performed on whole-body scan according to Perugini 4-point grading system from 0 (no uptake) to 3 (strong cardiac uptake with mild/absent bone uptake). A planar heart-to-background (H:B) ratio was calculated using whole-body scan (wb-H:B). CZT SPECT was quantified using three methods: planar H:B ratio calculated from anterior reprojection (ant-H:B), left anterior oblique reprojection (LAO-H:B), and 3D-H:B ratio calculated from transaxial slices as mean counts in a VOI encompassing the heart divided by background VOI in the contralateral lung. Interventricular septal thickness was obtained using echocardiography.
Results
H:Bs obtained from planar and reprojected data were not statistically different (wb-H:B, 2.05 ± 0.64, ant-H:B, 1.97 ± 0.61, LAO-H:B, 2.06 ± 0.64, all p = ns). However, 3D-H:B was increased compared to planar H:Bs (3D-H:B, 4.06 ± 1.77, all p < 0.0001 vs. wb-H:B, ant-H:B, and LAO-H:B). Bland-Altman plots demonstrated that the difference between 3D and planar H:Bs increased with the mean value of myocardial uptake. 3D-H:B was best correlated to septal thickness (r = 0.45, p < 0.001). Finally, abnormal right ventricular uptake was associated with higher values of cardiac retention.
Conclusion
3D semi-quantitative analysis of CZT SPECT optimized the assessment of 99mTc-labeled bone tracer myocardial uptake in patients with cardiac amyloidosis.
Similar content being viewed by others


Introduction
Transthyretin amyloidosis (ATTR) is an important cause of heart failure with preserved ejection fraction (HFpEF) [1,2,3], especially in patients with increased wall thickness [4]. Cardiac planar radionuclide imaging using 99mTc-labeled bone-seeking radiopharmaceuticals may identify cardiac ATTR amyloid deposits, even in the early course of the disease, and is now widely used as a noninvasive diagnostic criterion in patients without detectable monoclonal protein [5, 6].
After the diagnosis, median survival ranges from 25 to 69 months depending on the transthyretin genotype (i.e., hereditary variant or wild-type ATTR) and the stage of the disease [7,8,9]. Medical therapy using Tafamidis meglumine, that binds to transthyretin and prevents amyloidogenesis, recently demonstrated a reduction in all-cause mortality and cardiovascular-related hospitalizations, offering new therapeutic perspectives in patients with ATTR cardiac amyloidosis. Several studies demonstrated that a high level of cardiac retention of bone radiopharmaceuticals is associated with a decreased survival in patients with ATTR cardiac amyloidosis [10, 11]. However, there is no standardized method for semi-quantitative assessment of cardiac uptake of bone tracers. Besides the visual assessment proposed by Perugini and colleagues [12] to identify patients with cardiac ATTR, several semi-quantitative methods have been proposed to evaluate patients prognosis, including heart to whole-body (H:WB) retention, heart to contralateral lung (H:CL) uptake ratio, and variation of regional left ventricular tracer uptake [10, 13,14,15].
In the context of a new era for medical therapy of ATTR cardiac amyloidosis, there is a need for quantitative approaches that would be useful for diagnosis, assessment of patient prognosis, and also therapeutic response. With the widespread use of cadmium zinc telluride (CZT)-based single-photon emission computed tomography (SPECT) camera, it is now feasible to propose a semi quantitative assessment of a cardiac tracer uptake using either 3D reconstructed acquisition or reprojected planar images [16, 17].
The aim of this study was to compare several indexes of cardiac uptake of bone tracers obtained with CZT SPECT in comparison to conventional planar bone scan acquisition in patients with cardiac ATTR.
Material And methods
Study population
Between October 2015 and March 2019, 97 consecutive patients with suspected cardiac ATTR were referred to the Nuclear Medicine department in two participating centers (Caen University Hospital and Toulouse University Hospital) for planar whole-body bone scintigraphy as part of routine diagnostic investigations. The need for supplemental tomographic acquisition was determined by the nuclear medicine physician on the basis of the results of whole-body scan. The final diagnostic of cardiac ATTR was based on the results of immunofixation electrophoresis of serum and urine, serum free light chain assay, and bone scintigraphy. Patient characteristics and echocardiography results were obtained from hospital records. The investigation conforms with the principles outlined in the Declaration of Helsinki. This retrospective study was approved by our institutional review board.
Bone scintigraphy
Patients were scanned after intravenous injection of 10 MBq/kg of bisphosphonates ([99mTc]TcDPD in Caen and [99mTc]TcHMDP in Toulouse). Whole-body planar images were acquired 3 h after injection, followed by a SPECT acquisition.
Whole-body images were acquired using a conventional Anger camera (Symbia, Siemens, Erlangen, Germany) with low energy, high-resolution collimators and a scan speed of 10 cm/min. Cardiac retention was assessed by the semiquantitative visual score proposed by Perugini et al. [12] from 0 (no uptake) to 3 (uptake greater than bone, bone uptake attenuation, and soft tissue uptake). Additional tomographic acquisition was not performed in the case of Perugini score = 0.
The tomographic imaging was started with a 10-s prescan to help position the detectors on the cardiac area, followed by a 10-min list mode using a dedicated CZT cardiac SPECT camera (D-SPECT; Spectrum Dynamics, Biosensors, Caesarea, Israel) and a 10 % asymmetrical (− 7 to + 9 keV) energy windows centered on 140.5 keV. No scatter correction was performed, and reconstruction was performed using a dedicated workstation provided by the manufacturer. All acquisitions were gated at 16 intervals per cardiac cycle. Left ventricular volumes and ejection fraction were calculated using QGS software (Cedars-Sinai, Los Angeles, CA, USA). In addition to tomographic reconstruction, two planar equivalent images (planograms) were obtained as previously described [17] by projecting and summing all the elementary 2D images that shared the same angle onto one large field of view virtual plane in anterior and 45° left anterior oblique views.
Heart-to-background ratio analysis
Different heart-to-background (H:B) uptake ratio were calculated using planar and SPECT imaging by drawing regions of interest (ROI) manually on the left ventricle and over a background region. Using planar conventional imaging, a ROI was manually drawn over the heart in the anterior view, and then copied and pasted over the contralateral chest, including soft tissue, ribs, and blood pool. On planograms, a circular ROI was drawn over the heart while the size of the background ROI was determined automatically on the x and y dimensions and positioned manually over the contralateral chest (in anterior view) or the mediastinum (in LAO view). Finally, in transaxial reconstructed SPECT images, an elliptic volume of interest (VOI) was drawn manually to encompass the heart and a background VOI was placed over the contralateral lung. As a result, four different H:B uptake ratios were generated: wb-H:B (from planar whole-body image), ant-H:B (from anterior planogram), LAO-H:B (from left anterior oblique planogram), and 3D-H:B (from transaxial slices).
Statistical analysis
Paired data were compared using Student’s t test for paired samples, and unpaired data were compared using ANOVA. Correlations and concordance between quantitative variables were tested using linear regression analysis with Pearson’s correlation and Bland-Altman analysis. Multivariate analysis was performed using a linear model. A two-tailed p value ≤ 0.05 was considered statistically significant. Statistical analysis was performed using JMP® version 11.0 (SAS Institute Inc., Cary, NC).
Results
Study population
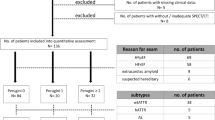
Among the 97 consecutive patients screened in two university hospital (CHU de Caen, n = 51, and CHU de Toulouse, n = 38), 3 were excluded due to a final diagnosis of AL amyloidosis, and 27 were excluded due to incomplete SPECT or whole-body dataset. Finally, SPECT and planar whole-body radionuclide imaging collected from 67 patients were reviewed. Patient characteristics are summarized in Table 1. The cohort was predominantly male (57/67 patients, 85%) with NYHA class II or class III symptoms. Patients received either [99mTc]TcDPD (n = 37) or [99mTc]TcHMDP (n = 30). These patients presented with cardiac hypertrophy and relatively preserved ejection fraction, and 15 patients (25%) were in NYHA class 0–I at the time of investigation.
Cardiac retention of bone radiopharmaceuticals
Whole-body planar images demonstrated an abnormal cardiac retention of bone radiopharmaceuticals, predominantly graded Perugini 2 and 3 (Table 1). All planar methods (whole-body and planograms) yielded H:B uptake ratios that were not statistically different. However, 3D-H:B ratio was dramatically increased compared to planar results in patients with Perugini grade 2 and grade 3 (Table 2). Multivariate analysis using linear model confirmed that H:B uptake ratio was significantly influenced by both the Perugini grade (p < 0.0001) and the calculation method (p < 0.0001).
The correlation was high between all H:B ratios (Table 3). Bland-Altman analysis confirmed a high agreement between all planar methods (Fig. 1).

Bland-Altman analysis showing (1) a high agreement between all planar methods for the measurement of the heart-to-background (H:B) uptake ratio (a-c) and (2) an underestimation of the high H:B uptake ratio using planar methods as shown by the increased difference between 3D-H:B and planar H:B ratios for high H:B ratio values (d–f). WB, whole-body H:B; Ant, anterior planogram H:B; LAO, left anterior oblique planogram H:B
However, compared to planar methods, 3D analyses consistently showed higher values and in addition showed increasing differences with higher uptake values.
Cardiac retention of bone radiopharmaceuticals was correlated to septal wall thickness. As depicted in Fig. 2, the higher correlation between cardiac uptake and septal wall thickness was obtained when using 3D-H:B. Finally, patients with an abnormal right ventricular uptake of bone radiopharmaceutical on CZT SPECT imaging demonstrated higher H:B ratios compared to patients without right ventricular uptake (Table 4).

Correlation of the heart-to-background (H:B) uptake ratio to the septal wall thickness. WB, whole-body H:B; Ant, anterior planogram H:B; LAO, left anterior oblique planogram H:B
Discussion
The results of this study demonstrated that a 3D semi-quantitative analysis of CZT SPECT is feasible and increases the heart-to-background ratio of 99mTc-labeled bone seeking tracer uptake compared to bidimensional methods, with a difference between the two methods increasing with the severity of the disease.
Cardiac ATTR is an underdiagnosed disease, more common than previously estimated [2], and that predominantly affects patients in their seventh and eighth decade of life [18]. Echocardiographic and cardiac magnetic resonance imaging patterns are non-specific, demonstrating a left ventricular hypertrophy that is frequently absent in the early phase. Advanced techniques using speckle-tracking imaging may reveal an apical sparing of longitudinal strain that enhances diagnostic accuracy but remain poorly investigated [19]. In addition to left ventricular hypertrophy, cardiac magnetic resonance imaging may show a late gadolinium enhancement, especially within the subendocardium, that increases diagnostic sensitivity [20]. On the other hand, it has been demonstrated that cardiac uptake of bone radiopharmaceuticals can early identify cardiac ATTR and help distinguish transthyretin from light chain cardiac amyloidosis [5, 11, 12, 21]. Consequently, bisphosphonate ([99mTc]TcDPD, [99mTc]PyP or [99mTc]TcHMDP) scintigraphy is now a key feature in the diagnostic algorithm in patients with suspected cardiac ATTR [5, 22].
However, the visual assessment of cardiac uptake according to the widely used Perugini grading failed to predict patient prognosis [23]. Recent data pointed out that the intensity of cardiac uptake is a powerful predictor of poor cardiac outcome [10, 11]. Rapezzi et al. [11] demonstrated that a H:WB ratio of [99mTc]TcDPD uptake > 7.5 was predictive of major cardiac adverse event. In this study, the calculation of the H:WB ratio required a correction for decay and scan speed and a subtraction of the urinary tract and bladder activity that are potential sources of errors. In a multicenter study, Castano et al. alternatively evaluated 99mTc-PYP cardiac retention by the H:CL ratio of total counts using planar cardiac imaging and demonstrated an increased 5-year mortality in patients with H:CL ≥ 1.6 [10]. Several other indices have been proposed to quantify the amyloid burden using conventional Anger cameras, including heart/skull ratio, SPECT left ventricle/blood pool ratio, and heart/pelvis and heart/mediastinum ratio [13, 21, 24], demonstrating the lack of standardization of nuclear imaging procedures. In a recent study, Gallini et al. evaluated six different indices obtained from planar whole body imaging using conventional Anger camera. Using ROC curve analysis, the sensitivity of these indices ranged from 89 to 100%, with cutoff values ranging from 1.29 to 3.28. In this study, the heart/whole-body ratios were the most accurate in identifying cardiac amyloidosis [13].
Despite the widespread use of dedicated cardiac CZT cameras, this is the first study comparing the assessment of amyloid load using these cameras in comparison with conventional whole-body bone scan. Planar equivalent images, i.e., planograms, were obtained from SPECT acquisition as previously described [17]. The H:B ratio obtained from planograms were significantly lowers than those obtained from 3D images. The count statistics in heart and background regions in the planograms take into account the projection of every anatomic structure that binds the bone radiopharmaceutical, including the rib cage, the sternum, and the soft tissues [25]. Extra-cardiac uptake, including soft tissue involvement, is not constant and varies according to the stage of the disease [23]. On the other hand, the H:B ratio obtained from 3D reconstructed images reflect the heart retention normalized to the lung uptake, a metric that is not influenced by sternum, rib cage, or muscle uptake that are not included in VOIs. Interestingly, Glaudemans et al. [21] using a conventional Anger SPECT camera found an increased left ventricle-to-blood pool ratio in patients with ATTR and left ventricular hypertrophy that was further increased compared to H:WB ratio (4.6 vs. 2.9). Compared to these previous results, we found relatively higher H:B ratio. A possible explanation is the increased sensitivity of dedicated CZT cameras, with a linear count rate response compared to the non-linear response with a saturation at high count rate observed with conventional Anger cameras [26]. Accordingly, our results demonstrated that the underestimation of cardiac retention by planar techniques increases with the mean value of this retention as assessed by 3D CZT SPECT imaging. In addition, 3D H:B provided a good correlation to myocardial thickness, and 3D analysis was able to demonstrate a right ventricular involvement in 30% of the patients, a condition associated with an increased cardiac retention.
Conclusion
The semi-quantitative analysis of 3D CZT SPECT optimized the assessment of bisphosphonate myocardial uptake compared to 2D methods in patients with cardiac amyloidosis.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request
References
Bennani Smires Y, Victor G, Ribes D, et al. Pilot study for left ventricular imaging phenotype of patients over 65 years old with heart failure and preserved ejection fraction: the high prevalence of amyloid cardiomyopathy. Int J Cardiovasc Imaging. 2016;32:1403–13.
González-López E, Gallego-Delgado M, Guzzo-Merello G, et al. Wild-type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur Heart J. 2015;36:2585–94.
Mohammed SF, Mirzoyev SA, Edwards WD, et al. Left ventricular amyloid deposition in patients with heart failure and preserved ejection fraction. JACC Heart Fail. 2014;2:113–22.
Damy T, Costes B, Hagège AA, et al. Prevalence and clinical phenotype of hereditary transthyretin amyloid cardiomyopathy in patients with increased left ventricular wall thickness. Eur Heart J. 2016;37:1826–34.
Gillmore JD, Maurer MS, Falk RH, et al. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation. 2016;133:2404–12.
Elliott PM, Anastasakis A, Borger MA, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014;35:2733–79.
Ruberg FL, Maurer MS, Judge DP, et al. Prospective evaluation of the morbidity and mortality of wild-type and V122I mutant transthyretin amyloid cardiomyopathy: the Transthyretin Amyloidosis Cardiac Study (TRACS). Am Heart J. 2012;164:222–8 e1.
Grogan M, Scott CG, Kyle RA, et al. Natural history of wild-type transthyretin cardiac amyloidosis and risk stratification using a novel staging systeM. J Am Coll Cardiol. 2016;68:1014–20.
Gillmore JD, Damy T, Fontana M, et al. A new staging system for cardiac transthyretin amyloidosis. Eur Heart J. 2018;39:2799–806.
Castano A, Haq M, Narotsky DL, et al. Multicenter study of planar technetium 99 m pyrophosphate cardiac imaging: predicting survival for patients with ATTR cardiac amyloidosis. JAMA Cardiol. 2016;1:880–9.
Rapezzi C, Quarta CC, Guidalotti PL, et al. Role of 99mTc-DPD scintigraphy in diagnosis and prognosis of hereditary transthyretin-related cardiac amyloidosis. JACC Cardiovasc Imaging. 2011;4:659–70.
Perugini E, Guidalotti PL, Salvi F, et al. Noninvasive etiologic diagnosis of cardiac amyloidosis using 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy. J Am Coll Cardiol. 2005;46:1076–84.
Gallini C, Tutino F, Martone R, et al. Semi-quantitative indices of cardiac uptake in patients with suspected cardiac amyloidosis undergoing 99mTc-HMDP scintigraphy. J Nucl Cardiol. 2019. https://doi.org/10.1007/s12350-019-01643-w.
Sperry BW, Vranian MN, Tower-Rader A, et al. Regional variation in technetium pyrophosphate uptake in transthyretin cardiac amyloidosis and impact on mortality. JACC Cardiovasc Imaging. 2018;11:234–42.
Van Der Gucht A, Cottereau A-S, Abulizi M, et al. Apical sparing pattern of left ventricular myocardial 99mTc-HMDP uptake in patients with transthyretin cardiac amyloidosis. J Nucl Cardiol Off Publ Am Soc Nucl Cardiol. 2018;25:2072–9.
Blaire T, Bailliez A, Ben Bouallegue F, Bellevre D, Agostini D, Manrique A. Determination of the heart-to-mediastinum ratio of 123 I-MIBG uptake using dual-isotope ( 123 I-MIBG/ 99m Tc-tetrofosmin) multipinhole cadmium-zinc-telluride SPECT in patients with heart failure. J Nucl Med. 2018;59:251–8.
Bellevre D, Manrique A, Legallois D, et al. First determination of the heart-to-mediastinum ratio using cardiac dual isotope (123I-MIBG/99mTc-tetrofosmin) CZT imaging in patients with heart failure: the ADRECARD study. Eur J Nucl Med Mol Imaging. 2015;42:1912–9.
Dharmarajan K, Maurer MS. Transthyretin cardiac amyloidoses in older North Americans. J Am Geriatr Soc. 2012;60:765–74.
Quarta CC, Solomon SD, Uraizee I, et al. Left ventricular structure and function in transthyretin-related versus light-chain cardiac amyloidosis. Circulation. 2014;129:1840–9.
Martinez-Naharro A, Treibel TA, Abdel-Gadir A, et al. Magnetic resonance in transthyretin cardiac amyloidosis. J Am Coll Cardiol. 2017;70:466–77.
Glaudemans AWJM, van Rheenen RWJ, van den Berg MP, et al. Bone scintigraphy with 99mtechnetium-hydroxymethylene diphosphonate allows early diagnosis of cardiac involvement in patients with transthyretin-derived systemic amyloidosis. Amyloid. 2014;21:35–44.
Seferović PM, Polovina M, Bauersachs J, et al. Heart failure in cardiomyopathies: a position paper from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2019;21:553-76.
Hutt DF, Fontana M, Burniston M, et al. Prognostic utility of the Perugini grading of 99mTc-DPD scintigraphy in transthyretin (ATTR) amyloidosis and its relationship with skeletal muscle and soft tissue amyloid. Eur Heart J Cardiovasc Imaging. 2017;18:1344–50.
Galat A, Van der Gucht A, Guellich A, et al. Early phase 99Tc-HMDP scintigraphy for the diagnosis and typing of cardiac amyloidosis. JACC Cardiovasc Imaging. 2017;10:601–3.
Hutt DF, Quigley A-M, Page J, et al. Utility and limitations of 3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy in systemic amyloidosis. Eur Heart J - Cardiovasc Imaging. 2014;15:1289–98.
Bocher M, Blevis IM, Tsukerman L, Shrem Y, Kovalski G, Volokh L. A fast cardiac gamma camera with dynamic SPECT capabilities: design, system validation and future potential. Eur J Nucl Med Mol Imaging. 2010;37:1887–902.
Acknowledgements
Not applicable
Funding
None
Author information
Authors and Affiliations
Contributions
AM participated in the design of the study, performed the statistical analysis, and drafted the manuscript. DD participated in the design of the study and data processing, SB, CN, and YLB participated in the revision of the manuscript. EC participated in data processing, DL and DA participated in the design of the study, and OL in the design of the study and data statistical analysis. All authors read and approved the final manuscript. This work was presented in part at the EANM Congress 2018.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
French observational studies without any additional therapy or monitoring procedure do not need the approval of a national ethical committee. Accordingly, this retrospective study was approved by our institutional Ethics Committee (CLERS #479).
Consent for publication
Not applicable
Competing interests
D. Agostini declares consultancy for Spectrum Dynamics.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Manrique, A., Dudoignon, D., Brun, S. et al. Quantification of myocardial 99mTc-labeled bisphosphonate uptake with cadmium zinc telluride camera in patients with transthyretin-related cardiac amyloidosis. EJNMMI Res 9, 117 (2019). https://doi.org/10.1186/s13550-019-0584-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13550-019-0584-8