
Abstract
Background
Catheter-based renal sympathetic denervation (RDN) has been considered a potential treatment for therapy resistant hypertension (RHT). However, in a randomized placebo-controlled trial, RDN did not lead to a substantial blood pressure (BP) reduction. We hypothesized that variation in the reported RDN efficacy might be explained by incomplete nerve disruption as assessed by renal 123I–meta-iodobenzylguanidine (123I–mIBG) scintigraphy.
Methods
In 21 RHT patients (median age 60 years), we performed 123I–mIBG scintigraphy before and 6 weeks after RDN. Additionally, we assessed changes in BP (24 h day, night, and average), plasma- and urinary-catecholamines and plasma renin activity (PRA) before and after RDN. Planar scintigraphy was performed at 15 min and 4 h after 123I–mIBG administration. The ratio of the mean renal (specific) counts vs. muscle (non-specific) counts represented 123I–mIBG uptake. Renal 123I–mIBG washout was calculated between 15 min and 4 h.
Results
After RDN office-based systolic BP decreased from 172 to 153 mmHg (p = 0.036), while diastolic office BP (p = 0.531), mean 24 h systolic and diastolic BP (p = 0.602, p = 0.369, respectively), PRA (p = 0.409) and plasma catecholamines (p = 0.324) did not significantly change post-RDN. Following RDN, 123I–mIBG renal uptake at 15 min was 3.47 (IQR 2.26–5.53) compared to 3.08 (IQR 2.79–4.95) before RDN (p = 0.289). Renal 123I–mIBG washout did not change post-RDN (p = 0.230). In addition, there was no significant correlation between the number of denervations and the renal 123I–mIBG parameters.
Conclusions
No changes were observed in renal 123I–mIBG uptake or washout at 6 weeks post-RDN. These observations support incomplete renal denervation as a possible explanation for the lack of RDN efficacy.
Similar content being viewed by others


Background
Reduction of sympathetic nerve activity by catheter-based renal sympathetic denervation (RDN) has raised considerable attention as a new treatment modality for resistant hypertension (RHT). This interest was fueled by the promising results of RDN in the initial open label studies Symplicity HTN-1 and HTN-2 [1,2,3]. However, the recent randomized sham-controlled Symplicity HTN-3 trial did not show a difference in blood pressure (BP) lowering efficacy between RDN and sham treatment [4]. One of the potential causes for the lack of efficacy might be the failure of the RDN procedure to sufficiently ablate renal sympathetic nerves. Yet, a routine technique to measure the extent of renal denervation is lacking and potential causes of insufficient denervation remain hypothetical.
123I–meta-iodobenzylguanidine (123I–mIBG) scintigraphy offers the possibility to evaluate organ specific presynaptic sympathetic nerve activity. mIBG is an analogue of the “false” neurotransmitter guanetidine, a potent neuron blocking agent that acts selectively on sympathetic nerves. mIBG follows similar uptake mechanisms as norepinephrine: as such, mIBG-uptake enables assessment of the intactness and density of the neural tissue. Radiolabelling of mIBG with 123Iodide enables scintigraphic assessment. 123I–mIBG organ uptake and washout reflect sympathetic activity. Uptake of 123I–mIBG reflects the density and functional intactness of the neural tissue within the organ, whereas washout is thought to reflect sympathetic activity [5, 6]. Previously, we tested this technique for visualizing renal sympathetic innervation by showing its ability to detect changes in sympathetic innervation during kidney allograft re-innervation [7].
Based on the inter-individual variation in BP response after RDN, we hypothesized that there is a wide variability in kidney sympathetic denervation following RDN. Secondly, we hypothesized that changes in renal sympathetic activity would relate to changes in BP and neurohormonal activity following RDN. Against this background, we examined changes in renal 123I–mIBG uptake and washout in RHT patients before and after RDN treatment.
Methods
From July 2011 to December 2013, we performed a prospective observational study using 123I–mIBG scintigraphy as a parameter of renal sympathetic activity in patients with RHT undergoing RDN. Objectives were to compare measures of renal 123I–mIBG uptake (uptake at 15 min and washout between 15 min and 4 h) on planar and single photon emission computed tomography-CT (SPECT-CT) images, changes in office based BP and ambulatory BP measurements (ABPM) and neurohormonal activation before and 6 weeks after RDN.
Patients
In the present study, we enrolled 21 consecutive patients aged 40–70 years with a clinical indication for RDN because of therapy resistant hypertension defined as a mean daytime BP ≥ 150/100 mmHg despite the use of three or more anti-hypertensive drugs including or with intolerance to a diuretic [8]. Secondary causes of hypertension (e.g., renal artery stenosis, pheochromocytoma, primary aldosteronism, and hyper- or hypothyroidism) and abnormal renal artery anatomy, including the presence of accessory renal arteries, were ruled out prior to the intervention. Patients with renal insufficiency (estimated glomerular filtration rate (eGFR) < 45 mL/min/1.73 m2) or proteinuria (> 1 g/24 h) or having a pacemaker, implantable cardioverter-defibrillator (ICD), atrial fibrillation, or type 1 diabetes mellitus were excluded.
Antihypertensive treatment was performed according to international guidelines and included instructions on dietary sodium restriction, physical activity, and instructions to remain compliant to antihypertensive medication [8, 9]. Six weeks prior to the first measurements, patients were screened to assess eligibility for study participation. Patients were deemed eligible for study participation if they were at least 3 weeks on stable BP lowering medication prior to the first study visit. BP lowering medication was kept unchanged throughout the study until the final visit 6 weeks after RDN.
When fully informed and willing to participate, patients were asked to provide written informed consent. Six weeks hereafter, office BP and ABPM were measured. Patients were required to maintain the same antihypertensive drug regimen throughout study participation. This study was a part of a larger effort to assess the sympaticolytic potential of RDN with the predetermined idea to assess the effects of RDN on renal 123I–mIBG uptake and washout.
For reference, we used data of five patients (aged 39–66 years) in whom 123I–mIBG was performed of the kidney allograft after recent kidney transplantation (0.1 to 1.5 years after transplantation), whose detailed characteristics are described elsewhere [7]. In summary, all these surgically denervated kidneys functioned well with creatinine clearance rates (calculated from 24 h urine collections) ranging from 54 to 128 ml/min. As a negative control, we also included 123I–mIBG data from a patient with complete renal denervation after autologous kidney transplantation for renal artery stenosis [10]. Although 123I–mIBG is primarily cleared via the kidneys, we have shown that both the cardiac as well as the renal 123I–mIBG parameters (i.e., late heart-to-mediastinal ratio, renal uptake, and renal washout) are not influenced by kidney function [7, 11].
Study protocol
The study protocol met the ethical guidelines of the Declaration of Helsinki (originally adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and last amended in Fortaleza, Brazil 2013) and was approved by the local ethics committee of the Academic Medical Center at the University of Amsterdam (number NL.36755.018.11). All patients gave oral and written informed consent before study inclusion.
Renal sympathetic denervation procedure
The renal denervation procedure was performed via the femoral artery approach by a single highly experienced interventional radiologist (JAR) with > 5 RDN procedures before this study was initiated. RDN was performed by use of radiofrequency energy delivered by the Symplicity renal-denervation catheter (Medtronic Inc., Santa Rosa, California, USA). Prior to the procedure, midazolam 1.0 mg and metoclopramide 10 mg was given intravenously. After inserting a 6 F introducer sheath in the right femoral artery, the guiding catheter was introduced in the aorta and an aortagram was made. The guiding catheter was advanced in the right and left renal artery in no pre-specified order. The denervation catheter was introduced in the renal artery via the guiding catheter. After nitroglycerine 0.2 mg and fentanyl 0.02 mg intravenously, catheter ablations were performed in a helical pattern with the goal of at least 4–6 ablations per renal artery to cover each short axis transaxial quadrant, according to the user’s instruction of the device. No peri-procedural complications occurred.
Blood pressure monitoring
At baseline and 6 weeks after RDN 24 h ABPM was performed using the Spacelabs 90,217 ABPM monitoring device (Spacelabs Healthcare, Issaquah, Washington, USA). During day time between 06.00 am and 23.00 pm, measurements were performed every 15 min and at night-time (i.e., 23.00 pm and 6.00 am) every 30 min. BP readings were accepted when the success rate of the measurements was minimally 70% per 24 h. Patients were blinded to their BP readings. Instructions were given to continue usual daily activities during 24 h of BP recording, but avoiding strenuous exercise. Office brachial BP using appropriate cuff-sizes was measured with a validated semi-automated oscillometric device (Omron 705it, Omron Healthcare Europe BV, Hoofddorp, The Netherlands), while seated and after 5 min rest in a quiet room, three times at 1 min intervals by a trained research assistant or physician. The mean of the last two measurements was recorded as representative of office brachial BP. No BP measurements were performed in the kidney transplant recipient group.
Blood and urine analysis
Plasma renin activity (PRA) (μgA1/L/h) was analyzed using radioimmunoassays. Urine and plasma epinephrine, norepinephrine (NE), metanephrine, and normetanephrine were analyzed using liquid chromatography-mass spectrometry. Epinephrine and NE and were obtained in supine as well as after 5 min in standing position. The delta of supine minus standing position was calculated. Urinary sodium excretion (mmol/24 h), urine creatinine (μmol/L), was calculated from 24 h urine collections obtained before and 6 weeks post-RDN.
123I–mIBG scintigraphy
The protocol of the renal 123I–mIBG scintigraphy has been previously described [7]. In summary, 2 h prior to the administration of 185 MBq (5 mCi ± 10%) 123I–mIBG (AdreView™, GE Healthcare, Eindhoven, the Netherlands) patients received 100 mg potassium-iodide to block thyroid uptake of “free” 123I. In addition subjects were given a single oral dose of furosemide retard 60 mg to promote the urinary excretion of 123I–mIBG. No specific instructions on fluid intake were given to enhance excretion of 123I–mIBG. Anterior and posterior planar semi-whole body images were performed at 15 min and 4 h after administration of 123I–mIBG. A vial with a reference amount of radioactivity of 123I was included in the planar images. Additionally, at 4 h post-injection (p.i.), SPECT-CT (low dose) was performed. The CT-images were used for an adequate anatomical registration of 123I–mIBG uptake.
Since we recently showed that uptake at 15 min p.i. of 123I–mIBG and washout between 15 min and 4 h can detect renal sympathetic reinnervation over time after transplantation, we report in this study the 123I–mIBG uptake on the 15 min p.i. images and analyzed the mean counts/pixel for calculation of washout between 15 min and 4 h [7].
123I–mIBG imaging procedures
The planar images were acquired with a 20% energy window centered at 159 keV, using medium-energy collimators. Anterior and posterior planar semi-whole body acquisitions were used to create geometrical mean images.
123I–mIBG image analysis
An investigator (LCD) analyzed the geometric mean (GM) planar images (Hybrid Viewer™, Hermes Medical Solutions, Stockholm, Sweden) by manually drawing regions of interest (ROI) for kidneys, muscle (M. quadriceps femoris), and the 123I vial. A predefined and fixed ROI for the muscle (50 pixels) was used for all patients.
We analyzed the counts of the left kidney only since scatter or overlay of the liver with a high uptake of 123I–mIBG resulted in poor delineation of the right kidney. Mean counts per pixel per ROI were used to calculate 123I–mIBG uptake: the relative uptake between kidney (specific) versus muscle (nonspecific) quantifies neural uptake of 123I–mIBG and reflects neuron function that results from 123I–mIBG uptake, storage and release. These can be derived using mean counts from the 15 min and 4 h p.i. GM images and the 4 h p.i. 123I–mIBG SPECT-CT images. Washout (WO) between 15 min and 4 h p.i. based on GM images reflects sympathetic activity and was calculated from the kidney-to-muscle ratio between 15 min and 4 h p.i.. Formulas to calculate uptake and washout were
The percentage uptake of the injected dosage of 123I–mIBG was calculated using the actual injected dose and mean counts per pixel in relation to the activity in the 123I–vial. Washout [WO) in the left kidney was calculated from 15 min and 4 h images using skeletal muscle as a reference.
A secondary analysis was focused on the SPECT-CT images. In this method, the transverse CT images were used to optimize anatomical delineation of the kidney contours. The main advantage of this method is the availability of anatomical information obtained from the low dose CT, allowing for a superior delineation of kidneys and subsequently a potential better estimation of the renal 123I–mIBG uptake. ROIs were drawn on the CT-images along the contours of kidney cortices, excluding the calyces. ROIs were then fused into volumes of interest (VOIs) and copied to the co-registered SPECT. Mean counts/voxel expressed 123I–mIBG uptake. VOIs in muscle served as background activity.
Based on the difference in 123I–mIBG uptake, we divided patients with a positive change in 123I–mIBG uptake, i.e., indicating an increase in 123I–mIBG uptake or washout and those with a negative change, i.e., a decrease in 123I–mIBG uptake or washout after RDN.
Statistical analysis
This study was part of a larger effort to study sympatholytic effects of RDN. The sample size has been described elsewhere [12]. Data are presented as medians and interquartile ranges (IQR with 25 and 75 percentiles) and comparisons were performed by non-parametrical tests (Wilcoxon signed rank tests as well as the Mann–Whitney U test). P values below 0.05 were considered statistically significant. All analyses were performed using IBM SPSS Statistics software for Windows version 21.0 (IBM Corp. Armonk, New York, USA).
Results
Baseline characteristics
We studied 21 patients with therapy resistant hypertension (Table 1). The majority of patients were male (71% with a median 60 years) and Caucasian (76%). Median body mass index was 28.0 kg/m2 (24.8–30.5 kg/m2). Type 2 diabetes mellitus was present in 33% and left ventricular hypertrophy, according to electrocardiography voltage criteria, was present in 29% of the patients. A history of a cardiovascular disease (coronary artery disease, angina pectoris, heart failure, stroke, peripheral arterial disease) was present in 48% of the study participants.
Renal 123I–mIBG uptake and washout in the left kidney
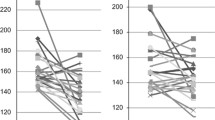
Renal 123I–mIBG uptake was evident in all patients (Fig. 1). The planar derived mean relative uptake of 123I–mIBG of the left kidney at 15 min p.i. did not change significantly from pre RDN 3.08 (2.79–4.95) to post RDN 3.47 (2.26–5.53), p = 0.289 (Table 2). Figure 2 represents pre vs. post RDN 123I–mIBG uptake at 15 min p.i. including recently transplanted kidneys as controls.

Anterior planar and SPECT-CT 123I–mIBG scintigraphy. The planar image (a) shows clear uptake of 123I–mIBG uptake in various organ: liver, urinary bladder and evident uptake of 123I–mIBG in both kidneys. b Shows the ROI on the planar image of the left kidney trying to exclude any pelvic activity. c Shows a coronal slice of the SPECT-CT showing the proximity of the liver to the right kidney. The proximity of the liver to the right kidney can also be appreciated on the planar images (a). Thereby, both planar and SPECT images illustrate the possible impact of liver activity on parameters of 123I–mIBG uptake in the right kidney

Change in renal uptake of 123I–mIBG after RDN. The planar derived mean relative uptake of 123I–mIBG of the left kidney at 15 min p.i. did not change significantly from pre RDN 3.08 (2.79–4.95) to post RDN 3.47 (2.26–5.53), p = 0.289. Included on the right side of the figure is depicted the relative kidney uptake of 123I–mIBG in a group patients with kidney transplantations, serving as a reference
The percentage uptake of the injected dosage of 123I–mIBG in the left kidneys showed a non-significant decrease after RDN from 17.8 to 15.4% (delta − 13%, p = 0.881). Washout rate between 15 min and 4 h p.i. was 41.5% before and 42.7% after RDN, p = 0.230. The SPECT derived uptake at 4 h decreased non-significantly after RDN (1.41 to 1.07, p = 0.526). None of the renal uptake or washout parameters were correlated with kidney function (data not shown).
Number of denervations and renal 123I–mIBG uptake and washout
No significant correlation was found between the number of denervations (left renal artery (4.3 ± 0.6), right renal artery 4.2 ± 0.5), and renal uptake of 123I–mIBG in the left kidney at either 15 min (R = − 0.27, p = 0.243), 4 h p.i. (R = − 0.37, p = 0.103) or 123I–mIBG washout (R = 0.05, p = 0.837).
Effect of RDN on blood pressure, PRA, and catecholamines
Table 3 shows the effect of RDN on blood pressure and catecholamines. RDN resulted in a significant decrease in systolic office BP (p = 0.036), without reducing diastolic BP (p = 0.531). Systolic and diastolic daytime ABPM were not significantly different after denervation. Neither antihypertensive medication nor sodium intake, as inferred from urinary sodium excretion, were significantly different between pre vs. post-RDN (Table 2).
At baseline, plasma and urine catecholamine levels were within reference values. Plasma epinephrine and NE did not change (p = 0.780 and p = 0.324, respectively) nor did the 24 h urinary excretion of metanephrine (p = 0.506) and normetanephrine (p = 0.911) following RDN (Table 3).
Renal 123I–mIBG uptake and washout and blood pressure, PRA, and catecholamines
Except for the correlation between renal 123I–mIBG uptake and office systolic BP (p = 0.018), no correlations were found between any of the renal 123I–mIBG uptake and washout parameters and blood pressure, PRA or catecholamines (Fig. 3).

Renal 123I–mIBG uptake in relation to blood pressure and biochemistry data. There was only a significant correlation between renal 123I–mIBG uptake and office systolic BP (p = 0.018). No other correlations were found between any of the renal 123I–mIBG uptake and washout parameters and blood pressure, PRA or catecholamines
Subgroup analyses
Patients with the largest decrease in 123I–mIBG uptake at 15 min (i.e., delta ≤ − 1.0) (n = 5) and patients with the largest increase in 123I–mIBG uptake at 15 min (i.e., delta of ≥1.0) (n = 5) did not differ in ABPM, kidney function, or catecholamine levels after RDN (Fig. 4 and Table 4), nor did the patients with the largest change (i.e., both increased and decreased) in 123I–mIBG uptake differ in baseline characteristics from the patients without these changes in 123I–mIBG uptake (data not shown).

a Pre- and post-RDN office systolic BP change in patients with the largest decrease in 123I–mIBG uptake. b Pre- and post-RDN mean 24 h systolic BP in patients with the largest decrease in 123I–mIBG uptake. c Pre- and post-RDN office systolic BP change in patients with the largest decrease in 123I–mIBG washout in patients with the largest decrease in 123I–mIBG uptake. d Pre- and post-RDN mean 24 h systolic BP change in patients with the largest decrease in 123I–mIBG washout in patients with the largest decrease in 123I–mIBG washout
In patients with the largest decrease in washout (i.e., delta ≤ − 5.0) (n = 5), there were no changes in BP measurements, neither in catecholamines nor in kidney function (data not shown). In patients with the largest decrease in 123I–mIBG washout, only the 24 h urine metanephrine was significantly higher at baseline compared to patients with the largest increase in washout after RDN (p = 0.045). In patients with the largest increase in 123I–mIBG washout (i.e. delta ≥5.0) (n = 10) there was a difference in office systolic BP only (pre vs. post RDN median 181.5 vs. 158.0 mmHg, p = 0.05), while diastolic BP did not change. In addition this subgroup did not show significant changes in ABPM, kidney function or catecholamines after RDN (data not shown).
No correlations were found between any of the renal 123I–mIBG uptake parameters and BP measurements (data not shown).
Discussion
In the present study we were unable to demonstrate that treatment with RDN results in significant changes in renal 123I–mIBG uptake and washout. These data suggest that RDN does not significantly alter renal sympathetic tone and does not sufficiently denervate renal sympathetic nerves. This is further supported by the finding that ABPM and biochemical markers of sympathetic nerve activity remained unchanged after RDN, while the reduction in office BP was similar compared to Symplicity HTN-1 and HTN-2 [1, 2]. The absence of consistent changes in 123I–mIBG uptake and washout as well as the lack of a sustained BP decrease after RDN suggests that the present RDN technique fails to achieve adequate denervation of the kidneys. The degree of renal sympathetic nerve disruption required for inducing a sustained BP response remains unclear, but likely falls short with the current RDN technique. The lack of efficacy may be related to the number of ablations, since in a subset of patients of Symplicity HTN-3 a more profound BP decrease was observed in patients with more ablations, suggesting a relation between the quantity of ablations and the BP lowering effects [4]. This effect, however, was also observed in patients receiving sham treatment. We found no association between the number of ablations and renal 123I–mIBG uptake or washout, while the number of denervations in our study was similar to the Symplicity HTN-1 and HTN-2 trials that demonstrated a significant decrease in office BP [1, 2].
In a post-mortem study of a patient who received RDN it was shown that nerves in the (peri-) adventitial parts of the renal artery were unaffected, indicating that interruption of the nerve fiber continuity had not been successful [13]. This suggests that the ablation pulse may not be sufficient to generate adequate denervation of renal sympathetic nerves [14]. A previous study using NE spill-over to assess the effect of the nerve fiber continuity had not been successful [13]. In another study, using NE spill-over to assess the effect of RDN on renal sympathetic activity in 10 patients with resistant hypertension showed that RDN reduced NE spill-over by 47% (95% CI 28–65%) [15]. In the present study, we could not replicate these findings.
Besides lack of procedural effectiveness, this discrepancy could also be explained by differences in population characteristics or technical shortcomings of 123I–mIBG scintigraphy. The patients in our study were however fully comparable to the populations studied in Symplicity HTN-1 and Symplicity HTN-2.
Although, we used ABPM instead of office BP to include patients with resistant hypertension, baseline office BP in our study and the number of BP lowering drugs were comparable to that observed in Symplicity HTN-1 and Symplicity HTN-2. In addition, office BP was reduced to a similar extent with a decrease of 29 mmHg for systolic office BP following RDN. All other baseline parameters of our study population were similar to that of previous studies [1, 2, 4]. In kidney transplant recipients we recently showed that uptake at 15 min p.i. of 123I–mIBG and washout is correlated with time after transplantation independent of kidney graft function [7]. This suggests that renal 123I–mIBG scintigraphy can be used to assess differences in renal innervation.
We previously showed that cardiac sympathetic activity did not change after RDN [12]. This is also supported by the lack of change in neurohormonal activation following RDN in the present and in previous studies [16, 17]. Whether this is caused by insufficient denervation or results from a limited overall contribution of renal nerves in determining efferent sympathetic activity could not be assessed because quality parameters for successful RDN are lacking. In the present study we show that the lack of change in renal sympathetic activity may be caused by an inability of RDN to cause a sufficient decrease in afferent sympathetic nerve activity as 123I–mIBG-uptake did not change significantly.
The amount of published data on renal 123I–mIBG imaging for the assessment of renal sympathetic innervation is very limited. In addition to our own data, Takamura et al. showed that renal 123I–mIBG scintigraphy was associated with measurements of muscle sympathetic nerve activity (as a measure of generalized sympathetic outflow) in patients with primary hypertension [18]. In line with our findings, these authors concluded that renal 123I–mIBG scintigraphy could be a non-invasive clinical tool for assessing renal sympathetic nerve function.
A few limitations of our study merit discussion. Firstly, it remains possible that the modulation of sympathetic nerve activity (SNA) induced by RDN lies below the detection level of 123I–mIBG. However, it may well be that sympathicolysis is achieved by RDN but that this does not influence BP nor activity of the renin-angiotensin system and 123I–mIBG parameters. Radiotracer dilution NE spill-over for organ specific assessment of sympathetic nerve activity is an alternative to 123I–mIBG scintigraphy. Although this technique is considered the gold standard, its application is limited by its invasive nature. Moreover a widespread use of the technique is restricted by the poor availability of the required compounds. Furthermore, 123I–mIBG is primarily cleared via the kidneys and therefore kidney function may have influenced our data. However, we have shown that both cardiac and renal 123I–mIBG parameters are not influenced by kidney function [7, 11]. Finally, we were aware of the potential influence of antihypertensive medication (calcium blocking agents, beta blocking agents) that may alter sympathetic drive and thereby uptake of 123I–mIBG. In two patients, BP lowering medication had to be tapered because of hypotension post RDN. In the remaining patients, however, BP lowering medication and sodium excretion were unchanged during the study period. We therefore feel that changes in antihypertensive medication do not explain the lack of change in the 123I–mIBG parameters.
In conclusion, we could not observe significant changes in functional kidney denervation as assessed with 123I–mIBG scintigraphy following RDN with the Symplicity Catheter System. Our data suggest that the lack of BP lowering efficacy in the sham-controlled Simplicity HTN-3 study may be related to lack of procedural effectiveness. In comparison to available clinical tools, renal 123I–mIBG scintigraphy is minimally invasive and more widely available for clinical use. For future studies, renal 123I–mIBG scintigraphy may be used as a parameter to assess RDN effectiveness.
Abbreviations
- 123I–mIBG:
-
123I–meta-Iodobenzylguanidine
- ABPM:
-
Ambulatory blood pressure measurement
- BP:
-
Blood pressure
- eGFR:
-
Estimated glomerular filtration rate
- HTN:
-
Hypertension
- MDRD:
-
Modification of diet in renal disease
- NE:
-
Norepinephrine
- p.i.:
-
Post-injection
- PRA:
-
Plasma renin activity
- RDN:
-
Catheter based renal sympathetic denervation
- ROI:
-
Region of interest
- RTH:
-
Resistant hypertension
- SNA:
-
Sympathetic nerve activity
- SPECT:
-
Single photon emission computed tomography
References
Esler MD, Krum H, Sobotka PA, Schlaich MP, Schmieder RE, Bohm M. Renal sympathetic denervation in patients with treatment-resistant hypertension (the Symplicity HTN-2 trial): a randomised controlled trial. Lancet. 2010;376(9756):1903–9. https://doi.org/10.1016/s0140-6736(10)62039-9.
Krum H, Schlaich MP, Sobotka PA, Bohm M, Mahfoud F, Rocha-Singh K, et al. Percutaneous renal denervation in patients with treatment-resistant hypertension: final 3-year report of the Symplicity HTN-1 study. Lancet. 2014;383(9917):622–9. https://doi.org/10.1016/s0140-6736(13)62192-3.
Schlaich MP, Sobotka PA, Krum H, Whitbourn R, Walton A, Esler MD. Renal denervation as a therapeutic approach for hypertension: novel implications for an old concept. Hypertension. 2009;54(6):1195–201. https://doi.org/10.1161/hypertensionaha.109.138610.
Bhatt DL, Kandzari DE, O'Neill WW, D'Agostino R, Flack JM, Katzen BT, et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370(15):1393–401. https://doi.org/10.1056/NEJMoa1402670.
Patel AD, Iskandrian AE. MIBG imaging. J Nucl Cardiol. 2002;9(1):75–94.
Somsen GA, Verberne HJ, Fleury E, Righetti A. Normal values and within-subject variability of cardiac I-123 MIBG scintigraphy in healthy individuals: implications for clinical studies. J Nucl Cardiol. 2004;11(2):126–33. https://doi.org/10.1016/j.nuclcard.2003.10.010.
Dobrowolski LC, Verberne HJ, van den Born BJ, ten Berge IJ, Bemelman FJ, Krediet CT. Kidney transplant (123)I-mIBG Scintigraphy and functional sympathetic reinnervation. Am J Kidney Dis. 2015;66(3):543–4. https://doi.org/10.1053/j.ajkd.2015.04.049.
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, et al. 2007 guidelines for the Management of Arterial Hypertension: the task force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hyperten. 2007;25(6):1105–87. https://doi.org/10.1097/HJH.0b013e3281fc975a.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. The seventh report of the joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289(19):2560–72. https://doi.org/10.1001/jama.289.19.2560.
Dobrowolski LC, Eeftinck Schattenkerk DW, Idu MM, van den Born BJ, Verberne HJ. Renal 123I-MIBG Scintigraphy before and after kidney autotransplantation. Clin Nucl Med. 2015;40(10):810–1. https://doi.org/10.1097/rlu.0000000000000901.
Verberne HJ, Verschure DO, Somsen GA, van Eck-Smit BL, Jacobson AF. Vascular time-activity variation in patients undergoing (1)(2)(3)I-MIBG myocardial scintigraphy: implications for quantification of cardiac and mediastinal uptake. Eur J Nucl Med Mol Imaging. 2011;38(6):1132–8. https://doi.org/10.1007/s00259-011-1783-3.
van Brussel PM, Eeftinck Schattenkerk DW, Dobrowolski LC, de Winter RJ, Reekers JA, Verberne HJ, et al. Effects of renal sympathetic denervation on cardiac sympathetic activity and function in patients with therapy resistant hypertension. Int J Cardiol. 2016;202:609–14. https://doi.org/10.1016/j.ijcard.2015.09.025.
Vink EE, Goldschmeding R, Vink A, Weggemans C, Bleijs RL, Blankestijn PJ. Limited destruction of renal nerves after catheter-based renal denervation: results of a human case study. Nephrol Dial Transplant. 2014;29(8):1608–10. https://doi.org/10.1093/ndt/gfu192.
Sakakura K, Ladich E, Cheng Q, Otsuka F, Yahagi K, Fowler DR, et al. Anatomic assessment of sympathetic peri-arterial renal nerves in man. J Am Coll Cardiol. 2014;64(7):635–43. https://doi.org/10.1016/j.jacc.2014.03.059.
Krum H, Schlaich M, Whitbourn R, Sobotka PA, Sadowski J, Bartus K, et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet. 2009;373(9671):1275–81. https://doi.org/10.1016/s0140-6736(09)60566-3.
Ewen S, Cremers B, Meyer MR, Donazzan L, Kindermann I, Ukena C, et al. Blood pressure changes after catheter-based renal denervation are related to reductions in total peripheral resistance. J Hyperten. 2015;33(12):2519–25. https://doi.org/10.1097/hjh.0000000000000752.
Ezzahti M, Moelker A, Friesema EC, van der Linde NA, Krestin GP, van den Meiracker AH. Blood pressure and neurohormonal responses to renal nerve ablation in treatment-resistant hypertension. J Hyperten. 2014;32(1):135–41. https://doi.org/10.1097/HJH.0b013e3283658ef7.
Takamura M, Murai H, Okabe Y, Okuyama Y, Hamaoka T, Mukai Y, et al. Significant correlation between renal 123I-metaiodobenzylguanidine scintigraphy and muscle sympathetic nerve activity in patients with primary hypertension. J Nucl Cardiol. 2017;24(2):363–71. https://doi.org/10.1007/s12350-016-0760-4.
Acknowledgements
We gratefully acknowledge Edwin Poel for his help in acquiring the 123I-mIBG images.
Funding
CTPK received grants from the Dutch Kidney Foundation (IP-11.40 and KJPB12.29, Bussum, The Netherlands) and from ZonMW Clinical Fellowship (40007039712461), Zorg Onderzoek Nederland/Medische Wetenschappen (ZonMW, Den Haag, The Netherlands). This support is gratefully acknowledged.
Author information
Authors and Affiliations
Contributions
LD carried out the patient recruitment, performed the image analysis and statistical analysis, and drafted the manuscript. DE carried out the patient recruitment and helped to draft the manuscript. CK participated in the design of the study. PB carried out the patient recruitment. LV participated in the design of the study. FB participated in the design of the study. JR conducted the renal denervation procedures. BB conceived of the study, participated in its design and coordination, and helped to draft the manuscript. HV conceived of the study, participated in its design and coordination, and helped to draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Dobrowolski, L.C., Eeftinck Schattenkerk, D.W., Krediet, C.T.P. et al. Renal sympathetic nerve activity after catheter-based renal denervation. EJNMMI Res 8, 8 (2018). https://doi.org/10.1186/s13550-018-0360-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13550-018-0360-1