
Abstract
Background
Diabetic foot (DF) is one of the most common and serious complications of diabetes mellitus (DM), which brings great psychological and economic pressure to patients. This study aimed to evaluate the efficacy of stem cells in the treatment of diabetic foot.
Methods
All relevant studies in Cochrane, Embase, PubMed, Web of Science, China National Knowledge Infrastructure, and WanFang databases were systematically searched for meta-analysis. The outcomes consisted of ulcer or wound healing rate, amputation rate, new vessels, ankle–brachial index (ABI), transcutaneous oxygen pressure (TcPO2), pain-free walking distance, and rest pain score. Dichotomous outcomes were described as risk ratios (RR) with 95% confidence intervals (CIs), while continuous data were presented as standardized mean differences (SMDs) with 95% CIs. Statistical analysis was performed with RevMan 5.3 software.
Results
A total of 14 studies with 683 participants were included in the meta-analysis. Meta-analysis showed that stem cell therapy was more effective than conventional therapy in terms of ulcer or wound healing rate [OR = 8.20 (5.33, 12.62)], improvement in lower extremity ischemia(new vessels) [OR = 16.48 (2.88, 94.18)], ABI [MD = 0.13 (0.04, 0.08)], TcO2[MD = 4.23 (1.82, 6.65)], pain-free walking distance [MD = 220.79 (82.10, 359.48)], and rest pain score [MD = − 1.94 (− 2.50, − 1.39)], while the amputation rate was significantly decreased [OR = 0.19 (0.10, 0.36)].
Conclusions
The meta-analysis of the current studies has shown that stem cells are significantly more effective than traditional methods in the treatment of diabetic foot and can improve the quality of life of patients after treatment. Future studies should conduct large-scale, randomized, double-blind, placebo-controlled, multicenter trials with high-quality long-term follow-up to demonstrate the most effective cell types and therapeutic parameters for the treatment of diabetic foot.
Similar content being viewed by others


Introduction
Diabetes mellitus is one of the most common chronic metabolic disorders, with 536.6 million people living with diabetes worldwide in 2021, and it is estimated that this number will rise to 783.2 million in 2045 [1]. According to International Diabetes Federation (IDF) estimates, around 50% of people with diabetes are unaware of their condition [2, 3]. DM brings a heavy psychological and financial burden to patients, and diabetes-related health expenditures were estimated at 966 billion USD in 2021 [1]. Diabetic foot is one of the most common and serious complications, and up to 20% of diabetic patients require hospitalization for DF [4]. Neuropathy and ischemia are the main pathological changes of the DF, leading to ulceration and, in severe cases, increased risk of amputation or death [5, 6].
Current standard regimens for DF treatment include metabolic control and comorbidity treatment, infection treatment, tissue perfusion restoration, local ulcer debridement care, wound dressings, pressure off-loading, vascular surgery, and other procedures [7,8,9]. Chronic diabetic foot is characterized by a damaged regeneration process. Most of the current treatment methods for DF target a single factor of wound healing, while stem cell treatment of DF can correct the factors leading to long-term wound healing through various mechanisms [10, 11]. The mechanisms include promoting collagen deposition, promoting new blood vessel formation, and improving lower extremity ischemia and inflammation [12]. In recent years, a large number of clinical trials have demonstrated the potential of stem cells in the treatment of DF [11].
Although several meta-analyses have reported the efficacy of stem cells in the treatment of diabetic ulcers, their sample size is small, and the outcome indicators are relatively single [13,14,15,16]. To more fully demonstrate the accuracy of the conclusions, it is necessary to include more studies to update the meta-analysis. Our study included more clinical trials and analyzed multiple indicators of DF prognosis.
Material and methods
Information sources and search strategy
We systematically searched Cochrane, Embase, PubMed, Web of Science, China National Knowledge Infrastructure, and WanFang databases for all related literature works. The final search was updated on April 10, 2022, using the terms (("stem cell*"[Title/Abstract] OR "bone marrow"[Title/Abstract] OR "progenitor cell*"[Title/Abstract] OR "lipoaspirate cell*"[Title/Abstract] OR "mononuclear cell*"[Title/Abstract]) AND ("diabetic*"[Title/Abstract] OR "diabetic*"[Title/Abstract])) AND ("wound"[Title/Abstract] OR "ulcer"[Title/Abstract] OR "foot"[Title/Abstract] OR "ischemia"[Title/Abstract] OR "ischaemia"[Title/Abstract]. The publication language was restricted to Chinese and English. The original and review articles were manually identified, and the references that met the requirements were included in this study.
Eligibility criteria
The studies were eligible if they adhered to the following criteria: (1) publication in English or Chinese language, (2) only controlled trials involving human subjects, (3) recruit patients with diabetic foot and divide them into a local treatment group using stem cells or a control group (with no treatment or placebo), and (4) report of one or more outcomes regarding the healing of the ulcers or wound, amputation, new vessels, ABI, TcPO2, pain-free walking distance, and rest pain.
Study selection and data extraction
Two authors (JH Z and LF Z) independently performed the literature search, data extraction, and quality assessment process according to the inclusion criteria. All disputes between the two authors were resolved by discussion with the third author (ZX L). Studies selection is based on title and abstract, with full text reviewed as necessary. The following data were extracted from studies that met the inclusion criteria: countries of the studies, characteristics of participants, year of publication, study design, intervention and regimen details, clinical endpoints, and follow-up period. We extracted ulcer or wound healing rate, amputation rate, new vessels, ABI, TcPO2, pain-free walking distance, and rest pain data to evaluate the effect of stem cell therapy on diabetic foot. Safety assessment included any adverse events (AEs) during stem cell therapy.
Quality assessment
The methodology of included systematic reviews was evaluated using the Cochrane Risk of Bias tool; evaluation indicators include: (1) whether the method of random sequence generation is correct (selection bias), (2) whether to achieve allocation concealment (selection bias), (3) whether to use blind methods for participants and implementers (performance bias), (4) whether to use blindness for outcome measurers (detection bias), (5) whether the result data are complete (attrition bias), (6) whether to report selectively (reporting bias), and (7) other bias. RevMan version 5.3 to generate the risk of bias tables. Study quality was assessed by one reviewer and checked by another. Any differences were resolved through discussion.
Data synthesis and analysis
A meta-analysis of only controlled trials including stem cell therapy regimens for the diabetic foot was performed. For these dichotomous results, we used estimated odds ratios (ORs) and 95% confidence intervals, while continuous data were presented as standardized mean differences (SMDs) with 95% CIs. I2 was used to assess heterogeneity among included studies, and if I2 ≤ 50%, we used a fixed-effects model. If I2 > 50%, it is considered that there is statistically significant heterogeneity [17], and we choose a random effect model to combine the results to reduce the influence of heterogeneity. Sensitivity analyses were performed to examine studies that contributed to heterogeneity. Subgroup analyses were performed to assess the impact of certain study characteristics on outcomes with high heterogeneity. Funnel plot asymmetry was measured to assess publication bias. Probability values of < 0.05 were considered statistically significant. All statistical analyses were conducted using RevMan Software (Version 5.3. Copenhagen: The Nordic Cochrane Centre, the Cochrane Collaboration, 2014).
Results
Search results
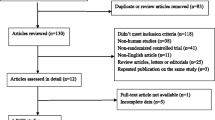
The latest version of the PRISMA flowchart shows the literature screening process used in our report (Fig. 1). A total of 7681 potentially relevant studies were identified in the literature search, 7173 records were marked as ineligible by automation tools, and 216 of them were duplicates. Then, 292 studies were excluded after screening the titles and abstracts, and 23 studies were excluded after screening the full text. The remaining 14 eligible publications were collected for this meta-analysis.

Flow chart of study selection in the meta-analysis
Studies and patient characteristics
A total of 14 [18,19,20,21,22,23,24,25,26,27,28,29,30,31] studies with 683 participants were included in the meta-analysis, of which 10 [18,19,20,21, 25,26,27,28,29,30] were RCTs, 3 [23, 24, 31] were controlled clinical studies, and 1 [22] was a retrospective study. The studies were performed in China [18, 21, 27, 30, 31], India [19, 20], Korea [24], Germany [25], Turkey [29], Czech Republic [22, 23], Iran [28], and Italy [26]. As for the stem cells applied, 2 used peripheral blood mononuclear cells (PBMNCs) [24, 29], 2 used bone marrow-derived mesenchymal stem cells (BMMSCs) [19, 27], 3 used bone marrow-derived mononuclear cells (BMMNCs) [23, 25, 27], 1 used bone marrow-enriched tissue repair cells (BMTRCs) [25], 1 used CD133+ cells [31], 1 used micro-fragmented adipose tissue [26]. 1 used human processed lipoaspirate cells (HPLAC) [24], 1 used bone marrow-derived cells (BMDC) [20], 1 used peripheral blood progenitor cells (PBPCs) [23], 1 used BMMNCs + PBPCs [22], and 2 used human umbilical cord mesenchymal stem cells (HUCMSCs) [21, 30]. The follow-up duration period varied from 2 to 18 months. Characteristics of included studies are presented in Table 1.
Quality of evidence
The risk of bias assessment of included studies using the Cochrane assessment tool is shown in Fig. 2a, b. The overall quality of included studies was moderate, and the quality of included studies varied from low to high. The included studies included 10 RCTs of relatively high quality. However, a total of 7 RCTs reported detailed methods for sequence generation and 4 RCTs did not mention specific methods for using blind methods for participants and implementers, which were therefore defined as uncertain risk. Three clinically controlled studies and 1 retrospective study were of low quality.

a: Risk of bias graph. b: Summary of study risk bias analysis
Ulcer and wound healing rate
Among the 14 included studies, 12 trials [18,19,20,21, 23,24,25,26,27,28,29, 31] reported detailed ulcer or wound healing rates. The meta-analysis showed that the healing rate of ulcers or wounds in the cell-treated group was higher than in the control group (201/263 vs 92/270 OR 8.20, 95% CI 5.33 to 12.62, I2 = 12%) (Fig. 3).

Forest plot showing the effect of stem cell therapy on ulcer or wound healing rate
Amputation rate
Eight trials [18, 22, 23, 25, 27,28,29, 31] reported detailed amputation rates. The meta-analysis showed that the rate of amputation in the stem cell treatment group was significantly lower than in the control group (13/184 vs 63/227 OR 0.19, 95% CI 0.10 to 0.36, I2 = 0%) (Fig. 4).

Forest plot showing the effect of stem cell therapy on amputation rate
New vessels
Four studies [18, 25, 27, 29] reported detailed new angiogenesis rates. The meta-analysis showed that the rate of new angiogenesis was significantly higher in the stem cell treatment group than in the control group (49/92 vs 7/111 OR 16.48, 95% CI 2.88 to 94.18, I2 = 65%) (Fig. 5a). Due to its high heterogeneity of I2 = 65%, we performed subgroup analysis according to ethnic skin color. Meta-analyses of 2 studies [18, 27] in the yellow race showed that the rate of new angiogenesis in the stem cell treatment group was higher than that in the control group (33/50 vs 2/85 OR 51.19, 95% CI 13.16 to 199.09, I2 = 31%); Meta-analyses of 2 studies [25, 29] in the white race showed that the rate of new angiogenesis in the stem cell treatment group was higher than that in the control group (16/42 vs 7/111 OR 3.06, 95% CI 0.92 to 10.22, I2 = 0%)(Fig. 5b).

a: Forest plot showing the effect of stem cell therapy on new vessels. b: Subgroup analysis showed a forest plot of the effects of stem cell therapy on new vessels
ABI
Five studies [18, 28,29,30,31] reported detailed ABI. Meta-analysis shows higher ABI in cell therapy group than in control group (MD 0.13, 95% CI 0.04 to 0.08, I2 = 53%) (Fig. 6a). We performed subgroup analysis according to ethnic skin color. Meta-analyses of 3 studies [18, 30, 31] in the yellow race showed that the ABI in the stem cell treatment group was higher than that in the control group (MD 0.06, 95% CI 0.02 to 0.10, I2 = 24%); meta-analyses of 2 studies [28, 29] in the white race showed that the ABI in the stem cell treatment group was higher than that in the control group (MD 0.08, 95% CI 0.04 to 0.12, I2 = 14%) (Fig. 6b).

a: Forest plot showing the effect of stem cell therapy on ABI. b: Subgroup analysis showed a forest plot of the effects of stem cell therapy on ABI
TcPO2
Three studies [29,30,31] reported detailed TcPO2. Meta-analysis shows that TcPO2 in the stem cell treatment group is higher than in the control group (MD 4.23, 95% CI 1.82 to 6.65, I2 = 65%) (Fig. 7a). Subgroup analysis showed that a meta-analysis of 2 studies [30, 31] in the yellow race showed that the TcPO2 of the stem cell treatment group was higher than that of the control group (MD 3.60, 95% CI 2.60 to 4.59, I2 = 0%) (Fig. 7b).

a Forest plot showing the effect of stem cell therapy on TcPO2. b: Subgroup analysis showed a forest plot of the effects of stem cell therapy on TcPO2
Pain-free walking distance
Only 2 studies [18, 19] reported detailed pain-free walking distances. Meta-analysis shows that the pain-free walking distance in the stem cell treatment group is higher than that in the control group (MD 220.79, 95% CI 82.10 to 359.48, I2 = 0%) (Fig. 8).

Forest plot showing the effect of stem cell therapy on Pain-free walking distance
Rest pain score
Only 2 studies reported detailed rest pain scores. The meta-analysis showed that the rest pain score of the stem cell treatment group was lower than that of the control group (MD − 1.94, 95% CI − 2.50 to − 1.39, I2 = 0%) (Fig. 9).

Forest plot showing the effect of stem cell therapy on rest pain score
Sensitivity analyses
Results of sensitivity analyses are shown in Additional file 1: Figure S1, Additional file 2: Figure S2, and Additional file 3: Figure S3. The results of new vessels, ABI, and TcPO2 were highly heterogeneous, and the results were consistent with the original analysis after excluding the studies that caused the high heterogeneity.
Adverse events
Adverse events were reported in only 5 studies [22, 23, 26, 27, 30] and were mainly pain in the recipient area and leg edema after stem cell transplantation.
Publication bias
Publication bias was qualitatively examined using funnel plots. The funnel plots of the effect of stem cell therapy on lower extremity ulcers or wound healing and the effect of amputation were nearly symmetrical on visual inspection, indicating no clear evidence of publication bias, as shown in Fig. 10 a and b.

a, b: Publication bias in relation to ulcer or wound healing rate (10a) and amputation rate (10b)
Discussion
According to the IDF report, the number of diabetes patients worldwide increased by 114.6 million from 2016 to 2021 and continues to rise due to current high-fat, high-sugar diets, sedentary lifestyles, and reduced physical activity [1, 14]. Diabetic foot is the most common chronic complication of diabetes. Diabetic foot is the most common chronic complication of diabetes. Its pathological manifestations are arteriosclerosis, occlusion, and neuropathy in the lower extremities, which leads to local accidental injury of the skin tissue of the foot or postoperative wounds that are difficult to heal and gradually form ulcers, resulting in amputation or even death [8, 32]. Diabetic foot not only reduces the quality of life, but also creates a huge economic burden, including direct and indirect costs of DF care and treatment. The traditional methods of treating diabetic foot are mainly systematic medical treatment, lower extremity surgical blood flow reconstruction, and wound debridement care [8, 12]. Drugs cannot fundamentally solve arterial stenosis, occlusion, and ischemia. Many small arterial lesions and the lack of distal arterial outflow tract, accompanied by cardiovascular and cerebrovascular diseases, are great challenges in surgery [9, 33]. Stem cells, platelet-rich plasma (PRP), and biomaterials show great potential in wound healing [34,35,36,37]. Angelis [35] et al. achieved good results in the treatment of chronic wounds caused by diabetes and vascular diseases by using the biological scaffolds made by platelet-rich plasma and hyaluronic acid, which not only accelerates the wound healing, but also reduces the pain of patients. Nicoli [38] et al. used PRP gel and Hyalomatrix PA to promote angiogenesis and stimulate wound dermal regeneration for wound healing after wide excision of severe Hidradenitis suppurativa. Porcine dermal matrix, double-layer dermal substitute, dermal regeneration template, and other biological materials have achieved good results in tissue reconstruction and repair in clinical practice [36, 39,40,41,42].
Stem cells are promising as a new treatment for diabetic foot. At present, the main types of stem cells and somatic cells used in the clinic are mesenchymal stem cells and mononuclear cells [11]. MSCs can be derived from umbilical cord, bone marrow, hair follicles, adipose tissue, gums, dental pulp, and menstrual blood, which are mainly used to treat diabetic foot by promoting angiogenesis, prolonging the reduction in the inflammatory period, and enhancing the content of type I collagen [12, 19, 21, 26, 27, 30, 43, 44]. Adipose-derived stem cells and adipose stem cells-rich stromal vascular fractions play an important role in chronic wound repair and regeneration after tissue defects [34, 45, 46]. Mononuclear cells are derived from bone marrow and peripheral blood, which have progenitor and stem cell characteristics, not require in vitro expansion. Mononuclear cells treat diabetic foot by promoting angiogenesis, reducing inflammation, enhancing re-epithelialization, and increasing collagen deposition [11, 18, 23, 27,28,29, 31]. Although somatic cells and stem cells are effective in the treatment of diabetic foot and there is some overlap in mechanism, it is still not clear which type of cells has a better therapeutic effect, and some high-quality clinical studies are still needed to explore.
Guo [14] et al. first conducted a meta-analysis of autologous stem cells in the treatment of diabetic foot ulcers in 2017. The results showed that compared with the control group, stem cells had better efficacy in the treatment of diabetic foot ulcers. However, only 4 trials were included, resulting in a low degree of confidence in the results. The meta-analysis reported by Shu [16] et al. in 2018 analyzed the efficacy of autologous stem cells in the treatment of diabetic foot ulcers, ABI and TcPO2; a total of 7 trials were included. The meta-analysis reported by Dai [13] et al. in 2020 included a total of 8 trials, which not only analyzed the efficacy of autologous stem cells in the treatment of diabetic foot ulcers, but also analyzed the amputation rate. The results showed that the amputation rate decreased after stem cell therapy. Fewer studies were included in these meta-analyses, and perhaps due to time reasons, fewer studies have been published on stem cells for the treatment of diabetic foot ulcers. The outcome indicators of DF treatment include not only the ulcer healing rate and amputation rate, but also the improvement in lower extremity ischemia and whether the patient's quality of life is improved after treatment.
This meta-analysis included 14 studies involving 683 patients with DF, which aimed to compare the efficacy of stem cell-based therapy with traditional treatments. After combining the study results, we found that after stem cell treatment, the ulcer or wound healing rate, the number of new vessels in the lower extremity, TcPO2, ABI, and pain-free walking distance increased significantly, while the amputation rate and rest pain score decreased significantly. This proves that the patient's physical condition and quality of life have been significantly improved after stem cell therapy. No significant change was observed with regard to the outcomes investigated, with the heterogeneity in the new vessels, ABI, and TcPO2 group that was decreased following the ethnic subgroup analysis. This implies that the therapeutic effect of stem cells is consistent in different races.
Although the sample size of our meta-analysis is large and the analysis indicators are comprehensive, there are still some limitations. (1) The included studies did not distinguish stem cells from other types of somatic cells. (2) Some of the included studies were of low quality, 4 were non-randomized controlled studies, and 3 RCTs did not describe specific methods for using blind methods for participants and implementers in detail, leading to combined conclusions. (3) Few studies are reporting the results of TcPO2, pain-free walking distance, and rest pain, which leads to lower reliability of the results after combined analysis.
Conclusion
The meta-analysis of the current studies has shown that stem cells are significantly more effective than traditional methods in the treatment of diabetic foot and can improve the quality of life of patients after treatment. However, which cell type is most efficacious and the optimal parameters for cell therapy have not been determined. Future studies should conduct large-scale, randomized, double-blind, placebo-controlled, multicenter trials with high-quality long-term follow-up to demonstrate the most effective cell types and therapeutic parameters for the treatment of diabetic foot.
Availability of data and materials
DOI: https://doi.org/10.2337/diacare.28.9.2155, https://doi.org/10.1089=rej.2009.0872, https://doi.org/10.1111/j.1524-475X. 2010.00593.x, https://doi.org/10.1016/j.diabres.2010.12.010, https://doi.org/10.1111/j.1742-1241. 2011. 02,886.x, https://doi.org/10.1016/j.jdiacomp.2011.11.007, https://doi.org/10.1002/dmrr.2399, https://doi.org/10.1055/s-0032-1311646, https://doi.org/10.1016/j.jcyt.2014.08.010, https://doi.org/10.1055/s-0042-103684, https://doi.org/10.1155/2016/6925357, https://doi.org/10.1186/s13287-019-1328-4, PMID: 21,904,014, An article from CNKI: https://kns.cnki.net/kcms/detail/detail.aspx?dbcode=CJFD&dbname=CJFD2014&filename=ZMGY201404005&uniplatform=NZKPT&v=C9hVdG5mO8RB4NZ2y-GB_VetSFdofkdl1G98_Mkpn-f6l0luiA_hf1BMvzcLE1OE.
References
Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183: 109119.
Ogurtsova K, Guariguata L, Barengo NC, et al. IDF diabetes atlas: global estimates of undiagnosed diabetes in adults for 2021. Diabetes Res Clin Pract. 2022;183: 109118.
Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas, 9(th) edition. Diabetes Res Clin Pract. 2019;157: 107843.
Bandyk DF. The diabetic foot: pathophysiology, evaluation, and treatment. Semin Vasc Surg. 2018;31(2–4):43–8.
Dekker RG 2nd, Qin C, Ho BS, et al. The effect of cumulative glycemic burden on the incidence of diabetic foot disease. J Orthop Surg Res. 2016;11(1):143.
Edmonds M, Manu C, Vas P. The current burden of diabetic foot disease. J Clin Orthop Trauma. 2021;17:88–93.
Chen P, Carville K, Swanson T, et al. Australian guideline on wound healing interventions to enhance healing of foot ulcers: part of the 2021 Australian evidence-based guidelines for diabetes-related foot disease. J Foot Ankle Res. 2022;15(1):40.
Dogruel H, Aydemir M, Balci MK. Management of diabetic foot ulcers and the challenging points: an endocrine view. World J Diabetes. 2022;13(1):27–36.
Eleftheriadou I, Samakidou G, Tentolouris A, et al. Nonpharmacological management of diabetic foot ulcers: an update. Int J Low Extrem Wounds. 2021;20(3):188–97.
Dinh T, Tecilazich F, Kafanas A, et al. Mechanisms involved in the development and healing of diabetic foot ulceration. Diabetes. 2012;61(11):2937–47.
Krasilnikova OA, Baranovskii DS, Lyundup AV, et al. Stem and somatic cell monotherapy for the treatment of diabetic foot ulcers: review of clinical studies and mechanisms of action. Stem Cell Rev Rep. 2022. https://doi.org/10.1007/s12015-022-10379-z.
Yu Q, Qiao GH, Wang M, et al. Stem cell-based therapy for diabetic foot ulcers. Front Cell Dev Biol. 2022;10: 812262.
Dai J, Jiang C, Chen H, et al. Treatment of diabetic foot with autologous stem cells: a meta-analysis of randomized studies. Stem Cells Int. 2020;2020:6748530.
Guo J, Dardik A, Fang K, et al. Meta-analysis on the treatment of diabetic foot ulcers with autologous stem cells. Stem Cell Res Ther. 2017;8(1):228.
Jiang X, Zhang H, Teng M. Effectiveness of autologous stem cell therapy for the treatment of lower extremity ulcers: a systematic review and meta-analysis. Medicine (Baltimore). 2016;95(11): e2716.
Shu X, Shu S, Tang S, et al. Efficiency of stem cell based therapy in the treatment of diabetic foot ulcer: a meta-analysis. Endocr J. 2018;65(4):403–13.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58.
Pingping H, Shangzhu L, Mingzhe H, et al. Autologous transplantation of granulocyte colony-stimulating factor-mobilized peripheral blood mononuclear cells improves critical limb ischemia in diabetes. Diabetes Care. 2005;28(9):2155–60.
Nihar Ranjan D, Surjya Narayan D, Padmanav R, et al. Targeting nonhealing ulcers of lower extremity in human through autologous bone marrow-derived mesenchymal stem cells. Rejuvenation Res. 2009;12(5):359–66.
Prakash J, Benjamin P, Mark Ranjan J, et al. The effect of autologous bone marrow-derived cells on healing chronic lower extremity wounds: results of a randomized controlled study. Ostomy Wound Manage. 2011;57(7):38–44.
Yangqing H. Clinical research on the umbilical cord mesenchymal stem cells in the treatment of type 2 diabetic skin ulcer. Chinese J Coal Industry Med. 2014;17(4):532–4.
Dubsky M, Jirkovska A, Bem R, et al. Comparison of the effect of stem cell therapy and percutaneous transluminal angioplasty on diabetic foot disease in patients with critical limb ischemia. Cytotherapy. 2014;16(12):1733–8.
Dubsky M, Jirkovska A, Bem R, et al. Both autologous bone marrow mononuclear cell and peripheral blood progenitor cell therapies similarly improve ischaemia in patients with diabetic foot in comparison with control treatment. Diabetes Metab Res Rev. 2013;29(5):369–76.
Han SK, Kim HR, Kim WK. The treatment of diabetic foot ulcers with uncultured, processed lipoaspirate cells: a pilot study. Wound Repair Regen. 2010;18(4):342–8.
Kirana S, Stratmann B, Prante C, et al. Autologous stem cell therapy in the treatment of limb ischaemia induced chronic tissue ulcers of diabetic foot patients. Int J Clin Pract. 2012;66(4):384–93.
Lonardi R, Leone N, Gennai S, et al. Autologous micro-fragmented adipose tissue for the treatment of diabetic foot minor amputations: a randomized controlled single-center clinical trial (MiFrAADiF). Stem Cell Res Ther. 2019;10(1):223.
Lu D, Chen B, Liang Z, et al. Comparison of bone marrow mesenchymal stem cells with bone marrow-derived mononuclear cells for treatment of diabetic critical limb ischemia and foot ulcer: a double-blind, randomized, controlled trial. Diabetes Res Clin Pract. 2011;92(1):26–36.
Mohammadzadeh L, Samedanifard SH, Keshavarzi A, et al. Therapeutic outcomes of transplanting autologous granulocyte colony-stimulating factor-mobilised peripheral mononuclear cells in diabetic patients with critical limb ischaemia. Exp Clin Endocrinol Diabetes. 2013;121(1):48–53.
Ozturk A, Kucukardali Y, Tangi F, et al. Therapeutical potential of autologous peripheral blood mononuclear cell transplantation in patients with type 2 diabetic critical limb ischemia. J Diabetes Complicat. 2012;26(1):29–33.
Qin HL, Zhu XH, Zhang B, et al. Clinical evaluation of human umbilical cord mesenchymal stem cell transplantation after angioplasty for diabetic foot. Exp Clin Endocrinol Diabetes. 2016;124(8):497–503.
Zhang X, Lian W, Lou W, et al. Transcatheter arterial infusion of autologous CD133(+) cells for diabetic peripheral artery disease. Stem Cells Int. 2016;2016:6925357.
Mavrogenis AF, Megaloikonomos PD, Antoniadou T, et al. Current concepts for the evaluation and management of diabetic foot ulcers. EFORT Open Rev. 2018;3(9):513–25.
Houlind K. Surgical revascularization and reconstruction procedures in diabetic foot ulceration. Diabetes Metab Res Rev. 2020;36(Suppl 1): e3256.
Gentile P, Garcovich S. Systematic review: adipose-derived mesenchymal stem cells, platelet-rich plasma and biomaterials as new regenerative strategies in chronic skin wounds and soft tissue defects. Int J Mol Sci. 2021;22(4):1538.
De Angelis B, D’Autilio MFLM, Orlandi F et al. Wound healing: in vitro and in vivo evaluation of a bio-functionalized scaffold based on hyaluronic acid and platelet-rich plasma in chronic ulcers. J Clinic Med 2019;8(9):1486 https://doi.org/10.3390/jcm8091486.
De Angelis B, Orlandi F, Morais D’Autilio MFL, et al. Vasculogenic chronic ulcer: tissue regeneration with an innovative dermal substitute. J Clin Med. 2019;8(4):525.
Gentile P, Garcovich S. Systematic review-the potential implications of different platelet-rich plasma (PRP) concentrations in regenerative medicine for tissue repair. Int J Mol Sci. 2020;21(16):5702.
Nicoli F, Balzani A, Lazzeri D, et al. Severe hidradenitis suppurativa treatment using platelet-rich plasma gel and Hyalomatrix. Int Wound J. 2015;12(3):338–43.
De Angelis B, Gentile P, Tati E, et al. One-Stage reconstruction of scalp after full-thickness oncologic defects using a dermal regeneration template (Integra). Biomed Res Int. 2015;2015: 698385.
De Angelis B, Orlandi F, Fernandes Lopes Morais D'Autilio M et al. Long-term follow-up comparison of two different bi-layer dermal substitutes in tissue regeneration: clinical outcomes and histological findings. Int Wound J 2018;15(5):695–706. https://doi.org/10.1111/iwj.12912.
Gentile P, Colicchia GM, Nicoli F, et al. Complex abdominal wall repair using a porcine dermal matrix. Surg Innovat. 2011;20(6):12–5.
Valerio C, Lucilla L, Diana S, et al. Use of platelet-rich plasma and hyaluronic acid in the loss of substance with bone exposure. Adv Skin Wound Care. 2011;24(4):176–81.
Xu J, Zgheib C, Hodges MM, et al. Mesenchymal stem cells correct impaired diabetic wound healing by decreasing ECM proteolysis. Physiol Genomics. 2017;49(10):541–8.
Zhang N, Li J, Luo R, et al. Bone marrow mesenchymal stem cells induce angiogenesis and attenuate the remodeling of diabetic cardiomyopathy. Exp Clin Endocrinol Diabetes. 2008;116(2):104–11.
Gentile P, Garcovich S. Concise review: adipose-derived stem cells (ASCs) and adipocyte-secreted exosomal microRNA (A-SE-miR) modulate cancer growth and promote wound repair. J Clin Med. 2019;8(6):855.
Gentile P, Sterodimas A, Pizzicannella J, et al. Systematic review: allogenic use of stromal vascular fraction (SVF) and decellularized extracellular matrices (ECM) as advanced therapy medicinal products (ATMP) in tissue regeneration. Int J Mol Sci. 2020;21(14):4982.
Acknowledgements
This work was supported by grants from the National Natural Science Foundation of China (8197081674).
Funding
Data collection and analysis were supported by the Funding. The publication of the article will also be funded by the Funding (The National Natural Science Foundation of China (8197081674)).
Author information
Authors and Affiliations
Contributions
ZL, YS, JZ, and LZ participated in performing the research and data analysis. ZL and JZ contributed to the research design, writing, and revising of the manuscript. SL, JZ, LZ, and YS participated in research design and data analysis. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors agreed to publish this manuscript.
Competing interests
The authors declare no conflict of interest in this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Fig. S1.
Sensitivity analysis results for New vessels.
Additional file 2: Fig. S2.
Sensitivity analysis results for ABI.
Additional file 3: Fig. S3.
Sensitivity analysis results for TcPO2.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sun, Y., Zhao, J., Zhang, L. et al. Effectiveness and safety of stem cell therapy for diabetic foot: a meta-analysis update. Stem Cell Res Ther 13, 416 (2022). https://doi.org/10.1186/s13287-022-03110-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13287-022-03110-9