
Abstract
Purpose
This study aimed to develop and validate CT-based models to predict pathological complete response (pCR) after neoadjuvant chemotherapy (NAC) for advanced adenocarcinoma of the esophagogastric junction (AEG).
Methods
Pre-NAC clinical and imaging data of AEG patients who underwent surgical resection after preoperative-NAC at two centers were retrospectively collected from November 2014 to September 2020. The dataset included training (n = 60) and external validation groups (n = 32). Three models, including CT-based radiomics, clinical and radiomics–clinical combined models, were established to differentiate pCR (tumor regression grade (TRG) = grade 0) and nonpCR (TRG = grade 1–3) patients. For the radiomics model, tumor-region-based radiomics features in the arterial and venous phases were extracted and selected. The naïve Bayes classifier was used to establish arterial- and venous-phase radiomics models. The selected candidate clinical factors were used to establish a clinical model, which was further incorporated into the radiomics–clinical combined model. ROC analysis, calibration and decision curves were used to assess the model performance.
Results
For the radiomics model, the AUC values obtained using the venous data were higher than those obtained using the arterial data (training: 0.751 vs. 0.736; validation: 0.768 vs. 0.750). Borrmann typing, tumor thickness and degree of differentiation were utilized to establish the clinical model (AUC-training: 0.753; AUC-validation: 0.848). The combination of arterial- and venous-phase radiomics and clinical factors further improved the discriminatory performance of the model (AUC-training: 0.838; AUC-validation: 0.902). The decision curve reflects the higher net benefit of the combined model.
Conclusion
The combination of CT imaging and clinical factors pre-NAC for advanced AEG could help stratify potential responsiveness to NAC.
Similar content being viewed by others
Key points
-
Radiomics method can predict that AEG patients can achieve pCR after NAC.
-
The combination of radiomics and clinical factors can improve the predicting performance.
-
Radiomics–clinical model can stratify patients according to potential responsiveness to NAC.
-
Radiomics–clinical model can help clinicians to develop individualized and precise treatment plans.
Introduction
The incidence of adenocarcinoma of the esophagogastric junction (AEG) has been increasing in recent years [1]. AEG is defined as adenocarcinoma with a tumor center located within 5 cm above or below the anatomical esophagogastric junction (EGJ) that crosses or touches the EGJ. Radical surgical resection and complete lymph node dissection are the basis of treatment, but most patients with AEG are already in the advanced stage when diagnosed, and surgical resection alone has a high rate of local recurrence and poor survival [2]. Neoadjuvant chemotherapy (NAC) followed by radical surgery has become a recommended treatment modality for advanced gastric cancer patients. NAC can reduce tumor load, lower tumor stage, improve the rate of radical resection and ultimately may prolong the survival of AEG patients [3,4,5]. However, the prognostic improvement that is achieved using NAC is largely dependent on the pathological response of the lesion after chemotherapy. The histological tumor regression grade (TRG) is an objective indicator used to evaluate the efficacy of therapy for AEG patients when cancer cells in the lesion are absent or when only a small number remain [6, 7]. In patients with a mild pathological response or poor response, NAC not only does not benefit the patient, but there is also a risk for toxic effects during chemotherapy and tumor progression, and delayed surgery may result in a decreased rate of radical resection and increased surgical complication rates [3, 8,9,10,11]. The current evaluation of the efficacy of NAC is based on the response evaluation criteria in solid tumors (RECIST) [12]. However, the indeterminate wall morphology of the GI tract and the fibrotic changes caused by NAC limit the application of RECIST; additionally, RECIST cannot be used to predict treatment response before treatment, and thus, there is a delay before it can be used [13,14,15,16,17,18]. Therefore, it is crucial to evaluate the efficacy of NAC in a timely and accurate manner before treatment to enable early identification of patients who will respond to NAC, and so that those who will respond poorly can immediately receive surgical treatment. Such an approach could help develop individualized treatment plans for AEG patients, improve patient prognosis and save valuable medical resources.
Along with traditional CT-based response evaluation, the radiomics method has great potential for revealing deep imaging information. The method adopts a combined medical-industrial approach to transform traditional images into deep-level digital quantitative features; the technique can be used to uncover the potential biological characteristics and heterogeneity within the tumor using the imaging data and to provide information beyond the morphological and functional characteristics of the tumor [19,20,21,22]. Several radiomics-based studies regarding the neoadjuvant treatment of esophageal and gastric cancers have been reported [3, 4, 23,24,25]. However, the use of this technique for the pre-NAC prediction of NAC response for AEG alone is rarely reported in most clinical studies of esophageal or gastric cancers, and most studies are single-center studies that lack independent external validation [26].
The purpose of our study was to retrospectively analyze the clinical, pathological and enhanced CT imaging data of patients with advanced AEG before NAC. The models used for predicting pathological complete response (pCR) to NAC were developed and externally validated. We hope the study will provide evidence for understanding tumor response-related quantitative imaging characteristics and contribute to the development of individualized and precise treatment strategies for AEG patients.
Materials and methods
The study protocol was approved by the Medical Ethics Committee of Zhengzhou University, and the need for informed consent was waived.
Patient selection
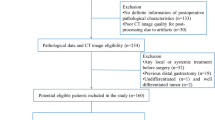
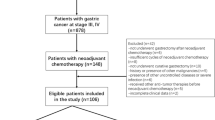
Clinical, pathological and CT imaging data of AEG patients who underwent surgical resection after preoperative NAC at the First Affiliated Hospital of Zhengzhou University and Henan Provincial Cancer Hospital were retrospectively collected from November 2014 to September 2020. The patient enrollment criteria included the following: (1) AEG confirmation by gastroscopic biopsy pathology prior to treatment; (2) pre-NAC clinical stage of cT2–4N0–3M0 stage; (3) NAC treatment in 2–6 cycles; (4) lack of other antitumor therapy administered before NAC; (5) enhanced CT scan obtained within 1 week prior to NAC treatment with complete imaging data; (6) lesion covering at least 3 slices on CT cross section and a maximum plane diameter of at least 2 cm; and (7) radical resection performed after NAC treatment with complete postoperative pathology data. The exclusion criteria included: (1) combined history of other malignancies; (2) poor CT image quality or lack of raw DICOM data; (3) adverse event during NAC or less than 2 cycles of NAC; (4) combined heart, lung and other important organ dysfunction in which a CT examination could not be performed; and (5) incomplete CT imaging data or clinical and pathological data.
Patients with AEG from the First Affiliated Hospital of Zhengzhou University were included in this study as the training group (n = 60), and 32 patients with AEG from Cancer Hospital of Zhengzhou University were included as the external validation group (n = 32).
Clinical data
The chemotherapy regimens included the following: (1) XELOX regimen: oxaliplatin given intravenously at 130 mg/m2 for 2 h on Day 1, repeated every 3 weeks; patients received capecitabine at a dose of 1000 mg/m2 (bid, 1–14 d) orally twice daily; (2) SOX regimen: oxaliplatin 130 mg/m2 intravenously + oral capsules 80 mg/m2 in combination for 14 days twice daily. Patients and families signed informed consent forms. The treatment consisted of between 2 and 6 cycles unless disease progression, intolerable toxicity, or death occurred. All patients underwent radical surgical resection within 1 week of the end of NAC treatment.
The clinical data collected in our study included age, sex, carcinoembryonic antigen levels (CEA, normal range 0–5 ng/mL), carbohydrate antigen 199 level (CA199, normal range 0.01–37 U/ml), carbohydrate antigen 125 levels (CA125, normal range 0.01–35 U/ml), and serum albumin levels (normal range 35–55 g/l). TNM staging of tumors performed using CT images was evaluated according to the 8th edition of the American Joint Committee on Cancer (AJCC) staging [27]. The Borrmann typing of the AEG was documented [28]. The postoperative pathological TRG grading was recorded as a criterion for evaluating the efficacy of NAC. A TRG grade of 0 is defined as complete response, with no viable cancer cells remaining in the primary lesion and lymph nodes; TRG grade 1 is defined as moderate response, with single or small clusters of cancer cells remaining in the lesion; TRG grade 2 is defined as mild response, with significant disappearance of cancer cells under the microscope but some amount of cancer cells remaining, but with less interstitial fibrosis; and TRG grade 3 is defined as poor response, with no significant disappearance of cancer cells under the microscope or only a few cancer cells remaining. Patients were divided into the pCR group (tumor regression grade [TRG] = grade 0) and the nonpCR group (TRG = grade 1–3) based on the postoperative pathological histological TRG evaluation. In the training group, there were 19 patients in the pCR group and 41 patients in the nonpCR group. In the external validation group, there were four patients in the pCR group and 28 patients in the nonpCR group. The clinical characteristics of the enrolled patients are summarized in Table 1.
CT image acquisition
All patients underwent contrast-enhanced CT scans, and informed consent forms were signed before inspection. The CT scans were acquired with a 64-row CT scanner (Discovery CT 750 HD, GE Healthcare, Waukesha, WI, United States) or a 256-row CT scanner (Revolution CT, GE Healthcare, Waukesha, WI, United States). Preparation for the examination occurred as follows: Patients fasted for more than 8 h before the examination and were given an intramuscular injection of scopolamine 10–20 mg 15–20 min before the examination to reduce gastrointestinal motility (Hangzhou Minsheng Pharmaceutical PG Roup Co., Ltd., Specifications: 10 mg/ml) and breath-holding exercises were performed. The patients also drank 800–1000 mL of warm water 10–15 min before the examination. The scanning parameters were as follows: tube voltage 120 kV; tube current using automatic milliampere second technology with a pitch of 1.375/1.1; field of view (FOV) of 500 mm; matrix 512 × 512 mm; and a scan thickness of 0.625–5 mm with scan spacing from 0.625 to 5 mm. The scan area at least encompassed the lower esophagus to the lower border of both kidneys. For the enhancement scan, 90–100 mL of nonionic contrast agent was injected through the elbow vein using a high-pressure syringe (iopromide, 370 mg/mL, GE Medical Systems, 1.5 mL/kg and 3 mL/s). Using the low-dose trigger technique, when the descending aorta reached 100 HU after the injection of contrast medium, arterial phase images were collected 10 s later, and venous phase images were collected at intervals of 30 s.
Image processing and ROI segmentation
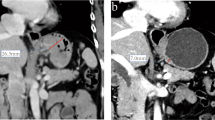
The CT images in arterial and venous phases were isotropically resampled by using trilinear interpolation in Artificial Intelligence Kit software (A. K, version: 3.3.0. R, GE Healthcare, USA) with a voxel size of 1 × 1 × 1 mm to minimize the effect of different scanning protocols or equipment on the radiomics features [29]. Region of interest (ROI) segmentation was performed by delineating around the tumor outline for the largest cross-sectional area in the CT axial plane (Fig. 1). Care was taken to avoid the gastric cavity and stomach contents, fatty tissue around the stomach wall and blood vessels when segmenting. Each ROI was outlined by a radiologist (L.C. 6 years of experience in abdominal imaging diagnosis) and supervised by a radiologist (Z.H., 8 years of experience in abdominal imaging diagnosis). To ensure the reliability and reproducibility of the radiomics features, 30 patients were randomly selected for their data to be segmented. For an analysis of interobserver agreement, a radiologist (L. CC) conducted the first-time whole-dataset segmentation, and another radiologist (H.W., 7 years of experience in abdominal imaging diagnosis) who was supervised by a radiologist (L.L., 9 years of experience in abdominal imaging diagnosis) delineated the images of the 30 selected patients during the same period. For analysis of intraobserver agreement, the radiologist (L. CC) repeatedly conducted segmentation 1 month after the first delineation.

Hypofractionated adenocarcinoma of the esophagogastric junction (AEG) in a 63-year-old man. A CT venous phase axial image before neoadjuvant chemotherapy (NAC), Borrmann staging type I, thickest tumor diameter of 3.4 cm. B Schematic diagram of region of interest (ROI) segmentation on ITK-SNAP software. C CT venous phase axial image after NAC, lesion near disappearance, and insignificant gastric wall thickening. D Postoperative pathological images; fibrous tissue hyperplasia with chronic inflammatory cell infiltration was seen; no tumor cells remained; and tumor regression was obvious (HE × 200). Hypofractionated AEG in a 36 years old man. E CT venous phase axial image before neoadjuvant chemotherapy (NAC), Borrmann staging type III, thickest tumor diameter of 3.2 cm. F Schematic diagram of region of interest (ROI) segmentation on ITK-SNAP software. G CT venous phase axial image after NAC, significantly smaller lesions with reduced enhancement. H Postoperative pathological images showed more chronic inflammatory cell infiltration in the mucosal and lamina propria layers with focal fibrosis (HE × 200)
Radiomics feature extraction
The radiomics features were automatically extracted by using the Python package Pyradiomics [30]. A total of 1409 radiomics features were separately extracted from the delineated ROI in the arterial and venous phases. There were 107 features extracted from the original images, including 32 first-order features (18 intensity statistical and 14 shape features). Among the 75 textural features, there were 24 gray-level cooccurrence matrix (GLCM), 16 gray-level run length matrix (GLRLM), 16 gray-level size zone matrix (GLSZM), 14 gray-level dependence matrix (GLDM) and 5 neighboring gray tone difference matrix (NGTDM) features. In addition, the same number of first-order grayscale statistical features and texture features were extracted based on different transformed images. A total of 744 features were extracted based on wavelet decomposition images with 8 filter channels, 279 features were extracted based on Laplacian of Gaussian (LoG) transform images (sigma parameters selected as 1.0 mm, 3.0 mm and 5.0 mm), and 279 features were extracted based on local binary pattern (LBP)-filtered images (2nd-order spherical harmonic function, spherical neighborhood operator with radius 1.0 and fine fraction 1) [30]. The features were extracted by discretizing the CT values of the ROI region based on a fixed interval width (bin width = 25 HU). Then, the intra/interclass correlation coefficients (ICCs) were calculated based on the features extracted from the 30 randomly selected patients. The features with intra- and interobserver ICC values simultaneously greater than 0.7 were retained for assessment of arterial- and venous-phase features, respectively [31].
Radiomics feature selection and model establishment
The training dataset was used for feature selection and modeling, and the same procedure and set of parameters were applied to the external dataset for model validation.
The same method described above was used to perform feature preprocessing and feature screening in the arterial and venous phases and to build independent arterial and venous radiomics models. The feature selection and modeling were performed as follows.
-
(1)
Outlier processing occurred with values greater than the third quartile + 2 × quartile distance being converted to the 95th percentile; values less than the first quartile − 2 × quartile distance were converted to the 10th percentile.
-
(2)
Features with relatively low variance values less than 1.0 were excluded.
-
(3)
Missing data were filled with the median value, and the Z Score standardization method was applied for data standardization and normalization.
-
(4)
The less redundant features were retained by using correlation analysis with a cutoff value of 0.9.
-
(5)
Features with importance coefficients greater than the maximum importance coefficient/3 assessed using the gradient-boosted decision trees (GBDT) feature importance ranking based on decision tree methods were retained.
-
(6)
Radiomics models were established using the naïve Bayes classifier, and the predicted probability of the model output was used as the Radscore for each individual model.
Based on the above feature screening and modeling methods, our study developed two radiomics models based on pCR outcome: (1) an arterial radiomics model with Radscore_AP_pCR and (2) a venous radiomics model with Radscore_VP_pCR.
Clinical feature selection and model establishment
The clinical features were screened using GBDT (selection of the top three features of importance) and univariate logistic regression (p < 0.1). Model building was performed using the naïve Bayes classifier, and the predicted probability of the model output was used as the model score of the clinical model. Based on the above feature screening and modeling methods, clinical models for predicting pCR (Score_clinic_pCR) were established.
Combined model establishment
Based on the established Radscores and clinical factors, radiomics–clinical combined models were developed using the naïve Bayes classifier. Four combined models were built, including the following: (1) arterial–venous combined model; (2) arterial–clinical combined model; (3) venous–clinical combined model; and (4) arterial–venous–clinical combined model.
Evaluation of model predictive performance
The performance of the model was evaluated by using receiver operating characteristic curve (ROC) analysis to obtain the area under the ROC curve (AUC). The sensitivity, accuracy, negative predictive value and positive predictive value were calculated from the cutoff values of the model score corresponding to the maximum Youden index to evaluate the discriminatory performance of the model. The cutoff value of the training group data was applied to the validation group data to obtain their corresponding discriminatory efficacies in the external validation group. The calibration ability of the model was mainly tested using calibration curve analysis and the Hosmer–Lemeshow test for goodness of fit (p > 0.05 indicates no significant difference between the predicted and actual values). To compare the AUC of different models, Delong’s test was applied (p < 0.05 indicates a significant difference). A decision curve analysis (DCA) was used to assess the net clinical benefit or clinical utility obtained by the model at different threshold probabilities.
Statistical analysis
Statistical analysis was performed using R software (version 3.6.3, http://www.r-project.org). Continuous variable comparisons between two groups were made using independent samples t tests (for data conforming to a normal distribution) or Mann–Whitney U tests (for data not conforming to a normal distribution). Categorical variables were tested by the chi-square test or Fisher's exact test. A two-sided p value of < 0.05 was considered statistically significant. The following R packages were applied: “icc” for intra/interclass correlation coefficient; “glmnet” for logistic regression; “pROC” for ROC analysis; “rmda” for DCA; calibration function in the “rms” package for calibration analysis, “gbm” for GBDT feature importance analysis, “naïveBayes” function for Naïve Bayes classifier, “adabag” package for AdaBoost classifier, “e1071” package for SVM classifier, and “rpart” package for decision tree classifier.
Results
Model establishment for predicting pCR
Arterial model for predicting pCR
By using intra/interclass consistency analysis, 395 radiomics features with ICCs > 0.70 were retained among 1409 features. After removing features with a variance less than 1.0, 150 features were retained. Then, 43 features were retained after correlation analysis by using a cutoff value of 0.9. Six features were retained by GBDT feature importance ranking (Fig. 2A), and the arterial model was established using the naïve Bayes classifier. The AUC values and 95% confidence intervals for the analysis of AEG using single arterial features for predicting pCR in the training and external validation groups are summarized in Additional file1: Table S1, and the ROC curves are shown in Additional file1: Fig. S1A, B. The arterial model radiomics features and the differences in Rad-scoreAP_pCR in the training and external validation groups are summarized in Additional file1: Table S2.

The ranked importance of GBDT selected features for each independent model. A Arterial-phase radiomics features. B The venous-phase radiomics features. C The clinical factors
Venous model for predicting pCR
By using intra/interclass consistency analysis, 410 radiomics features with ICCs > 0.70 were retained among 1409 features. After removing features with variance less than 1.0, 165 features were retained. Then, 52 features were retained after correlation analysis by using a cutoff value of 0.9. Seven features were retained by GBDT feature importance ranking (Fig. 2B), and the venous model was established using the naïve Bayes classifier. The AUC values and 95% confidence intervals for the analysis of AEG using single venous features for predicting pCR in the training and external validation groups are shown in Additional file1: Table S3, and the ROC curves are shown in Additional file1: Fig. S1C, D. The venous model radiomics features and the differences in Rad-scoreVP_pCR in the training and validation groups are shown in Additional file1: Table S4.
Clinical model for predicting pCR
The results of the GBDT feature importance ranking are plotted in Fig. 2C, and the univariate logistic regression results for the clinical factors are summarized in Additional file1: Table S5. The Borrmann classification, tumor thickness, and differentiation degree were finally selected and incorporated into the naïve Bayes classifier to establish the clinical model.
The evaluation of model performance
The AUC values, specificity, sensitivity, accuracy, positive predictive value and negative predictive value of the seven models developed in this study for predicting pCR in the training and external validation groups are shown in Table 2. The ROC curves are shown in Fig. 3A, B. The results of the Delong test used to compare the AUC values of the seven models in the training and validation groups are shown in Additional file1: Table S6. The calibration curves were used to visualize the calibration of all models (Fig. 3C, D), the Hosmer–Lemeshow test was used to assess the goodness of fit (Additional file1: Table S7), and the decision curves were used to confirm the clinical usefulness of the models (Fig. 3E, F).

The performance of different models. A, B ROC curves of different models for predicting pathological complete response (pCR) of adenocarcinoma of the esophagogastric junction (AEG) in the training group (A) and external validation group (B). C, D Calibration curves of different models predicting pCR in the training group (C) and external validation group (D). The 45-degree sloping line indicates the ideal calibration, and the closer the model calibration curve is to the ideal calibration line, the better the agreement between the model predicted probability and the actual probability. E, F Decision curves of different prediction models in the training group (E) and external validation group (F). The X-axis is the threshold probability range, and the Y-axis is the net benefit. The black line labeled "NONE" indicates that no lesions are assumed to be pCR, and the gray line labeled "ALL" indicates that all lesions are assumed to be pCR. The further away from both the black and gray lines, the higher the net benefit of the model compared to performance utilizing the "NONE" and "ALL" assumptions. When comparing the decision curves of different models within the same range of threshold probability, the larger the area under the curve for the same threshold probability interval, the higher the net benefit of the model at that threshold probability
To explore the reliability of the developed model, we also used other modeling methods (logistic regression, support vector machine, decision tree, AdaBoost) for the establishment of a pCR radiomics model and a clinical model based on the same feature sets, and the results are shown in Additional file1: Tables S8–S10. These results indicated that the Naïve Bayes classifier could achieve better model performance in the radiomics and clinical models.
Discussion
In this retrospective study, we analyzed the clinical, pathological and enhanced CT imaging data of patients with advanced AEG before NAC at two medical centers to develop radiomics, clinical, and combined models for predicting pathologically determined TRG grading. The results showed that the combined radiomics–clinical model has the potential to be a reference for evaluating tumor response and developing treatment strategies for patients with AEG.
Preoperative NAC has been shown to reduce the stage of AEG, increase the rate of radical surgical resection, and improve the long-term prognosis of patients [2,3,4,5, 11, 32]. However, 40–70% of patients have a poor response to NAC. Some patients miss the best opportunity for direct operation due to tumor progression during the process of NAC [33, 34]. Therefore, it is clinically relevant to monitor the efficacy of NAC during treatment and to identify patients who respond to NAC in a timely and accurate manner. Radiomics integrates meaningful quantitative imaging features for modeling, which is a major difference from methods utilizing the traditional visual interpretation of images [35,36,37,38,39]. Chen et al. [40] used the features of the CT venous phase and established a predictive model to distinguish between advanced gastric cancer patients with potentially pathologically significant reactions and those with mild reactions and were able to effectively stratify patients according to their response to NAC. Mazzei et al. [41] performed a multicenter study to predict NAC response by delta radiomics in locally progressive gastric cancer. The only significant TA variable was the delta gray-level cooccurrence matrix (GLCM) contrast, with a model AUC value of 0.763. However, there are few reports on the predicted efficacy of NAC for AEG alone. Therefore, we attempted to establish prediction models that help decision-making for the development of individualized and precise treatment strategies for AEG patients.
In this study, 6 and 7 potential radiomics features were selected following screening of the arterial and venous phase images, respectively, and the types of features that appeared in both the arterial and venous phases were LargeDependenceEmphasis (GLDM), InterquartileRange (first-order) and SizeZoneNonUniformity (GLSZM). The GLDM matrix describes the dependence of the voxel intensity. The LargeDependenceEmphasis feature had higher values in the pCR group, while the InterquartileRange and SizeZoneNonUniformity features had lower values in the pCR group. These feature characteristics might indicate that smaller grayscale distribution intervals and a more uniform grayscale distribution of the lesion may suggest the possibility of pCR. It has also been reported that lower GLSZM variants, which represent lower tumor heterogeneity, may be useful in assessing the response to bevacizumab treatment in colorectal cancer [42].
More features were retained in the venous phase images than in the arterial phase images. When the tumor regressed after NAC, the new capillaries and proliferating fibroblasts with rich blood supply were transformed into scar tissue and fibrous connective tissue, and the blood supply in the tissues was reduced. Therefore, venous phase images can reflect the blood supply characteristics of AEG more clearly and comprehensively. In future studies, venous phase images can be selected as the source of radiomics features.
In the pCR-based prediction model, the AUC values obtained using the venous model were higher than those obtained using the arterial model in both the training and external validation groups (0.751 vs. 0.736, 0.768 vs. 0.750), which was consistent with the fact that the venous phase images reflect the AEG blood supply more clearly and comprehensively. Among all clinical characteristics analyzed, the Borrmann type, tumor thickness, and degree of tumor differentiation had predictive value for NAC efficacy. The combination of multiphase radiomics and clinical factors could be used to further improve the discriminatory performance beyond that achieved with independent models. When the Rad-scoreAP_pCR, Rad-scoreVP_pCR and clinical factors were combined simultaneously, an AUC value of 0.838 was achieved in the training cohort and a value of 0.902 was achieved in the external validation cohort. The potential reasons for the good performance of the combined model may be related to the intratumoral heterogeneity reflected by the radiomics features and clinical features that describe the biological behavior of the tumor as well as the cell cycle regulation and chemokine signaling that are occurring, which are important factors affecting the efficacy of NAC [43]. Several studies have reported that tumors with greater heterogeneity tend to be more aggressive in terms of proliferation, metastasis and angiogenesis and may be more resistant to NAC [44, 45]. The complete mechanism underlying the correlation between radiomics features and NAC response has not been elucidated, and studies utilizing radiogenomics are necessary to provide evidence in addressing this issue [46], including studies on the characteristics and the textural features of responsive lesions and the composition of the solid region of the tumor and the surrounding infiltrative environment, which can be described by quantitative radiomics features.
The current study demonstrated the potential use of enhanced CT radiomics features for predicting pCR after NAC in AEG patients. The external validation of the established model also guarantees the reliability of the model performance. It is worth noting that there are some remaining limitations of this study. First, the CT images were obtained from different CT scanners, and there were some differences in the CT scanning protocols of the patients. However, we minimized these differences to the greatest extent by resampling the CT images of the enrolled patients and normalizing the extracted radiomics features. Standardized scanning protocols need to be uniformly applied in future prospective studies. Second, for TRG classification, some patients with progressive disease after NAC could not be operated on and were not included in our study. Because the NAC protocol has not yet been unified, in our study, patients who underwent the XELOX protocol and SOX protocol were selected, which is consistent with the actual clinical treatment situation at present but also introduces a certain selection bias. In addition, our study only included data from two centers, the sample size was still small, the molecular typing of AEG was not performed, and the effect of genes on NAC was not considered. The naïve Bayes classifier selected in the current study is a probabilistic classifier that is suitable for a small dataset. Large sample studies combined with genetic information are needed to further improve and validate the testing efficacy and generalizability of the model. A predictive model with better efficacy that could be translated into clinical practice is needed.
Conclusion
In conclusion, a radiomics method based on enhanced CT imaging before NAC was validated as a potential method for predicting whether advanced AEG patients could achieve pCR after NAC in our study. The combination of radiomics and clinical factors can be used to effectively improve the predictive performance. The prediction model established in our study can be used to stratify patients according to their potential responsiveness to NAC, which can help provide a basis for clinicians to develop individualized and precise treatment plans.
Availability of data and material
The dataset used or analyzed during the current study is available from the corresponding author on reasonable request.
Abbreviations
- AEG:
-
Adenocarcinoma of the esophagogastric junction
- AJCC:
-
American Joint Committee on Cancer
- AUC:
-
Under the ROC curve
- CA125:
-
Carbohydrate antigen 125
- CA199:
-
Carbohydrate antigen 199
- CEA:
-
Carcinoembryonic antigen
- DCA:
-
Decision curve analysis
- EGJ:
-
Esophagogastric junction
- GBDT:
-
The gradient-boosted decision trees
- GLCM:
-
Gray-level co-occurrence matrix
- GLDM:
-
Gray-level dependence matrix
- GLRLM:
-
Gray-level run length matrix
- GLSZM:
-
Gray-level size zone matrix
- NAC:
-
Neoadjuvant chemotherapy
- NGTDM:
-
Neighboring gray tone difference matrix
- pCR:
-
Pathological complete response
- RECIST:
-
Response evaluation criteria in solid tumors
- ROC:
-
Receiver operating characteristic curve
- TRG:
-
Tumor regression grade
References
Manabe N, Matsueda K, Haruma K (2022) epidemiological review of gastroesophageal junction adenocarcinoma in Asian countries. Digestion 103:29–36
Coccolini F, Nardi M, Montori G et al (2018) Neoadjuvant chemotherapy in advanced gastric and esophago-gastric cancer: meta-analysis of randomized trials. Int J Surg 51:120–127
Ychou M, Boige V, Pignon JP et al (2011) Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol 29:1715–1721
Al-Batran SE, Homann N, Pauligk C et al (2019) Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet 393:1948–1957
Kano M, Hayano K, Hayashi H et al (2019) Survival benefit of neoadjuvant chemotherapy with S-1 plus docetaxel for locally advanced gastric cancer: a propensity score-matched analysis. Ann Surg Oncol 26:1805–1813
Kodera Y (2017) Neoadjuvant chemotherapy for gastric adenocarcinoma in Japan. Surg Today 47:899–907
D’Ugo D, Persiani R, Rausei S et al (2006) Response to neoadjuvant chemotherapy and effects of tumor regression in gastric cancer. Eur J Surg Oncol 32:1105–1109
Cunningham D, Allum WH, Stenning SP et al (2006) Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med 355:11–20
Davies AR, Gossage JA, Zylstra J et al (2014) Tumor stage after neoadjuvant chemotherapy determines survival after surgery for adenocarcinoma of the esophagus and esophagogastric junction. J Clin Oncol 32:2983–2990
Xu AM, Huang L, Liu W, Gao S, Han WX, Wei ZJ (2014) Neoadjuvant chemotherapy followed by surgery versus surgery alone for gastric carcinoma: systematic review and meta-analysis of randomized controlled trials. PLoS One 9:e86941
Téoule P, Trojan J, Bechstein W, Woeste G (2015) Impact of neoadjuvant chemotherapy on postoperative morbidity after gastrectomy for gastric cancer. Dig Surg 32:229–237
Eisenhauer EA, Therasse P, Bogaerts J et al (2009) New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 45:228–247
Liu K, Li G, Fan C, Zhou C, Li J (2012) Adapted Choi response criteria for prediction of clinical outcome in locally advanced gastric cancer patients following preoperative chemotherapy. Acta Radiol 53:127–134
Schwartz LH, Litière S, de Vries E et al (2016) RECIST 1.1-Update and clarification: from the RECIST committee. Eur J Cancer 62:132–137
Ott K, Fink U, Becker K et al (2003) Prediction of response to preoperative chemotherapy in gastric carcinoma by metabolic imaging: results of a prospective trial. J Clin Oncol 21:4604–4610
Park S, Ha S, Kwon HW et al (2017) Prospective evaluation of changes in tumor size and tumor metabolism in patients with advanced gastric cancer undergoing chemotherapy: association and clinical implication. J Nucl Med 58:899–904
Tang L, Li ZY, Li ZW et al (2015) Evaluating the response of gastric carcinomas to neoadjuvant chemotherapy using iodine concentration on spectral CT: a comparison with pathological regression. Clin Radiol 70:1198–1204
De Cobelli F, Giganti F, Orsenigo E et al (2013) Apparent diffusion coefficient modifications in assessing gastro-oesophageal cancer response to neoadjuvant treatment: comparison with tumour regression grade at histology. Eur Radiol 23:2165–2174
Bhandari A, Ibrahim M, Sharma C, Liong R, Gustafson S, Prior M (2021) CT-based radiomics for differentiating renal tumours: a systematic review. Abdom Radiol (NY) 46:2052–2063
Reginelli A, Nardone V, Giacobbe G et al (2021) Radiomics as a new frontier of imaging for cancer prognosis: a narrative review. Diagnostics 11:1796
Ibrahim A, Primakov S, Beuque M et al (2021) Radiomics for precision medicine: current challenges, future prospects, and the proposal of a new framework. Methods 188:20–29
Scapicchio C, Gabelloni M, Barucci A, Cioni D, Saba L, Neri E (2021) A deep look into radiomics. Radiol Med 126:1296–1311
Kao YS, Hsu Y (2021) A meta-analysis for using radiomics to predict complete pathological response in esophageal cancer patients receiving neoadjuvant chemoradiation. In Vivo 35:1857–1863
Beukinga RJ, Wang D, Karrenbeld A et al (2021) Addition of HER2 and CD44 to 18F-FDG PET-based clinico-radiomic models enhances prediction of neoadjuvant chemoradiotherapy response in esophageal cancer. Eur Radiol 31:3306–3314
Hu Y, Xie C, Yang H et al (2020) Assessment of intratumoral and peritumoral computed tomography radiomics for predicting pathological complete response to neoadjuvant chemoradiation in patients with esophageal squamous cell carcinoma. JAMA Netw Open 3:e2015927
Sun J, Wang X, Zhang Z et al (2021) The sensitivity prediction of neoadjuvant chemotherapy for gastric cancer. Front Oncol 11:641304
In H, Solsky I, Palis B et al (2017) Validation of the of the AJCC TNM staging system for gastric cancer using the national cancer database. Ann Surg Oncol 24:3683–3691
In H, Solsky I, Palis B, Langdon-Embry M, Ajani J, Sano T (2007) Gastric cancer: preoperative local staging with 3D multi-detector row CT–correlation with surgical and histopathologic results. Radiology 242:472–482
Mackin D, Fave X, Zhang L et al (2017) Harmonizing the pixel size in retrospective computed tomography radiomics studies. PLoS One 12:e0178524
van Griethuysen JJM, Fedorov A, Parmar C et al (2017) Computational radiomics system to decode the radiographic phenotype. Cancer Res 77:e104–e107
Reddavid R, Sofia S, Chiaro P et al (2018) Neoadjuvant chemotherapy for gastric cancer: is it a must or a fake? World J Gastroenterol 24:274–289
Wang L, Zhang Y, Chen Y et al (2021) The performance of a dual-energy CT derived radiomics model in differentiating serosal invasion for advanced gastric cancer patients after neoadjuvant chemotherapy: iodine map combined with 120-kV equivalent mixed images. Front Oncol 10:562945
Xiong BH, Cheng Y, Ma L, Zhang CQ (2014) An updated meta-analysis of randomized controlled trial assessing the effect of neoadjuvant chemotherapy in advanced gastric cancer. Cancer Invest 32:272–284
Samalin E, Ychou M (2007) Neoadjuvant treatment in upper gastrointestinal adenocarcinomas: new paradigms from old concepts? Curr Opin Oncol 19:384–389
Gao X, Ma T, Cui J et al (2021) A CT-based radiomics model for prediction of lymph node metastasis in early stage gastric cancer. Acad Radiol 28:e155–e164
Hamm CA, Beetz NL, Savic LJ, Penzkofer T (2020) Künstliche intelligenz und radiomics in der MRT-basierten Prostatadiagnostik [Artificial intelligence and radiomics in MRI-based prostate diagnostics]. Radiologe 60:48–55
Walsh S, de Jong EEC, Timmeren JE et al (2019) Decision support systems in oncology. JCO Clin Cancer Inform 3:1–9
Qin Y, Deng Y, Jiang H, Hu N, Song B (2021) Artificial intelligence in the imaging of gastric cancer: current applications and future direction. Front Oncol 11:631686
Bi WL, Hosny A, Schabath MB et al (2019) Artificial intelligence in cancer imaging: clinical challenges and applications. CA Cancer J Clin 69:127–157
Chen Y, Wei K, Liu D et al (2021) A machine learning model for predicting a major response to neoadjuvant chemotherapy in advanced gastric cancer. Front Oncol 11:675458
Mazzei MA, Di Giacomo L, Bagnacci G et al (2021) Delta-radiomics and response to neoadjuvant treatment in locally advanced gastric cancer-a multicenter study of GIRCG (Italian Research Group for Gastric Cancer). Quant Imaging Med Surg 11:2376–2387
Bashir U, Weeks A, Goda JS, Siddique M, Goh V, Cook GJ (2019) Measurement of 18F-FDG PET tumor heterogeneity improves early assessment of response to bevacizumab compared with the standard size and uptake metrics in a colorectal cancer model. Nucl Med Commun 40:611–617
Jin Y, Xu Y, Li Y, Chen R, Cai W (2021) Integrative radiogenomics approach for risk assessment of postoperative and adjuvant chemotherapy benefits for gastric cancer patients. Front Oncol 11:755271
Braman NM, Etesami M, Prasanna P et al (2017) Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI. Breast Cancer Res 19:57
Wang WT, Yang L, Yang ZX et al (2018) Assessment of microvascular invasion of hepatocellular carcinoma with diffusion kurtosis imaging. Radiology 286:571–580
Mazurowski MA (2015) Radiogenomics: what it is and why it is important. J Am Coll Radiol 12:862–866
Funding
This work was supported by the grants from National Natural and Science Fund of China (NSFC) (No. 81971615).
Author information
Authors and Affiliations
Contributions
All authors have read and approved the final version of this manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We have abided by ethical standards of journal and the institutional review board of The First Affiliated Hospital of Zhengzhou University approved this retrospective study and waived the requirement for informed consent.
Consent for publication
Not applicable.
Competing interests
The authors of this manuscript declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Radiomics features predict performance of neoadjuvant chemotherapy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, W., Li, L., Liu, S. et al. Enhanced CT-based radiomics predicts pathological complete response after neoadjuvant chemotherapy for advanced adenocarcinoma of the esophagogastric junction: a two-center study. Insights Imaging 13, 134 (2022). https://doi.org/10.1186/s13244-022-01273-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13244-022-01273-w