
Abstract
Background
Southeast Asia represents 10% of the global population, yet little is known about regional clinical characteristics of dementia and risk factors for dementia progression. This study aims to describe the clinico-demographic profiles of dementia in Southeast Asia and investigate the association of onset-type, education, and cerebrovascular disease (CVD) on dementia progression in a real-world clinic setting.
Methods
In this longitudinal study, participants were consecutive series of 1606 patients with dementia from 2010 to 2019 from a tertiary memory clinic from Singapore. The frequency of dementia subtypes stratified into young-onset (YOD; <65 years age-at-onset) and late-onset dementia (LOD; ≥65 years age-at-onset) was studied. Association of onset-type (YOD or LOD), years of lifespan education, and CVD on the trajectory of cognition was evaluated using linear mixed models. The time to significant cognitive decline was investigated using Kaplan-Meier analysis.
Results
Dementia of the Alzheimer’s type (DAT) was the most common diagnosis (59.8%), followed by vascular dementia (14.9%) and frontotemporal dementia (11.1%). YOD patients accounted for 28.5% of all dementia patients. Patients with higher lifespan education had a steeper decline in global cognition (p<0.001), with this finding being more pronounced in YOD (p=0.0006). Older patients with a moderate-to-severe burden of CVD demonstrated a trend for a faster decline in global cognition compared to those with a mild burden.
Conclusions
There is a high frequency of YOD with DAT being most common in our Southeast Asian memory clinic cohort. YOD patients with higher lifespan education and LOD patients with moderate-to-severe CVD experience a steep decline in cognition.
Similar content being viewed by others


Background
The prevalence of dementia types and their clinical trajectory has been extensively reported from western settings [1,2,3,4,5,6,7,8,9]. The estimates from Asia are quite variable, likely related to differing diagnostic criteria and variations in diagnostic tools. There is also limited literature on dementia progression in Asia, especially involving naturalistic patient follow-up over long durations. Longitudinal studies in Asia have largely focussed on older populations [10] and cognitive changes in non-dementia participants [11]. Cognitive trajectories in young-onset dementia (YOD) have not been compared with late-onset dementia (LOD) counterparts in Asia [12,13,14]. Additionally, the prevalence of dementia sub-types remains to be elucidated in Southeast Asia.
From an etiological perspective, reports illustrate cerebrovascular contribution to dementia in Asia [15, 16], involving white matter hyperintensities (WMH) as surrogate MRI markers for cerebrovascular disease (CVD) [17]. While vascular cognitive impairment (VCI) is more prevalent in Asia [18, 19], there is limited data from naturalistic studies comparing cognitive trajectories in such patients. Additionally, the contribution of education attainment to cognitive decline between YOD and LOD remains to be further elucidated.
This study describes the demographic and clinical trends and longitudinal profile of YOD and LOD patients from a dementia clinic of a tertiary hospital, in Singapore between 2010 and 2019. The tertiary hospital is the largest provider of neuroscience care in Singapore, providing care to 70% of the population. Additionally, the study examined the association between education and longitudinal cognitive change in YOD and LOD. The impact of CVD determined by the modified Fazekas scale on clinically relevant time to a significant decline in global cognition was examined, as this may allow clinicians to institute intensive management of vascular risk factors for those with CVD. We also assessed the influence of education and CVD on depression. We hypothesized that higher levels of lifespan education would be protective against cognitive decline and higher CVD load would result in a more rapid cognitive decline.
Methods
Participants and study design
Data was extracted from a longitudinal database of consecutive series of patients with cognitive impairment. The database included patients attending the dementia clinic of a tertiary hospital in Singapore between 2010 and 2019. All patients were evaluated by a team comprising cognitive neurologists, psychologists, and dementia-trained nurses. Patients underwent neuroimaging with MRI or a CT scan as part of the diagnostic workup where clinically indicated. Diagnoses included subjective cognitive impairment, mild cognitive impairment, and dementia. For the purposes of this study, only patients with dementia were included in the analysis. Dementia was diagnosed based on the DSM IV and 5 criteria [20, 21]. Patients with dementia included dementia of the Alzheimer’s type (DAT), frontotemporal dementia (FTD), vascular dementia (VaD), Parkinsonism spectrum dementia, rapidly progressing dementia (RPD), and autoimmune dementia. Clinical symptoms and presentation largely informed the diagnoses in the case of mixed dementias, wherein the consulting team arrived at a final diagnosis based on the presentation and clinical history of individual patients. Parkinsonism spectrum dementia consisted of Parkinson’s dementia (PDD), dementia with Lewy body (DLB), and normal pressure hydrocephalus (NPH); diagnosis of DAT was per the NINCDS-ADRDA [22] and NIA-AA criteria [23]. VaD was diagnosed based on the NINDS-AIREN criteria [24], FTD was diagnosed based on the Raskovsky criteria [25], PDD was diagnosed based on the MDS task force criteria [26, 27], while DLB was diagnosed based on the McKeith criteria [28, 29]. Patients who were under the age of 65 years at the time of symptom onset were classified as YOD [30], while patients aged 65 years or older were classified as LOD. A total of 2890 unique patients attended the tertiary memory clinic from 2010 to 2019. Of them, 1606 were given a consensus diagnosis of dementia based on clinical criteria (as referenced above) on their initial visit, a subset of whom came back for follow-up visits every 6 to 9 months. At every follow-up visit, patient diagnosis and demographics were determined and they underwent cognitive testing as detailed in section 2.2. Dementia patients were included in the study if they had at least one follow-up visit following the initial visit and based on these criteria a total of 786 dementia patients completed one or more follow-up visits. As part of the routine clinical screening, patients were evaluated for thyroid function and vitamin B12 levels at every visit. While we have not collected individual data on these measures, appropriate management was employed for patients with any abnormal findings.
The study was approved by the Singhealth Centralized Review Board. The informed consent process was in accordance with Declaration of Helsinki and local clinical research regulations.
Cognitive and behavioral measurements
Patients underwent evaluation for global cognition with the local versions of the Mini Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA), which have been validated in Singapore [31, 32]. The local version of the MMSE and MOCA has a score range of 0–30 points and score categories similar to the original versions. Patients were also screened for depression with the geriatric depression scale (GDS). Clinically relevant depression was determined using a cut-off of GDS≥5. The MMSE and MoCA evaluation was conducted at the patient’s initial visit to the clinic and was classified as the baseline MMSE and baseline MoCA score. These evaluations were then repeated at every clinical visit which ranged from 6 to 9 months and were used as follow-up measurements in the statistical analyses. The MMSE was the most regularly recorded measure due to the ease of administration with limited patient-facing time in a naturalistic clinical setting. It was also an effective tool for consistent tracking of cognitive performance as disease progression did not hinder the administration of the test until more advanced stages. All evaluations were performed by psychologists and trained dementia nurses using a standardized protocol.
Measurement of cerebrovascular disease burden
Patients underwent neuroimaging using either 1.5T MRI scanner (Philips Ingenia) or 3T Siemens Prisma Fit (Siemens, Erlangen, Germany) or coronal fine cut CT scans. T1-weighted and fluid-attenuated inversion recovery were used for visual rating of scans based on the modified Fazekas scale for WMH severity [33]. Specifically, periventricular WMH and deep subcortical WMH were separately rated on a 0–3 point scale for both hemispheres. The scoring criteria were as follows: for periventricular WMH, the absence of any WMH = 0; the presence of caps or pencil-thin lining = 1; a smooth halo along the edges of the lateral ventricle = 2; and irregular hyperintensities extending into deep white matter = 3. For deep subcortical WMH, the absence of any WMH = 0; the presence of non-confluent foci of WMH in the deep subcortical region = 1; beginning confluence of WMH foci = 2; and the presence of large confluent areas = 3. The modified Fazekas scale allows for quantification of white matter lesions in four brain regions, namely right periventricular, left periventricular, right deep subcortical, and left deep subcortical to provide a score range of 0–12. All visual ratings were performed by two independent raters, and any significant discordance in scores was resolved by consensus. Absent-to-mild CVD was defined as a score of 0–4 on the total Fazekas scale while those with a score of 5–12 were defined as moderate-to-severe CVD. A score of 5–12 on the modified Fazekas score corresponds to Fazekas grades 2–3 of the original grading, indicative of significant CVD.
Statistical analyses
Analyses of baseline demographic information for the dementia group included descriptive statistics, and continuous variables were reported as mean and standard deviation and categorical variables as frequency and percentage across YOD and LOD cohorts. Group differences were examined using two independent samples t test or Mann-Whitney U test (where appropriate) and χ2 or Fisher’s exact test (where appropriate) for continuous and categorical outcomes, respectively.
In order to investigate the cognitive trajectories of YOD and LOD over time (duration of follow-up), linear mixed model analysis was conducted to examine two-way interactions between onset-type and time, for patients with at least one follow-up MMSE score. Longitudinal MMSE scores were the key dependent variable. The key independent variable was onset-type, coded as either YOD (<65 years) or LOD (≥65 years) and an onset-type*Time interaction term. Baseline age, race, sex, and lifespan education years (referring to education from primary school and throughout the lifespan) and duration of follow-up were included as covariates. Additionally, a separate model also assessed the effect of lifespan education years on MMSE decline over time with a lifespan education years*time interaction term as the key independent variable. Baseline age, race, sex, baseline MMSE score, and duration of follow-up were included as covariates. The random effects were modeled at the individual subject level represented by the individual variability in intercepts and longitudinal slopes.
Additionally, the relationship between onset-type, lifespan education, and cognition was elucidated in a linear mixed model three-way interaction analysis. The key dependent and independent variables remained longitudinal MMSE scores and onset-type respectively with an onset-type*lifespan education years*time interaction term. Baseline age, sex, race, lifespan education years, baseline MMSE score, and duration of follow-up were included as covariates. The random effects were modeled at the individual subject level represented by the individual variability in intercepts and longitudinal slopes.
The linear mixed model analyses were performed using R 3.6.3 (R Core Team, 2014) with RStudio (RStudio Team, 2012).
A subset of our patients also had longitudinal GDS scores. Thus, we also investigated what factors contributed to the onset of clinically relevant depression or the continued presence of depression using a cut-off of GDS≥5. Based on this cut-off, we classified patients on a binary scale (0=not depressed; 1=depressed). In binary logistic regression models, we assessed whether lifespan education years, sex, and white matter hyperintensity (Fazekas visual rating scores) influenced the development of depression in YOD and LOD separately.
In order to examine a clinically relevant effect of CVD burden on the rapid progression of cognitive decline, a sub-group analysis looking at the long-term effect of CVD burden on those diagnosed with DAT and VaD was conducted. We investigated the effect of CVD burden on the significant decline in MMSE and MoCA using a Kaplan-Meier plot and log-rank test. For MMSE and MoCA scores, a three-point drop was used to define significant decline within the maximum duration of follow-up for each patient. As defined earlier, patients with absent-to-mild cerebrovascular disease (CVD) had a score of 0–4 on the total Fazekas scale while those with a score of 5–12 were defined as moderate-to-severe CVD. The sub-group statistical analysis was conducted using SAS software version 9.4 for Windows (Cary, NC: SAS Institute Inc.) and R 3.6.3 (R Core Team, 2014) with RStudio (RStudio Team, 2012).
Results
Demographics of dementia
A total of 2890 unique patients attended the tertiary memory clinic from 2010 to 2019. Of them, 1606 were diagnosed with dementia. The mean age of the dementia cohort was 71.2 (± 10.5) years, 53.9% females, and 85.4% Chinese ethnicity with a mean lifespan education of 7.4 (± 5.2) years. DAT was the most common diagnosis (59.8%), followed by VaD (14.9%), FTD (11.1%), Parkinsonism spectrum (11.1%), autoimmune dementia (1.6%), and RPD (1.4%). YOD patients accounted for 28.5% of all dementia patients. Over the 10-year period, there was an increasing trend in the yearly incidence of YOD and LOD patients (Additional File 1: Supplementary Fig. 1).
Clinical profiles of young-onset and late-onset dementia
Patients in the LOD group had significantly lower years of lifespan education (6.5 vs. 9.6, p<0.001), and lower baseline MMSE (17.7 vs. 18.9, p=0.003) and MoCA (16.8 vs. 18.1, p=0.002) compared to YOD patients (Table 1). LOD participants also had a higher frequency of diabetes mellitus (22.2 vs. 15.7, p=0.002), hypertension (46.8 vs. 29.7 p<0.001), hyperlipidemia (42.1 vs. 31.2, p<0.001), and coronary artery disease (8.8 vs. 3.9, p=0.001) but lower frequency of smoking (12.6 vs 15.5, p=0.010) and alcohol use (7.9 vs. 12.0, p=0.007) (Table 1). The LOD group had a significantly higher proportion of DAT patients (66.4% vs. 43.5%, p<0.001) and Parkinsonism spectrum patients (12.3% vs. 8.3%, p=0.028) compared to the YOD group (Table 1). However, there was a significantly higher proportion of VaD patients (18.1% vs. 13.7%, p=0.029), FTD patients (24.5% vs. 5.8%, p<0.001), RPD patients (2.8% vs. 0.8%, p=0.003), and autoimmune dementia patients (2.8% vs. 1.1%, p=0.026) in the YOD than the LOD group (Table 1; Fig. 1).

Diagnostic breakdown in young-onset dementia and late-onset dementia. Dementia of the Alzheimer’s type was the most common diagnosis in both the young-onset and late-onset groups. The late-onset dementia group had a significantly higher proportion of dementia of the Alzheimer’s type patients. Abbreviations: YOD young-onset dementia, LOD late-onset dementia
Effect of onset-type and education on cognitive trajectories of patients with amnestic-type dementia
Change in global cognition indexed using MMSE was studied in 786 patients with DAT and VaD having follow-up MMSE scores. There were 194 patients (24.7%) in the YOD group with a mean age of 58.4 (± 5.0) years, mean lifespan education of 9.3 (± 4.0) years, 47.9% of females, 80.9% of Chinese ethnicity, baseline MMSE of 19.8 (± 5.8), and baseline MoCA of 17.8 (± 5.7). There were 592 (75.3%) LOD patients with a mean age of 76.5 (± 5.9), an average of 6.2 (± 5.0) years of lifespan education, 62.7% female and 90.4% Chinese ethnicity, and baseline MMSE of 18.6 (± 5.5) and baseline MoCA of 16.7 (± 4.9). The average duration of follow-up for the YOD group was 2.3 (± 1.8) years and 2.8 (± 2.0) years for the LOD group.
YOD patients, while demonstrating a higher MMSE score at baseline compared to the LOD group (19.8 vs. 18.6, p=0.014), showed a steeper decline in MMSE scores over a mean follow-up time of 2.7 years (onset-type*Time: β=−0.33, p=0.030; Additional File 1: Supplementary Fig. 2; Table 2) compared to LOD patients after controlling for age, sex, race, and lifespan education years.
Years of lifespan education were found to be a predictor of baseline MMSE (p<0.001) such that higher years of education resulted in higher baseline MMSE scores. Despite the higher baseline MMSE scores, higher years of education related in a steeper decline in MMSE scores over time (years of education*Time: β=−0.05, p<0.001; Table 2) after controlling for age, race, and sex. These results remained even after controlling for baseline MMSE score.
When onset-type was added in the model evaluating lifespan education and MMSE trajectory, the effect of years of education was found to be more pronounced. Patients with higher years of education in the YOD group experienced a steeper decline than patients with comparable years of education in the LOD group (onset-type*Lifespan education years*Time: β=−0.13, p=0.0006; Fig. 2, Table 2). At baseline, there was no statistical difference in the MMSE score between those in the YOD and LOD groups with comparable years of education (p=0.812). Importantly, these results remained even after controlling for baseline MMSE score.

Mini Mental State Examination scores over time for young and late-onset dementia with low, medium, and high education. Patients with higher years of education in the young-onset dementia group experienced a steeper decline than patients with comparable years of education in the late-onset dementia group. Abbreviations: YOD young-onset dementia, LOD late-onset dementia, MMSE Mini Mental State Examination
Longitudinal depression in young-onset and late-onset dementia
From the total cohort, a subset of 430 patients had longitudinal GDS scores comprising YOD (n=104) and LOD (n=326) patients. In our memory clinic, we found that 23.07% (n=24) of our YOD and 23.33% (n=76) of our LOD patients were classified as having depression at follow-up. In separate binary logistic regression models for YOD and LOD, lifespan education years, sex, and white matter hyperintensity (Fazekas visual rating scores) were not significant predictors of depression development (Table 2).
Influence of cerebrovascular disease burden on a global cognitive trajectory in DAT and VaD
The influence of CVD on global cognitive MMSE trajectory was studied among 592 DAT and VaD YOD and LOD patients who had baseline MRI or CT brain. These patients had a baseline MRI scan for quantification of CVD and longitudinal MMSE scores. CVD burden was coded as a categorical variable, absent-to-mild CVD burden and moderate-to-severe CVD burden as described in the “Methods” section. A three-point drop in MMSE was used to define a significant decline in global cognition [34].
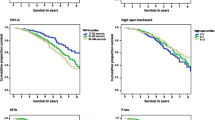
Among the 592 patients, 417 (70.4%) had a moderate-to-severe burden of CVD while 175 (29.6%) had an absent-to-mild burden of CVD. Kaplan-Meier analysis demonstrated that patients in the LOD group with the moderate-to-severe burden of CVD demonstrated a statistical trend for faster decline compared to those with absent-to-mild CVD. Among LOD patients with moderate-to-severe CVD, 75% of them demonstrated a 3-point MMSE decline at 2.5 years, while it took 3.6 years for 75% of LOD patients with absent-to-mild CVD to have a similar MMSE decline (p=0.063; Fig. 3). There was no significant difference in time to cognitive decline among YOD patients based on CVD severity (p=0.715).

Time to a significant decline in Mini Mental State Examination scores for those with moderate-to-severe cerebrovascular burden and absent-to-mild cerebrovascular burden. Seventy-five percent of late-onset patients with moderate-to-severe cerebrovascular burden, demonstrated a 3-point MMSE decline at 2.5 years, while it took 3.6 years for 75% of patients with an absent-to-mild cerebrovascular burden to have a similar MMSE decline. Abbreviations: YOD young-onset dementia, LOD late-onset dementia, MMSE Mini Mental State Examination
Additionally, a subset of patients also had longitudinal MoCA scores and the influence of CVD on MoCA trajectory was studied among 368 YOD and LOD patients who had baseline MRI or CT brain. There was no significant difference in the average time to 3-point MoCA decline between the absent-to-mild CVD group (2.09 years) and the moderate-to-severe CVD group (2.03 years, p=0.69). Additionally, there was also no significant difference in a significant decline in MoCA scores based on CVD severity in both the YOD and LOD groups.
Discussion
In a Southeast Asian memory clinic cohort with data spanning a decade, we found a trend towards increasing yearly incidence of both YOD and LOD. We additionally demonstrate that YOD accounted for 28.5% of all dementia patients. DAT was the leading type of dementia as in western cohorts, with VaD being the second leading cause of dementia. Our data also showed that while patients with higher education have higher baseline global cognition, they however have a steeper decline in global cognition, with this finding being more pronounced in YOD patients. LOD patients with moderate-to-severe CVD burden also displayed a faster decline in global cognition compared to those with absent-to-mild CVD.
Over the period from 2010 to 2019, overall, there has been an increasing trend in patients with YOD. The reasons for this increase are likely to be multifactorial. Specifically, awareness of YOD both among the general public and within the healthcare system has steadily increased owing to dementia awareness campaigns by many organizations including the Health Promotion Board and the National Neuroscience Institute. The increase in YOD may also be related to the increasing burden of vascular risk factors. Our findings demonstrate that there is a high frequency of vascular risk factors among younger patients. The frequency of hypertension among YOD was 29.7%, while the frequency of hyperlipidemia, diabetes mellitus, and smoking in YOD was 31.2%, 15.7%, and 15.5%, respectively. These vascular risk factors may have contributed to cerebrovascular disease via vascular injury to the brain as well as accelerated amyloid pathology [35,36,37]. Recent studies in Asian and Western cohorts have also indicated a significant role of vascular disease burden in YOD [38,39,40]. In support of our findings, prior studies have shown a high prevalence of vascular risk factors and cerebrovascular disease burden in Singapore and other cities in Asia [19, 41]. In turn, high vascular disease burden has been shown to increase the odds of conversion from a prodromal to clinical dementia stage in patients from Singapore [42].
Our findings additionally demonstrate that LOD patients with a moderate-to-severe burden of CVD experience a faster decline in global cognition compared to those with an absent-to-mild CVD burden. Among LOD patients with moderate-to-severe CVD, 75% demonstrated a 3-point decline in MMSE within 2.5 years from diagnosis of dementia, compared to patients with absent-to-mild CVD, wherein a 3-point MMSE decline was observed after 3.6 years These findings suggest that CVD may have a major role in the pathogenesis of dementia in LOD. In this regard, findings from Asia indicate a high co-occurrence of CVD in LOD [43]. Such a co-occurrence and additional presence of vascular risk factors in Asian cohorts have also been associated with greater memory and executive function decline and worse clinical outcomes [44,45,46,47,48]. Additionally, greater dysconnectivity in the default mode network as well as executive control network with consequent impairment in episodic memory as well as executive function has been associated with CVD burden in studies from Asia [46, 49, 50]. Findings from our group demonstrate that the presence of CVD may also result in atrophy of specific gray matter regions crucial for episodic memory and executive function [51, 52]. Moreover, in the Honolulu-Asia Ageing Study, dementia frequency increased with increasing neuritic plaque density and increased further in the presence of cerebrovascular lesions. The association was strongest in patients with sparse neuritic plaques where dementia frequency more than doubled with coexistent cerebrovascular lesions [53]. These findings suggest that CVD may result in accelerated accumulation of amyloid pathology. As for the stronger CVD effect in LOD compared to YOD, it is likely that CVD interacts with the multiple pathologies in the older brain to result in more accelerated neurodegeneration, hence the faster decline in cognition in LOD patients harboring CVD. From a clinical management perspective, our finding of more rapid cognitive decline in patients with concomitant CVD may help clinicians in selecting intensive management of vascular risk factors to slow the rate of decline in their patients with a high CVD burden.
The finding that longitudinal cognitive decline in YOD patients was steeper, especially among those with a higher number of years of lifespan education has important clinical and public health implications. Similar to our findings, previous studies have also reported a steeper decline in cognition among those with higher education [54, 55]. Higher levels of education have been reported to increase cognitive reserve and thus hypothesized to delay the onset of dementia. However, it is likely that once dementia sets in, patients with higher education may have exhausted their cognitive reserve and thus experience a steeper decline in cognition compared to those with lower education. Additionally, YOD is also associated with pure pathologies affecting specific brain regions with a more aggressive disease course, resulting in greater neuronal loss and cerebral hypometabolism than LOD. Thus, the protective role of education is unable to sustain optimal cognitive function in YOD and hence they experience a greater cognitive decline [56,57,58]. This is an indication that more resources may need to be devoted to the care, treatment, and research for young-onset dementia. Findings from our group indicate that the opportunity cost to the young-onset group in terms of economic, social, and emotional well-being may be more drastic coupled with ripple effects that impact family members of those with young-onset dementia [59, 60]. Notably, little is known about the relationship between onset-type, lifespan education, and cognitive decline in Asian populations and needs further exploration. Findings from our study thus provide important insights into the influence of lifespan education on the future cognitive decline between YOD and LOD in an Asian clinic cohort.
Limitations
The limitations of our paper include that the data came from a single memory clinic and thus may lack generalizability. However, this being the first report from a memory clinic population, we believe our findings will allow other centers in Southeast Asia to examine their cohorts and perform comparisons with our cohort. The lack of biomarker data may be viewed as a weakness, although the availability of clinical data may allow better allocation of resources for the development of biomarkers in this growing region of the world. Additionally, we were unable to include information on the longitudinal progression of CVD as well as diagnostic status and its influence on cognitive decline in the current study. This will be a key focus of our future studies. The availability of data over a 10-year period as well as the use of neuroimaging to define cerebrovascular disease is key strengths of our study.
Conclusion
In conclusion, we demonstrate that there is a high frequency of YOD in our cohort with DAT and VaD being the most common in our clinic cohort. Younger patients with greater years of lifespan education and LOD patients with moderate-to-severe CVD experienced a steep decline in cognition.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- YOD:
-
Young-onset dementia
- LOD:
-
Late-onset dementia
- WMH:
-
White matter hyperintensities
- CVD:
-
Cerebrovascular disease
- VCI:
-
Vascular cognitive impairment
- DAT:
-
Dementia of the Alzheimer’s type
- FTD:
-
Frontotemporal dementia
- VaD:
-
Vascular dementia
- RPD:
-
Rapidly progressing dementia
- PDD:
-
Parkinson’s dementia
- DLB:
-
Dementia with Lewy body
- NPH:
-
Normal pressure hydrocephalus
- MMSE:
-
Mini Mental State Examination
- MoCA:
-
Montreal Cognitive Assessment
- GDS:
-
Geriatric Depression Scale
References
Anstey KJ, Burns RA, Birrell CL, Steel D, Kiely KM, Luszcz MA. Estimates of probable dementia prevalence from population-based surveys compared with dementia prevalence estimates based on meta-analyses. BMC Neurol. 2010;21(10):62.
Bäckman L, Small BJ. Cognitive deficits in preclinical Alzheimer’s disease and vascular dementia: patterns of findings from the Kungsholmen Project. Physiol Behav. 2007;92(1–2):80–6.
Baker E, Ehtesham I, Caroline J, Matthew B, Hitesh S, Robert S, et al. Trajectories of dementia-related cognitive decline in a large mental health records derived patient cohort. PLoS One. 2017;12(6):e0178562.
Brodaty H, Connors MH, Xu J, Woodward M, Ames D, Group PS. The course of neuropsychiatric symptoms in dementia: a 3-year longitudinal study. J Am Med Dir Assoc. 2015;16(5):380–7.
Doblhammer G, Fink A, Fritze T, Günster C. The demography and epidemiology of dementia. Geriatr Ment Heal Care. 2013;1(2):29–33.
Haaksma ML, Rizzuto D, Leoutsakos J-MS, Marengoni A, Tan EC, Olde Rikkert MG, et al. Predicting cognitive and functional trajectories in people with late-onset dementia: 2 population-based studies. J Am Med Dir Assoc. 2019;20(11):1444–50.
Mahon S, Parmar P, Barker-Collo S, Krishnamurthi R, Jones K, Theadom A, et al. Determinants, prevalence, and trajectory of long-term post-stroke cognitive impairment: results from a 4-year follow-up of the ARCOS-IV study. Neuroepidemiology. 2017;49(3–4):129–34.
Perera G, Pedersen L, Ansel D, Alexander M, Arrighi HM, Avillach P, et al. Dementia prevalence and incidence in a federation of European Electronic Health Record databases: the European Medical Informatics Framework resource. Alzheimers Dement. 2018;14(2):130–9.
Roberts RO, Aakre JA, Kremers WK, Vassilaki M, Knopman DS, Mielke MM, et al. Prevalence and outcomes of amyloid positivity among persons without dementia in a longitudinal, population-based setting. JAMA Neurol. 2018;75(8):970–9.
Han JW, Kim TH, Kwak KP, Kim K, Kim BJ, Kim SG, et al. Overview of the Korean longitudinal study on cognitive aging and dementia. Psychiatry Investig. 2018;15(8):767.
Leong RL, Lo JC, Sim SK, Zheng H, Tandi J, Zhou J, et al. Longitudinal brain structure and cognitive changes over 8 years in an East Asian cohort. Neuroimage. 2017;147:852–60.
Kandiah N, Wang V, Lin X, Nyu MM, Lim L, Ng A, et al. Cost related to dementia in the young and the impact of etiological subtype on cost. J Alzheimers Dis. 2016;49(2):277–85.
Han L-H, Xue Y-Y, Zheng Y-C, Li X-Y, Lin R-R, Wu Z-Y, et al. Genetic analysis of chinese patients with early-onset dementia using next-generation sequencing. Clin Interv Aging. 2020;15:1831–9.
Park JE, Kim HJ, Kim Y-E, Jang H, Cho SH, Kim SJ, et al. Analysis of dementia-related gene variants in APOE ε4 noncarrying Korean patients with early-onset Alzheimer’s disease. Neurobiol Aging. 2020;85:155.e5–8.
Sachdev P, Lo J, Crawford J, Mellon L, Hickey A, Williams D, et al. STROKOG (stroke and cognition consortium): an international consortium to examine the epidemiology, diagnosis, and treatment of neurocognitive disorders in relation to cerebrovascular disease. Alzheimer’s Dement (Amsterdam, Netherlands). 2016;7:11–23.
Snyder H, Corriveau R, Craft S, Faber J, Greenberg S, Knopman D, et al. Vascular contributions to cognitive impairment and dementia including Alzheimer’s disease. Alzheimers Dement. 2015;11(6):710–7.
Debette S, Markus H. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2010;341(7767):288.
Fratiglioni L, De Ronchi D, Agüero-Torres H. Worldwide prevalence and incidence of dementia. Drugs Aging. 1999;15(5):365–75.
Hilal S, Mok V, Youn YC, Wong A, Ikram MK, Chen CLH. Prevalence, risk factors and consequences of cerebral small vessel diseases: data from three Asian countries. J Neurol Neurosurg Psychiatry. 2017;88(8):669–74.
Association AP. Diagnostic and statistical manual of mental disorders. In: Vol. 4th Editio. ed. Arlington: American Psychiatry Publishing; 2000.
Association AP. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington: American Psychiatric Publishing; 2013.
McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan E. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939–44 Available from: https://pubmed.ncbi.nlm.nih.gov/6610841/.
Albert M, DeKosky S, Dickson D, Dubois B, Feldman H, Fox N, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270–9.
Erkinjuntti T. Clinical criteria for vascular dementia: the NINDS-AIREN criteria. Dementia. 1994;5(3–4):189–92.
Rascovsky K, Hodges J, Knopman D, Mendez M, Kramer J, Neuhaus J, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain. 2011;134(Pt 9):2456–77.
Hoogland J, Boel JA, de Bie RM, Schmand BA, Geskus RB, Dalrymple-Alford JC, et al. Risk of Parkinson’s disease dementia related to level I MDS PD-MCI. Mov Disord. 2019;34(3):430–5.
Postuma R, Berg D, Stern M, Poewe W, Olanow C, Oertel W, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591–601.
McKeith IG, Boeve BF, Dickson DW, Halliday G, Taylor J-P, Weintraub D, et al. Diagnosis and management of dementia with Lewy bodies. Neurology. 2017;89(1):88–100.
McKeith I, Dickson D, Lowe J, Emre M, O’Brien J, Feldman H, et al. Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium. Neurology. 2005;65(12):1863–72.
Kuruppu DK, Matthews BR. Young-onset dementia. Semin Neurol. 2013;33(4):365–85.
Feng L, Chong MS, Lim WS, Ng TP. The modified mini-mental state examination test: normative data for Singapore Chinese older adults and its performance in detecting early cognitive impairment. Singapore Med J. 2012;53(7):458–62.
Ng A, Chew I, Narasimhalu K, Kandiah N. Effectiveness of Montreal cognitive assessment for the diagnosis of mild cognitive impairment and mild Alzheimer’s disease in Singapore. Singapore Med J. 2013;54(11):616–9.
Fazekas F, Chawluk JB, Alavi A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. Am J Neuroradiol. 1987;149(2):351–6.
Bernard BA, Goldman JG. MMSE - Mini-Mental State Examination. Encycl Mov Disord. 2010;1:187–9.
Yatawara C, Ng KP, Cristine Guevarra A, Wong B, Yong TT, Kandiah N. Small vessel disease and associations with cerebrospinal fluid amyloid, tau, and neurodegeneration (ATN) biomarkers and cognition in young onset dementia. J Alzheimers Dis. 2020;77(3):1305–14.
Zlokovic B V. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat Rev Neurosci 2011;12(12):723–38.
Mawuenyega KG, Sigurdson W, Ovod V, Munsell L, Kasten T, Morris JC, et al. Decreased clearance of CNS beta-amyloid in Alzheimer’s disease. Science. 2010;330(6012):1774.
Ikejima C, Yasuno F, Mizukami K, Sasaki M, Tanimukai S, Asada T. Prevalence and causes of early-onset dementia in Japan: a population-based study. Stroke. 2009;40(8):2709–14.
Carcaillon-Bentata L, Quintin C, Boussac-Zarebska M, Elbaz A. Prevalence and incidence of young onset dementia and associations with comorbidities: a study of data from the French national health data system. PLOS Med. 2021;18(9):e1003801.
Heath CA, Mercer SW, Guthrie B. Vascular comorbidities in younger people with dementia: a cross-sectional population-based study of 616 245 middle-aged people in Scotland. J Neurol Neurosurg Psychiatry. 2015;86(9):959–64.
Lam BYK, Yiu B, Ampil E, Chen CL-H, Dikot Y, Dominguez JC, et al. High burden of cerebral white matter lesion in 9 Asian cities. Sci Reports 2021;11(1):1–12.
Heng LC, Lim SH, Foo H, Kandiah N. Confluent white matter in progression to alzheimer dementia. Alzheimer Dis Assoc Disord. 2021;35(1):8–13.
Chen C, Homma A, Mok VCT, Krishnamoorthy E, Alladi S, Meguro K, et al. Alzheimer’s disease with cerebrovascular disease: current status in the Asia–Pacific region. J Intern Med. 2016;280(4):359–374.
Chou PS, Wu MN, Chou MC, Chien I, Yang YH. Angiotensin-converting enzyme insertion/deletion polymorphism and the longitudinal progression of Alzheimer’s disease. Geriatr Gerontol Int. 2017;17(10):1544–50.
Vipin A, Wong BYX, Kumar D, Low A, Ng KP, Kandiah N. Association between white matter hyperintensity load and grey matter atrophy in mild cognitive impairment is not unidirectional. Aging (Albany NY). 2021;13(8):10973–88.
Chen X, Huang L, Ye Q, Yang D, Qin R, Luo C, et al. Disrupted functional and structural connectivity within default mode network contribute to WMH-related cognitive impairment. Neuroimage (Amst). 2019;24:102088.
Yang Y, Fuh J, Mok VCT. Vascular contribution to cognition in stroke and Alzheimer’s disease: https://doi.org/1026599/BSA20189050001. 2018;4(1):39–48.
Xu X, Chan YH, Chan QL, Gyanwali B, Hilal S, Tan BY, et al. Global cerebrovascular burden and long-term clinical outcomes in Asian elderly across the spectrum of cognitive impairment. Int psychogeriatrics. 2018;30(9):1355–63.
Kumar D, Vipin A, Wong B, Ng KP, Kandiah N. Differential effects of confluent and nonconfluent white matter hyperintensities on functional connectivity in mild cognitive impairment. Brain Connect. 2020;10(10):547–54.
Vipin A, Loke YM, Liu S, Hilal S, Shim HY, Xu X, et al. Cerebrovascular disease influences functional and structural network connectivity in patients with amnestic mild cognitive impairment and Alzheimer’s disease. Alzheimer’s Res Ther. 2018;10(1):82.
Wong FCC, Yatawara C, Low A, Foo H, Wong BYX, Lim L, et al. Cerebral small vessel disease influences hippocampal subfield atrophy in mild cognitive impairment. Transl Stroke Res. 2021;12(2):284–92 Available from: https://pubmed.ncbi.nlm.nih.gov/32894401/.
Wong BYX, Yong TT, Lim L, Tan JY, Ng ASL, Ting SKS, et al. Medial temporal atrophy in amyloid-negative amnestic type dementia is associated with high cerebral white matter hyperintensity. J Alzheimer’s Dis. 2019;70(1):99–106.
Petrovitch H, Ross GW, Steinhorn SC, Abbott RD, Markesbery W, Davis D, et al. AD lesions and infarcts in demented and non-demented Japanese-American men. Ann Neurol. 2005;57(1):98–103.
Wilson RS, Hebert LE, Scherr PA, Barnes LL, Leon CFM de, Evans DA. Educational attainment and cognitive decline in old age. Neurology. 2009;72(5):460.
Scarmeas N, Albert S, Manly J, Stern Y. Education and rates of cognitive decline in incident Alzheimer’s disease. J Neurol Neurosurg Psychiatry. 2006;77(3):308–16.
Jacobs D, Sano M, Marder K, Bell K, Bylsma F, Lafleche G, et al. Age at onset of Alzheimer’s disease: relation to pattern of cognitive dysfunction and rate of decline. Neurology. 1994;44(7):1215–20.
Migliaccio R, Agosta F, Possin KL, Canu E, Filippi M, Rabinovici GD, et al. Mapping the progression of atrophy in early- and late-onset alzheimer’s disease. J Alzheimer’s Dis. 2015;46(2):351–64.
Lehmann M, Ghosh PM, Madison C, Laforce R, Corbetta-Rastelli C, Weiner MW, et al. Diverging patterns of amyloid deposition and hypometabolism in clinical variants of probable Alzheimer’s disease. Brain. 2013;136(Pt 3):844–58.
Lim L, Zhang A, Lim L, Choong T-M, Silva E, Ng A, et al. High caregiver burden in young onset dementia: what factors need attention? J Alzheimers Dis. 2018;61(2):537–43.
Svanberg E, Spector A, Stott J. The impact of young onset dementia on the family: a literature review. Int Psychogeriatrics. 2011;23(3):356–71.
Acknowledgements
Not applicable.
Funding
This study was supported by the National Neuroscience Institute, Singapore.
Author information
Authors and Affiliations
Contributions
AV contributed to the study design, carried out data analyses, and drafted the manuscript and figures. VS conceptualized and designed the study, carried out data analyses, and drafted the manuscript and figures. NK conceptualized and designed the study, drafted the manuscript and figures, and carried out the final review. SES contributed to the study design and drafting of the manuscript and figures and carried out the final review. WK contributed to the study design and drafting of the manuscript and figures and carried out the final review. KPN contributed to the study design and drafting of the manuscript and figures and carried out the final review. LL contributed to the acquisition of the data and design of the study. ES contributed to the acquisition of the data and design of the study. MMN contributed to the acquisition of the data and design of the study. T-MC contributed to the acquisition of the data and design of the study. EC contributed to the acquisition of the data and design of the study. LL contributed to the acquisition of the data and design of the study. ASLN contributed to the acquisition of the data and design of the study. HJC contributed to the acquisition of the data and design of the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Singhealth Centralized Review Board. The informed consent process was in accordance with the Declaration of Helsinki and local clinical research regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Figure 1.
Number of young-onset and late-onset patients in a tertiary dementia clinic over 10 years. Supplementary Figure 2. Mini Mental State Examination score over time for young and late-onset dementia.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Vipin, A., Satish, V., Saffari, S.E. et al. Dementia in Southeast Asia: influence of onset-type, education, and cerebrovascular disease. Alz Res Therapy 13, 195 (2021). https://doi.org/10.1186/s13195-021-00936-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13195-021-00936-y