
Abstract
Background
Over the past two decades, the APOE gene and its polymorphisms have been among the most studied risk factors of Alzheimer disease (AD) development; yet, there are discrepancies between various studies regarding their impact. For this reason, the evaluation of the APOE genotype has not been included in the current European Federation of Neurological Societies guidelines for AD diagnosis and management. This aim of this study was to add to this discussion by assessing the possible influence of multiple polymorphisms in the promoter region of the APOE gene and genotypes of its allele E on the risk for dementia.
Methods
We performed a comprehensive analysis of APOE gene polymorphisms, assessed the detected genotypes and correlated molecular findings with serum apolipoprotein E concentrations. The study comprised 110 patients with AD and 110 age-matched healthy individuals from the Polish population.
Results
Four polymorphisms of the APOE gene had minor allele frequency exceeding 5 % and were included in the analysis: −491A/T (rs449647), −427T/C (rs769446), −219T/G (rs405509) in the promoter region and +113G/C (rs440446) in intron 1. A protective effect of the −219G allele on AD development was observed. Also, the −491T and −219G alleles were found to be underrepresented in the carriers of the APOE E4 variant. On the basis of the genotype and linkage disequilibrium studies, a relative score was attributed to given genotypes with respect to the estimated probability of their protective effects against AD, giving rise to the ‘preventive score’. This ‘preventive score’, based on the total sums of the relative scores, expresses the protective effect deriving from the synergistic action of individual single-nucleotide polymorphisms. The ‘preventive score’ was identified as an independent predictive factor.
Conclusions
We propose a novel, more complex approach to AD risk assessment based on the additive effect of multiple polymorphic loci within the APOE promoter region, which on their own may have too weak an impact to reach the level of significance. This has potentially practical implications, as it may help to improve the informative potential of APOE testing in a clinical setting. Subsequent studies of the proposed system in large, multi-ethnic cohorts are necessary for its validation and to assess its potential practical value for clinical applications.
Similar content being viewed by others


Background
In various studies on multiple distinct ethnic groups and several different data sets performed over the last two decades, it has been shown that the epsilon 4 (E4 or ε4) variant of the apolipoprotein E (APOE) gene is associated with an increased risk for both sporadic and familial forms of Alzheimer disease (AD). However, it is also generally acknowledged that the APOE E4 variant alone is neither indispensable nor sufficient to cause the disease [1]. Subsequent series of genome-wide association studies performed with the aim of identifying further genetic predisposition sites produced contradictive outcomes [2]. Therefore, in the pursuit of identifying AD risk factors, additional APOE gene polymorphisms in the transcriptional regulatory regions of the gene —the −1000 to +400 proximal promoter region in particular—were investigated [1]. Three single-nucleotide polymorphisms (SNPs) were identified as the most promising: −491A/T (rs449647), −427T/C (rs769446) and −219T/G (rs405509) [3]. Of these, rs449647 AA and rs405509 TT genotypes were most commonly associated with AD. A number of validation studies, including a large meta-analysis consisting of 1732 patients with dementia and 1926 healthy control subjects [4], performed with individuals from various ethnic groups supported this association. The rs449647 polymorphism was shown to affect constitutional APOE transcriptional level in vitro [5], with its A allele found to increase APOE promoter activity and to confer an increased risk of AD independently of APOE E4. Alleles C and G of rs769446 and rs405509 polymorphisms, respectively, were also shown to increase APOE promoter activity [6, 7]. Further in silico studies provided additional evidence that these promoter polymorphisms are functional [1]. Interestingly, some studies suggested the role of rs405509 polymorphism to be age-dependent, with a more pronounced effect in the older population, both in the context of normal aging [8] and in the development of dementia [4, 9]. However, not all studies reproduced the reported associations and/or showed rs449647, rs769446 and rs405509 polymorphisms to be independent of E4 status [1, 9, 10]. In an attempt to clarify such discrepancies, our aim in this study was to assess possible associations between polymorphisms in the promoter region of the APOE gene and genotypes of its allele E, and the risk for dementia. We also aimed to assess associations of these polymorphisms with levels of the APOE protein in the serum. An additional aim was to assess the existence of the linkage (haplotype analysis) between APOE gene polymorphisms and dementia syndrome.
Methods
Study group
Our study included 110 patients with confirmed AD recruited from psychiatric hospitals and outpatient clinics by specialists in geriatric psychiatry. The diagnosis of AD was made on the basis of medical interviews, clinical symptoms and appropriate imaging examinations and clinical scales. All patients had a magnetic resonance imaging (MRI), computed tomography or single-photon emission computed tomography examination done and were tested on clinical scales and tests including the Hachinski Ischemic Scale, the Geriatric Depression Scale, the Mini Mental State Examination (MMSE) and the Clock Drawing Test. Relevant tests aimed at eliminating other possible causes of impairments in cognitive function were performed during the diagnostic process. These included a complete blood count, a lipidogram and other tests clinically appropriate for somatic diseases the patients had.
The age-matched control group consisted of adults (n = 110) with no signs or symptoms of dementia or a severe somatic disorder. In the whole group, a detailed questionnaire was completed by the physicians in charge, addressing putative environmental risk factors and/or the presence of somatic co-morbidities. All participants were of European origin and homogeneous ethnic (Polish) background.
Molecular and biochemical studies
Genomic DNA was extracted from peripheral blood leucocytes using ionic detergent lysis and proteinase K digestion, phenol/chloroform extraction and isopropanol precipitation according to standard methods. APOE E2/E3/E4 alleles (rs429358, rs7412) and promoter polymorphisms (rs439382, rs1799981, rs1081103, rs72654465, rs449647, rs1799982, rs769446, rs72654466, rs405509, rs72654467, rs9282609, rs440446, rs877973, rs769447) were determined by polymerase chain reaction (PCR) followed by Sanger sequencing. The following pairs of primers were used: 5′-TCT TGC TGA GGC TGG AGT G-3′ and 5′-CAA GGA TCC CAG ACT TGT CC-3′, 5′-AAG ACC TCT ATG CCC CAC CT-3′ and 5′-CCA GTC TCG CAT TCC TCA TT-3′, 5′-ACG CGG GCA CGG CTG TCC AAG GAG-3′ and 5′-CTC GCG GGC CCC GGC CTG GTA CAC-3′. Bidirectional sequencing analysis of PCR products was performed using an Applied Biosystems 3130 Genetic Analyzer and the BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems, Foster City, CA, USA). Sequences were analysed using Sequencher version 4.10.1 DNA sequencing software (Gene Codes Corporation, Ann Arbor, MI, USA). The ApoE level (expressed as milligrams per decilitre) was estimated by using the electroimmunodiffusion method using HYDRAGEL Protein(E) assay (Sebia, Evry Cedex, France) as described previously [11].
Statistical analyses
Minor allele frequency (MAF) <5 % was the criterion for exclusion from further statistical analysis. Genotype analysis was performed using additive, genotypic and dominant models; (only significant findings are presented further in the paper). Frequencies were compared using χ2 tests with continuity corrections or Fisher’s exact test with Freeman-Halton extension for 2 × 3 and 2 × 4 tables when applicable. For continuous variables, differences between groups were evaluated using the Kruskal-Wallis test for global comparisons and Mann-Whitney U tests for pairwise comparisons. Unconditional logistic regression was used to examine the association between APOE genotypes and AD. In univariate analyses, the Bonferroni correction for multiple testing was applied. Background characteristics (age, sex, education level, residence) were incorporated into the analyses. In the logistic regression analysis, indicator variables for the sex, education level and residence were added to the models. All calculations were performed using STATISTICA 12 software (StatSoft, Tulsa, OK, USA) data analysis software system.
Results
Clinical and demographic data
No significant differences were noted between patients and control subjects with respect to age, family history or the most common factor risk factors associated with dementia: previous episodes of depression, past head traumas, concomitant cardiovascular disorders, diabetes or thyroid disease. The control group included more females due to availability of participants via established and ethically approved recruitment routes (see Table 1). The median MMSE scores were 20.3 (range 15–25) for the study group and 30 (range 28–30) for the control group.
Univariable analyses of individual SNPs
The genotyping rate was 100 % in the study and control groups. Only six polymorphisms were found to have MAF exceeding 5 % and hence were eligible for statistical evaluation: rs449647, rs769446 and rs405509 in the promoter region; rs440446 in intron 1; and rs429358 and rs7412 in exon 4. The genotype distribution did not deviate significantly from the Hardy-Weinberg equilibrium. The observed frequencies of each SNP are presented in Table 2.
For each of the studied SNPs of the promoter/intron 1 region, no correlations between age at disease onset, sex, family history or somatic co-morbidities were observed. The presence of allele G of rs405509 conferred a protective effect against AD (OR 0.52 (95 % CI 0.36–0.75; p < 0.001). A similar tendency was observed with respect to allele T of rs449647; however, the correlation did not reach the level of significance (Table 2). Alleles T, G and C of rs449647, rs405509 and rs440446 SNPs, respectively, were significantly underrepresented in the carriers of the E4 variant.
ApoE serum levels were significantly lower in patients with AD (5.7 mg/dl vs. 6.5 mg/dl; p < 0.0001). Of the studied SNPs, only the rs449647 polymorphism significantly correlated with ApoE serum concentration. The presence of its allele A was associated with lower ApoE levels. Also, the differences in ApoE levels with respect to APOE epsilon variants were statistically significant (p < 0.001). The lowest levels of ApoE were noted among E4 carriers (3.72 ± 0.8 mg/dl for E4/E4 genotype, 5.54 ± 1.2 mg/dl for E3/E4 genotype), while the highest values were observed in E2 carriers (7.04 ± 1.36 mg/dl for E2/E3 genotype, 7.23 ± 0.5 mg/dl for E2/E4 genotype). Cases with E3/E3 genotype had a mean value of 6.38 ± 1.48 mg/dl. No subject with E2/E2 genotype was present in either the study or the control group. Table 2 summarizes the results of univariable analyses.
Haplotype and linkage disequilibrium analyses
Haplotype analysis of the entire APOE gene sequence (chromosome 19q, 50,100,879–50,104,489; GRCh36.3/hg18) was performed using Haploview 4.2 software, and data representative of the four distinct populations with African, Asian and European ancestry were retrieved from the HapMap database (http://hapmap.ncbi.nlm.nih.gov [accessed May 2011]) [12]. The analysis revealed five tag SNPs forming no haplotype blocks (Additional file 1). Subsequently, we evaluated the impact of APOE genotypes reported previously as predictive of the risk of AD [13]. In the genotypes comprising the E2 variant, no statistically significant differences between the study and control groups were observed. In the genotypes comprising at least one E4 variant, the −491AA/−219TT/E4 genotype was shown to increase the risk of AD (OR 5.4, 95 % CI 1.14–25.6; p = 0.02).
Afterwards, the experimental data for Polish population was analysed for the putative linkage disequilibrium (LD). LD between loci rs449647, rs405509 and rs440446 on one side, and the APOE exon 4 loci coding for epsilon variants (distant by 3 kb) on the other, was observed. Of all SNPs analysed, the strongest LD was observed for rs440446 and rs429358 (Lewontin coefficient D′ 0.956, logarithm of [base 10] odds [LOD] 11.51, r 2 = 0.127). The rs440446 locus was simultaneously linked with promoter SNPs, too, for instance with rs405509 locus distant by 0.3 kb (Lewontin coefficient D′ 0.925, LOD 32.78, r 2 = 0.428).
Multivariable analyses of the analysed risk factors
In the multivariate logistic regression analysis, the initial testing was performed using six covariates identified in the aforesaid univariate analyses (−491A/T, −219 T/G, +113G/C, E4, E2, ApoE level) and the demographic indicator variables for sex, education level and residence. The initial analysis of all nine plausible factors identified four covariates: E4, education level, male sex and residence in large cities as the significant predictors of risk of AD development. Next, the best subsets search method was used to verify the optimal set of predictors. The model likelihood statistics were computed for every possible predictor subset to identify the best subset. Eventually, the best model comprising four independent predictors of AD development was identified. The significant factors included two associated with higher risk (E4 with OR 4.12, 95 % CI 1.55–11.00; male sex with OR 3.26, 95 % CI 1.46–7.27) and two associated with lower risk (residence in large cities with OR 0.04, 95 % CI 0.01–0.37; education level with OR 0.23, 95 % CI 0.14–0.40).
‘Preventive score’
The results of simple and multivariable analyses of promoter SNPs along with linkage disequilibrium data were ultimately used as the foundation for the ‘preventive score’. Since, on the one hand, none of the studied promoter SNPs was identified as an independent prognostic factor by logistic regression, and on the other, the promoter SNPs were found in strong linkage disequilibrium, we decided to test the plausible additive benefit of their joint analysis. Accordingly, for a given genotype, a relative score was attributed with respect to its estimated probability of protective effect against AD (Table 3).
The risk for AD development expressed as the ‘preventive score’ resulting from the total sum of the relative scores (minimum 0, maximum 4) was found to be inversely related to its value. The average ‘preventive score’ in the AD group was 1.08, compared with 1.55 in the control group (p = 0.0001). ‘Preventive score’ correlated with presence of the E2 allele (Spearman rank correlation 0.40; p < 0.05) and inversely with the E4 allele (Spearman rank correlation 0.13; p < 0.05). The ‘preventive score’ correlated significantly with protein ApoE levels (Spearman rank correlation 0.25; p < 0.05), while such a correlation was not seen for individual SNPs.
The significance of 'preventive score' was further tested with multivariate logistic regression, performed in the same way as described above. The only difference was the replacement of the −491A/T, −219T/G, +113G/C and E2 covariates by the ‘preventive score’. The resulting best subset consisted of five independent prognostic factors: two associated with higher risk (E4 with OR 3.96, 95 % CI 1.90–8.26; male sex with OR 3.09, 95 % CI 1.42–6.74) and three associated with lower risk (education level with OR 0.25, 95 % CI 0.15–0.41; residence in large cities with OR 0.04, 95 % CI 0.01–0.38; ‘preventive score’ with OR 0.62, 95 % CI 0.40–0.96). The additive benefit of the ‘preventive score’ is roughly half the effect of E4 in the model.
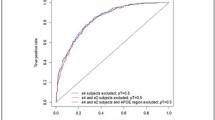
Additional statistical analyses using the logistic regression model in the subgroups of patients resulting from an inclusion/exclusion of the E2 and E4 allele carriers and in the sub-group homozygous for the E3 allele, have shown that the ‘preventive score’ allows for further delineation of the eventual risk of AD development in the subgroup of E4 carriers (for more details, see Additional file 2).
Discussion
We report a 9.1 % incidence of the APOE E4 variant in our sample derived from the Polish population, which is in line with previously published values [14]. Similarly to previous studies, we were able to show that the presence of at least one E4 variant confers almost a five times higher risk of AD development and that this correlation is gender-dependent [2]. For women, the presence of E4 variant conferred almost an eight times higher risk, while for men the association was not statistically significant (data not shown). In contrast to previously published results, no correlation between the presence of the E4 variant and the age of AD onset was observed [15]. However, our study group did not include many individuals diagnosed when they were older than 80 years of age, as late-onset AD was not a priority in our study. This might have resulted in the lack of such a correlation in our data.
Despite the reproducibility of the APOE E4 variant association with AD development, also shown in our study, the pathomechanism of such a correlation remains largely unsolved. Hence, an intense search for additional modifying factors, both intragenic and located at other loci of the genome, has been conducted worldwide. Of these, two APOE promoter SNPs—rs449647 (−491A/T) and rs405509 (−219T/G)—were shown to have predictive value for AD development [1–3, 5, 6, 9, 16–22]. However, not all studies were able to reproduce the protective effect in their populations, for instance in French [10], Irish [23], Finnish [24] or Japanese [25]. Hence, the exact role of these SNPs and their interaction with epsilon variants—in other words, their predictive character being independent or derivative of epsilon status—remains a subject of intensive debate.
In the present study, we were able to show a protective effect of −219G (rs405509) allele in a sample derived from the Polish population, while the correlation with the −491T (rs449647) allele did not reach the level of significance. This is interesting in light of an MRI study by Chen et al. [4], who showed an accelerated age-related reduction of thickness in the left parahippocampal gyrus in −219 TT carriers and suggested it as the neural substrate underlying a faster decline in cognition in individuals with this genotype. Hence, carrying a G allele might offer protection against such a process and act protectively in terms of cognition. The Chen et al. [4] study, as well as a few others (see, e.g., [9]), showed the effect of this polymorphism to be age-related. As most individuals (95 of 110) in our study were mostly older than 60 years of age, this effect might have been more pronounced.
In addition, we observed that both alleles, −219G and −491T, were significantly underrepresented in the carriers of the E4 variant. Such characteristics render the variants plausible candidates for independent risk/protective factors for AD development. However, the latter was not confirmed in the multivariable logistic regression analysis.
The inconsistent findings in previous studies regarding the presence of LD between promoter polymorphisms and the APOE epsilon variant coding SNPs were explained by the suggestion that LD may vary significantly depending on ethnic background. Here, we have shown the presence of a significant LD in the coherent group of Polish patients, being a large ethnic group with a low rate of consanguinity. The analysis of data retrieved from the HapMap project showed no haplotype blocks within the APOE gene. However, various differences in LD between individual SNPs have been observed in all ethnic groups. Lescai et al. [13] performed a similar, large-scale haplotype analysis in a group of more than 1000 Italian subjects and showed the presence of individual LDs but not haplotype blocks. In their study of the prognostic role of APOE SNPs on AD risk, the only significant additive effect has been observed for the rs405509 allele T/E4 haplotype present in phase (i.e., ‘in cis’). They did not perform a more comprehensive analysis that would include other in phase SNP loci. In our present study, we were able to show that the presence of the −491AA/−219TT/E4 genotype appears to be even more informative. It has been shown that lower ApoE levels are associated with a higher risk of developing AD. As −491A, −219T and E4 alleles have all been shown to independently decrease APOE gene expression, and hence ApoE levels [5–7], a haplotype containing all three alleles might confer a higher risk for AD because of the synergistic action of all three variants. Promoter SNPs confer a mild but additive effect on APOE expression. We showed that the ‘preventive score’ correlated significantly with protein ApoE levels, while this was not the case when individual SNPs were considered. It is possible that the SNPs need to be assessed jointly for their impact to reach significance, which might be one of the possible explanations for discrepancies in the previous reports. The results of the analysis of the above-tested polymorphisms in the promoter region of the APOE gene, in addition to increasing knowledge of the allelic variants of the gene, can be important for determining the risk of the incidence of dementia.
We believe that one of the most important findings of this study is the identification of the ‘preventive score’. Its importance derives from the fact that it takes into account an additive risk related to the presence of alleles and genotypes, which on their own may have too weak an impact to reach the level of significance. This has potentially practical implications, as it may help improve the informative potential of APOE testing in a clinical setting. The APOE testing, limited to the evaluation of the E4 variant, was not found to be sufficiently informative to be included in the current European Federation of Neurological Societies guidelines for AD diagnosis and management [26]. Here, we show that the ‘preventive score’ has an independent prognostic value, regardless of E4 status. Moreover, it has been shown to be more informative than serum ApoE levels, the ultimate marker of gene expression. The latter, owing to the complexity of protein-protein interactions and the impossibility of their direct measurement in the tissue of choice (i.e., brain), appears to be a less preferable parameter.
One important issue is the relationship between the ‘preventive score’ and epsilon variants, namely whether the ‘preventive score’ is independent of their effect, and especially the effect of the E2 allele. We attempted to tackle this issue by performing additional statistical analyses using the logistic regression model in the subgroups of patients resulting from inclusion/exclusion of the E2 and E4 allele carriers and in the subgroup homozygous for the E3 allele. They have shown that the ‘preventive score’ allows for further delineation of the eventual risk of AD development in the subgroup of E4 carriers and supports the role of the ‘preventive score’ as an additional diagnostic tool. However, these results need to be viewed with caution, as the sizes of the subgroups after the removal of the E2 and E4 alleles carriers were small (for example, only 5 % of patients with AD and 12 % of control subjects were E2 carriers), and a well-discriminating distribution of the epsilon alleles was not possible to obtain; for example, E2 homozygotes were lacking in both cohorts.
We believe that the utility of the ‘preventive score’ is an interesting and potentially useful finding; however, our results need to be replicated to confirm the validity of the score. Hence, future studies by independent research groups with larger numbers of patients are warranted.
Conclusions
We propose the ‘preventive score’ as a new predictive factor in AD. In contrast to known AD susceptibility markers, the score does not predispose to AD development but allows an estimation of individual risk for the disease. Nevertheless, further studies with large, multi-ethnic cohorts are necessary to establish its realistic utility in clinical settings.
Ethical approval and consent to participate
All patients and healthy individuals gave written informed consent for molecular genetic testing. The study was approved by the Independent Bioethics Commission for Research at the Medical University of Gdansk. The experiments were done in accordance with the Helsinki Declaration of 1975.
Abbreviations
- AD:
-
Alzheimer disease
- ApoE:
-
apolipoprotein E
- E:
-
epsilon isoform of the apolipoprotein E
- LD:
-
linkage disequilibrium
- LOD:
-
logarithm of (base 10) odds
- MAF:
-
minor allele frequency
- MMSE:
-
Mini Mental State Examination
- MRI:
-
magnetic resonance imaging
- PCR:
-
polymerase chain reaction
- SNP:
-
single-nucleotide polymorphism
References
Laws SM, Hone E, Gandy S, Martins RN. Expanding the association between the APOE gene and the risk of Alzheimer’s disease: possible roles for APOE promoter polymorphisms and alterations in APOE transcription. J Neurochem. 2003;84:1215–36.
Lambert JC, Amouyel P. Genetic heterogeneity of Alzheimer’s disease: complexity and advances. Psychoneuroendocrinology. 2007;32 Suppl 1:S62–70.
Bizzarro A, Seripa D, Acciarri A, Matera MG, Pilotto A, Tiziano FD, et al. The complex interaction between APOE promoter and AD: an Italian case-control study. Eur J Hum Genet. 2009;17:938–45.
Lambert JC, Araria-Goumidi L, Myllykangas L, Ellis C, Wang JC, Bullido MJ, et al. Contribution of APOE promoter polymorphisms to Alzheimer’s disease risk. Neurology. 2002;59:59–66.
Bullido MJ, Artiga MJ, Recuero M, Sastre I, Garcia MA, Aldudo J, et al. A polymorphism in the regulatory region of APOE associated with risk for Alzheimer’s dementia. Nat Genet. 1998;18:69–71.
Artiga MJ, Bullido MJ, Frank A, Sastre I, Recuero M, Garcia MA, et al. Risk for Alzheimer’s disease correlates with transcriptional activity of the APOE gene. Hum Mol Genet. 1998;7:1887–92.
Artiga MJ, Bullido MJ, Sastre I, Recuero M, Garcia MA, Aldudo J, et al. Allelic polymorphisms in the transcriptional regulatory region of apolipoprotein E gene. FEBS Lett. 1998;421:105–8.
Chen Y, Li P, Gu B, Liu Z, Li X, Evans AC, et al. The effects of an APOE promoter polymorphism on human cortical morphology during nondemented aging. J Neurosci. 2015;35:1423–31.
Lambert JC, Berr C, Cottel D, Amouyel P, Helbecque N. APOE promoter polymorphisms and dementia in the elderly. Neurosci Lett. 2004;365:116–9.
Zurutuza L, Verpillat P, Raux G, Hannequin D, Puel M, Belliard S, et al. APOE promoter polymorphisms do not confer independent risk for Alzheimer’s disease in a French population. Eur J Hum Genet. 2000;8:713–6.
Łojkowska W, Witkowski G, Bednarska-Makaruk M, Wehr H, Sienkiewicz-Jarosz H, Graban A, et al. Correlations between cerebellar and brain volumes, cognitive impairments, ApoE levels and APOE genotypes in patients with AD and MCI. Curr Alzheimer Res. 2013;10:964–72.
Barrett JC, Fry B, Maller J, Daly MJ. Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics. 2005;21:263–5.
Lescai F, Chiamenti AM, Codemo A, Pirazzini C, D’Agostino G, Ruaro C, et al. An APOE haplotype associated with decreased ε4 expression increases the risk of late onset Alzheimer’s disease. J Alzheimers Dis. 2011;24:235–45.
Kowalska A, Wiechmann I, Walter H. Genetic variability of apolipoprotein E in a Polish population. Hum Biol. 1998;70:1093–9.
Raber J, Huang Y, Ashford JW. ApoE genotype accounts for the vast majority of AD risk and AD pathology. Neurobiol Aging. 2004;25:641–50.
Beyer K, Lao JI, Gomez M, Riutort N, Latorre P, Mate JL, et al. The Th1/E4cs-G apolipoprotein E (APOE) promoter allele is a risk factor for Alzheimer disease of very later onset. Neurosci Lett. 2002;326:187–90.
Alvarez-Arcaya A, Combarros O, Llorca J, Sánchez-Guerra M, Berciano J, Fernández-Luna JL. The −491 TT apolipoprotein E promoter polymorphism is associated with reduced risk for sporadic Alzheimer’s disease. Neurosci Lett. 2001;304:204–8.
Town T, Paris D, Fallin D, Duara R, Barker W, Gold M, et al. The −491A/T apolipoprotein E promoter polymorphism association with Alzheimer’s disease: independent risk and linkage disequilibrium with the known APOE polymorphism. Neurosci Lett. 1998;252:95–8.
Casadei VM, Ferri C, Veglia F, Gavazzi A, Salani G, Cattaneo M, et al. APOE −491 promoter polymorphism is a risk factor for late-onset Alzheimer’s disease. Neurology. 1999;53:1888–9.
Yang JD, Feng GY, Zhang J, Cheung J, St. Clair D, He L. Apolipoprotein E −491 promoter polymorphism is an independent risk factor for Alzheimer’s disease in the Chinese population. Neurosci Lett. 2003;350:25–8.
Parra-Bonilla G, Arboleda G, Tunis J, Solano E, Pardo R, Arango G, et al. Haplogroup analysis of the risk associated with APOE promotor polymorphisms (−219T/G, −491A/T and −427T/C) in Colombian Alzheimer’s disease patients. Neurosci Lett. 2003;349:159–62.
Nicodemus KK, Stenger JE, Schmechel DE, Welsh-Bohmer KA, Saunders AM, Roses AD, et al. Comprehensive association analysis of APOE regulatory region polymorphisms in Alzheimer disease. Neurogenetics. 2004;5:201–8.
Lynch CA, Brazil J, Cullen B, Coakley D, Gill M, Lawlor BA, et al. Apolipoprotein E promoter polymorphisms (−491A/T and −427T/C) and Alzheimer’s disease: no evidence of association in the Irish population. Ir J Med Sci. 2008;177:29–33.
Helisalmi S, Hiltunen M, Valonen P, Mannermaa A, Koivisto AM, Lehtovirta M, et al. Promoter polymorphism (−491A/T) in the APOE gene of Finnish Alzheimer’s disease patients and control individuals. J Neurol. 1999;246:821–4.
Kimura M, Matsushita S, Arai H, Matsui T, Yuzuriha T, Higuchi S. No evidence of association between apolipoprotein E gene regulatory region polymorphism and Alzheimer’s disease in Japanese. J Neural Transm. 2000;107:1449–56.
Hort J, O’Brien JT, Gainotti G, Pirttila T, Popescu BO, Rektorova I, et al. EFNS guidelines for the diagnosis and management of Alzheimer’s disease. Eur J Neurol. 2010;17:1236–48.
Acknowledgements
We thank the Drs. D. Ussorowska, K. Gustaw-Rothenberg, I. Trzebiatowska, K. Soltys, J. Kosinska, J. Lapin and J. Turczynski for providing AD cases. We are grateful also to the patients and healthy individuals who participated in this research.
Funding
This work was supported by Polish Ministry of Science and Higher Education grant 2 P05A 03027.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
ALS conceived of the study, participated in its design and coordination, coordinated clinical aspects of the study, performed clinical evaluations of healthy volunteers, carried out the molecular genetic studies, participated in the sequence alignment and drafted the manuscript. BSL-Z performed the statistical analysis and drafted the manuscript. MC and BW carried out the molecular genetic studies, participated in the sequence alignment evaluations and helped to draft the manuscript. LB helped with clinical evaluations and drafting of the manuscript. BRG helped with data analyses and drafting of the manuscript. JL conceived of the study, participated in its design and coordination, and helped to draft the manuscript. All authors read and approved the final manuscript.
Additional files
Additional file 1:
Haplotype analysis of the SNPs representative of APOE locus. Results of the haplotype analysis of the SNPs representative of APOE locus based on data retrieved from the HapMap Project database. (PDF 348 kb)
Additional file 2:
Logistic regression analyses in the subgroups of patients carrying E2/E3/E4 alleles. Summary of the statistical analyses using the logistic regression model approach in the subgroups of patients resulting from inclusion and/or exclusion of the E2 and E4 allele carriers and in the subgroup homozygous for the E3 allele. (PDF 312 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Limon-Sztencel, A., Lipska-Ziętkiewicz, B.S., Chmara, M. et al. The algorithm for Alzheimer risk assessment based on APOE promoter polymorphisms. Alz Res Therapy 8, 19 (2016). https://doi.org/10.1186/s13195-016-0187-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13195-016-0187-9