
Abstract
Background
The Curcuma longa L. (CLL) rhizome has long been used to treat patients with hepatic dysfunction. CLL is a member of the ginger family of spices that are widely used in China, India, and Japan, and is a common spice, coloring, flavoring, and traditional medicine. This study was performed to evaluate the hepatoprotective activity of CLL extract and its active component curcumin in an acute carbon tetrachloride (CCl4)-induced liver stress model.
Methods
Acute hepatic stress was induced by a single intraperitoneal injection of CCl4 (0.1 ml/kg body weight) in rats. CLL extract was administered once a day for 3 days at three dose levels (100, 200, and 300 mg/kg/day) and curcumin was administered once a day at the 200 mg/kg/day. We performed alanine transaminase (ALT) and aspartate transaminase (AST). activity analysis and also measured total lipid, triglyceride, and cholesterol levels, and lipid peroxidation.
Results
At 100 g CLL, the curcuminoid components curcumin (901.63 ± 5.37 mg/100 g), bis-demethoxycurcumin (108.28 ± 2.89 mg/100 g), and demethoxycurcumin (234.85 ± 1.85 mg/100 g) were quantified through high liquid chromatography analysis. In CCl4-treated rats, serum AST and ALT levels increased 2.1- and 1.2-fold compared with the control. AST but not ALT elevation induced by CCl4 was significantly alleviated in CLL- and curcumin-treated rats. Peroxidation of membrane lipids in the liver was significantly prevented by CLL (100, 200, and 300 mg/kg/day) on tissue lipid peroxidation assay and immunostaining with anti-4HNE antibody. We found that CLL extract and curcumin exhibited significant protection against liver injury by improving hepatic superoxide dismutase (p < 0.05) and glutathione peroxidase activity, and glutathione content in the CCl4-treated group (p < 0.05), leading to a reduced lipid peroxidase level.
Conclusion
Our data suggested that CLL extract and curcumin protect the liver from acute CCl4-induced injury in a rodent model by suppressing hepatic oxidative stress. Therefore, CLL extract and curcumin are potential therapeutic antioxidant agents against acute hepatotoxicity.
Similar content being viewed by others

Background
Curcumin, the pure active component of Curcuma longa L. (CLL) and the yellow pigment that is a characteristic feature of curry [1], has been studied for its anti-inflammatory [2], immunoregulatory [3], and other beneficial effects in models of hepatic dysfunction. Researchers have performed a variety of studies to develop natural products that improve hepatic function, including studies of CLL extracts. The mechanism of the protective effects of CLL against hepatic dysfunction has been suggested to be the inhibition of tumor necrosis factor (TNF)-induced apoptosis [4, 5]. As a polyphenolic antioxidant, curcumin has been suggested to inhibit the activation of fibrosis in vitro by reducing cell proliferation and inducing apoptosis [5]. The antioxidant effects of CLL extracts and curcumin have also been studied in a rat model of carbon tetrachloride (CCl4)-induced liver injury [6, 7]. Similarly, the hepatoprotective activity of Silybum marianum [8], Tridax procumbens [9], Andrographis paniculata [10], and Eucommia ulmoides [11] have been studied to develop herbal medicines and functional foods to improve hepatic function. The systems used for developing natural products and medicines are usually based upon severe hepatic dysfunction models such as liver necrosis, necrosis, and cirrhosis [12]. However, people are frequently exposed to subclinical hepatic stress, and, if a hepatotoxin-associated hepatic event exceeds the hepatic capacity for clearing these toxins, hepatic function can be transiently decreased, leading to acute liver failure. Chemicals often cause subclinical injury to the liver that manifests only as abnormal liver enzyme levels, such as AST. Drug-induced liver injury is responsible for 5% of all hospital admissions and 50% of all cases of acute liver failure [13]. Although treatment of acute liver failure is considered clinically important [14, 15], few preventive products or medicines have been established. In this study, we evaluated the hepatoprotective activity of CLL extract and curcumin in a CCl4-induced acute liver toxicity rat model. Compared with other studies of CCl4-induced liver cirrhosis, fibrosis and other severe hepatic toxicities [16–19], our research design is an acute/transient toxicity study based on “a low dose of chemical toxin and one time exposure without histological abnormalities.” Considering that transient or acute toxicity can be more frequently happening to human, the acute/transient toxicity model might have a more importantly clinical meaning than other chronic/severe toxicity. We also sought to determine whether the antioxidant properties of CLL extracts or curcumin are involved in the protective effects against acute liver toxicity.
Methods
Extract preparation
Korean CLL rhizomes were harvested from Jindo, Korea and extracts were manufactured by the Ottogi Corporation (Seoul, Korea). The roots were crushed and loaded into an extractor. The first and second extractions were carried out with 50% ethanol. The second extracts were filtered and gathered with the first extracts and were concentrated under reduced pressure (20 brix). Twenty percent dextrin was added to the final extracts and they were sterilized. The total yield was 18% based upon weight.
Quantitation of curcumin and curcuminoids using HPLC–DAD
Curcumin and curcuminoids were prepared with 100% methanol and quantitated with an HPLC system (Agilent 1100 series, Germany) equipped with a Zorbax Eclipse C18 column (250 × 4.0 mm2). The mobile phase consisted of 1% acetic acid in water (A) and 52% acetonitrile (B); the column was equilibrated for 10 min in the mobile phase and then washed with 100% (B) for 10 min. The column was operated at room temperature with a 1 ml/min flow rate. The injection volume was 5 μl, and curcumin, curcuminoids, bis-demethoxycurcumin (BDMC), and demethoxycurcumin (DMC) were detected at a wavelength of 424 nm.
Reagents and chemicals
Carbon tetrachloride and curcumin were purchased from Sigma Chemicals Co. (St. Louis, MO, USA). The commercial kits used for assaying liver enzymes and antioxidants are described below.
Animals
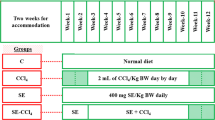
One hundred male Sprague–Dawley (SD) rats (250–280 g) were purchased from Central Lab Animal Inc. (Seoul, Korea) randomly assigned into groups. The experimental animals were given free access to standard diet and water in rooms maintained at 25 °C on 12-h light/dark cycles. Four rats were sacrificed for preliminary CCl4 toxicity testing, and 12 of the surviving rats were placed in each of the following groups. Control rats were injected with olive oil (vehicle; 0.1 ml/kg body weight, i.p.) for 72 h. The curcumin group was intragastrically administered with 200 mg/kg curcumin for 72 h. The CLL group was intragastrically administered with 300 mg/kg CLL extract. The CCl4 group received CCl4 (0.1 ml/kg, i.p.) for 72 h. The CCl4-curcumin group received curcumin (200 mg/kg) intragastrically before 3 days of CCl4 treatment. The CCl4-CLL groups received 100 mg/kg, 200 mg/kg, or 300 mg/kg of CLL extract intragastrically before 3 days of CCl4 treatment. All of the experimental protocols conducted on rats were performed in accordance with internationally accepted principles for laboratory animal use and care and approval was obtained from the Care and Use of Laboratory Animals Committee of Chonbuk National University Hospital. All procedures were also approved by the Institutional Animal Care and Use Committee of Chonbuk National University Hospital (IACUC protocol CBU 150608-25).
Liver immunohistochemistry
Immunohistochemistry was performed using 4-μm-thick deparaffinized liver tissue sections as described earlier [20]. Briefly, deparaffinized liver slices were incubated overnight with antibodies against 4-hydroxynonenal (4-HNE). Antibody detection was performed using the DAKO EnVision + System Peroxidase/DAB kit.
AST and ALT activity
Serum levels of liver enzymes AST and ALT were estimated using commercially available diagnostic kits (Cat. AM101-K, Asan Pharm, Seoul, Korea) according to the manufacturer’s protocol.
Lipid profile analysis
Total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein cholesterol (LDL), and triglycerides (TG) were estimated using commercially available diagnostic kits (Cat. AM203-K and AM 202-K, Asan Pharm).
Antioxidant enzymes
The activity of SOD and glutathione peroxidase (GPx) was analyzed using assay kits from Cayman according to the manufacturer’s instructions (Cat.706002 and 703102, Cayman, Ann Arbor, MI, USA).
GSH/GSSG analysis
The level of serum reduced and oxidized glutathione (GSH and GSSG) was measured using a kit from BioVision (Cat. K264, BioVision, Inc, CA, USA) according to the manufacturer’s protocol.
Determination of tissue lipid peroxidation
The level of serum and liver lipid peroxidation was measured using a thiobarbituric acid reactive substances (TBARS) kit from Cayman (Cat. 10009055) according to the manufacturer’s protocol.
Statistics
Results are presented as the mean ± SEM. MicroCal Origin software (Northampton, MA, USA) was used for all statistical calculations. Differences were tested for significance using one-way analysis of variance (ANOVA) with Duncan’s multiple range test. Statistical significance was set at p < 0.05.
Results
Curcuminoid components of CLL turmeric
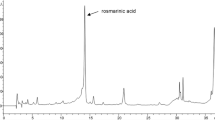
From the CLL extract, major compounds including curcumin, bis-demethoxycurcumin (BDMC), and demethoxycurcumin (DMC) (Fig. 1a) were identified and quantified using HPLC. From 100-g CLL extracts, curcumin (901.63 ± 5.37 mg/100 g), BDMC (108.28 ± 2.89 mg/100 g), DMC (234.85 ± 1.85 mg/100 g) and total curcuminoids (1244.76 ± 3.86 mg/100 g) were quantified (Table 1). The representative HPLC chromatogram is presented in Fig. 1b.

HPLC analysis of CLL extract. a Chemical structure of curcumin, demethoxycurcumin (DMC), and bisdemethoxycurcumin (BDMC). b HPLC chromatogram analysis of CLL extract
CLL turmeric extract and curcumin protect against the CCl4-induced toxicity profile
To examine the role of CLL turmeric extract and curcumin in hepatic toxicity, the extract and curcumin were applied to a CCl4-induced acute toxicity model. The serum activity of AST was increased in the CCl4 group compared with the control group (Fig. 2). CCl4-increased AST activity was significantly reduced in the presence of CLL extract or curcumin. Although serum ALT level showed a similar pattern to AST level, there were no significance differences between CCl4 and the combined CLL extract or curcumin groups. Consistent with these data, AST serum level rather than ALT has been used as a biochemical marker for early acute hepatotoxicity [21, 22].

Effects of CLL extract on serum liver biomarkers. Serum AST (a) and ALT (b) were analyzed in control, 0.1 ml/kg CCl4, CCl4 with curcumin, CCl4 with CLL extract (100, 200, or 300 mg/kg), 200 mg/kg curcumin alone, and 300 mg/kg CLL extract alone groups. Each bar represents the mean value of experiments performed in triplicate ± S.E.M. (n = 10). *p < 0.05 compared with the CCl4 group
CLL turmeric extract does not affect serum lipid profile in a CCl4-induced acute toxicity model
Serum cholesterol, triglycerides, and LDL levels did not vary significantly between the CCl4 group and the control group. Administration of CLL extract alone resulted in a non-significant change in lipid profiles compared to the control group (Table 2).
CLL turmeric extract increases antioxidant enzymes in a CCl4-induced acute toxicity model
Liver activity of SOD and GPx was decreased in the CCl4 group compared with the control group (Fig. 3a, b). The CCl4-induced decrease in SOD and GPx activity recovered after treatment with CLL extract or curcumin. In the SOD activity analysis, CLL extract showed a dose-dependent recovery effect; the highest CLL extract dose, 300 mg/kg, showed the greatest protective effect against decreased SOD activity. In the GPx activity analysis, a relatively low dose of 100 mg/kg CLL showed the greatest recovery effect against decreased GPx activity, similar to the recovery effect of curcumin.

Effects of CLL extract on SOD and GPx activity. a Hepatic SOD and b GPx activity was analyzed in control, 0.1 ml/kg CCl4, CCl4 with curcumin, CCl4 with CLL extract (100, 200, or 300 mg/kg), 200 mg/kg curcumin alone, and 300 mg/kg CLL extract alone groups. Each bar represents the mean value of experiments performed in triplicate ± S.E.M. (n = 10). *p < 0.05 compared with the CCl4 group
CLL turmeric extract inhibits lipid peroxidation in a CCl4-induced acute toxicity model
Increased levels of reactive oxygen species (ROS) induce membrane lipid peroxidation and the production of associated by-products such as malondialdehyde (MDA) and 4HNE [23]. As a product of lipid peroxidation, the MDA level can reflect the liver lipid peroxidation level [24]. In damaged tissues, 4HNE has been found in higher quantities during oxidative stress due to the increase in the lipid peroxidation chain reaction [25]. Figure 4a shows that the liver MDA level increased significantly in CCl4-treated mice compared with the control group. Treatment with CLL extract (200 and 300 mg/kg) reduced this CCl4-induced increase in MDA. In addition, our results showed that the number of 4-HNE-stained hepatocytes increased in the CCl4-treated mice (Fig. 4b). Treatment with CLL extract (100, 200, and 300 mg/kg) reduced the CCl4-induced increase in 4-HNE-stained cells. Curcumin treatment consistently showed similar effects to CLL extract. These data collectively suggest that CLL extract protects the liver against CCl4-induced oxidative stress.

Effects of CLL extract on hepatic lipid peroxidation. The formation of a malondialdehyde (MDA) and b 4-HNE was analyzed in control, 0.1 ml/kg CCl4, CCl4 with 200 mg/kg curcumin, CCl4 with CLL extract (100, 200, or 300 mg/kg), 200 mg/kg curcumin, and 300 mg/kg CLL extract groups. Each bar represents the mean value of experiments performed in triplicate ± S.E.M. (n = 10). *p < 0.05 compared with the CCl4 group
CLL turmeric extract and curcumin affect GSH profiles in a CCl4-induced acute toxicity model
GSH is an important cellular antioxidant that protects cells against ROS-induced liver injury [26]. The efficient transformation of GSH to GSSG has been suggested to be a marker of redox capacity to explain the cellular redox environment [27, 28]. The data shown in Fig. 5a confirm the decrease in GSH level in CCl4-treated rats. CLL extract dose-dependently rescued the CCl4-induced decrease in liver GSH level. The oxidation product, GSSG, showed a similar pattern (data not shown). Compared to the control group, the level of total glutathione, including GSSG, was significantly reduced by CCl4 (Fig. 5b). CLL extract significantly recovered the decreased total GSH level in a dose-dependent manner. The recovery effect of 300 mg/kg CLL was similar to that of curcumin, suggesting that CLL extract and its pure component curcumin protect against oxidative stress by enhancing the intrahepatic redox capacity.

Effects of CLL extract on hepatic redox capacity. a Reduced glutathione (GSH), b total GSH, c GSH/oxidized glutathione (GSSG) ratio and d GSH+GSSG content were analyzed in control, 0.1 ml/kg CCl4, CCl4 with 200 mg/kg curcumin, CCl4 with CLL extract (100, 200, or 300 mg/kg), 200 mg/kg curcumin, and 300 mg/kg CLL extract groups. Each bar represents the mean value of experiments performed in triplicate ± S.E.M. (n = 10). *p < 0.05 compared with the CCl4 group
Discussion
In this report, we showed that the application of CLL extracts markedly inhibited acute hepatic failure in a rat model of acute hepatic injury, which was induced at least in part by free radical formation. Our data suggest that CLL and its active component curcumin are effective against acute liver stress by enhancing redox capacity and antioxidant enzyme activity. In this study, the acute CCl4 toxicity model was used to evaluate the efficacy of CLL extract in acute hepatic stress. Acute CCl4 administration is a widely used experimental model that mimics the acute liver failure caused by toxic substances [29–31]. Although the liver plays a key role in transforming and clearing chemicals, certain medicinal agents, when taken in excess, may injure the organ. Other chemical agents or industrial agents can also induce hepatotoxicity. These chemicals often cause subclinical injury to the liver, increasing liver enzymes, but not causing pathological abnormalities such as histological and hepatosteatosis status changes. Drug-induced acute liver failure is an important clinical issue [13], and thus therapeutic and preventive strategies against acute liver toxicity need to be developed. In the acute toxicity model, CCl4 did not induce hepatic lipid accumulation (Table 2), but did increase activity of the main liver enzyme AST (Fig. 2), a routinely observed acute toxicity-associated clinical symptom. CLL extract inhibited this increase in AST activity. Although AST and ALT aminotransferases are both highly concentrated in the liver, this model showed an increase in AST, but not ALT. A similar pattern was reported recently in cases of acute hepatic and transient stress [22, 32]. AST is localized in the mitochondria, whereas ALT is distributed throughout the cytoplasm. In the case of hepatic stress, mitochondrial damage with ROS accumulation tends to increase the level of AST rather than ALT [33, 34]. The manifestation of acute hepatotoxicity in acute stress is highly variable, ranging from asymptomatic elevation of liver enzymes to fulminant hepatic failure [35]. Because of the considerable disease burden, there is growing interest in understanding acute hepatic failure. One representative system for understanding acute hepatic failure is the CCl4 model. Metabolic activation of CCl4 by mixed function oxidases is required to induce hepatotoxicity. The initial step in liver injury induction by CCl4 is mainly its dehalogenation by cytochrome p-450 2E1 (CYP2E1) to a trichloromethyl free radical (\({\text{CCl}}_{3}^{ - }\)), which leads to hepatic toxicity [36]. A single injection of CCl4 did not induce hepatic lipid accumulation, but simply resulted in increased AST activity and hepatic ROS accumulation. The damage pattern was transient, with recovery to a normal state (data not shown). The main point of this study was transient stress. Hepatic stress that occurs during life is typically transient; at rest, the liver recovers after a short period of time and therefore the stress often goes unnoticed clinically. The initial hypothesis of this study was that foods that prevent routine acute stress might be good for maintaining hepatic health; in this regard, CLL extract was a strong candidate for testing the hypothesis. Curcumin and CLL extracts have been frequently studied with regard to hepatoprotective function. However, the main design of those studies was based on a high level of toxin-induced hepatic dysfunction [2, 37, 38], which varied from the present study’s design; acute or transient toxicity without abnormal liver function except liver enzyme. Throughout this study, CLL extract and its active component curcumin showed antioxidant enzyme activity and a regulatory effect against the accumulation of ROS, including lipid peroxidation, resulting in a protective effect against CCl4-induced acute hepatotoxicity. Although the suggested antioxidant mechanism is similar to its application in severe hepatotoxicity, this study strongly suggests the possible application of CLL to transient or acute hepatic stress conditions. Other studies indicated that CLL treatment induces an augmentation of hepatic Nrf-2 protein levels [2] and stimulates antioxidant activity [38–40]. Curcumin, the main component of CLL, significantly reduced the CCl4-induced increase in hepatic MDA [7], implying that CLL exerts protective effects against CCl4-induced liver damage by preventing lipid peroxide formation and by blocking the oxidative chain reaction [41]. Our results indicated that CCl4 administration led to a marked depletion of glutathione (GSH) level in the liver. GSH, a cytosolic tripeptide, is ubiquitously present in all cell types at millimolar concentrations and is the major non-enzymatic regulator of intracellular redox homeostasis [42]. GSH is oxidized to GSSG by the enzymatic reaction catalyzed by glutathione peroxidase (GPx), which is reduced back to GSH by glutathione reductase [43]. Our results showed a drastic reduction in the activity of GPx in the liver caused by CCl4, which could compromise the defenses of the liver. Our results suggested that CCl4 administration decreased the concentrations of reduced GSH and total GSH in the liver, altering the redox status of the cells, and that treatment with CLL extract and its active component curcumin led to recovery of redox balance. Increases in the levels of reduced GSH and total GSH upon treatment with CLL extracts may be involved in the protective mechanism against CCl4-induced liver toxicity.
Conclusion
In this study, CLL extract and its active component curcumin showed protective activity against CCl4-induced hepatotoxicity. In addition to antioxidant activity, CLL extracts and their active components might play a role in restoring the liver redox capacity, as represented by GSH-GSSG cycling capacity. In future studies, derivatives of CLL extracts should be examined in various experimental models of acute toxicity in addition to CCl4. Active derivatives may be potential drug candidates for acute liver failure and toxicity.
Change history
11 June 2024
An Editorial Expression of Concern to this paper has been published: https://doi.org/10.1186/s13104-024-06818-4
Abbreviations
- CLL:
-
Curcuma longa L. turmeric
- CCl4 :
-
carbon tetrachloride
- AST:
-
aspartate transaminase
- ALT:
-
alanine transaminase
- MDA:
-
malondialdehyde
- SOD:
-
superoxide dismutase
- GPx:
-
glutathione peroxidase
- 4-HNE:
-
4-hydroxynonenal
- ROS:
-
reactive oxygen species
- CYP2E1:
-
cytochrome p-450 2E1
- BDMC:
-
demethoxycurcumin
- DMC:
-
demethoxycurcumin
- LDL:
-
low-density lipoprotein
- HDL:
-
high density lipoprotein
References
Rezaei-Moghadam A, Mohajeri D, Rafiei B, Dizaji R, Azhdari A, Yeganehzad M, Shahidi M, Mazani M. Effect of turmeric and carrot seed extracts on serum liver biomarkers and hepatic lipid peroxidation, antioxidant enzymes and total antioxidant status in rats. Bioimpacts. 2012;2(3):151–7.
Lee HS, Li L, Kim HK, Bilehal D, Li W, Lee DS, Kim YH. The protective effects of Curcuma longa Linn. extract on carbon tetrachloride-induced hepatotoxicity in rats via upregulation of Nrf2. J Microbiol Biotechnol. 2010;20(9):1331–8.
Nagpal M, Sood S. Role of curcumin in systemic and oral health: an overview. J Nat Sci Biol Med. 2013;4(1):3–7.
Li M, Wu Z, Niu W, Wan Y, Zhang L, Shi G, Xi X. The protective effect of curcumin against the 19 kDa Mycobacterium tuberculosis protein-induced inflammation and apoptosis in human macrophages. Mol Med Rep. 2014;10(6):3261–7.
Xu J, Fu Y, Chen A. Activation of peroxisome proliferator-activated receptor-gamma contributes to the inhibitory effects of curcumin on rat hepatic stellate cell growth. Am J Physiol Gastrointest Liver Physiol. 2003;285(1):G20–30.
Wu SJ, Lin YH, Chu CC, Tsai YH, Chao JC. Curcumin or saikosaponin a improves hepatic antioxidant capacity and protects against CCl4-induced liver injury in rats. J Med Food. 2008;11(2):224–9.
Fu Y, Zheng S, Lin J, Ryerse J, Chen A. Curcumin protects the rat liver from CCl4-caused injury and fibrogenesis by attenuating oxidative stress and suppressing inflammation. Mol Pharmacol. 2008;73(2):399–409.
Shahbazi F, Sadighi S, Dashti-Khavidaki S, Shahi F, Mirzania M, Abdollahi A, Ghahremani MH. Effect of silymarin administration on cisplatin nephrotoxicity: report from a pilot, randomized, double-blinded, placebo-controlled clinical trial. Phytother Res. 2015;29(7):1046–53.
Ravikumar V, Shivashangari KS, Devaki T. Effect of Tridax procumbens on liver antioxidant defense system during lipopolysaccharide-induced hepatitis in d-galactosamine sensitised rats. Mol Cell Biochem. 2005;269(1–2):131–6.
Zou Y, Xiong H, Xiong H, Lu T, Zhu F, Luo Z, Yuan X, Wang Y. A polysaccharide from Andrographis paniculata induces mitochondrial-mediated apoptosis in human hepatoma cell line (HepG2). Tumour Biol. 2015;36(7):5179–86.
Jin CF, Li B, Lin SM, Yadav RK, Kim HR, Chae HJ. Mechanism of the inhibitory effects of Eucommia ulmoides Oliv. cortex extracts (EUCE) in the CCl 4-induced acute liver lipid accumulation in rats. Int J Endocrinol. 2013;2013:751854.
Wang K. Molecular mechanisms of hepatic apoptosis. Cell Death Dis. 2014;5:e996.
Ostapowicz G, Fontana RJ, Schiodt FV, Larson A, Davern TJ, Han SH, McCashland TM, Shakil AO, Hay JE, Hynan L, et al. Results of a prospective study of acute liver failure at 17 tertiary care centers in the United States. Ann Intern Med. 2002;137(12):947–54.
Jalan R. Acute liver failure: current management and future prospects. J Hepatol. 2005;42(Suppl (1)):S115–23.
Polson J, Lee WM, American Association for the Study of Liver D. AASLD position paper: the management of acute liver failure. Hepatology. 2005;41(5):1179–97.
Domitrovic R, Jakovac H, Tomac J, Sain I. Liver fibrosis in mice induced by carbon tetrachloride and its reversion by luteolin. Toxicol Appl Pharmacol. 2009;241(3):311–21.
Louka ML, Ramzy MM. Involvement of fibroblast-specific protein 1 (S100A4) and matrix metalloproteinase-13 (MMP-13) in CCl4-induced reversible liver fibrosis. Gene. 2016;579(1):29–33.
Munoz-Ortega MH, Llamas-Ramirez RW, Romero-Delgadillo NI, Elias-Flores TG, Tavares-Rodriguez Ede J, Campos-Esparza Mdel R, Cervantes-Garcia D, Munoz-Fernandez L, Gerardo-Rodriguez M, Ventura-Juarez J. Doxazosin treatment attenuates carbon tetrachloride-induced liver fibrosis in hamsters through a decrease in transforming growth factor beta secretion. Gut Liver. 2016;10(1):101–8.
Wang Z, Zhang Z, Du N, Wang K, Li L. Hepatoprotective effects of grape seed procyanidin B2 in rats with carbon tetrachloride-induced hepatic fibrosis. Altern Ther Health Med. 2015;21(Suppl 2):12–21.
Domitrovic R, Jakovac H, Marchesi VV, Sain I, Romic Z, Rahelic D. Preventive and therapeutic effects of oleuropein against carbon tetrachloride-induced liver damage in mice. Pharmacol Res. 2012;65(4):451–64.
Tossige-Gomes R, Ottone VO, Oliveira PN, Viana DJ, Araujo TL, Gripp FJ, Rocha-Vieira E. Leukocytosis, muscle damage and increased lymphocyte proliferative response after an adventure sprint race. Braz J Med Biol Res. 2014;47(6):492–8.
Andres-Hernando A, Altmann C, Bhargava R, Okamura K, Bacalja J, Hunter B, Ahuja N, Soranno D, Faubel S. Prolonged acute kidney injury exacerbates lung inflammation at 7 days post-acute kidney injury. Physiol Rep. 2014;2(7):e12084.
Singh R, Wang Y, Schattenberg JM, Xiang Y, Czaja MJ. Chronic oxidative stress sensitizes hepatocytes to death from 4-hydroxynonenal by JNK/c-Jun overactivation. Am J Physiol Gastrointest Liver Physiol. 2009;297(5):G907–17.
Misra HP, Rabideau C. Pirfenidone inhibits NADPH-dependent microsomal lipid peroxidation and scavenges hydroxyl radicals. Mol Cell Biochem. 2000;204(1–2):119–26.
Hartley DP, Kolaja KL, Reichard J, Petersen DR. 4-Hydroxynonenal and malondialdehyde hepatic protein adducts in rats treated with carbon tetrachloride: immunochemical detection and lobular localization. Toxicol Appl Pharmacol. 1999;161(1):23–33.
Srivastava S, Sinha D, Saha PP, Marthala H, D’Silva P. Magmas functions as a ROS regulator and provides cytoprotection against oxidative stress-mediated damages. Cell Death Dis. 2014;5:e1394.
Nur E, Verwijs M, de Waart DR, Schnog JJ, Otten HM, Brandjes DP, Biemond BJ, Elferink RP, Group CS. Increased efflux of oxidized glutathione (GSSG) causes glutathione depletion and potentially diminishes antioxidant defense in sickle erythrocytes. Biochim Biophys Acta. 2011;1812(11):1412–7.
Mizuashi M, Ohtani T, Nakagawa S, Aiba S. Redox imbalance induced by contact sensitizers triggers the maturation of dendritic cells. J Invest Dermatol. 2005;124(3):579–86.
Ma JQ, Li Z, Xie WR, Liu CM, Liu SS. Quercetin protects mouse liver against CCl(4)-induced inflammation by the TLR2/4 and MAPK/NF-kappaB pathway. Int Immunopharmacol. 2015;28(1):531–9.
Cao G, Li Q, Chen X, Cai H, Tu S. Hepatoprotective effect of superfine particles of herbal medicine against CCl4-induced acute liver damage in rats. Biomed Res Int. 2014;2014:934732.
Li W, Wu Y, Zhu C, Wang Z, Gao R, Wu Q. Anti-fibrosis effects of Huisheng oral solution in CCl4-induced hepatic fibrosis in rat. Indian J Pharmacol. 2014;46(2):216–21.
Wang XY, Luo JP, Chen R, Zha XQ, Wang H. The effects of daily supplementation of Dendrobium huoshanense polysaccharide on ethanol-induced subacute liver injury in mice by proteomic analysis. Food Function. 2014;5(9):2020–35.
Shen J, Zhang J, Wen J, Ming Q, Zhang J, Xu Y. Correlation of serum alanine aminotransferase and aspartate aminotransferase with coronary heart disease. Int J Clin Exp Med. 2015;8(3):4399–404.
Hu Z, Lausted C, Yoo H, Yan X, Brightman A, Chen J, Wang W, Bu X, Hood L. Quantitative liver-specific protein fingerprint in blood: a signature for hepatotoxicity. Theranostics. 2014;4(2):215–28.
Jiao J, Friedman SL, Aloman C. Hepatic fibrosis. Curr Opin Gastroenterol. 2009;25(3):223–9.
Khan RA, Khan MR, Sahreen S. CCl4-induced hepatotoxicity: protective effect of rutin on p53, CYP2E1 and the antioxidative status in rat. BMC Complement Altern Med. 2012;12:178.
Park EJ, Jeon CH, Ko G, Kim J, Sohn DH. Protective effect of curcumin in rat liver injury induced by carbon tetrachloride. J Pharm Pharmacol. 2000;52(4):437–40.
Deshpande UR, Gadre SG, Raste AS, Pillai D, Bhide SV, Samuel AM. Protective effect of turmeric (Curcuma longa L.) extract on carbon tetrachloride-induced liver damage in rats. Indian J Exp Biol. 1998;36(6):573–7.
Sharma OP. Antioxidant activity of curcumin and related compounds. Biochem Pharmacol. 1976;25(15):1811–2.
Salama SM, Abdulla MA, AlRashdi AS, Ismail S, Alkiyumi SS, Golbabapour S. Hepatoprotective effect of ethanolic extract of Curcuma longa on thioacetamide induced liver cirrhosis in rats. BMC Complement Altern Med. 2013;13:56.
Kim Y, You Y, Yoon HG, Lee YH, Kim K, Lee J, Kim MS, Kim JC, Jun W. Hepatoprotective effects of fermented Curcuma longa L. on carbon tetrachloride-induced oxidative stress in rats. Food Chem. 2014;151:148–53.
Circu ML, Aw TY. Glutathione and modulation of cell apoptosis. Biochim Biophys Acta. 2012;1823(10):1767–77.
Franco R, Cidlowski JA. Apoptosis and glutathione: beyond an antioxidant. Cell Death Differ. 2009;16(10):1303–14.
Authors’ contributions
GHL, HYL, HWC, and MKC made substantial contributions to the conception and design of the study, acquisition of data, and analysis and interpretation of data. SWK was involved in the acquisition of data and participated in designing study. HJC was involved in the conception and design of the study, and revised the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Acknowledgements
This work was supported by the “Food Functionality Evaluation Program” under the Ministry of Agriculture, Food, and Rural Affairs and in part by the Korea Food Research Institute.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article and all datasets supporting our findings are available. A sample of the CLL used in this study has been deposited at the Ottogi company.
Ethics approval and consent to participate
All procedures in the animal studies complied with standards for the care and use of experimental animals and were approved by Animal Care Committee of Chonbuk National University Hospital (IACUC protocol CBU 150608-25).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lee, GH., Lee, HY., Choi, MK. et al. Protective effect of Curcuma longa L. extract on CCl4-induced acute hepatic stress. BMC Res Notes 10, 77 (2017). https://doi.org/10.1186/s13104-017-2409-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13104-017-2409-z