
Abstract
Introduction
Heading is an integral part of football and frequent media reports and previous studies about potential danger of heading and head trauma in football fuelled discussions. Epidemiological data and video analyses regarding headings situation and associated head injuries are still missing in male adult professional football.
Methods
In a prospective cohort study in the male fourth German football league, 100 official matches of the 2015–2016 season were assessed by video analysis and a standardized protocol. Heading situations and concomitant circumstances as well as incidents with a propensity of injury (critical incidents) were analyzed. Critical incidents (CI) and seasonal reported head injuries were cross-referenced.
Results
Overall, 11,514 headings were analysed in detail. Video analysis yielded a mean of 5.7 headings per player and match (SD: 1.2; range 0–15). Heading was predominantly performed with the frontal part of the head (76.8%), and nearly two thirds of all headings occurred during defending (65.8%). 71.0% of all headings occured during tacklings, of which 71.9% involved body contact with the opponent player. Video analysis yielded 31 CI on the head due to heading (incidence: 1.02 per 1000 h match exposure and player). 29 CI occurred during heading duels (odds ratio: 5.91), 30 CI with body contact (odds ratio: 28.8) and 6 CI with elbow contact (odds ratio: 6.13).
Conclusion
Heading frequency in male semi-professional football could be determined with a rate of 5.7 headings per match and field player. Cross referencing CI and seasonal reported head injuries revealed a very low number of reported head injuries.
Similar content being viewed by others


Introduction
Football is a unique type of ball sports that allows its players to use the head for controlling, passing and shooting a ball [1,2,3]. For more than 20 years, there has been a growing discussion about the potential harm of headings for the brain [2, 4,5,6,7,8,9]. This discussion was fueled by the first studies describing several structural and biochemical changes in former football players, even in those without a history of concussion [7, 8, 10, 11], and by the ban on headings for under 13-year old children by the US Soccer Federation (USSF) in 2015. Especially long-term consequences of headings such as neuro-psychological changes are dreaded [10, 12,13,14]. Epidemiological data on headings and its concomitant circumstances as well as caused injuries by heading situations are sparse, therefore most experiences and evident data on long-term structural changes are derived from other contact sports such as ice hockey or American football. The few interventional studies available on headings mostly describe heading sessions of about 10–15 min [15, 16] with estimated rates of 50 to 100 headings per player. However, it is unclear whether the designs of these interventional studies allow an interpretation of the impact of heading in practial football routine. The present study investigated for the first time heading rates per player and match as well as incidents with a propensity of injury in semi-professional mals by using video analysis.
Methods
Study design
In a prospective cohort study, the fourth male German football league, which displays a semi-professional league, were analysed by means of video analysis and injury reports during the 2015–2016 season. Video analysis has been identified as a useful tool for characterising headings in detail and for identifying critical incidents leading to head injuries in football [1, 17]. The investigated fourth male league included 18 teams with professional football players. The Regional Football Association of Bavaria (BFV) provided the television recordings of all 306 matches of the 2015–2016 season for video analysis. The recordings had been filmed by at least one camera fixed to the grandstand of each football stadium. All headings (every head contact or intended or attempted head contact situation with the ball of different players in the match) and incidents with a propensity of injury (critical incident, CI) of the entire season were monitored exploratively by using standardised questionnaires. Seasonal injury reports were obtained by a using a questionnaire and a report handed out to the staff of each of the 18 teams, which allowed an anonymous data collection. Injuries were documented according to previously published injury definitions and data collection standards in football [18, 19].
Video analysis protocol
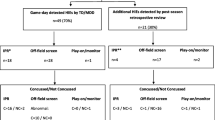
A representative, randomly chosen sample of 100 matches was investigated by video analysis. At first, all videos were reviewed to identify the frequency of headings. Every header was then analysed by means of a standardised video analysis protocol developed prior to the study and used here for the first time (see Fig. 1). In this protocol, 18 characteristics of heading were queried including the duelling situation, the areas of body contact or the elbow position during the heading. Furthermore, the type, distance and angle of the ball to the player were documented as well as the impact surface of the ball on the head and any concomittant jumps or movements of the players. Headings were viewed in slow-motion and freeze-frame in a standardised manner to allow a precise examination of the header. Video analysis was performed by three trained raters. Unclear situations were discussed with the video analyzing team online, which consisted of all raters and two supervisors. Because of differences in distances and position of the video camera in each stadium, distances or angles on the video could not precisely be measured. In such cases, auxiliary quantities such as the size and boundaries of the field, penalty areas or centre circles were used to interpret the different heading situations (Fig. 1).

Heading protocol for analysing heading situations in football
Critical incident assessment and cross-referencing to reported injuries
Additionally, critical incidents (CI) on the football field according to the criteria first published by Anderson et al. [1] and further developed by Bjorneboe et al. [20] were seperately analysed. According to the previously published standard, a CI is a situation in which the player has a risk for conducting an injury. In the present study, the focus was on risky situations on the head. An incident was recorded if the match was interrupted by the referee and if one of the players involved in the tackling was lying on the ground for more than 15 s or had to be carried off. Every head trauma observed on video was assessed by specific items such as the starting situation and its triggers, the contact area on the head and co-injured body areas. Position on field and evaluation by the referees were also documented. Each CI was viewed several times at different slow-motion speeds and freeze-frames. Any uncertain situation was managed as described above. After match completion, each reported CI was cross-referenced with the standardised epidemiological injury investigation over the season, which was conducted prospectively.
Statistics
Critical incident and injury incidence were calculated by the number of injuries devided by hours of match exposure multiplied by 1000. Descriptive data such as injury characteristics are presented as absolute numbers and percentages. Rates of contact injuries between different types of heading situations were compared by chi-square test of independence. Odds ratios with corresponding 95% confidence intervals were calculated as effect estimates. A p value < 0.05 was considered as statistically significant. All analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Heading frequency and distribution
Video analysis yielded 11,514 headings in 9229 match minutes (115.1 headings per match/ standard deviation (SD): 24.4; 1.2 headings per match minute/SD: 0.3, see Table 1). With the exception of goalkeepers, who only performed 7 headings in 100 matches, the mean heading rate per male field player and match was 5.7 (SD: 1.2). While many players had 0 headings in football matches, the highest number of headings per match of one male player was 15. With regard to the position on field, defenders showed the highest percentage of headings (44.1%, 5084 headings) followed by strikers with 12.5% (1435 headings) and midfield players with 35.3% (4019 headings, see Fig. 2). Most headings were performed after high passes (32.0%), goal kicks (18.4%) and previous headings (15.7%). Headings after corners (4.7%), free kicks (8.0%) and crosses (5.0%) were less frequent. In 3.8% (440) of headings the elbow was at or above shoulder-height. The majority of headings was recorded in the midfield area of the football field (5971, 52.8%). The total rate of headings in the penalty area (2364, 20.9%) was lower than in the outer tracks (2973 headings, 26.3%; Fig. 2). About 71% of all headings occurred during tackling, of which 71.9% involved physical contact between the players. Less than 5% of all headings involved body contact with more than one player. About 3% of all headings were judged as a foul by the referee.

Heading frequency in football field areas
Critical incidents due to heading situations
Video analysis identified 45 CIs (0.39%) due to heading (see Table 2). The head was the most affected body area (31 players, 68.9%) followed by the back (6 players, 13.3%) and the ankles (4 players, 8.9%). The CI rate for the head per match and player was 0.0016 (1.02 per 1000 h match exposure and player). The distribution of CIs due to heading regarding the playing positions was similar to that of the heading rates with defenders being the most affected players (15 CI, 48.4%; see Fig. 3). 29 CIs (93.5%) involved a time-out of which 5 (16.1%) resulted in the substitution of the injured player. 29 of 31 CIs (93.5%) occurred in duelling situations, and 30 CIs (96.8%) involved active body contact. 13 of 31 CIs (41.9%) were judged as a foul by the referee, and 4 CIs (13.4%) resulted in a yellow or red card. 30 CI (5.1 Cl per 1000 headings) resulted from 5884 (51.2%) headings with body contact, while 1 CI on the head occurred in 5616 (48.8%) headings without body contact (0.18 Cl per 1000 headings; Odds ratio: 28.8; 95%-CI 4.8, 1174; p < 0.001). 29 CI (3.5 Cl per 1000 headings) occurred in 8178 duelling situations (71.1%), while 2 CI resulted from 3334 non-dueling situations (28.9%) (0.6 Cl per 1000 headings; Odds ratio: 5.91 95%-CI 1.49, 51.15, p = 0.006). 6 CI (13.7 Cl per 1000 headings) were observed in 438 (3.8%) situations with elbow on or over shoulder height occurred, while 25 CI occurred in 11,055 (96.2%) headings without lifted elbow (2.3 Cl per 1000 headings; Odds ratio: 6.13; 95%-CI 2.04, 15.40; p < 0.001).

Heading (above) and critical incident frequency (below) in playing positions
Cross-referencing of critical incidents with seasonal injury reports
When cross-referencing the CIs with seasonal injury reports of head injuries, only 4 head injuries had been reported by the teams in the 100 investigated matches. 1 nasal fracture, 1 skin laceration and 2 concussions were diagnosed resulting in a concussion rate after heading of 0.017% and a concussion incidence of 0.065 per 1000 match hours and player.
Discussion
In the so far largest cohort study on video analysis of heading in male football, this study provides detailled information on the incidence and circumstances of headings in semi-professional football. One important finding of this study was the quantification of heading per player and match with a mean of 5.7 or a maximum of 15 for one player during the match. The impact of heading on neurological or neuropsychological symptoms was previously published in experimental studies with significantly higher heading frequencies per intervention [11, 21,22,23,24] than in this study yielding a need for a discussion on how the previous data is applicable to real game situations. The importance of this topic for sports medicine has been documented in several studies over the past few years and the increasing interest in the results of the international conference on concussion in sports. Previously published study results have indicated that heading in football may be dangerous for the brain, changing its microstructure and neurochemistry and effecting neurocognitive changes [7, 8, 10, 11, 25,26,27]. Additionally, the ban on heading for under 13-year olds by the US Soccer Federation (USSF) in 2015 has given a further impetus to the ongoing discussion about the harmfulness of heading, in particular because scientific evidence on the danger of heading in football is still lacking.
Epidemiological classification
So far, epidemiological data on heading and head injuries in football are scarce [5, 6]. Detailed video analyses of headings and situations for a propensity for injuries are rare, although such analyses are a commonly used analytical method for characterising specific situations in sports matches [1, 17, 28,29,30,31,32,33]. Several studies have concluded that traumatic brain injuries due to head trauma, especially when incurred several times within a short period of about 2–4 weeks, are a major risk factor for changes in the brain [34,35,36]. As this investigation showed, injuries to the head resulting from heading are rather rare in football compared to common injuries predominately affecting thighs, knees and ankle [18, 37, 38]. Head injuries, which also include midfacial lesions and fractures, account for 5–20% of all reported injuries and have been recently considered an underrepresented problem in sports [39]. The total number of sports-related concussion is still often overlooked, in part because of the non-apparent clinical signs that are only revealed by a clinical examination that occasionally medical doctors are not proficient in. Especially at lower skills levels and in junior football there might not even be a medical team available to carry out such an examination [39]. This situation defines the urgent need for improved and sufficent injury prevention steps for head injuries of football players.
Approach to prevention of head injuries
One other important finding of this study is that CIs on the head and propably head injuries directly result from heading duels, body contacts and high elbow-positioning. Head injuries are known to often occur during tackling, so that different strategies for preventing head injuries have been developed over the past few years [40, 41]. Rule modifications like the advice to ban a player for intentional elbow-to-head contact, have significantly reduced the rate of head injury [1, 3]. However, further strategies should be considered in connection with the results of this study, such as education in fair play in heading duels, avoiding fouls during tackling and training in correct heading techniques [39]. Above all, football players need to be informed about the possible consequences of head injuries to reduce their willigness of risking a contact between their head with the body of other players. Such education of football players may be an important factor for preventing head injuries in heading duels [42, 43].
With a rate of critical incidents and concussions in this study, the risk of sustaining a concussion in football is much lower than in other male sports such as Australian football, American Football or Ice hockey [31, 44]. Nevertheless, the total number of head injuries in male football worldwide is substantial because of the high number of football players, since football is the most important sport worldwide. It is essential to reduce the number of head injuries and to eliminate the uncertainty of football players on this topic. Besides injury prevention of head injuries, both football players and staff should be further educated about the incidence, diagnostics, symptoms and first aid on field [43, 45]. The problem of late diagnosis or overlooked concussion [39] is still a problem in all team sports and should also be improved in football.
One other important result of this study is the low concussion rate of the injury statistics provided by the teams compared to the rate of CIs on the head documented by means of video analysis. According to the definition of a CI, only 2 concussions in 31 CIs to the head were verified in our video analysis. This situation may illustrate that either there is an overcasting for minor head injuries in video analysis or that these minor head impacts are not gaining enough attention of the football players or other staff on field. Potentially overlooked minor head injuries may not be worked up properly (for example by a detailed (neurological) examination) and may not receive sufficent treatment with adequate further clinical diagnostic work up or rest, so that players are at risk of sustaining recurrent hits on the head in further heading duels [45].
Limitations
This study also has some limitations. At first, all study findings were obtained in male football, so that all observations and conclusions can only be compared or transferred to male sports.
Further on, in the fourth male football league, television recordings were often only obtained by 1 video camera per match and football field. Evaluating heading and situations with a risk for head injuries may therefore be different to football matches in professional football, in which football matches are continuously recorded by several cameras in different positions. Additionally, the transfer of our study results to other football subpopulations is somewhat limited. Professional players may even have better tackling abilities in headings duels than amateur or junior players. The different constitution of football players, especially of women and junior players, influence heading situations as well as the aetiology of injuries. The incidence of heading, CIs and head trauma of football players is generally assessed by match and training exposure, whereas this study only included match exposure. Competitions as well as official matches are assumed to be associated with higher injury rates than training sessions [46].
Conclusion
The biggest so-far analysis of headings in male semi-proferssional football revealed a mean heading rate of 5.7 per field player and match, which seems to be a lower number than previously estimated in the literature. Analyzation of situations with a propensity for injuries showed that these situations occurred more often after body contact and high elbow positioning, even if cross-referencing with season injury rates only showed low injury and concussion rates. Future research is necessary to investigate heading rates in other subpopulations and, especially, head trauma caused by heading in a larger number.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request, except insurance data which is property of the insurance itself.
Abbreviations
- BFV:
-
Bayrischer Fußball Verband (Bavarian Football Association)
- CI:
-
Critical incident
- SD:
-
Standard deviation
- USSF:
-
United States Soccer Federation
- VBG:
-
Verwaltungsberufsgenossenschaft (General Insurance in Professional Sports)
References
Andersen TE, Arnason A, Engebretsen L, Bahr R. Mechanisms of head injuries in elite football. Br J Sport Med. 2004;38(6):690–6. https://doi.org/10.1136/bjsm.2003.009357.
Barnes BC, Cooper L, Kirkendall DT, Mcdermott TP, Jordan BD, Garrett WE. Concussion History in Elite Male and Female Soccer Players. 1998;26(3):433–8.
Beaudouin F, Aus der Fünten K, Trü T, Reinsberger C, Meyer T. Head injuries in professional male football (soccer ) over 13 years : 29% lower incidence rates after a rule change (red card ). Br J Sport Med. 2017. https://doi.org/10.1136/bjsports-2016-097217
Mackay DF, Russell ER, Stewart K, et al. Neurodegenerative disease mortality among former professional soccer players. N Engl J Med. 2019;381(19):1801–8. https://doi.org/10.1056/NEJMoa1908483.
Kontos AP, Braithwaite R, Chrisman SPD, et al. Meta-analytical review of the effects of football heading. BJSM. 2016. https://doi.org/10.1136/bjsports-2016-096276.
Kontos AP, Dolese A, Elbin RJ, Covassin T, Warren BL. Relationship of soccer heading to computerized neurocognitive performance and symptoms among female and male youth soccer players. Brain Inj. 2011;25:1234–41. https://doi.org/10.3109/02699052.2011.608209.
Koerte IK, Ertl-Wagner B, M R, Zafonte R, Shenton M. White matter integrity in the brains of professional soccer players without a symptomatic concussion. JAMA. 2014;308(18):1859–1861. https://doi.org/10.1093/ageing/afp226.
Koerte IK, Mayinger M, Muehlmann M, et al. Cortical thinning in former professional soccer players. Brain Imaging Behav. 2016;10:792–8. https://doi.org/10.1007/s11682-015-9442-0.
Stephens R, Rutherford A, Potter D, Fernie G. Neuropsychological consequence of soccer play in adolscent U.K. School Team Soccer Players. J Neuropsychiatry Clin Neurosci. 2012;22(3):295–303.
Koerte IK, Lin AP, Muehlmann M, et al. Altered neurochemistry in former professional soccer players without a history of concussion. J Neurotrauma. 2015;32:1287–93. https://doi.org/10.1089/neu.2014.3715.
Haran FJ, Thierney R, Wright WG, Keshner E, Silter M. Acute changes in postural control after soccer heading. Int J Sport Med. 2013;34:350–4. https://doi.org/10.1136/bjsm.2003.004887.
Helmich I, Berger A, Lausberg H. Neural control of posture in individuals with persisting postconcussion symptoms. Med Sci Sports Exerc. 2016;48(12):2362–9. https://doi.org/10.1249/MSS.0000000000001028.
Moser RS, Iverson GL, Echemendia RJ, et al. Neuropsychological evaluation in the diagnosis and management of sports-related concussion. Arch Clin Neuropsychol. 2007;22(8):909–16. https://doi.org/10.1016/j.acn.2007.09.004.
Maher ME, Hutchison M, Cusimano M, Comper P, Schweizer TA. Concussions and heading in soccer: a review of the evidence of incidence, mechanisms, biomarkers and neurocognitive outcomes. Brain Inj. 2014;28(3):271–85. https://doi.org/10.3109/02699052.2013.865269.
Rieder C, Jansen P. No neuropsychological consequence in male and female soccer players after a short heading training. Arch Clin Neuropsych. 2011;26:583–5.
Putukian M, Echemendia RJ, Mackin S. The acute neuropsychocological effects of heading in soccer: A Pilot Study. Clin J Sport Med. 2000;10(2):104–9.
Tucker R, Raftery M, Fuller GW, Hester B, Kemp S, Cross MJ. A video analysis of head injuries satisfying the criteria for a head injury assessment in professional Rugby Union: a prospective cohort study. Br J Sport Med. 2017;51:1147–51. https://doi.org/10.1136/bjsports-2017-097883.
Hägglund M, Waldén M, Bahr R, Ekstrand J. Methods for epidemiological study of injuries to professional football players: developing the UEFA model. Br J Sport Med. 2004;39(6):340–6.
Fuller C, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer). Clin J Sport Med. 2006;16(2):97–106. https://doi.org/10.1136/bjsm.2005.025270.
Bjørneboe J, Bahr R, Andersen TE. Video analysis of situations with a high-risk for injury in Norwegian male professional football; a comparison between 2000 and 2010. Br J Sport Med. 2014;48:774–8. https://doi.org/10.1136/bjsports-2012-091856.
Rieder C, Jansen P. No neuropsychological consequence in male and female soccer players after a short heading training. Arch Clin Neuropsychol. 2011;26(7):583–91. https://doi.org/10.1093/arclin/acr055.
Putukian M, Echemendia RJ, Mackin S. The acute neuropsychological effects of heading in soccer: A Pilot Study. Clin J Sport Med. 2000;10(2):104–9. https://doi.org/10.1097/00042752-200004000-00004.
Straume-Naesheim TM, Andersen TE, Dvorak J, Bahr R. Effects of heading exposure and previous concussions on neuropsychological performance among Norwegian elite footballers. Br J Sport Med. 2005;39(Suppl I):i70–7. https://doi.org/10.1136/bjsm.2005.019646.
Jansen P, Lehmann J. Investigating cognitive performance deficits in male and female soccer players after a 4-week heading-training programme: a controlled study. Brain Impairment. 2017;4:1–8. https://doi.org/10.1017/BrImp.2017.4.
Allen B, Karceski S. Soccer and head injuries- What is the risk? Neurology. 2017;88(February):e74–7.
Di Virgilio TG, Hunter A, Wilson L, et al. Evidence for acute electrophysiological and cognitive changes following routine soccer heading. EBioMedicine. 2016;13:66–71. https://doi.org/10.1016/j.ebiom.2016.10.029.
Lipton M, Kim N, Zimmerman M, et al. Soccer heading is associated with white matter microstructural and cognitive abnormalities. Radiology. 2013;268(3):850–7. https://doi.org/10.1148/radiol.13130545.
Burger N, Lambert MI, Viljoen W, Brown JC, Readhead C, Hendricks S. Tackle technique and tackle-related injuries in high-level South African Rugby Union under-18 players: real-match video analysis. Br J Sport Med. 2016;50:932–8. https://doi.org/10.1136/bjsports-2015-095295.
Gardner A, Kohler R, Levi C, Iverson G. Usefulness of video review of possible concussions in National Youth Rugby League. Int J Sport Med. 2017;38:71–5.
Makdissi M, Davis G. The reliability and validity of video analysis for the assessment of the clinical signs of concussion in Australian football. J Sci Med Sport. 2016;19(10):859–63.
Makdissi M, Davis G. Using video analysis for concussion surveillance in Australian football. J Sci Med Sport. 2016;19(12):958–63. https://doi.org/10.1016/j.jsams.2016.02.014.
Tucker R, Raftery M, Kemp S, et al. Risk factors for head injury events in professional rugby union: a video analysis of 464 head injury events to inform proposed injury prevention strategies. Br J Sport Med Med. 2017;51:1152–7. https://doi.org/10.1136/bjsports-2017-097895.
Waldén M, Krosshaug T, Bjørneboe J, Andersen TE, Faul O, Hägglund M. Three distinct mechanisms predominate in non- contact anterior cruciate ligament injuries in male professional football players : a systematic video analysis of 39 cases. Br J Sport Med. 2015;49:1452–60. https://doi.org/10.1136/bjsports-2014-094573.
Cantu R. Second-impact syndrome. Clin Sport Med. 1998;17(1):37–44.
Matser EJT, Lezak MD, Jordan BD, Traumatic H, In B. Neuropsychological impairment in amateur soccer players. JAMA. 1999;282(10):971–3.
Vagnozzi R, Signoretti S, Tavazzi B, et al. Hypothesis of the postconcussive vulnerable brain: experimental evidence of its metabolic occurrence. Neurosurgery. 2005;57(1):164–71. https://doi.org/10.1227/01.NEU.0000163413.90259.85.
Krutsch W, Zeman F, Zellner J, Pfeifer C, Nerlich M, Angele P. Increase in ACL and PCL injuries after implementation of a new professional football league. Knee Surg Sport Traumatol Arthrosc. 2014. https://doi.org/10.1007/s00167-014-3357-y.
Koch M, Zellner J, Berner A, et al. Influence of preparation and football skill level on injury incidence during an amateur football tournament. Arch Orthop Trauma Surg. 2016;136(3):353–60.
Krutsch V, Gesslein M, Loose O, et al. Injury mechanism of midfacial fractures in football causes in over 40% typical neurological symptoms of minor brain injuries. Knee Surg Sport Traumatol Arthrosc. 2017. https://doi.org/10.1007/s00167-017-4431-z.
Klügl M, I S, McBain K, et al. The prevention of sport injury: an analysis of 12,000 published manuscripts. Clin J Sport Med. 2010;20(6):407–4012. https://doi.org/10.1097/JSM.0b013e3181f4a99c.The.
Krutsch V, Krutsch W, Jansen P, et al. Prevention of head and brain injuries in football: Is there a need to ban headings? Sport Sport. 2017;31(3):143–53.
Myrdal CN, Huang S, Beach HN, Waterbrook AL. Comparison of knowledge, perception and attitudes of concussion in previously concussed versus non-concussed youth soccer players. Phys Sportsmed. 2017;45(3):286–92. https://doi.org/10.1080/00913847.2017.1345569.
Kurowski BG, Pomerantz WJ, Schaiper C, et al. Impact of preseason concussion education on knwledge, attitudes, and behaviors of high school athletes. J Trauma Acute Care Surg. 2015;79(3 Suppl 1):S21-28. https://doi.org/10.1097/TA.0000000000000675.
Ruhe A, Gänsslen A, Klein W. The incidence of concussion in professional and collegiate ice hockey: are we making progress? A systematic review of the literature. Br J Sports Med. 2014;48(2):102–11.
Haran HP, Bressan S, Oakley E, et al. On-field management and return-to-play in sports-related concussion in children: Are children managed appropriately? J Sci Med Sport. 2016;19(3):194–9. https://doi.org/10.1016/j.jsams.2015.09.009.
Agel J, Evans Ta, Dick R, Putukian M, Marshall SW. Descriptive Epidemiology of Collegiate Men’s Soccer Injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 Through 2002–2003. J Athl Train. 2007;42(2):270–7. https://doi.org/10.1016/S0276-1092(08)79204-6.
Acknowledgements
Special thanks to the Bavarian Football Association (Bayerischer Fußball Verband, BFV) for providing video material of the fourth German football league. Additionally, we want to thank Christian Klein, Patrick Luig and Hendrik Bloch from the German Public Trauma Insurance for Elite Athletes (VBG) for the exchange and support in preparing the detailed and sport-specific study protocol for video analysis. Many thanks also to the Centre of Clinical Studies at the University Medical Centre Regensburg.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors have no relevant financial or non-financial interests to disclose.
Author information
Authors and Affiliations
Contributions
JW and WK writing, conceptualization, AE and WK and JW analysis, DP, VA, MN and CR acquisition and interpretation of data, substantial revision. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the University of Regensburg (no. 15-101-0134). According to national regulations, an informed consent to participate was not necessary.
Informed consent
Not necessary, as study was performed on video material in which no patient-specific data was obtained.
Competing interest
All the authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Weber, J., Ernstberger, A., Reinsberger, C. et al. Video analysis of 100 matches in male semi-professional football reveals a heading rate of 5.7 headings per field player and match. BMC Sports Sci Med Rehabil 14, 132 (2022). https://doi.org/10.1186/s13102-022-00521-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-022-00521-2