
Abstract
Background
Measurement of estimated glucose disposal rate (eGDR) has been demonstrated to be an indicator of insulin resistance (IR) and a risk sign for long-term outcomes in those with ischemic heart disease and type 2 diabetes mellitus (T2DM) having coronary artery bypass grafting (CABG). After elective percutaneous coronary intervention (PCI), the usefulness of eGDR for prognosis in those with non-ST-segment elevation acute coronary syndrome (NSTE-ACS) and non-diabetes is yet unknown.
Methods
1510 NSTE-ACS patients with non-diabetes who underwent elective PCI in 2015 (Beijing Anzhen Hospital) were included in this study. Major adverse cardio-cerebral events (MACCEs), such as all-cause mortality, non-fatal myocardial infarction, non-fatal ischemic stroke, and also ischemia-driven revascularization, were the main outcome of follow-up. The average number of follow-up months was 41.84.
Results
After multivariate Cox regression tests with confounder adjustment, the occurrence of MACCE in the lower eGDR cluster was considerably higher than in the higher eGDR cluster, demonstrating that eGDR is an independent prognostic indicator of MACCEs. In particular, as continuous variate: hazard ratio (HR) of 1.337, 95% confidence interval (CI) of 1.201–1.488, P < 0.001. eGDR improves the predictive power of usual cardiovascular risk factors for the primary endpoint. Specifically, the results for the area under the receiver operating characteristic (ROC) curve, this is AUC, were: baseline model + eGDR 0.699 vs. baseline model 0.588; P for contrast < 0.001; continuous net reclassification improvement (continuous-NRI) = 0.089, P < 0.001; and integrated discrimination improvement (IDI) = 0.017, P < 0.001.
Conclusion
Low eGDR levels showed a strong correlation with poor NSTE-ACS prognosis for nondiabetic patients undergoing PCI.
Similar content being viewed by others


Introduction
In recent years, with the widespread application of optimized drug therapy and the improvement of interventional strategies such as revascularization, patients’ prognosis with cardiovascular disease (CVD) has been significantly improved. However, patients with CVD still have a high risk of recurrent cardiovascular events [1,2,3,4]. Therefore, identifying remaining risk factors in patients with CVD and expanding new treatment targets are of significant clinical importance. The incidence of CVD and its poor prognosis are strongly predicted by insulin resistance (IR), according to numerous prior investigations [5,6,7]. It is notable that IR has an equal impact on how CVD develops in those who do not have diabetes [8, 9]. Using the homeostasis model assessment of insulin resistance (HOMA-IR), a meta-analysis of 65 trials with 516,325 individuals revealed that the possibility of coronary heart disease increased by 46% in the non-diabetic for every 1 standard deviation increase in IR [10]. Although the hyperinsulinemic–euglycemic (HIEG) clamp is thought as the most accurate method for detecting IR, clinical researchers are more likely to search for IR assessment methods with broader applicability scenarios due to its complex and invasive characteristics. The estimated glucose disposal rate (eGDR) is an alternative to the HIEG clamp to assess insulin responsiveness when undergoing type 1 diabetes mellitus (T1DM) [11]. Calculation of eGDR is based on waist circumference (WC), hypertension, and glycosylated hemoglobin (HbA1c) [11, 12], which are widely recognized as risk elements for CVD and are readily available from clinical data. The IR level increases when eGDR decreases. Low eGDR has been connected to a higher long-term danger of all-cause death in people with type 2 diabetes mellitus (T2DM) following coronary artery bypass grafting (CABG), suggesting that eGDR may efficaciously indicate poor projection in T2DM patients with ischemic heart disease after revascularization [13]. Considering the economic and efficient characteristics of eGDR, it is suitable to be popularized as a routine screening method for CVD high-risk groups. Thus, we aimed to investigate the connection between eGDR and long-term outlook for CVD nondiabetic patients. We explored the prognostic worth of eGDR in subjects that did not have diabetes but were undergoing non-ST-segment elevation acute coronary syndrome (NSTE-ACS) and had experienced percutaneous coronary intervention (PCI).
Materials and methods
Study subjects
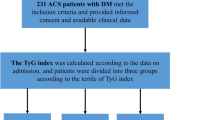
This was a single-center study with an observational cohort. Enrolled subjects had a diagnosis of NSTE-ACS (Beijing Anzhen Hospital, 2015) and underwent elective PCI. Patients with previously or newly diagnosed diabetes at admission were excluded. The diagnostic principles for NSTE-ACS [which involved unstable angina (UA) and non-ST-segment elevation myocardial infarction (NSTEMI)] and diabetes followed the authority’s guidelines [14, 15]. Figure 1 depicts further exclusion requirements. Finally, 1510 patients were enrolled for this investigation.

Flow diagram for the enrollment of study population. NSTE-ACS Non-ST-segment elevation acute coronary syndrome, PCI Percutaneous coronary intervention, CABG Coronary artery bypass grafting, eGFR estimated glomerular filtration rate, eGDR estimated glucose disposal rate
Data gathering and descriptions
The baseline facts attained in this study, including demographic data, patient features, laboratory examinations, imaging data, PCI-related data, and medication information, were quality-controlled by the hospital information center. After several measurements taken on various days, hypertension was determined to entail systolic blood pressure (SBP) of over 140 mmHg and/or diastolic blood pressure (DBP) of values below 90 mmHg [16]. Following current recommendations, the diagnostic standards for peripheral arterial disease (PAD), stroke, and dyslipidemia were also employed [17,18,19]. The WC was the width of the line separating the iliac crest's upper border from the nethermost part of the rib. On the operation day’s morning, blood for hematological and bio-chemical analyses was collected from patients who had fasted for 8–12 h. High-performance liquid chromatography served as a detection method for HbA1c. Two qualified professionals assessed the outcomes of the PCI and echocardiography tests, respectively. Coronary intervention procedures were performed according to the most recent recommendations [20,21,22]. Using the standard formula found in https://syntaxscore.org, the Synergy between percutaneous coronary intervention with taxus and cardiac surgery (SYNTAX) scores was computed. The severity of coronary lesions was also assessed by the Gensini score [23]. The calculation of eGDR was conducted as [11, 12, 24]: eGDR = 21.16−(0.09*WC [in cm])−(3.41*Hypertension [affirmative or negative])−(0.55*HbA1c [in %]).
Follow-up and research endpoint
The monitoring period entailed 48 months after hospital release or until the patient died (average monitoring time: 41.84 months). The primary end point was major adverse cardio-cerebral events (MACCEs), counting all-cause mortality, non-fatal myocardial infarction (MI), non-fatal ischemic stroke, and ischemia-driven revascularization. MI shows that the level of creatine kinase or heart troponin is higher than the superior limit in the reference range, and electrocardiogram (ECG) results and/or ischemic factors indicate ischemia in the myocardium. Using magnetic resonance images (MRI) or computed tomography (CT), ischemic lesions that induce nerve injury are what define a stroke. Revascularization of vessels of target and/or non-target nature reveals ischemia-induced revascularization as a result of recurrent or insistent ischemic signs, such as CABG and PCI.
Statistical evaluation
Included participants were divided into two groups regarding their median eGDR, this is lower eGDR: eGDR ≤ 7.76, and higher eGDR: eGDR > 7.76. The mean standard deviation of continuous variables with normal distribution is displayed and contrasted by a two independent t-test. In the case of the Mann–Whitney U test, it compares continuous variables with skew distributions represented by the median, 25th, and 75th percentiles. Nominal variables were expressed as numbers and percentages, and then contrasted by chi square, continuity-corrected chi square, or using the Fisher's exact.
The Kaplan–Meier curve employed described the growing amounts of the primary endpoint events under diverse eGDR levels, and a log-rank test allowed comparison. Variables that probably had collinearity were eliminated from the 4 multivariate models, which included contained potential risk factors for MACCE that were initially identified in univariate Cox regression analysis. Nominal and continuous variables, respectively, were used to evaluate eGDR. Correlations involved hazard ratios (HR) and 95% confidence intervals (CI). In particular, the multivariate Cox regression models were as follows: in Model 1, adjustments comprised age, sex, body mass index (BMI); Model 2 as Model 1 plus previous MI, previous PCI, previous stroke, smoking history and family history of coronary artery disease (CAD); Model 3 adjusted as Model 2 plus triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), estimated glomerular filtration rate (eGFR), high-sensitivity C-reactive protein (hs-CRP), angiotensin-converting enzyme inhibitor (ACEI)/angiotensin receptor blocker (ARB) at admission, and left ventricular ejection fraction (LVEF); Model 4 adjusted as Model 3 plus left main artery (LM) lesion, bifurcation, SYNTAX score, multi-vessel lesion, in-stent restenosis, chronic total occlusion lesion, complete revascularization, number of drug-eluting stent (DES), and treatments for: LM, left anterior descending artery (LAD), left circumflex artery (LCX), and right coronary artery (RCA).
In agreement with model 4, a restricted cubic spline curve represents the dose–response connection of eGDR and the primary endpoint. Nonlinear hypotheses are tested using a likelihood ratio analysis. Stratified scrutiny adjusted for model 4 variables considered sex, age, BMI, hyperlipidemia, family history of CAD, smoking history, diagnosis, ACEI/ARB at admittance, and statins at admittance to define the consistency of eGDR in MACCEs prediction. To evaluate eGDR's ability to predict MACCEs, the area under the receiver operating characteristic (ROC) curve, this is, AUC, was obtained. Integrated discrimination improvement (IDI) plus continuous net reclassification improvement (continuous-NRI) confirmed the progressive influence of eGDR introduction on the prognostic competency of presently recognized risk models.
Data examination was performed using SPSS v26.0 and R3.6.3. Statistical significance was acknowledged when two-tailed P < 0.05 was obtained.
Results
Patient characterization at the starting point
This study comprised 1510 individuals (mean age = 59.67 ± 9.27) with a 73.7% male participation rate (n = 1113). Age, BMI, WC, SBP, DBP, TG, hs-CRP, HbA1c, FBG, uric acid, creatinine, incidence of hypertension and prior stroke were all higher in the lower eGDR cluster when contrasted to the higher eGDR cluster, whereas HDL-C and eGFR were lower. Patients with lower eGDRs received more ACEI/ARB and β-blocker prescriptions for admission and discharge medication. Participants with low eGDR presented a higher multi-vessel lesions rate and target vessels of LCX and RCA treated, an inferior percentage of complete revascularization, and increased DES implanted. Additionally, the lower eGDR group's SYNTAX score was higher than the higher eGDR group’s (Table 1). A representative case of the extent of coronary artery disease is shown in Additional file 1: Figure S1.
Incidence of MACCE
A total of 316 patients (20.9%) experienced MACCE throughout the course of the 48-month follow-up period, including 205 (13.6%) cases of ischemia-induced revascularization, 65 (4.3%) non-fatal myocardial infarctions, 27 (1.8%) non-fatal ischemic strokes, and 19 (1.3%) all-cause mortality. The lower eGDR group had significantly greater incidences of MACCEs (P < 0.001), non-fatal ischemic stroke (P = 0.011), and revascularization due to ischemia (P < 0.001) than the higher eGDR group. Nevertheless, no statistically significant difference was found when the two groups were contrasted in the proportion of all-cause mortality and non-fatal MI (Table 2).
MACCE cumulative risk during follow-up
The time-subject cumulative occurrence of MACCE and its components in the two clusters were evaluated using the Kaplan–Meier method. Lower eGDR had a greater cumulative incidence of MACCE (Fig. 2A, log-rank P < 0.001), non-fatal ischemic stroke (Fig. 2D, log-rank was P = 0.011), and ischemia-driven revascularization (Fig. 2E, log-rank was P < 0.001). The cumulative incidence of all-cause mortality (Fig. 2B, log-rank was P = 0.814) and non-fatal MI (Fig. 2C, log-rank was P = 0.383) had no statistical variance between the two clusters.

Kaplan–Meier survival curves according to the median of eGDR. A Kaplan–Meier survival curve of MACCE; B Kaplan–Meier survival curve of all-cause death; C Kaplan–Meier survival curve of non-fatal MI; D Kaplan–Meier survival curve of non-fatal ischemic stroke; E Kaplan–Meier survival curve of ischemia-driven revascularization. eGDR estimated glucose disposal rate, MACCE major adverse cardio-cerebral events, MI myocardial infarction, PCI percutaneous coronary intervention
Prognostic worth of eGDR for MACCE
To evaluate the eGDR’s ability to predict the primary endpoint, four multivariate models were built (as shown in Methods). Additional file 1: Table S1 summarizes the test of univariate Cox proportional hazards that originally identified predictors of MACCE. After adjusting the variables in the four models, whether eGDR is regarded as a variable either nominal or continuous, it shows substantial independent predictive worth in all models (see Table 3). eGDR was found to be strongly correlated with the possibility of revascularization due to ischemia as a nominal variable and with the possibility of non-fatal MI and revascularization due to ischemia as a continuous variable in the study's further examination of the impact of eGDR in terms of prognosis on each constituent of MACCE (Table 4).
Dose–response association of eGDR with MACCE
A restricted cubic spline curve showed the dose response relationship between eGDR and MACCE (Fig. 3). It was found that the risk of MACCE decreased with the surge of eGDR (P < 0.001). This suggested that eGDR was linearly correlated with the risk of MACCE. A non-linear correlation analysis (P < 0.001) confirmed the above results.

Restricted cubic smoothing for the risk of MACCE according to the eGDR. The analysis was adjusted for Model 4. HR was evaluated by per 1-unit increase of eGDR. eGDR estimated glucose disposal rate, MACCE major adverse cardio-cerebral events, CI confidence interval
Stratified analysis of eGDR
Stratified analysis revealed no difference in the eGDR predictive performance for MACCE considering age (< 65 or ≥ 65 years), sex (male/female), hyperlipidemia (no/yes), smoking history (no/yes), family history of CAD (no/yes), diagnosis (UA or NSTEMI), ACEI/ARB at admittance (on/yes) and statins at admittance (no/yes) (for all, P for interaction > 0.05). More importantly, the eGDR predictive value seemed higher in patients with a higher BMI level [HR (95%CI) BMI < 28 kg/m2 1.267 (1.133–1.417) vs. BMI ≥ 28 kg/m2 1.542 (1.277–1.862), P for interaction = 0.030] (Fig. 4).

Subgroup analysis evaluating the robustness of eGDR in predicting the risk of the MACCE. The analysis was adjusted for Model 4 except for variates applied for grouping. HR was evaluated by per 1-unit decrease of eGDR. eGDR estimated glucose disposal rate, MACCE major adverse cardio-cerebral events, HR hazard ratio, CI confidence interval, BMI body mass index, CAD coronary artery disease, UA unstable angina, NSTEMI non-ST-segment elevation myocardial infarction, ACEI angiotensin-converting enzyme inhibitor, ARB angiotensin receptor blocker
eGDR enhances the prognostic capacities of further parameters in MACCE
On the basis of currently acknowledged cardiovascular risk factors, a baseline model was created (including age, sex, BMI, previous stroke, MI, or PCI, hyperlipidemia, family history of CAD, smoking history, LVEF, SYNTAX score, eGFR, complete revascularization). Adding eGDR significantly enhances the prediction ability of the starting-point model for MACCE (AUCs: baseline model + eGDR 0.699 vs. baseline model 0.588; P for contrast < 0.001) (Table 5; Fig. 5). After adding eGDR, the re-categorizing and discrimination aptitudes considerably outperformed the starting-point risk model (continuous-NRI = 0.089, P < 0.001, IDI = 0.017, P < 0.001) (Table 5).

ROC curve to assess the predictive value of eGDR for MACCE. The baseline risk model includes age, sex, BMI, previous MI, previous PCI, previous stroke, hyperlipidemia, smoking history, family history of CAD, eGFR, LVEF, SYNTAX score, complete revascularization. ROC receiver-operating characteristic, eGFR estimated glomerular filtration rate, MACCE major adverse cardio-cerebral events, AUC area under curve
Discussion
The predictive value of eGDR for unfortunate prognosis in those with NSTE-ACS but no diabetes following PCI is being assessed for the first time in this study. Studies have shown an increment in the incidence frequency of MACCEs in those with low eGDR levels. The decline in eGDR is still a relevant independent forecaster of poor prognosis in the evaluated subjects even after adjusting confounding variables. The ability of baseline models comprising traditional risk factors to forecast the possibility of unfortunate prognosis was greatly enhanced by eGDR.
The development of atherosclerosis in non-diabetic patients was highly correlated with IR evaluated by the gold standard for diagnosing IR, the HIEG clamp [25]. Since HIEG cannot be extensively employed, studies on the relationship between IR and CVD progression and prognosis mostly use HOMA-IR to evaluate IR [8, 9]. HOMA-IR assessment of IR requires the detection of fasting insulin levels in patients. Even diabetic patients who were hospitalized for PCI in the cardiovascular department do not routinely have their fasting insulin levels checked in clinical practice. Moreover, the accuracy of insulin measurement methods is difficult to ensure consistently across laboratories, especially when insulin levels are low. Several investigations have found a slight correlation between HOMA-IR and the level of IR in healthy individuals [26, 27]. As a result, clinical practice is more likely to adopt more operable alternative assessment indicators to assess each patient's level of IR in non-diabetic patients. Studies revealed that IR is frequently characterized by elevated fasting glucose, elevated TG, and obesity in addition to elevated fasting insulin levels (especially increased visceral fat) [28]. Based on these factors, a selection of less complex alternative indicators of IR have been proposed by researchers, such as TG/HDL-C, triglyceride-glucose (TyG) index, visceral adiposity index (VAI), etc., and have been confirmed to be significantly correlated with HIEG clamp [29,30,31]. Subsequent studies have established that the development and prognosis of diabetes and cardiovascular disease are closely associated to these simple surrogate assessment indicators of IR [32,33,34]. Studies have indicated that excessive TG/HDL-C levels and the TyG index are independently related to a greater risk of coronary heart disease in non-diabetic patients, while this correlation is not significant in diabetic patients [35]. Compared to the HIEG clamp, eGDR was shown to have similar accuracy. The simplicity of eGDR calculation makes it suitable for large-scale clinical applications. When using as a simple surrogate for assessing IR, eGDR proved a significant correlation with an increased possibility of CVD in T1DM patients [36, 37]. Minor eGDR is associated with an increased possibility of stroke and death in T2DM patients, indicating that eGDR may behave as a predictive marker for these outcomes [38]. Therefore, eGDR is speculated to have good performance in predicting long-standing poor forecast after PCI.
Our study shows that low eGDR is a strong and stable predictor of poor prognosis after PCI in NSTE-ACS and non-diabetic populations. The findings in this study are consistent with previous related studies. Analyzing our findings in terms of pathophysiological mechanisms, as a potent growth factor, the compensatory increase of insulin in the state of IR stimulates the growth, proliferation, and differentiation of vascular smooth muscle cells and activates inflammatory pathways [39]. IR can cause vascular endothelial dysfunction by affecting the activation of nitric oxide, which may be the most important mechanism that causes cardiovascular disease at the cellular level [39, 40]. Therefore, as a simple surrogate index for IR assessment, eGDR can predict the prognosis of patients with cardiovascular disease to a certain extent. On the other hand, eGDR holds three elements: HbA1c, hypertension, and WC. As a recognized traditional risk factor for CVD, hypertension is the most essential constituent of eGDR [11]. In CVD patients with or without diabetes, HbA1c is thought as an independent forecaster of poor outcomes following PCI [41, 42]. Obesity is not only highly correlated with IR [28], but also with maladies such dyslipidemia, CVD, hypertension, and stroke [43]. In patients undergoing PCI, WC is connected with an augmented possibility of cardiac death and non-lethal MI [44]. The release of various cytokines from visceral adipose tissue can lead to inflammation and thrombosis, induce endothelial dysfunction, and accelerate the atherosclerotic process [45, 46]. In the Kaplan–Meier analysis, the differences between the two groups were not statistically significant in all-cause death and non-fatal MI. Because, in this study, patients were predominantly with UA, resulting in a low incidence of adverse events and potentially leading to bias. In addition, it may also be because eGDR is difficult to reflect relatively severe poor prognosis. Notably, in the subgroup analysis, eGDR presented greater predictive worth in the high BMI subcategory (BMI ≥ 28 kg/m2) versus the low BMI subgroup (BMI < 28 kg/m2). Earlier studies have shown that obesity can cause and exacerbate IR [47]. At the same time, obesity is also a recognized traditional risk factor for CVD. We conjecture that elevated BMI enhances the predictive power of eGDR for long-term outcomes in the study population, but further research is needed to verify this.
There are several limitations to this study as well, which cannot be overlooked. Firstly, it should be considered that this is a single-center, observational study. Therefore, a larger-scale multi-center clinical trial involving more ethnic groups is needed to further validate the conclusions of this study. Secondly, this study did not perform a cross-sectional comparison of eGDR with other simple surrogate metrics for assessing IR. Therefore, future studies need to further clarify the role of eGDR as a predictor of CVD prognosis. Thirdly, since most of the NSTE-ACS patients in this investigation had UA, the predictive value of eGDR in NSTEMI patients may not be accurately reflected by these data. Fourthly, the end points of this study did not include heart failure and cardiac death.
Conclusions
eGDR proved to be an independent predictor of a poor prognosis in diabetes-negative patients with NSTE-ACS and PCI. The prediction ability that conventional risk variables showed for a poor prognosis was greatly improved by eGDR.
Availability of data and materials
The dataset for this study is available from the authors upon reasonable request.
Abbreviations
- CVD:
-
Cardiovascular disease
- IR:
-
Insulin resistance
- HOMA-IR:
-
Homoeostasis model assessment of insulin resistance
- HIEG:
-
Hyperinsulinemic–euglycemic
- eGDR:
-
Estimated glucose disposal rate
- T1DM:
-
Type 1 diabetes mellitus
- WC:
-
Waist circumference
- HbA1c:
-
Glycosylated hemoglobin
- CABG:
-
Coronary artery bypass grafting
- T2DM:
-
Type 2 diabetes mellitus
- NSTE-ACS:
-
Non-ST-segment elevation acute coronary syndrome
- PCI:
-
Percutaneous coronary intervention
- NSTEMI:
-
Non-ST-segment elevation myocardial infarction
- UA:
-
Unstable angina
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- PAD:
-
Peripheral arterial disease
- SYNTAX:
-
The synergy between PCI with taxus and cardiac surgery
- MACCE:
-
Major adverse cardio-cerebral event
- MI:
-
Myocardial infarction
- ECG:
-
Electrocardiogram
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- BMI:
-
Body mass index
- CAD:
-
Coronary artery disease
- TG:
-
Triglyceride
- TC:
-
Total cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- LVEF:
-
Left ventricular ejection fraction
- ACEI:
-
Angiotensin-converting enzyme inhibitor
- ARB:
-
Angiotensin receptor blocker
- LM:
-
Left main artery
- LAD:
-
Left anterior descending artery
- LCX:
-
Left circumflex artery
- RCA:
-
Right coronary artery
- DES:
-
Drug-eluting stent
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under curve
- Continuous-NRI:
-
Continuous net reclassification improvement
- IDI:
-
Integrated discrimination improvement
- TyG:
-
Triglyceride-glucose
- VAI:
-
Visceral adiposity index
References
Jernberg T, Hasvold P, Henriksson M, Hjelm H, Thuresson M, Janzon M. Cardiovascular risk in post-myocardial infarction patients: nationwide real world data demonstrate the importance of a long-term perspective. Eur Heart J. 2015;36(19):1163–70.
Fox KA, Carruthers KF, Dunbar DR, Graham C, Manning JR, De Raedt H, et al. Underestimated and under-recognized: the late consequences of acute coronary syndrome (GRACE UK-Belgian Study). Eur Heart J. 2010;31(22):2755–64.
Schwartz GG, Abt M, Bao W, DeMicco D, Kallend D, Miller M, et al. Fasting triglycerides predict recurrent ischemic events in patients with acute coronary syndrome treated with statins. J Am Coll Cardiol. 2015;65(21):2267–75.
Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–22.
Bonora E, Kiechl S, Willeit J, Oberhollenzer F, Egger G, Meigs JB, et al. Insulin resistance as estimated by homeostasis model assessment predicts incident symptomatic cardiovascular disease in caucasian subjects from the general population: the Bruneck study. Diabetes Care. 2007;30(2):318–24.
Jeppesen J, Hansen TW, Rasmussen S, Ibsen H, Torp-Pedersen C, Madsbad S. Insulin resistance, the metabolic syndrome, and risk of incident cardiovascular disease: a population-based study. J Am Coll Cardiol. 2007;49(21):2112–9.
Uetani T, Amano T, Harada K, Kitagawa K, Kunimura A, Shimbo Y, et al. Impact of insulin resistance on post-procedural myocardial injury and clinical outcomes in patients who underwent elective coronary interventions with drug-eluting stents. JACC Cardiovasc Interv. 2012;5(11):1159–67.
Isomaa B, Almgren P, Tuomi T, Forsén B, Lahti K, Nissén M, et al. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care. 2001;24(4):683–9.
Hanley AJ, Williams K, Stern MP, Haffner SM. Homeostasis model assessment of insulin resistance in relation to the incidence of cardiovascular disease: the San Antonio heart study. Diabetes Care. 2002;25(7):1177–84.
Gast KB, Tjeerdema N, Stijnen T, Smit JW, Dekkers OM. Insulin resistance and risk of incident cardiovascular events in adults without diabetes: meta-analysis. PLoS ONE. 2012;7(12): e52036.
Williams KV, Erbey JR, Becker D, Arslanian S, Orchard TJ. Can clinical factors estimate insulin resistance in type 1 diabetes? Diabetes. 2000;49(4):626–32.
Kietsiriroje N, Pearson S, Campbell M, Ariëns R, Ajjan RA. Double diabetes: a distinct high-risk group? Diabetes Obes Metab. 2019;21(12):2609–18.
Nyström T, Holzmann MJ, Eliasson B, Svensson AM, Kuhl J, Sartipy U. Estimated glucose disposal rate and long-term survival in type 2 diabetes after coronary artery bypass grafting. Heart Vessels. 2017;32(3):269–78.
Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, et al. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(3):267–315.
Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81-90.
Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 International Society of Hypertension Global Hypertension practice guidelines. Hypertension. 2020;75(6):1334–57.
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–88.
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3):e46–110.
Creager MA, Belkin M, Bluth EI, Casey DJ, Chaturvedi S, Dake MD, et al. 2012 ACCF/AHA/ACR/SCAI/SIR/STS/SVM/SVN/SVS key data elements and definitions for peripheral atherosclerotic vascular disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on clinical data standards (writing committee to develop clinical data standards for peripheral atherosclerotic vascular disease). J Am Coll Cardiol. 2012;59(3):294–357.
Editorial Board of Chinese. Chinese guideline for percutaneous coronary intervention. Zhonghua Xin Xue Guan Bing Za Zhi. 2016;44(5):382–400.
Brilakis ES, Mashayekhi K, Tsuchikane E, Abi RN, Alaswad K, Araya M, et al. Guiding principles for chronic total occlusion percutaneous coronary intervention. Circulation. 2019;140(5):420–33.
Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165.
Rampidis GP, Benetos G, Benz DC, Giannopoulos AA, Buechel RR. A guide for gensini score calculation. Atherosclerosis. 2019;287:181–3.
Epstein EJ, Osman JL, Cohen HW, Rajpathak SN, Lewis O, Crandall JP. Use of the estimated glucose disposal rate as a measure of insulin resistance in an urban multiethnic population with type 1 diabetes. Diabetes Care. 2013;36(8):2280–5.
Bressler P, Bailey SR, Matsuda M, DeFronzo RA. Insulin resistance and coronary artery disease. Diabetologia. 1996;39(11):1345–50.
Malita FM, Karelis AD, St-Pierre DH, Garrel D, Bastard JP, Tardif A, et al. Surrogate indexes vs euglycaemic–hyperinsulinemic clamp as an indicator of insulin resistance and cardiovascular risk factors in overweight and obese postmenopausal women. Diabetes Metab. 2006. https://doi.org/10.1016/S1262-3636(07)70276-8.
Ruige JB, Mertens IL, Bartholomeeusen E, Dirinck E, Ferrannini E, Van Gaal LF. Fasting-based estimates of insulin sensitivity in overweight and obesity: a critical appraisal. Obesity (Silver Spring). 2006;14(7):1250–6.
Di Pino A, DeFronzo RA. Insulin resistance and atherosclerosis: implications for insulin-sensitizing agents. Endocr Rev. 2019;40(6):1447–67.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity comparison with the euglycemic–hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010. https://doi.org/10.1210/jc.2010-0288.
McLaughlin T, Reaven G, Abbasi F, Lamendola C, Saad M, Waters D, et al. Is there a simple way to identify insulin-resistant individuals at increased risk of cardiovascular disease? Am J Cardiol. 2005;96(3):399–404.
Amato MC, Giordano C, Galia M, Criscimanna A, Vitabile S, Midiri M, et al. Visceral adiposity index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care. 2010;33(4):920–2.
Kouli GM, Panagiotakos DB, Kyrou I, Georgousopoulou EN, Chrysohoou C, Tsigos C, et al. Visceral adiposity index and 10-year cardiovascular disease incidence: the ATTICA study. Nutr Metab Cardiovasc Dis. 2017;27(10):881–9.
Sultani R, Tong DC, Peverelle M, Lee YS, Baradi A, Wilson AM. Elevated triglycerides to high-density lipoprotein cholesterol (TG/HDL-C) ratio predicts long-term mortality in high-risk patients. Heart Lung Circ. 2020;29(3):414–21.
Luo E, Wang D, Yan G, Qiao Y, Liu B, Hou J, et al. High triglyceride–glucose index is associated with poor prognosis in patients with acute ST-elevation myocardial infarction after percutaneous coronary intervention. Cardiovasc Diabetol. 2019;18(1):150.
Cho YR, Ann SH, Won KB, Park GM, Kim YG, Yang DH, et al. Association between insulin resistance, hyperglycemia, and coronary artery disease according to the presence of diabetes. Sci Rep. 2019;9(1):6129.
Šimonienė D, Platūkiene A, Prakapienė E, Radzevičienė L, Veličkiene D. Insulin resistance in type 1 diabetes mellitus and its association with patient’s micro-and macrovascular complications, sex hormones, and other clinical data. Diabetes Ther. 2020;11(1):161–74.
Nyström T, Holzmann MJ, Eliasson B, Svensson AM, Sartipy U. Estimated glucose disposal rate predicts mortality in adults with type 1 diabetes. Diabetes Obes Metab. 2018;20(3):556–63.
Zabala A, Darsalia V, Lind M, Svensson AM, Franzén S, Eliasson B, et al. Estimated glucose disposal rate and risk of stroke and mortality in type 2 diabetes: a nationwide cohort study. Cardiovasc Diabetol. 2021;20(1):202.
DeFronzo RA. Insulin resistance, lipotoxicity, type 2 diabetes and atherosclerosis: the missing links the claude bernard lecture 2009. Diabetologia. 2010;53(7):1270–87.
Zeng G, Nystrom FH, Ravichandran LV, Cong LN, Kirby M, Mostowski H, et al. Roles for insulin receptor, PI3-kinase, and Akt in insulin-signaling pathways related to production of nitric oxide in human vascular endothelial cells. Circulation. 2000;101(13):1539–45.
Ueda H, Mitsusada N, Harimoto K, Miyawaki M, Yasuga Y, Hiraoka H. Glycosylated hemoglobin is a predictor of major adverse cardiac events after drug-eluting stent implantation in patients with diabetes mellitus. Cardiology. 2010;116(1):51–7.
Naito R, Miyauchi K, Ogita M, Kasai T, Kawaguchi Y, Tsuboi S, et al. Impact of admission glycemia and glycosylated hemoglobin A1c on long-term clinical outcomes of non-diabetic patients with acute coronary syndrome. J Cardiol. 2014;63(2):106–11.
Upadhyay J, Farr O, Perakakis N, Ghaly W, Mantzoros C. Obesity as a disease. Med Clin North Am. 2018;102(1):13–33.
Lee Y, Jin U, Lee WM, Lim HS, Lim YH. Relationship of body mass index and waist circumference with clinical outcomes following percutaneous coronary intervention. PLoS ONE. 2018;13(12):e0208817.
Pickup JC. Inflammation and activated innate immunity in the pathogenesis of type 2 diabetes. Diabetes Care. 2004;27(3):813–23.
Laakso M, Kuusisto J. Insulin resistance and hyperglycaemia in cardiovascular disease development. Nat Rev Endocrinol. 2014;10(5):293–302.
Greenfield JR, Campbell LV. Insulin resistance and obesity. Clin Dermatol. 2004;22(4):289–95.
Acknowledgements
Not applicable.
Funding
The study was funded by Beijing Municipal Administration of Hospitals “Mission plan” (SML20180601) and National Key Research and Development Program of China (2017YFC0908800).
Author information
Authors and Affiliations
Contributions
CL made substantial contributions to data collection, data analysis and manuscript writing. QZ, YJZ made substantial contributions to study design and intellectual direction. XLL, XTM, YJC, YS, DZ made contributions to data collection and analysis. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethical approval and consent to participate
This research protocol was approved by the Clinical Research Ethics Committee of Beijing Anzhen Hospital, Capital Medical University. Although the study design was retrospective, participants provided written or verbal informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Table S1. Unadjusted Cox regression analysis investigating predictors of MACCE. Figure S1. Calculation of Gensini score of representative case.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, C., Liu, X., Ma, X. et al. Predictive worth of estimated glucose disposal rate: evaluation in patients with non-ST-segment elevation acute coronary syndrome and non-diabetic patients after percutaneous coronary intervention. Diabetol Metab Syndr 14, 145 (2022). https://doi.org/10.1186/s13098-022-00915-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-022-00915-9