
Abstract
Objective
To investigate the clinical efficacy and safety of dapagliflozin in the treatment of diabetic nephropathy (DN).
Methods
A total of 120 DN patients admitted to our hospital from June 2017 to March 2020 were divided into control and experimental groups, with 60 cases in each group. The control group received valsartan, and the experimental group received dapagliflozin for 3 months. Body mass index (BMI), hemoglobin A1c (HbA1c), serum creatinine (sCr), uric acid (UA), urine microalbumin (uMA), urine creatinine (uCr), and bilateral kidney function were compared before and after treatment, and adverse reactions in both groups were observed. Serum interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) levels were also evaluated.
Results
After treatment, except for BMI in the control group, all indexes in both groups were significantly improved. The BMI, HbA1c, sCr, UA, and uMA/uCr ratios of the experimental group were lower than those of the control group. Serum albumin (sAlb) levels were increased in both groups, and the experimental group showed a significant difference compared with the control group. Estimated glomerular filtration rate (eGFR) levels were increased in both groups, and the experimental group was higher than the control group, with no significant differences. Serum IL-6 and TNF-α levels in both groups were lower, and the experimental group was significantly lower than the control group. No serious adverse reactions were observed in either group.
Conclusion
The efficacy of dapagliflozin was demonstrated by its ability to improve diabetes, prevent nephropathy exacerbation, and reduce symptomatic reactions. The low rate of adverse reactions makes dapagliflozin a very safe medication.
Similar content being viewed by others


Introduction
Diabetic nephropathy (DN) is one of the common microvascular complications of diabetes and is characterized by albuminuria and glomerular filtration rate (GFR) reduction [1]. Hyperglycemia and glucose metabolites such as advanced glycation end products (AGEs) have long been regarded as initial factors of DN, which promote the loss of podocytes, the hyperfiltration of endothelial cells, the expansion of mesangial cells, and the thickening of the glomerular basement membrane. [2]. Although many therapies have been used to improve DN, the quality of life of an increasing number of patients is severely impacted [3]. As a result, more novel therapeutic strategies are needed for DN treatment.
Recent advances emphasized the therapeutic value of sodium-glucose cotransporter-2 inhibitors (SGLT2i), which reduced the risk of progression of renal disease by 45% [4]. Dapagliflozin is an SGLT2i that has been shown to decrease glycated hemoglobin (HbA1c) by promoting urinary glucose excretion, body weight, systolic blood pressure, and albuminuria [5]. A large cardiovascular outcome trial demonstrated that dapagliflozin also significantly reduced the risks of heart failure and progression of chronic kidney disease in people with type 2 diabetes [6]. Some recent studies have focused on the DN therapeutic effect of dapagliflozin. It was reported that ticagrelor and dapagliflozin have additive effects on ameliorating diabetic nephropathy in mice with type-2 diabetes mellitus [7]. Additionally, dapagliflozin treatment improved histopathological examinations, inflammatory and apoptotic markers in a dose-dependent manner when compared to diabetic vehicles, implying that dapagliflozin may have renoprotective effects, which are promising in diabetic patients with nephropathy. [8]. Furthermore, dapagliflozin attenuates early markers of diabetic nephropathy in fructose-streptozotocin-induced diabetes in rats [9]. However, most research on the DN therapeutic effect of dapagliflozin has been performed in mice or rat models, and the clinical data are minimal.
Thus, in this study, we conducted a clinical study on the efficacy and safety of dapagliflozin in patients with diabetic nephropathy by evaluating body mass index (BMI), hemoglobin A1c (HbA1c), serum creatinine (sCr), uric acid (UA), urine microalbumin (uMA), urinary creatinine (uCr), bilateral kidney function, and the occurrence of adverse reactions.
Materials and methods
General information
A total of 120 Chinese patients with DN in our hospital (Zhuhai People’s Hospital) from June 2017 to March 2020 were selected and randomly divided into the control group (n = 60) and experimental group (n = 60). Power analysis was used to calculate sample size, and patients were randomly assigned to one of two groups in a 1:1 ratio. The control group was treated with valsartan, and the experimental group was treated with dapagliflozin. The primary characteristics, including age, sex, course of disease (years), BMI (kg/m2), HbA1c (%), sCr (μmol/L), UA (μmol/L), and urinary amylase/urinary creatinine ratio uMA/uCr (μg/mg), were compared before and after treatment.
Inclusion and exclusion criteria
Inclusion criteria: (i) age between 18 and 70 years; (ii). patients who met the diagnostic criteria for diabetes mellitus published by the World Health Organization (WHO) in 2021, 1999 and had stable glucose control (less than 10% change in the previous 2 months); (iii) persistent albuminuria (≥ 30 mg/24 h) or eGFR < 60 ml/min/1.73 m2; glycated HbA1c was 7.0% ~ 11.0%, and the patients with inadequate blood glucose control but good compliance were treated with oral hypoglycemic agents or subcutaneous insulin injections to control blood glucose; (iv) individuals with normal cognitive function and written informed consent.
Exclusion criteria: (i) patients with non-diabetic nephropathy, such as glomerulonephritis and urinary tract infection; (ii) patients with severe cardiovascular and cerebrovascular diseases; and heart failure (New York Heart Association functional class III-IV); (iii) liver dysfunction (aspartate transaminase and alanine transaminase levels > 100 IU/L); (iv) patients with acute complications of diabetes, such as diabetic ketoacidosis and diabetic hyperosmolar coma; patients with malignant tumors; patients with a previous history of SGLT-2i medication and patients allergic to angiotensin receptor blocker (ARB) drugs.
Methods
Routine nursing followed the standard management of diabetes, including daily diet, physical exercise, and blood glucose monitoring. Based on oral hypoglycemic drugs or subcutaneous insulin injections to control blood glucose, the control group was given 80 mg valsartan (Beijing Novartis Pharmaceutical Co., Ltd., approval number: Guoyao Zhun H20040217, specification: 80 mg/tablet) twice a day, and the experimental group was given 10 mg of dapagliflozin (AstraZeneca Pharmaceutical Co., Ltd., batch number: H20170040, specification: 10 mg/tablet) once a day. Both groups received treatment for 3 months.
Diabetic nephropathy- and symptomatic reaction-associated indexes
The sAlb was detected by the bromocresol green (BCG) method; the estimated glomerular filtration rate (eGFR) was affected by the level of sAlb, and an automatic biochemical analyzer detected blood glucose and renal function. The eGFR was calculated using the Modification of Diet in Renal Disease (MDRD) formula.
The BMI of the two groups before and after treatment was calculated. HbA1c, sCr, UA, uMA, and uCr were detected by the Abbott chemiluminescence method, and the uMA/uCr ratio was calculated.
Adverse reactions (such as hypoglycemia, hypotension, dizziness, and urinary tract infection) were recorded, and the total incidence of adverse reactions was calculated.
Inflammatory indexes, including interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α), were detected before and after treatment. Radioimmunoassays were used to detect IL-6 and TNF-α.
Statistical analysis
All data were analyzed by SPSS 22.0. The measurement data are expressed as the mean ± standard deviation (x ± s) and were compared with a t-test. The count data were expressed as a percentage (%) and compared with the χ2 test. P < 0.05 was considered statistically significant.
Results
Comparison of the primary characteristics
The average age of the control group was 55.67 ± 11.46 years, 36 males and 24 females, and the average course of the disease was 9.65 ± 2.55 years; the average age of the experimental group was 56.21 ± 11.18 years, 34 males and 26 females, and the average course of the disease was 10.04 ± 2.31 years. There was no significant difference in age, sex, course of the disease, or other general information between the two groups (P > 0.05), which was comparable, as shown in Table 1.
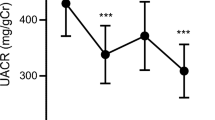
After treatment, in addition to the BMI of the control group, all the other indexes of both groups were significantly improved (P < 0.05). After the treatment, the BMI, HbA1c, sCr, UA, and uMA/uCr ratio of the experimental group were lower than those of the control group (P < 0.05), as shown in Table 2. These results indicate that dapagliflozin improves the basic indicators of DN patients.
Comparison of sAlb and eGFR levels
Before treatment, there was no significant difference in sAlb or eGFR between the two groups (P > 0.05). After treatment, the sAlb levels of the two groups were increased, and experimental group results were significantly higher than those of the control group (P < 0.05). The eGFR levels of the two groups were also increased after treatment; however, the experimental group exhibited higher levels than the control group, but the difference was not statistically significant (P > 0.05) (Table 3). These results indicate that the levels of sAlb were increased by dapagliflozin treatment.
Comparison of serum inflammatory factors before and after treatment
Before treatment, there was no significant difference in serum IL-6 and TNF-α levels between the two groups (P > 0.05). On the 1st day after the operation, the levels of serum IL-6 and TNF-α in both groups were lower than those before treatment, and the levels in the experimental group were significantly lower than those in the control group (P < 0.05) (Table 4). These results indicate that the serum inflammatory factors were decreased after dapagliflozin treatment.
Comparison of adverse reactions
The patients in the control group were well tolerated, including 2 cases of hypoglycemia, 2 cases of hypotension, and 3 cases of urinary tract infection. There were 3 cases of dizziness and 3 cases of hypotension in the experimental group. There was no significant difference in the total incidence of adverse reactions between the two groups (P > 0.05). No other severe adverse reactions occurred in either group (Table 5). These data indicate that dapagliflozin has a low total incidence of adverse reactions.
Discussion
The incidence rate of diabetes and its complications has become increasingly higher because of changes in diet structure. DN is the leading cause of chronic kidney disease (CKD) and renal failure [10]. At present, there is no definite conclusion on the pathogenesis of DN, which is generally believed to be the result of the action of multiple factors, which may be related to abnormal glomerular hemodynamics, increased glomerular pressure, and activation of inflammatory factors. Edema and proteinuria are common clinical symptoms. When they develop to a certain extent, they will cause renal vascular damage due to high blood glucose and blood pressure. A load of renal filtered blood will aggravate and lead to renal disease. Later, they are likely to develop into uremia [11]. Therefore, the early treatment of the disease is very important, and the main principle of treatment is to control blood sugar and reduce the burden on the kidney [12].
Sodium-glucose cotransporter (SGLT) is expressed in the renal proximal convoluted tubules and can be divided into SGLT-1 and SGLT-2i subtypes. The SGLT-2i receptor is a glucose transporter with high capacity, high transport capacity, and low affinity. It is expressed in the S1 and S2 segments of proximal convoluted tubules and mainly undertakes glucose reabsorption [13, 14]. In diabetic patients, the upregulation of SGLT-2i helps to maintain hyperglycemia, while inhibition of SGLT-2i can effectively improve blood glucose control. SGLT-2i can reduce blood glucose by inhibiting the reabsorption of sodium and glucose by renal proximal convoluted tubules, increasing the excretion of urine glucose, increasing the function of islet β cells, improving insulin resistance, and greatly reducing renal metabolic disorders caused by chronic hyperglycemia [15, 16]. In addition, SGLT-2i also increases the excretion of sodium in renal tubules, resulting in a diuretic effect, that reduces the volume of body fluid and blood pressure, thus reducing glomerular ultrafiltration [17]. Dapagliflozin is a representative SGLT-2i drug that has been widely used in patients with diabetes [18]. The results of this study showed that after 3 months of treatment with dapagliflozin, the BMI, HbA1c, sCr, UA, and uMA/uCr ratio of the patients decreased, indicating that dapagliflozin can effectively control glucose and protect the kidney, which is consistent with the results of previous studies [19]. After treatment, the indexes of the experimental group were lower than those of the control group, indicating that dapagliflozin is more effective than valsartan in the treatment of DN. In addition, the sAlb and eGFR levels of both groups increased after treatment, and the sAlb levels in the study group were significantly higher than those of the control group. Although there was no significant difference in eGFR levels between the two groups. The possible reason is that in the early stage of diabetic nephropathy, sodium-glucose cotransporters (SGLTs) can increase the reabsorption of sodium ions and fluid in renal proximal convoluted tubules. This reabsorption can lead to glomerular hyperfiltration by reducing the concentrations of Na and K in dense plaques and increasing the GFR is caused by tubule feedback. As an inhibitor of SGLT-2, dapagliflozin can improve the glomerular hyperfiltration state and protect the kidney [20,21,22].
The traditional pathogenesis of DN is the dual effects of hemodynamic changes and severe persistent hyperglycemia. Recent studies have shown that DN is a chronic low-grade inflammatory state, and inflammation-related molecules and pathways play an important role in the process of early DN, indicating that targeted inflammation may be one of the methods to treat DN [23]. Krishan et al. [24] showed that high mobility group box-1 (HMGB1) was closely related to the occurrence and development of DN and positively correlated with TNF-α and IL-6. In addition, dapagliflozin may have an additional anti-inflammatory effect on the kidneys, which is independent of blood glucose and blood pressure [25]. Urinary excretion of renal tubular injury markers and inflammatory markers (such as IL-6) decreased in type 2 diabetes (T2DM) patients after treatment with dapagliflozin [26]. This study showed that the inflammatory indexes (TNF-α, IL-6) of the dapagliflozin group were significantly lower than those at baseline after 3 months of treatment, which was consistent with the above results. After 3 months of treatment, although the indexes of both groups improved, the changes in the dapagliflozin group were more significant than those in the valsartan group. Therefore, dapagliflozin has a renal protection function independent of reducing blood glucose, blood pressure, and body weight, which can improve the glomerular and renal tubular function of patients with early DN, reduce the release of TNF-α and IL-6 inflammatory factors, and improve renal function through anti-chronic inflammatory effects.
Conclusion
In the clinical treatment of patients with diabetic nephropathy, dapagliflozin has a significant effect, which can effectively improve the condition of patients with diabetes, control the aggravation of patients with nephropathy, reduce the symptoms of patients, and have an outstanding curative effect. In addition, the probability of adverse reactions in patients after the medication is low, safe, and effective.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AGE:
-
Advanced glycation end
- ARB:
-
Angiotensin receptor blocker
- BCG:
-
Bromocresol green
- BMI:
-
Body mass index
- CKD:
-
Chronic kidney disease
- DN:
-
Diabetic nephropathy
- GFR:
-
Glomerular filtration rate
- eGFR:
-
Estimated glomerular filtration rate
- IL-6:
-
Interleukin-6
- TNF-α:
-
Tumor necrosis factor-alpha
- SGLT:
-
Sodium-glucose cotransporter
- T2DM:
-
Type 2 diabetes
- SGLT:
-
Sodium-glucose cotransporter
- MDRD:
-
Modification of Diet in Renal Disease
- UA:
-
Uric acid
- WHO:
-
World Health Organization
- HbA1c:
-
hemoglobin A1c
- sCr:
-
Serum creatinine
- uMA/uCr:
-
Microalbumin to creatinine ratio
References
Natesan V, Kim SJ. Diabetic nephropathy—a review of risk factors, progression, mechanism, and dietary management. Biomol Ther. 2021;29(4):365–72.
Shao BY, et al. Epigenetics and Inflammation in Diabetic Nephropathy. Front Physiol. 2021;12:649587.
Ruiz-Ortega M, et al. Targeting the progression of chronic kidney disease. Nat Rev Nephrol. 2020;16(5):269–88.
Zelniker TA, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393(10166):31–9.
Komoroski B, et al. Dapagliflozin, a novel, selective SGLT2 inhibitor, improved glycemic control over 2 weeks in patients with type 2 diabetes mellitus. Clin Pharmacol Ther. 2009;85(5):513–9.
Wiviott SD, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–57.
Birnbaum Y, et al. Ticagrelor and Dapagliflozin have additive effects in ameliorating diabetic nephropathy in mice with type-2 diabetes mellitus. Cardiovasc Drugs Ther. 2021. https://doi.org/10.1007/s10557-021-07222-x.
Elkazzaz SK, et al. Role of sodium glucose cotransporter type 2 inhibitors dapagliflozin on diabetic nephropathy in rats; Inflammation, angiogenesis and apoptosis. Life Sci. 2021;280:119018.
Oraby MA, et al. Dapagliflozin attenuates early markers of diabetic nephropathy in fructose-streptozotocin-induced diabetes in rats. Biomed Pharmacother. 2019;109:910–20.
van Bommel EJM, et al. The renal hemodynamic effects of the SGLT2 inhibitor dapagliflozin are caused by post-glomerular vasodilatation rather than pre-glomerular vasoconstriction in metformin-treated patients with type 2 diabetes in the randomized, double-blind RED trial. Kidney Int. 2020;97(1):202–12.
Zhang D, et al. Proteomics analysis reveals diabetic kidney as a ketogenic organ in type 2 diabetes. Am J Physiol Endocrinol Metab. 2011;300(2):E287–95.
Nosadini R, et al. Kidney hemodynamics after ketone body and amino acid infusion in normal and IDDM subjects. Diabetes. 1989;38(1):75–83.
Pfeffer MA, et al. A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease. N Engl J Med. 2009;361(21):2019–32.
Mazer CD, et al. Effect of Empagliflozin on erythropoietin levels, iron stores, and red blood cell morphology in patients with type 2 diabetes mellitus and coronary artery disease. Circulation. 2020;141(8):704–7.
Eckardt KU, Kurtz A. Regulation of erythropoietin production. Eur J Clin Invest. 2005;35(Suppl 3):13–9.
Persson P, Palm F. Hypoxia-inducible factor activation in diabetic kidney disease. Curr Opin Nephrol Hypertens. 2017;26(5):345–50.
Paliege A, et al. Hypoxia-inducible factor-2alpha-expressing interstitial fibroblasts are the only renal cells that express erythropoietin under hypoxia-inducible factor stabilization. Kidney Int. 2010;77(4):312–8.
Rankin EB, et al. Hypoxia-inducible factor-2 (HIF-2) regulates hepatic erythropoietin in vivo. J Clin Invest. 2007;117(4):1068–77.
Kato S, et al. TP0463518, a novel prolyl hydroxylase inhibitor, specifically induces erythropoietin production in the liver. J Pharmacol Exp Ther. 2019;371(3):675–83.
Yuan Y, Beitner-Johnson D, Millhorn DE. Hypoxia-inducible factor 2alpha binds to cobalt in vitro. Biochem Biophys Res Commun. 2001;288(4):849–54.
Ohtomo S, et al. Cobalt ameliorates renal injury in an obese, hypertensive type 2 diabetes rat model. Nephrol Dial Transplant. 2008;23(4):1166–72.
Olmos G, et al. Impaired erythropoietin synthesis in chronic kidney disease is caused by alterations in extracellular matrix composition. J Cell Mol Med. 2018;22(1):302–14.
Schonenberger MJ, Kovacs WJ. Hypoxia signaling pathways: modulators of oxygen-related organelles. Front Cell Dev Biol. 2015;3:42.
Walter KM, et al. Hif-2alpha promotes degradation of mammalian peroxisomes by selective autophagy. Cell Metab. 2014;20(5):882–97.
Krishan P, Singh G, Bedi O. Carbohydrate restriction ameliorates nephropathy by reducing oxidative stress and upregulating HIF-1alpha levels in type-1 diabetic rats. J Diabetes Metab Disord. 2017;16:47.
Brunelle JK, et al. Oxygen sensing requires mitochondrial ROS but not oxidative phosphorylation. Cell Metab. 2005;1(6):409–14.
Acknowledgements
Not applicable.
Funding
The authors declare that there are no sources of funding to be acknowledged.
Author information
Authors and Affiliations
Contributions
YH and HL were involved in the conception and design of this study. YH and WL performed the data analysis and interpretation of the results. YH and WL prepared the first draft of the manuscript. HL did a critical revision of the manuscript. HL supervised the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was carried out in accordance with the Helsinki Declaration and was approved by the Ethics Committee of Zhuhai Hospital, affiliated with Jinan University. All participants provided written informed consent when they were enrolled in the study.
Consent for publication
Not applicable.
Competing interests
The authors report no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huang, Y., Lu, W. & Lu, H. The clinical efficacy and safety of dapagliflozin in patients with diabetic nephropathy. Diabetol Metab Syndr 14, 47 (2022). https://doi.org/10.1186/s13098-022-00815-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-022-00815-y