
Abstract
Background
This study aims to ascertain whether (1) an educational program is sufficient to achieve adequate Diaphragm Ultrasound (DUS) assessments on healthy volunteers and (2) combining a video tutorial with a practical session is more effective in making learners capable to obtain accurate DUS measurements, as opposed to sole video tutorial.
Results
We enrolledstep 1: 172 volunteers naïve to ultrasound. After watching a video tutorial, a questionnaire was administered and considered to be passed when at least 70% of the questions were correctly answered. Course participants who passed the theoretical test were randomized to either intervention or control group. Learners randomized to the interventional group underwent to a practical training, tutored by an expert, before accessing DUS examination. Participants randomized to the control group directly accessed DUS examination, without any practical training. DUS measurements by learners and tutors were recorded and checked for accuracy, according to predefined criteria. Detection of both acoustic windows and accurate DUS assessment was achieved by 83.7% learners of the intervention group while 3.5% only among controls (p < 0.0001). The subcostal view of the diaphragm was correctly identified by 92% and 65% learners in the intervention and control groups, respectively (p < 0.0001) while the apposition zone by 86% and 71% learners, respectively (p = 0.026). An accurate diaphragm displacement (DD) measurement was obtained by 91% and 45% learners in the intervention and control groups, respectively (p < 0.0001) while an accurate thickening fraction (TF) measurement by 99% and 21%, respectively (p < 0.0001). DD measurements by both groups of learners were significantly correlated with those assessed by expert tutors; however, a significant improvement of measurement accuracy was found in learners randomized to receive also the practical training, compared to controls.
Conclusions
A combined approach consisting of a theoretical module followed by a practical training is more effective in managing acoustic windows and performing accurate measurements when compared to an exclusively theoretical course.
Trial registration prospectively registered on clinicaltrials.gov (Identifier: NCT03704129; release date 17th October 2018).
Similar content being viewed by others

Background
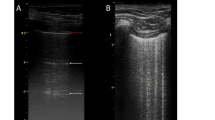
Diaphragm ultrasonography (DUS) allows serial radiation-free bedside evaluations of diaphragmatic function in critically ill patients [1, 2]. DUS allows the assessment of both cranio-caudal diaphragm displacement (DD) from subcostal acoustic windows, and thickness at the end of inspiration (Thickinsp) and expiration (Thickexp) in the zone of apposition, to compute the thickening fraction (TF) as Thickinsp − Thickexp/Thickexp [1].
While some studies evaluated the educational approaches for the achievement of skills for specific cardiac and lung ultrasound assessments, no study has so far evaluated how to develop appropriate DUS skills, despite the increased interest for this technique [3, 4]. Though a fair amount of tutored examinations is necessary to achieve appropriate skills for patient assessment by ultrasonography [5], basic knowledge is necessary before starting evaluating patients.
The present study aims to ascertain whether (1) a brief educational program is sufficient to achieve adequate DUS assessments on healthy volunteers and (2) combining a video tutorial with a practical session on healthy volunteers is more effective in making learners with no previous experience capable to obtain accurate DUS measurements, as opposed to the sole video tutorial. We, therefore, compared these two educational approaches and assessed the rates of learners able to correctly detect the two acoustic windows (subcostal view and apposition zone), and the correlation between measurements (DD, Thickinsp, Thickexp, and TF) performed by learners and tutors.
Materials and methods
The study was carried out from December 1st 2018 to February 28th 2019 in the educational rooms of eight Italian University Hospitals (“Magna Graecia” University of Catanzaro, IRCCS San Raffaele Scientific Institute of Milan, University of Udine, “Eastern Piedmont” University of Novara, University of Pisa, University of Parma, University of Catania and Catholic University of the “Sacred Heart” of Rome). The study was approved by the local Ethics Committees and written informed consent was obtained from all participants. The trial was prospectively registered on clinicaltrials.gov (Identifier: NCT03704129; release date 17th October 2018).
Subjects
We recruited 172 voluntary learners with no experience of ultrasound assessments among medical students or first-year residents. We also designated 14 tutors, two in each centre, with a minimum 2-year experience of DUS in critical care US. Prior to study initiation, all tutors met on the web to standardize the practical training to be administered to the interventional group.
Study protocol
A video tutorial based on the current literature [1, 6,7,8,9] and focusing on key principles of the technique, including acoustic windows and anatomical landmarks featuring diaphragmatic US, was shown to all learners. The video tutorial is available online at https://youtu.be/B7AYP9fElyE.
Afterwards, a questionnaire including 10 multiple-choice questions was administered and considered to be passed when at least 70% of the questions were correctly answered. The questionnaire is enclosed as Additional file 1. Course participants who passed the theoretical test were then randomized to either intervention or control group.
Randomization was achieved with an allocation ratio of 1:1 by means of a computer-generated sequence, operated by an investigator not involved in the trial. Allocation blindness was assured using sequentially numbered sealed opaque envelopes, prepared by the aforementioned investigator. Each envelope contained the allocation of the learners to either control or interventional group, with a unique identifier code. The randomization was based on a centralized phone call system.
Learners randomized to the interventional group had access to the practical training, tutored by an expert evaluator who interactively explained how to perform DUS, before accessing DUS examination. Learners randomized to the control group directly accessed DUS examination, without any practical training by expert tutors. DUS examination was performed on healthy volunteers, not involved in the study protocol. Irrespective of the group of randomizations, learners were asked to independently perform DUS using both acoustic windows. All measurements were performed by learners after images’ acquisition and storage. A local investigator recorded the measurements. A tutor then judged if the images were correctly acquired, and only in such a case, he performed his own measurements on the same acquired images, being blind to the results obtained by the learners. These measurements were also recorded by the local investigator.
Data acquisition and analysis
Diaphragm US was performed by course participants and tutors using one of the following devices: MyLab™30, Esaote, Genova, Italy; MySono U6, Samsung, Seoul, South Korea; EPIQ7 ultrasound system, Philips Healthcare, Bothell, WA, USA.
Sonographic evaluation was conducted on the right hemi-diaphragm, as previously described [1, 6, 9,10,11]. Briefly, DD was ascertained through a 3.5–5 MHz phased array probe, placed immediately below the costal margin in the mid-clavicular line and directed medially, cephalad and dorsally, so that the US beam reached perpendicularly the posterior third of the hemi-diaphragm [1, 6, 9, 11]. The motion of the diaphragm and other anatomical structures along the selected line was displayed in “time-motion” mode (M-mode). DD was measured placing the first caliper at the end of expiration phase, while the second caliper was placed at the apex of inspiration slope [1, 6, 9, 11]. Diaphragm thickness was assessed through a linear 13 MHz probe placed in the 9th–10th intercostal space, closed to the midaxillary line, angled perpendicular to the chest wall, to identify the apposition zone of the diaphragm. Diaphragmatic thickness was the determined in M-mode at end-expiration (Thickexp) and at peak inspiration (Thickinsp) as the distance between the diaphragmatic pleura and the peritoneum [6, 7, 9]. TF was then computed as Thickinsp − Thickexp/Thickexp and expressed in percentage [6, 7, 9].
If a learner failed to correctly display the diaphragm in one of the two acoustic windows, the examination was considered to be negative. Only the measurements by learners who correctly identified both acoustic windows were considered for further analysis. Based on the previous agreement among members of the steering committee, the measurements were considered to be accurate when in the following predetermined ranges: (1) DD ± 2 mm from the value reported by the tutor and (2) TF ± 20% of the assessment recorded by the tutor. If both acoustic windows were correctly identified, and the resulting measurements were included within the predetermined ranges, the participant passed the examination, so that the first study outcome was achieved.
Statistical analysis
Gaussian data distribution was tested by means of the Kolmogorov–Smirnov test. Data are presented as mean (± standard deviation) or as median [25th–75th interquartile], as indicated. Categorical data were compared through Chi-square test while continuous data with Student t test or Mann–Whitney U test, as appropriate. By means of the Spearman’s rank correlation test, we determined the correlation coefficients (ρ) [95% interval confidence] between measurements (i.e., DD, Thickinsp, Thickexp, and TF) obtained by tutors and learners of each group, and the corresponding p values. To test the statistical significance of the difference, the ρ values separately obtained in the intervention and control groups were then compared and the z and p values were determined [12]. For all comparisons, p values < 0.05 were considered to be significant.
Results
All 172 learners passed the multiple-choice questionnaire test (score 95.5 ± 7.6%) accessing to the second phase of the study, and were randomized to either intervention or control group (86 subjects in both groups). Neither age nor female/male ratio were different between groups.
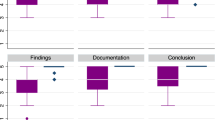
As depicted in Fig. 1, correct detection of both acoustic windows and accurate measurements was overall obtained by 72/86 (83.7%) learners allocated in the intervention (white bar) group, as opposed to 3/86 (3.5%) in the control group (grey bar) (p < 0.0001). The subcostal view of the diaphragm was correctly identified by 79/86 (92%) and 56/86 (65%) learners in the intervention and control groups, respectively (p < 0.0001) while the apposition zone of the diaphragm by 74/86 (86%) and 61/86 (71%) learners in the intervention and control groups, respectively (p = 0.026). An accurate DD measurement was obtained by 72/79 (91%) and 25/56 (45%) learners in the intervention and control groups, respectively (p < 0.0001) while an accurate TF measurement by 73/74 (99%) and 13/61 (21%) learners in the intervention and control groups, respectively (p < 0.0001) (see Fig. 1).

Number of learners reaching the study aims. From left to the right, the figure depicts the number of learners that: (1) correctly detected both acoustic windows and performed accurate measurements (first outcome); (2) correctly identified the subcostal view; (3) correctly identified the apposition zone; (4) accurately performed the DD measurement; and (5) accurately performed the TF measurement. White bars represent the intervention group while grey ones the control group. The dashed line represents the total number of learners randomized per group (n = 86)
Table 1 displays correlations of the measurements done by tutors and learners in the two groups. DD measurements by both groups of learners were significantly correlated with those assessed by expert tutors; however, a significant improvement of measurement accuracy was found in learners randomized to receive also the practical training, compared to controls. The measurements of Thickinsp, Thickexp, and TF performed by learners randomized in the intervention group were found to be strongly correlated with those obtained by the tutors, in contrast to those obtained by learners in the control group, as also indicated by the significant differences of the correlation comparisons.
Discussion
Our results show that (1) a brief educational program can make learners naive to the technique able to perform DUS on healthy volunteers; (2) compared to the sole theoretical teaching, the addition of a brief practical training improves (i) the ability to correctly detect the two acoustic windows and to perform accurate diaphragm US measurements; (ii) the rate of correct identifications of the two acoustic windows of the diaphragm; and (iii) the accuracy of DUS measurements.
To our knowledge, this is the first study evaluating a DUS educational program. Some studies evaluated educational programs for other applications of bedside ultrasound. Beaulieu et al., an initial web-based theoretical program followed by hands-on training performed by simulation and on both healthy and sick individuals, improved the ability of 37 junior emergency medicine residents to recognize both venous vessels (5.5 h) and pleura (2.5 h) [13]. Lim et al. showed that a 3-h educational course of lung ultrasound, combining 1 h of theory and 2 h of hands-on training on healthy subjects, significantly improved 40 medical students’ knowledge, image acquisition, and interpretation [14]. Melamed et al. administered a 2-h theoretical instruction on transthoracic echocardiography followed by a 4-h hands’ training on critically ill patients with (20 patients) or without (24 patients) left ventricular abnormalities, to previously untrained ICU physicians [15]. Afterwards, they evaluated their ability to detect normal or altered left ventricular function and found a proper detection in 86% of the cases. None of these studies, however, did not evaluate the importance of adding a practical training session, compared to the sole theory [13,14,15].
The accuracy of DD measurement was overall fairly reliable. However, in the control group, the rate of learners who properly identified through the subcostal acoustic window the hemidiaphragm was lower compared with the corrected detection of the hemidiaphragm thickness in the zone of apposition, 58% vs. 67%. Indeed, a poor acoustic window may occur in up to 10% of cases [16]. Moreover, the identification of the right hemidiaphragm through the subcostal acoustic window requires recognizing the anatomy of the liver, which is strongly dependent on the ability of the operator to direct the ultrasound beam cephalically and dorsally to this organ to reach the hemidiaphragm perpendicularly [17]. Quite the opposite, with the high-frequency and low-penetrance linear probe used to identify the diaphragm zone of apposition, the thickness is easily identified being located just below the skin [18]. However, measuring Thickinsp and Thickexp is much more difficult than assessing DD because of the small dimensions, which also makes the M-mode image hard to measure. Small errors in Thickinsp and Thickexp determination may consequently affect TF computation. That said, it is quite striking that learners in the intervention group were able to achieve measurements quite close to those obtained by the tutors.
Compared to the previous studies evaluating training on ultrasound for lung, heart, and venous vessels bedside evaluation [13,14,15], our study has the point of strength of enrolling a high number of trainees on a multicenter basis.
The major limitation of this study, that we share with the previous analogous investigations [13, 14, 19], is that learners performed DUS in healthy volunteers, which does not imply they would successfully perform unattended DUS evaluation in the clinical arena, where potential confounding factors such as underlying disease, mechanical ventilation, or abdominal distension can make DUS assessment more problematic. Rouby et al. demonstrated that 25 lung ultrasound examinations supervised by an expert tutor are enough to acquire adequate technical skills in critically ill patients [5]. Bergamaschi et al. also showed that a 3-h course followed by 6-h practical training and 25 supervised examinations was enough to acquire the ability to determine cardiac output by trans-thoracic echocardiography [20]. Data for DUS at this regard lack, but we believe that 25 supervised examinations would be sufficient to achieve adequate DUS skills for critically ill patients’ examination.
Conclusions
DUS can be easily taught to naïve to ultrasounds students. A combined approach consisting of a theoretical module followed by a practical training is more effective in managing acoustic windows and performing accurate measurements when compared to an exclusively theoretical session. After theoretical and practical training, the vast majority of learners accurately explored the diaphragm, thus obtaining DUS results consistent with those detected by an expert tutor.
Availability of data and materials
The authors will share all of the individual participant data collected during the trial after deidentification, to researchers who provide a methodologically sound proposal. For data availability contact: longhini.federico@gmail.com
Abbreviations
- DD:
-
diaphragm displacement
- DUS:
-
diaphragm ultrasound
- TF:
-
thickening fraction
- Thickinsp :
-
thickness at the end of inspiration
- Thickexp :
-
thickness at the end of expiration
References
Matamis D, Soilemezi E, Tsagourias M, Akoumianaki E, Dimassi S, Boroli F et al (2013) Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med 39(5):801–810
Goligher EC, Fan E, Herridge MS, Murray A, Vorona S, Brace D et al (2015) Evolution of diaphragm thickness during mechanical ventilation impact of inspiratory effort. Am J Respir Crit Care Med 192(9):1080–1088
Kuhl M, Wagner R, Bauder M, Fenik Y, Riessen R, Lammerding-Koppel M et al (2012) Student tutors for hands-on training in focused emergency echocardiography—a randomized controlled trial. BMC Med Educ 12:101
Diaz-Gomez JL, Perez-Protto S, Hargrave J, Builes A, Capdeville M, Festic E et al (2015) Impact of a focused transthoracic echocardiography training course for rescue applications among anesthesiology and critical care medicine practitioners: a prospective study. J Cardiothorac Vasc Anesth 29(3):576–581
Rouby JJ, Arbelot C, Gao Y, Zhang M, Lv J, An Y et al (2018) Training for lung ultrasound score measurement in critically ill patients. Am J Respir Crit Care Med. 198(3):398–401 (Epub ahead of print)
Longhini F, Pisani L, Lungu R, Comellini V, Bruni A, Garofalo E et al (2019) High-flow oxygen therapy after noninvasive ventilation interruption in patients recovering from hypercapnic acute respiratory failure: a physiological crossover trial. Crit Care Med 47(6):e506–e511
Goligher EC, Laghi F, Detsky ME, Farias P, Murray A, Brace D et al (2015) Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity. Intensive Care Med 41(4):642–649
Zambon M, Greco M, Bocchino S, Cabrini L, Beccaria PF, Zangrillo A (2017) Assessment of diaphragmatic dysfunction in the critically ill patient with ultrasound: a systematic review. Intensive Care Med 43(1):29–38
Garofalo E, Bruni A, Pelaia C, Cammarota G, Murabito P, Biamonte E et al (2019) Evaluation of a new interface combining high-flow nasal cannula and CPAP. Respir Care. https://doi.org/10.4187/respcare.06871 (Epub ahead of print)
Goligher EC, Laghi F, Detsky ME, Farias P, Murray A, Brace D et al (2015) Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity. Intensive Care Med 41(4):734
Boussuges A, Gole Y, Blanc P (2009) Diaphragmatic motion studied by m-mode ultrasonography: methods, reproducibility, and normal values. Chest 135(2):391–400
Hinkle DE, Wiersma W, Jurs SG (eds) (1988) Applied statistics for the behavioral sciences, 2nd edn. Houghton Mifflin Company, Boston
Beaulieu Y, Laprise R, Drolet P, Thivierge RL, Serri K, Albert M et al (2015) Bedside ultrasound training using web-based e-learning and simulation early in the curriculum of residents. Crit Ultrasound J. 7:1
Lim JS, Lee S, Do HH, Oh KH (2017) Can Limited Education of Lung Ultrasound Be Conducted to Medical Students Properly? A Pilot Study. Biomed Res Int. 2017:8147075
Melamed R, Sprenkle MD, Ulstad VK, Herzog CA, Leatherman JW (2009) Assessment of left ventricular function by intensivists using hand-held echocardiography. Chest 135(6):1416–1420
Kim WY, Suh HJ, Hong SB, Koh Y, Lim CM (2011) Diaphragm dysfunction assessed by ultrasonography: influence on weaning from mechanical ventilation. Crit Care Med 39(12):2627–2630
Vetrugno L, Guadagnin GM, Barbariol F, Langiano N, Zangrillo A, Bove T (2019) Ultrasound imaging for diaphragm dysfunction: a narrative literature review. J Cardiothorac Vasc Anesth 33(9):2525–2536
Khurana J, Gartner SC, Naik L, Tsui BCH (2018) Ultrasound identification of diaphragm by novices using ABCDE technique. Reg Anesth Pain Med 43(2):161–165
Greenstein YY, Littauer R, Narasimhan M, Mayo PH, Koenig SJ (2017) Effectiveness of a critical care ultrasonography course. Chest 151(1):34–40
Bergamaschi V, Vignazia GL, Messina A, Colombo D, Cammarota G, Corte FD et al (2019) Transthoracic echocardiographic assessment of cardiac output in mechanically ventilated critically ill patients by intensive care unit physicians. Rev Bras Anestesiol. 69(1):20–26
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
Study conception and design: Eugenio Garofalo; Andrea Bruni; Corrado Pelaia; Giovanni Landoni; Alberto Zangrillo; Massimo Antonelli; Giorgio Conti; Daniele Guerino Biasucci; Giovanna Mercurio; Andrea Cortegiani; Antonino Giarratano; Luigi Vetrugno; Tiziana Bove; Francesco Forfori; Francesco Corradi; Rosanna Vaschetto; Gianmaria Cammarota; Marinella Astuto; Paolo Murabito; Valentina Bellini; Massimo Zambon; Federico Longhini; Paolo Navalesi; and Elena Bignami. Data acquisition and analysis: Eugenio Garofalo; Andrea Bruni; Giovanni Landoni; Daniele Guerino Biasucci; Giovanna Mercurio; Andrea Cortegiani; Luigi Vetrugno; Tiziana Bove; Francesco Forfori; Francesco Corradi; Rosanna Vaschetto; Gianmaria Cammarota; Marinella Astuto; Paolo Murabito; Valentina Bellini; and Massimo Zambon. Data interpretation: Eugenio Garofalo; Andrea Bruni; Corrado Pelaia; Giovanni Landoni; Alberto Zangrillo; Massimo Antonelli; Giorgio Conti; Andrea Cortegiani; Antonino Giarratano; Luigi Vetrugno; Tiziana Bove; Francesco Forfori; Francesco Corradi; Rosanna Vaschetto; Gianmaria Cammarota; Marinella Astuto; Paolo Murabito; Massimo Zambon; Federico Longhini; Paolo Navalesi; and Elena Bignami. Creation of the video tutorial: Eugenio Garofalo; Andrea Bruni; and Corrado Pelaia. Manuscript drafting and revision: Eugenio Garofalo; Andrea Bruni; Corrado Pelaia; Giovanni Landoni; Alberto Zangrillo; Massimo Antonelli; Giorgio Conti; Daniele Guerino Biasucci; Giovanna Mercurio; Andrea Cortegiani; Antonino Giarratano; Luigi Vetrugno; Tiziana Bove; Francesco Forfori; Francesco Corradi; Rosanna Vaschetto; Gianmaria Cammarota; Marinella Astuto; Paolo Murabito; Valentina Bellini; Massimo Zambon; Federico Longhini; Paolo Navalesi; and Elena Bignami. All authors have approved the submitted version, have agreed both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained by the coordinating center (Ethical Committee “Regione Calabria Area Centro”, Approval No. 179, 21st June 2018).
Consent for publication
Not applicable.
Competing interests
Dr. Navalesi’s research laboratory has received equipment and grants from Maquet Critical Care, Draeger and Intersurgical S.p.A. He also received honoraria/speaking fees from Maquet Critical Care, Orionpharma, Philips, Resmed, MSD and Novartis. Dr. Navalesi contributed to the development of the helmet Next, whose licence for patent belongs to Intersurgical S.P.A., and receives royalties for that invention. Dr. Longhini and Dr. Navalesi contributed to the development of a new device not discussed in the present study whose patent is in progress (European Patent Application Number EP20170199831). The remaining authors declared that they no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Theoretical test.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Garofalo, E., Bruni, A., Pelaia, C. et al. Comparisons of two diaphragm ultrasound-teaching programs: a multicenter randomized controlled educational study. Ultrasound J 11, 21 (2019). https://doi.org/10.1186/s13089-019-0137-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13089-019-0137-4