
Abstract
Background
Patients with obstructive sleep apnea (OSA) might be at risk of gout because of pathophysiological mechanisms that can lead to hyperuricemia and eventually gout or because of shared risk factors between both diseases. The objective of the present study was to investigate the risk of gout in patients with OSA.
Methods
A population-based case-control study using the UK Clinical Practice Research Datalink GOLD including all patients aged 40 years and older with a first diagnosis of gout between 1987 and 2014. Gout cases were matched by year of birth, sex, and practice to non-gout controls. Conditional logistic regression estimated the risk of gout with an earlier diagnosis of OSA. Analyses were adjusted for lifestyle factors, comorbidities, and recent drug use.
Results
One hundred eleven thousand five hundred nine cases were matched with 210,241 controls. Patients with OSA were at increased risk of gout (OR 1.86; 95%CI (1.71–2.02). However, this association disappeared (OR 1.05; 95% CI 0.96–1.16) after adjustment for smoking status, body mass index (BMI), alcohol use, a history of heart failure, diabetes mellitus, renal function, and recent use of diuretics and other medications. Among females with OSA and patients with OSA associated with heart failure, renal impairment, or higher BMI, the risk of gout was however still increased when compared to the total control population.
Conclusion
This study showed that the observed association between OSA and gout disappeared after adjustment.
Similar content being viewed by others


Introduction
Gout is the most common inflammatory arthritis [1], affecting up to 1–2% of adults, and leads to disability and reduced quality of life [2]. Gout is characterized by the deposition of monosodium urate (MSU) crystals in synovial fluids and other tissues. Individuals suffering from gout often have a complex profile of comorbidities, including cardiovascular disease, diabetes mellitus, and kidney disease [3]. One of the comorbidities in gout that has received more attention over the past years is obstructive sleep apnea (OSA) [4]. Various underlying mechanisms may explain an association between gout and OSA. First, OSA-induced hypoxemia causes a rise in adenosine triphosphate (ATP) degradation which eventually increases purine concentrations and their end product uric acid [5]. Second, hypercapnia and acidosis caused by OSA could influence the likelihood of MSU precipitation [6]. Third, excretion of lactic acid, generated during the hypoxic episodes in OSA, could result in a higher renal reabsorption of uric acid [7].
Alternatively, the relationship could also be explained by shared risk factors of gout and OSA, such as age, obesity, metabolic syndrome, renal impairment, and heart failure [8].
Two prospective studies in large United Kingdom (UK) primary care databases have demonstrated a 1.5-fold increased risk of developing gout among patients with OSA [4, 9] with the overall risk peaking 1 to 2 years after OSA diagnosis [9]. While both papers statistically adjusted their analyses for body mass index (BMI), type 2 diabetes mellitus, ischemic heart disease, hypertension, the use of diuretics of an unspecified class, and alcohol consumption, renal impairment was either ignored or considerably under-recorded [4]. Under-recording could be explained by selecting only medical diagnoses of chronic kidney disease (CKD), not taking > 30 million records of estimated glomerular filtration (eGFR) rates into consideration (that are available as of 2018) [4]. As CKD is a well-known risk factor for gout [10, 11], adequate statistical adjustment for this risk factor is important. Furthermore, both studies ignored the presence of heart failure, which is associated with both gout [12] and with sleep disorders, especially OSA [13].
The objective of the present study was to investigate the risk of gout in patients with OSA, while accounting for all relevant potential confounders, including CKD and heart failure.
Methods
Data source
Data for the present study were obtained from the Clinical Practice Research Datalink (CPRD) in the UK, previously known as the General Practice Research Database (http://www.cprd.com). CPRD contains the computerized medical records of approximately 13 million patients under the care of general practitioners (GPs) in the UK, representing 6.9% of the total UK population [14]. Practices contribute to CPRD only if their data quality meets research standards. Since 1987, data recorded in the CPRD include demographic information, prescription details, lifestyle parameters, clinical events, preventive care provided, and specialist referrals. CPRD has been extensively validated [15] and has been previously used to study gout [16].
Study population
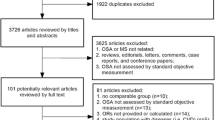
We conducted a population-based case-control study (Fig. 1). The cases consisted of all patients aged 40 years and older with a first diagnosis of gout during the period of valid data collection (from 1 January 1987 to 30 June 2014). Each case with gout was identified using READ codes [17]. READ codes are a set of clinical codes used in primary care in the UK for the registration of clinical diagnosis, processes of care (tests, screening, symptoms, patient administration, etc.), and medication. Each case with gout was matched by year of birth, sex, and practice to up to two randomly selected controls without a diagnosis of gout using incidence density sampling [18]. The date of the first recorded diagnosis of gout defined the index date for the cases and controls were assigned the same index date as their matched case. Cases and controls with a history of exposure to colchicine and uric acid-lowering therapy (ULT) (allopurinol, febuxostat, and/or uricosuric drugs) before the index date as well as their matched case or control were excluded.

Flow chart, study population
Exposure and potential confounders
Clinical READ codes were used to determine OSA exposure. Cases and controls with a read code for OSA before the index date were classified as being exposed to OSA.
The following variables were considered as potential confounders and were assessed prior to the index date: smoking status, BMI, alcohol use, socioeconomic status, a history of hypertension, diabetes mellitus (as recorded by either a diagnostic code for diabetes mellitus or a history of prescription(s) for anti-diabetic treatment, British National Formulary Chapters 6.1.1 and 6.1.2), hypercholesterolemia, postmenopausal status/hysterectomy, acute myocardial infarction, stroke, or heart failure. The use of the following medication was assessed in the 6 months before the index date: thiazide diuretics, loop diuretics, beta-blockers, calcium channel blockers, angiotensin-converting enzyme inhibitors (ACE-inhibitors), angiotensin II receptor blockers (ARBs), low-dose aspirin, statins, non-insulin antidiabetic drugs (NIADDs), insulin, or benzodiazepines. In addition, the most recent eGFR before the index date was assessed. Electronic lab test data were used to extract the eGFR. Furthermore, when only serum creatinine measurements were available, these were used to estimate the eGFR by the use of the abbreviated MDRD formula (186 × (serum creatinine/88.4)−1.154 × (age)−0.203 × (0.742 if female)). In addition, we identified diagnostic codes for stages of CKD. When there were multiple records on the same day, the best eGFR was chosen. The following categories were used to stratify for renal function by eGFR: CKD 1 (eGFR > 90 ml/min), CKD 2 (eGFR 60–89 ml/min), CKD 3 (eGFR 30–59 ml/min), CKD 4 (eGFR 15–29 ml/min), and CKD 5 (< 15 ml/min).
Statistical analysis
Conditional logistic regression was used to estimate the risk of gout associated with a diagnosis of OSA (SAS version 9.4, PHREG procedure). In the analyses, risk was expressed as odds ratios (OR) with corresponding 95% confidence intervals (CIs). Potential confounders were included in the final model if they independently changed the beta-coefficient for OSA by at least 5% or when a consensus about inclusion existed within the team of researchers, supported by clinical evidence from the literature. Missing data of confounders such as BMI, smoking status, alcohol use, and renal function were treated as separate levels using dummy variables. OSA exposure was further stratified by gender, age categories, and the presence of important confounders. Finally, we studied the effect of univariately adding the most important confounders to the main analyses as well as adjusting simultaneously for these confounders.
Results
Table 1 shows the baseline characteristics of the study population. The cohort encompassed 111,509 gout cases and 210,241 controls with a mean age of 62 years (standard deviation SD 13.3), of whom 27% were female. Gout cases had a higher BMI than controls (29 kg/m2 SD 5.3 in cases vs. 26.8 kg/m2 SD 4.8 in controls). On average, gout cases used alcohol more often (73.9% in cases vs. 65.5% in controls) and were more likely to be ex-smokers than controls (34.2% cases vs. 26% controls). With regard to comorbidities, gout cases more often had a history of hypertension, heart failure, or reduced renal function. They were also more frequently recent users of diuretics.
Patients with OSA had an almost doubled risk of gout (crude odds ratio [OR] 1.86; 95% confidence interval [CI] 1.71–2.02, Table 2). However, the effect disappeared after statistical adjustment for alcohol use, a history of diabetes mellitus, renal function, the most recently recorded eGFR measurement, heart failure, smoking status, BMI category, and recent use of statins, beta-blockers, ACE-inhibitors, ARBs, calcium channel blockers, loop diuretics, or thiazide diuretics (adjusted [adj.] OR 1.05; 95% CI 0.96–1.16). Further exploration identified that this shift was almost entirely explained by statistical adjustment for BMI, heart failure, recent use of diuretics, and renal function (Table 3).
Stratification of the fully adjusted models (Table 2) revealed that as compared to patients without OSA, those with OSA and with a high BMI remained at an increased risk of gout (BMI 30–34 kg/m2—adj. OR 1.34; 95% CI 1.13–1.59; BMI ≥ 35 kg/m2—1.56; 95% CI 1.33–1.83). Also, in comparison to patients without OSA, those with OSA and a history of heart failure had an almost doubled risk of gout (adj. OR 1.82; 95% CI 1.21–2.73). Furthermore, recent use of loop diuretics (adj. OR 1.73; 95% CI 1.33–2.26) and use of thiazide diuretics (adj. OR 1.85; 95% CI 1.47–2.33) was also associated with an increased risk of gout. The risk of gout among patients with OSA also further rose with increasing renal impairment (adj. OR 2.22; 95% CI 1.70–2.91 for CKD 3 (eGFR 30–59 ml/min), adj. OR 3.93; 95% CI 1.06–14.56 for CKD 4 (eGFR 15–29 ml/min) (Table 2). With regard to sex, women with OSA remained at an increased risk of gout in contrast to men with OSA (adj. OR 1.64; 95% CI 1.19–2.27).
Compared to patients without OSA, patients with OSA and diabetes mellitus had a statistically significant decreased risk of gout (adj. OR 0.70; 95%CI 0.58–0.85). Patients with OSA and hypercholesterolemia also had a 6% decreased risk, although not statistically significant (adj. OR 0.94; 95%CI 0.82–1.08).
Discussion
Our study showed that the almost doubled risk of gout with OSA disappeared after adequate statistical adjustment for BMI, renal function, heart failure, and recent use of diuretics. Notwithstanding, subgroups of patients with OSA, more specifically women and those with a history of heart failure, who had recently used diuretics, who had an eGFR between 59 and 15 ml/min, or who had a BMI above 30 kg/m2, still had a 2- to 4-fold increased risk of gout.
The absence of an overall association between OSA and gout in our study contrasts with a 1.5-fold increased risk of gout with OSA that was reported by two previous studies [4, 9] which had used the same data source, i.e., the CPRD GOLD database, or a data source (THIN) that partly overlaps with CPRD [19]. Table 3 shows that this difference can be largely explained by more comprehensive statistical adjustment for potential confounding in the current study, in particular for renal impairment, as measured by eGFR and READ codes, and heart failure. When renal function declines, less uric acid is excreted which leads to hyperuricemia and eventually gout [20] (Fig. 2).

Possible biological pathways linking OSA to gout. XOR, xanthine oxidoreductase; OSA, obstructive sleep apnea
Heart failure is probably under-recorded in large observational studies based on diagnostic codes [21]. Specific for the UK primary care databases, under-diagnosis might be related to manual coding of cardiology discharge letters by general practice staff. Therefore, we statistically adjusted our analyses for proxy indicators of heart failure such as recent use of diuretics. We also statistically adjusted our analysis for the use of other medications that are commonly used for heart failure, including beta-blockers, ACE-inhibitors, and ARBs [22]. Since (repeated) prescriptions, including outpatient prescriptions of cardiologists, are generally issued by GPs every 4 weeks, this proxy indicator is likely to be better captured and therefore more likely to further reduce the level of residual confounding. Notwithstanding, heart failure remained associated with gout, even after full adjustment. The explanation might be found in insufficient adjustment for the known increased xanthine oxidoreductase (XOR) activity in the myocardium of the failing heart which leads to an elevation of uric acid [23] (Fig. 2). Filippatos et al. demonstrated in their study that hyperuricemia was associated with poor outcomes in patients with heart failure without CKD but not in those with CKD, confirming the hypothesis that hyperuricemia in patients with heart failure could not only be explained by reduced uric acid excretion because of a poor kidney function [24]. Otaki et al. also demonstrated an association between XOR activity and severity and clinical outcomes in patients with heart failure [25]. Further evidence on a possible role of an increased XOR activity in heart failure can be found in studies demonstrating a beneficial effect of adding allopurinol to the treatment of patients with heart failure [26, 27]. This beneficial effect was not demonstrated with benzbromarone, which is a uricosuric drug and therefore decreases the uric acid concentration by increasing its excretion [28]. An alternative explanation for the independent contribution of heart failure to OSA can also be found in the influence of overnight rostral fluid shifts to the neck and lungs in patients with heart failure [29].
Unexpectedly, we found that the risk of gout with OSA disappeared in men after adjustment for confounders, while in women, the risk remained elevated. It is widely accepted that females are at lower risk of gout, as a result of the uricosuric effect of estrogens in women before menopause [30]. However, even after menopause, the risk in females remains lower and we can therefore assume that other causal factors probably play a role. Sex differences have also been noted in the prevalence and severity of OSA, with women presenting with less severe and less prevalent disease. These differences are decreased after menopause [31]. Differences in fat distribution, upper airway anatomy (in particular the posterior tongue region), mechanisms affecting ventilatory stability, and sex hormones might explain the differences between men and women in OSA [31]. In this line, it is of note that a study by Wang et al. showed that fat accumulation around the head measured by dual-energy X-ray absorptiometry was positively correlated with uric acid levels in women but not in men [32].
Obesity, which itself is associated with hypoxemia, is the main risk factor for the development of OSA. In more obese patients, OSA is aggravated with more severe oxygen desaturations and hypoxemia, which may explain why the risk of gout remains high in the highest BMI category [33, 34] (Fig. 2).
Our study had several limitations. First, there probably is underreporting of both OSA and gout, especially in the less severe cases [17, 35]. Misclassification of both exposure (OSA) and our outcome of interest, i.e., gout, is probably random and may therefore lead to regression towards null [36]. It could have masked a true association between OSA and gout among men. Among women, it could have masked a higher true association. With respect to confounders, although our data regarding renal function were more accurate, renal function is not routinely measured in primary care. This could lead to residual confounding. Another limitation in our study, which is present in all epidemiological studies where researchers try to estimate the total causal effect of an exposure on an outcome of interest, is the problem of potential over-adjustment. Ideally, one should not control for factors which lie in the causal pathway between exposure and outcome, as it leads to a regression of the risk towards null [37]. In our case, renal function could also be influenced by OSA itself as nocturnal hypoxemia present in OSA could accelerate the decline in kidney function and therefore reduce uric acid excretion and induce or exacerbate hyperuricemia and eventually the risk of gout [38]. Renal function would then be in the causal pathway from OSA to gout. Another limitation concerns the limited number of patients present in some subgroups, especially women and the groups with the worst CKD (CKD 4 and 5). The conclusion drawn from those results should therefore be interpreted with caution.
Our study had several strengths. First, we were able to include a large number of patients with gout and controls. The findings of this study are therefore likely to be generalizable to patients with gout and OSA in the total UK population [14]. Second, the large amount of clinical information routinely and longitudinally collected in clinical practice allowed us to statistically adjust for many potential confounders such as age, sex, smoking status, alcohol use, kidney function, comorbidity, and use of medication.
Conclusion/key message
This study showed that the observed association between OSA and gout disappeared after extensively adjusting for BMI, heart failure, diuretics, and renal function, in particular. As the latest guidelines for the treatment of gout by the British Society of Rheumatology recommend to discuss the use of ULT with every patient, even after a first attack of gout, we think that it is important that physicians are aware that gout occurs more frequently in the presence of various comorbidities, among which OSA. Our study also emphasizes the importance of using frequently recorded electronic lab test data to assess renal function in UK primary care data, rather than READ codes.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- OSA:
-
Obstructive sleep apnea
- BMI:
-
Body mass index
- MSU:
-
Monosodium urate
- ATP:
-
Adenosine triphosphate
- UK:
-
United Kingdom
- CKD:
-
Chronic kidney disease
- eGFR:
-
Estimated glomerular filtration
- CPRD:
-
Clinical Practice Research Datalink
- GP:
-
General practitioner
- ULT:
-
Uric acid-lowering therapy
- ACE-inhibitors:
-
Angiotensin-converting enzyme inhibitors
- ARBs:
-
Angiotensin II receptor blockers
- NIADDs:
-
Non-insulin antidiabetic drugs
- CI:
-
Confidence interval
- SD:
-
Standard deviation
- OR:
-
Odds ratio
- Adj.:
-
Adjusted
References
Harrold L, Mazor K, Peterson D, Naz N, Firneno C, Yood R. Patients’ knowledge and beliefs concerning gout and its treatment: a population based study. BMC Musculoskelet Disord. 2012;13:180.
Singh JA, Strand V. Gout is associated with more comorbidities, poorer health related quality of life and higher health care utilization in US veterans. Ann Rheum Dis. 2008;67(9):1310–6.
Robinson P, Merriman T, Herbison P, Highton J. Hospital admissions associated with gout and their comorbidities in New Zealand and England 1999-2009. Rheumatology. 2013;52(1):118–26.
Zhang Y, Peloquin CE, Dubreuil M, Roddy E, Lu N, Neogi T, et al. Sleep apnea and the risk of incident gout: a population-based, body mass index-matched cohort study. Arthritis Rheumatol (Hoboken, NJ). 2015;67(12):3298–302.
Saito H, Nishimura M, Shibuya E, Makita H, Tsujino I, Miyamoto K, et al. Tissue hypoxia in sleep apnea syndrome assessed by uric acid and adenosine. Chest. 2002;122(5):1686–94.
Abrams B. High prevalence of gout with sleep apnea. Med Hypotheses. 2012;78(2):349.
Kanbay A, Inonu H, Solak Y, Erden A, Uslu E, Yuksel SA, et al. Uric acid as a potential mediator of cardiovascular morbidity in obstructive sleep apnea syndrome. Eur J Intern Med. 2014;25(5):471–6.
Jennum P, Riha RL. Epidemiology of sleep apnoea/hypopnoea syndrome and sleep-disordered breathing. Eur Respir J. 2009;33(4):907–14.
Blagojevic-Bucknall M, Mallen C, Muller S, Hayward R, West S, Choi H, et al. The risk of gout among patients with sleep apnea: a matched cohort study. Arthritis Rheumatol (Hoboken, NJ). 2019;71(1):154–60.
van Durme C, van Echteld IA, Falzon L, Aletaha D, van der Heijde DM, Landewe RB. Cardiovascular risk factors and comorbidities in patients with hyperuricemia and/or gout: a systematic review of the literature. J Rheumatol Suppl. 2014;92:9–14.
Lee YC, Hung SY, Wang HK, Lin CW, Wang HH, Chen SW, et al. Sleep apnea and the risk of chronic kidney disease: a nationwide population-based cohort study. Sleep. 2015;38(2):213–21.
Krishnan E. Gout and the risk for incident heart failure and systolic dysfunction. BMJ Open. 2012;2(1):e000282.
Herrscher TE, Akre H, Overland B, Sandvik L, Westheim AS. High prevalence of sleep apnea in heart failure outpatients: even in patients with preserved systolic function. J Card Fail. 2011;17(5):420–5.
Herrett E, Gallagher AM, Bhaskaran K, Forbes H, Mathur R, van Staa T, et al. Data resource profile: Clinical Practice Research Datalink (CPRD). Int J Epidemiol. 2015;44(3):827–36.
Herrett E, Thomas SL, Schoonen WM, Smeeth L, Hall AJ. Validation and validity of diagnoses in the General Practice Research Database: a systematic review. Br J Clin Pharmacol. 2010;69(1):4–14.
Wijnands JM, van Durme CM, Driessen JH, Boonen A, Klop C, Leufkens B, et al. Individuals with type 2 diabetes mellitus are at an increased risk of gout but this is not due to diabetes: a population-based cohort study. Medicine. 2015;94(32):e1358.
Meier CR, Jick H. Omeprazole, other antiulcer drugs and newly diagnosed gout. Br J Clin Pharmacol. 1997;44(2):175–8.
Spaetgens B, de Vries F, Driessen JHM, Leufkens HG, Souverein PC, Boonen A, et al. Risk of infections in patients with gout: a population-based cohort study. Sci Rep. 2017;7(1):1429.
Carbonari DM, Saine ME, Newcomb CW, Blak B, Roy JA, Haynes K, et al. Use of demographic and pharmacy data to identify patients included within both the Clinical Practice Research Datalink (CPRD) and The Health Improvement Network (THIN). Pharmacoepidemiol Drug Saf. 2015;24(9):999–1003.
Prasad Sah OS, Qing YX. Associations between hyperuricemia and chronic kidney disease: a review. Nephrourol Mon. 2015;7(3):e27233–e.
McCormick N, Lacaille D, Bhole V, Avina-Zubieta JA. Validity of heart failure diagnoses in administrative databases: a systematic review and meta-analysis. PLoS One. 2014;9(8):e104519.
Koudstaal S, Pujades-Rodriguez M, Denaxas S, Gho J, Shah AD, Yu N, et al. Prognostic burden of heart failure recorded in primary care, acute hospital admissions, or both: a population-based linked electronic health record cohort study in 2.1 million people. Eur J Heart Fail. 2017;19(9):1119–27.
Gustafsson D, Unwin R. The pathophysiology of hyperuricaemia and its possible relationship to cardiovascular disease, morbidity and mortality. BMC Nephrol. 2013;14:164.
Filippatos GS, Ahmed MI, Gladden JD, Mujib M, Aban IB, Love TE, et al. Hyperuricaemia, chronic kidney disease, and outcomes in heart failure: potential mechanistic insights from epidemiological data. Eur Heart J. 2011;32(6):712–20.
Otaki Y, Watanabe T, Kinoshita D, Yokoyama M, Takahashi T, Toshima T, et al. Association of plasma xanthine oxidoreductase activity with severity and clinical outcome in patients with chronic heart failure. Int J Cardiol. 2017;228:151–7.
Cappola TP, Kass DA, Nelson GS, Berger RD, Rosas GO, Kobeissi ZA, et al. Allopurinol improves myocardial efficiency in patients with idiopathic dilated cardiomyopathy. Circulation. 2001;104(20):2407–11.
Malek F, Ostadal P, Parenica J, Jarkovsky J, Vitovec J, Widimsky P, et al. Uric acid, allopurinol therapy, and mortality in patients with acute heart failure--results of the Acute HEart FAilure Database registry. J Crit Care. 2012;27(6):737 e11–24.
Ogino K, Kato M, Furuse Y, Kinugasa Y, Ishida K, Osaki S, et al. Uric acid-lowering treatment with benzbromarone in patients with heart failure: a double-blind placebo-controlled crossover preliminary study. Circ Heart Fail. 2010;3(1):73–81.
Lyons OD, Bradley TD. Heart failure and sleep apnea. Can J Cardiol. 2015;31(7):898–908.
Pui K, Waddell C, Dalbeth N. Early onset of hyperuricaemia and gout following treatment for female to male gender reassignment. Rheumatology (Oxford, England). 2008;47(12):1840–1.
Wimms A, Woehrle H, Ketheeswaran S, Ramanan D, Armitstead J. Obstructive sleep apnea in women: specific issues and interventions. Biomed Res Int. 2016;2016:1764837.
Wang XC, Liu H, Huang YY, Sun H, Bu L, Qu S. Head fat is a novel method of measuring metabolic disorder in Chinese obese patients. Lipids Health Dis. 2014;13:113.
Parameswaran K, Todd DC, Soth M. Altered respiratory physiology in obesity. Can Respir J. 2006;13(4):203–10.
Peppard PE, Ward NR, Morrell MJ. The impact of obesity on oxygen desaturation during sleep-disordered breathing. Am J Respir Crit Care Med. 2009;180(8):788–93.
Kapur V, Strohl KP, Redline S, Iber C, O'Connor G, Nieto J. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep Breath. 2002;6(2):49–54.
Jurek AM, Greenland S, Maldonado G, Church TR. Proper interpretation of non-differential misclassification effects: expectations vs observations. Int J Epidemiol. 2005;34(3):680–7.
Schisterman EF, Cole SR, Platt RW. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology (Cambridge, Mass). 2009;20(4):488–95.
Ahmed SB, Ronksley PE, Hemmelgarn BR, Tsai WH, Manns BJ, Tonelli M, et al. Nocturnal hypoxia and loss of kidney function. PLoS One. 2011;6(4):e19029.
Acknowledgements
None
Funding
There was no funding for this study.
Author information
Authors and Affiliations
Contributions
CD, BS, MS, AB, and FV conceived the study. Analysis was undertaken by CD, JD, and JN. All authors were involved in the design, interpretation of data, and drafting, revising, and final approval of the manuscript. FV is the guarantor and affirms that the manuscript is an honest, accurate, and transparent account of the study being reported and that no important aspects of the study have been omitted. There are no discrepancies from the study as planned. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
CPRD has been granted Multiple Research Ethics Committee approval (05/MRE04/87) to undertake purely observational studies with external data linkages, including ONS mortality data. The present study is based on anonymized and unidentifiable CPRD data and is also approved by the Independent Scientific Advisory Committee (ISAC) of the Medicine and Healthcare products Regulatory Agency (protocol number 14_231R), which is primarily responsible for reviewing the study protocols. In the case of this observational research, no further ethical approval was deemed necessary by ISAC.
Consent for publication
This manuscript does not contain any individual data.
Competing interests
FV currently supervises two PhD students who are employed with F. Hoffmann La Roche Ltd. (Basel, Switzerland and Welwyn Garden City, UK). He has not received any feeds or reimbursements for this. The topics of their PhD theses do not relate to the current manuscript.
MS received speakers’ fees for a lecture on obstructive sleep apnea from the European Academy of Dental Sleep Medicine (2015) as well as for a lecture on COPD and Sleep from Astra Zeneca (2016).
CvD received speakers’ fees for lectures on gout and advisory board (Grünenthal) and speaker fees for a lecture on biosimilars (Amgen). The topic of the lecture and the advisory board on gout was not related to the topic of the present article.
BS: none to declare
JN: none to declare
JD: none to declare
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
van Durme, C., Spaetgens, B., Driessen, J. et al. Obstructive sleep apnea and the risk of gout: a population-based case-control study. Arthritis Res Ther 22, 92 (2020). https://doi.org/10.1186/s13075-020-02176-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13075-020-02176-1