
Abstract
Background
Echinococcosis is a parasitic zoonotic disease that threatens human health and economic development. In China, 370 counties are endemic for echinococcosis. Qinghai-Tibet Plateau has the most patients and people at risk. Therefore, analyzing the societal factors related to susceptibility to the disease is critical for efficient prevention and control of echinococcosis.
Methods
The demographic characteristics and lifestyle of echinococcosis cases were clustered using K-means cluster analysis to determine the main factors of risk of echinococcosis.
Results
Middle-aged and young people as well as those with a low education level and herdsmen are at risk of contracting echinococcosis. Nomadism, domestic and feral dogs in the surrounding environment, and drinking heavily polluted natural surface water are the main behavioral risk factors. The cystic echinococcosis (CE) and alveolar echinococcosis (AE) cluster analysis focused on female, middle-aged, and young people, winter settlement and summer nomadism, and domestic and feral dogs in the surrounding environment. There were significant differences in lifestyle between Qinghai-Tibet Plateau cases and non-Qinghai-Tibet-Plateau cases.
Conclusion
According to the distribution of cases and CE and AE, this study identified the factors of risk of echinococcosis in the Qinghai-Tibet Plateau and non-Qinghai-Tibet Plateau. Adapted control techniques appropriate for the various epidemic areas should be established to serve as a reference for echinococcosis prevention.
Graphical Abstract

Similar content being viewed by others


Introduction
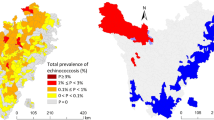
Echinococcosis is a zoonotic parasitic disease caused by the larval stages of cestodes of Echinococcus found in humans and animals. China is one of the countries with the most serious epidemics of echinococcosis worldwide. There are two types of echinococcosis epidemics: cystic echinococcosis (CE) caused by the larvae of Echinococcus granulosus and alveolar echinococcosis (AE) caused by the larvae of Echinococcus multilocularis [1]. Echinococcosis is primarily found in pastoral or semi-agricultural-semi-pastoral areas in Western China, affecting 370 counties in provinces or autonomous regions such as Inner Mongolia, Yunnan, Tibet, Sichuan, Gansu, Qinghai, Ningxia, Xinjiang, and Shaanxi [2]. China echinococcosis endemic areas are separated into Qinghai-Tibet Plateau endemic areas and non-Qinghai-Tibet Plateau endemic areas based on geography and landform. There are 148 endemic counties on the Qinghai-Tibet Plateau, including all 74 counties in Tibet, 30 counties in Qinghai Province, 32 counties in Sichuan Province, 9 counties in Gansu Province, and 3 counties in Yunnan Province, while there are 222 endemic counties on the non-Qinghai-Tibet Plateau. The Qinghai-Tibet Plateau is the “hot spot” in terms of prevalence of human echinococcosis in China [2]. The epidemiological assessment of echinococcosis conducted from 2012 to 2016 reported the average detection rate of echinococcosis in the population of 1.28% in the Qinghai-Tibet Plateau and the non-Qinghai-Tibet Plateau with an average detection rate of 0.13% [3]. The detection rate in the Qinghai-Tibet Plateau is almost 10 times that in the non-Qinghai-Tibet Plateau because of animal husbandry and specific economy, culture, and production lifestyles [4]. Echinococcosis not only endangers people’s health and life but also stifles the healthy growth of agriculture and animal husbandry economies [5]. It is also one of the primary reasons why people in these epidemic areas “become poor and return to poverty” [6].
CE mostly damages and impairs the target organs of the liver, lungs, brain, spleen, kidneys, and heart, etc. [7]. CE’s liver cysts grow slowly, and population screening showed that more than half of the liver cysts did not change in size for 10 years. In addition, the early stages of CE and AE do not cause symptoms, and the lesions of CE and AE could remain asymptomatic for 10–15 years [8, 9]. AE, often known as “worm cancer,” is more dangerous than CE with a faster growth and death rate of up to 90% within 10 years if untreated or improperly treated [10, 11]. The cyst grows and ruptures as the disease advances, resulting in lethal anaphylactic shock. CE in China accounts for 40% of the disease burden worldwide, with as much as 398,000 disability-adjusted life years (DALYs) [12]. AE in China accounts for 90% of total cases and 91% of new cases worldwide [13].
In susceptible populations, echinococcosis can create major medical, social, and economic difficulties. The identification of susceptible populations is thus critical for prevention and control. Similarly, properly targeting health education to the most susceptible population will also help reduce or eliminate risk factors and improve the efficiency of echinococcosis prevention and control. It will also help optimize the allocation of public health resources. Most communities in the Qinghai-Tibet Plateau are Tibetans, and their lifestyles and customs differ from those of non-Qinghai-Tibet Plateau communities. Correlations were found between gender, age, education, occupation, and other societal traits and echinococcosis. However, most studies focused on only one population feature, and the other population characteristics were insufficiently detailed. One study used clustering analysis to identify vulnerable populations but only according to human demographics in Tibet Autonomous Region [14]. Thus, this work was undertaken as a comparative analysis of echinococcosis cases from Qinghai-Tibet Plateau and non-Qinghai-Tibet Plateau integrating together gender, age, education, occupation, and societal aspects.
Materials and methods
Source of data
Demographic information (gender, age, education, occupation, etc.) of echinococcosis patients, but also societal information (lifestyle, drinking water source, neighbors own dogs, feral dogs in the surrounding environment, and slaughter types) were collected from 2012 to 2016 in 370 endemic counties by cross-sectional cluster sampling. Human echinococcosis cases were identified using China's approved “Diagnostic criteria for echinococcosis” (WS 257–2006) by using portable B-mode ultrasonography, a standard in line with that of WHO [15]. Suspected cases were confirmed by two positive serological tests [15]. A questionnaire was used to collect the related life behavior factors of patients. Cases are standardized by gender, age, education, occupation, and other factors based on diagnosed cases (Table 1). Drinking water sources was classified according to the degree of cleanliness as level 1 (tap water and well water), level 2 (river water and spring water), and level 3 (water accumulation, ditch water, ponding).
Statistical analyses
Analyses were conducted using the SPSS 21.0 software package (IBM, Armonk, NY, USA). A chi-square test was used to compare the lifestyle composition of cases from Qinghai-Tibet Plateau and non-Qinghai-Tibet Plateau. Clustering analysis was used to group data objects as previously described [16]. The k-means algorithm was used to separate n objects into k clusters, each having a high similarity of data objects, whereas data objects inside the other clusters are less similar [17].
The procedure was the following [18]:
-
(i)
Any k point was chosen as the initial cluster center.
-
(ii)
The distance between the remaining points and the cluster center was calculated based on the minimum distance, as follows:
$$dis(xi,xj)=\sqrt{{{\sum }_{d=1}^{D}({x}_{i,d} ,{x}_{j,d})}^{2}}$$ -
(iii)
A new cluster center was calculated for each cluster.
-
(iv)
Steps (ii) and (iii) were repeated until no new cluster centers could be created.
R 4.0.0 was used (R Development Core Team; R Foundation for Statistical Computing; Vienna, Austria) for k-means clustering.
Results
General situation
There were 4323 cases, including 1811 men and 2512 women, with a sex ratio of 1:1.39, accounting for 41.89% and 58.11% of cases, respectively. The youngest patient was 2 years old and the oldest 95 years old with a median age of 42. The Qinghai-Tibet Plateau was the host of 3286 cases while 1037 cases were found in the non-Qinghai-Tibet Plateau area (Table 2). CE represented 3194 cases, and AE was responsible for 1064 cases (Table 2). There were 65 cases of co-infections with CE and AE. In analysis CE cases comprised confirmed CE cases and co-infections with CE and AE. Similarly, AE cases included confirmed AE cases and co-infections with CE and AE.
Identification of common risk factors for both CE and AE
The cluster analysis was performed on Qinghai-Tibet Plateau and non-Qinghai-Tibet Plateau cases, respectively. Each ring was built from the inside out based on proportion, gender, age, education, and occupation (Fig. 1).

Cluster results of vulnerable populations in the Qinghai-Tibet Plateau and non-Qinghai-Tibet Plateau
Cluster analysis of populations at risk in the Qinghai-Tibet Plateau
The range of k-clusters was defined as 2–7 [19, 20]. After determining the best k value, the instances from Qinghai-Tibet Plateau were grouped using k = 4 as the optimal cluster number (Fig. 1a). The first cluster comprised 1672 cases, essentially composed of women in age class 2, i.e. 21–64 years old, and illiterate herders (Fig. 1a). The second cluster comprised 730 cases, the majority being women under the age of 21 and with only primary school education (Fig. 1a). The third cluster was made of 675 individuals who were primarily women in age class 2 (21–64 years old), having a primary school education and working with herders. The last cluster comprised 209 individuals, the majority being men in age class 2 (21–64 years old) with a low educational level (primary school) and a religious profession.
Cluster analysis of populations at risk in the non-Qinghai-Tibet Plateau
Four clusters were also found in the non-Qinghai-Tibet Plateau (Fig. 1b). The first one comprised 353 cases, mostly women and farmers of age class 2 (21–64 years) with primary school education. The second cluster grouped 296 individuals, mostly male farmers of age class 2 with elementary and junior middle school education. The 286 individuals making the third cluster were mostly elderly women in class age 3 (≥ 65 years old), uneducated and farmers. The last cluster included 102 cases comprised mostly men of age class 2 (21–64 years old), educated in junior high and senior high school, and having diverse occupational activities.
Clustering according to lifestyle
Cluster analysis of CE cases
There were 3259 CE cases (including co-infection of CE and AE). Four clusters were found (Fig. 2a). The first comprised 1062 individuals, mostly women in age class 2 (21–64), living in a winter settlement and summer nomadic lifestyle, with dogs in the vicinity and feral dogs in surrounding areas. The second cluster grouped 506 cases, also mostly women in age class 2 (21–64), living in a permanent residence, without dogs in the vicinity but with feral dogs in surrounding areas. The third cluster gathered 982 individuals and corresponded to women in age class 2, living in permanent settlements with dogs in the vicinity and feral dogs in the surrounding environment. The last cluster comprised 709 individuals, mostly women again but from age class 3 (≥ 65 years old), also living in permanent settlements, with both domestic dogs in the vicinity and feral dogs in the surrounding environment.

Clustering results for susceptible populations in CE and AE cases
Cluster analysis AE cases
There were 1129 AE cases (including co-infection of CE and AE). Only three clusters were identified in the case of AE (Fig. 2b). The first cluster comprised 290 cases, mostly women in age class 1 (< 21 years old), living in permanent settlements with dogs in the vicinity and feral dogs in the surrounding environment. The second cluster grouped 608 individuals, also mostly women but in age class 2 (21–64 years old) with a lifestyle of permanent winter residence and summer nomadism and with domestic dogs in the vicinity and feral dogs in the surrounding environment. The last cluster grouped 231 individuals and predominantly comprised men in age class 2 (21–64 years old) in permanent settlements and with domestic dogs in the vicinity and feral dogs in the surrounding area.
Lifestyle and human echinococcosis
The lifestyle patterns of human echinococcosis cases of Qinghai-Tibet Plateau and non-Qinghai-Tibet Plateau were analyzed using the following parameters: living patterns (permanent or nomadic), drinking water sources, neighborhood domestic dogs situation, and presence of feral dogs in the environment.
Lifestyle clustering analysis of Qinghai-Tibet Plateau cases
There were 2251 CE cases in Qinghai-Tibet Plateau (including co-infection of CE and AE). We used k = 3 as the best clustering number to cluster CE cases in Qinghai-Tibet Plateau (Fig. 3). There were 1152 cases in the first category, concentrated in groups whose lifestyle was winter residence and summer nomadism, drinking water cleanliness was level 2, neighbors had dogs, and there were feral dogs in the surrounding area. The settlement lifestyle, level 2 and 3 drinking water cleanliness, and domestic and feral dogs in the surrounding environment were factors in the 997 cases in the second category. There were 102 cases in the third category, mainly concentrated in groups where the living style was settlement, there was drinking water level 1 cleanliness, neighbors had no domestic dogs, and the surrounding environment had no feral dogs. For AE, there were 1076 AE cases in Qinghai-Tibet Plateau (including co-infection of CE and AE). There were 458 cases in the first category, concentrated in groups whose lifestyle was winter residence and summer nomadism, drinking water cleanliness was level 2, and neighbors had dogs and feral dogs in the surrounding area. Nomadic lifestyle, level 2 and 3 drinking water cleanliness, and domestic and feral dogs present in the surrounding environment were factors in the 376 cases in the second category. There were 242 cases in the third category, concentrated in groups where the lifestyle was: settlement, level 1 drinking water cleanliness, neighbors having dogs, and feral dogs in the surrounding environment.

Results of lifestyle clustering in cases for CE and AE in Qinghai-Tibet Plateau
Lifestyle clustering analysis of non-Qinghai-Tibet Plateau cases
There were 1008 CE cases in non-Qinghai-Tibet Plateau (including co-infection of CE and AE). The findings of clustering cases for CE in non-Qinghai-Tibet Plateau with k = 3 as the optimal clustering number are displayed in Fig. 4. In the first group, there were 510 cases, concentrated in the population who had settlement lifestyle, level 1 cleanliness of drinking water, neighbors with dogs, and no feral dogs in the surrounding environment. In the second category, there were 406 cases, concentrated in groups with a settled lifestyle, level 1 cleanliness of drinking water, neighbors with dogs, and feral dogs in the surrounding environment. There were 92 cases in the third group, concentrated in groups with a settled lifestyle, level 3 cleanliness of drinking water, neighbors with dogs, and no feral dogs in the surrounding environment. For AE, there were 53 AE cases in non-Qinghai-Tibet Plateau (including co-infection of CE and AE). In the first group there were 20 cases, concentrated in the population with settled lifestyle, level 2 cleanliness of drinking water, neighbors with dogs, and feral dogs in the surrounding environment. In the second category, there were 13 cases, concentrated in groups with a settled lifestyle, level 3 cleanliness of drinking water, neighbors with dogs, and feral dogs in the surrounding environment. There were 13 cases in the third group, concentrated in groups with a settled lifestyle, level 1 cleanliness of drinking water, neighbors with dogs, and no feral dogs in the surrounding environment. Seven cases in the fourth category were primarily concentrated in the population whose lifestyle consisted of winter residence and summer nomadism, the purity of drinking water was secondary water, neighbors owned dogs, and feral dogs in the surrounding environment.

Results of lifestyle clustering in cases of CE and AE in non-Qinghai-Tibet Plateau
Comparison of behavior patterns in Qinghai-Tibet Plateau and non-Qinghai-Tibet Plateau cases
Summer nomadism and winter permanent settlements were more frequent in the Qinghai-Tibet plateau cases than in non-Qinghai-Tibet Plateau ones. The proportion of cleanliness levels 2 and 3 of drinking water source selection was higher in Qinghai-Tibet plateau cases than in the non-Qinghai-Tibet Plateau ones; for the latter, the proportion of cleanliness level 1 was higher. As indicated in Table 3, the presence of domestic dogs in the neighborhood and that of feral dogs in the surrounding environment were higher on the Qinghai-Tibet Plateau than the non-Qinghai-Tibet Plateau. In Qinghai-Tibet Plateau, the families of the 1202 cases (36.6%) did not choose to slaughter livestock. Among the families, a total of 1101 (33.5%) cases chose to slaughter livestock at home. Only the families of 146 cases (4.4%) chose to slaughter animals in centralized facilities, while the families of 837 (25.5%) cases used sporadic random livestock slaughter. A total of 276 non-Qinghai-Tibet Plateau subjects (26.6%) did not slaughter livestock. As stated in Table 3, the families of 551 subjects (53.1%) chose to slaughter livestock at home, and the families of 133 (12.8%) cases were involved in intensive slaughter.
Discussion
The specific characteristic of the echinococcosis epidemic in China is that dogs are the common source of infection for both CE and AE. CE and AE display common risk factors with 115 counties endemic for both diseases. The natural and geographical environment, climate, and customs of the Qinghai-Tibet Plateau are different from those of the non-Qinghai-Tibet Plateau, as are the transmission cycles of E. granulosus and E. multilocularis. Population characteristics and risk factors in the Qinghai-Tibet Plateau and in the non-Qinghai-Tibet Plateau regions are thus also different. Some risk factors are similar in both regions, such as middle-aged populations, low education level, and occupations as herdsman or farmers [14]. Within the Qinghai-Tibet Plateau some groups at risk of CE and AE are similar: middle-aged, low-educated women who spend most of their time at home [21]. They frequently feed dogs and livestock, collect cow dung for fuel, shear wool, and perform other household duties. Therefore, they are extremely susceptible to E. granulosus and E. multilocularis [21] infection. Age and low education level are risk factors for echinococcosis based on community studies conducted in Argentina [22]. According to an epidemiological survey conducted in Chile, poor socioeconomic status and lack of education have also been linked to CE in humans [23].
In both the Qinghai-Tibet Plateau and the non-Qinghai-Plateau, the susceptibility factors for echinococcosis are centered on children. However, in the former, children accounted for 15%, while in the latter 6.94%. Because of the pastoral lifestyle and conditions, children are expected to help with household duties from a young age. The process involves contact with cattle and possible direct or indirect contact with dogs, which is exacerbated by inadequate local sanitation and lack of hygiene awareness among children. There is thus a considerable chance of contracting echinococcosis. Unlike schistosomiasis, malaria, and other parasitic infections, echinococcosis has a slow onset and hidden course. Most patients have been infected as children and are very vulnerable since the symptoms are unclear and difficult to detect and treat [24].
Therefore, improving surveillance, prevention, and control of echinococcosis infection in children is critical. It is possible to carry out serological and ultrasonic imaging examinations for echinococcosis as well as health education programs in schools on a regular basis. It is crucial to expand health education and raise public awareness of echinococcosis prevention and control. Religious practices, in particular when associated with poor education, might be an aggravating factor in the Qinghai-Tibet Plateau. People in this region are Buddhists and thus praise and highly respect all life forms. Lamas in temples will often take in or feed abandoned stray dogs, leading to a higher concentration of these dogs, which represent a major risk of infection near temples [20, 21].
The drinking water source is also a major risk factor [25]. Echinococcus granulosus eggs can only be inactivated after being stored at −80 °C for at least 7 days, and they can survive for > 200 days at 7 °C and 50 days at 21 °C [26]. Echinococcus multilocularis eggs can also survive in water at 4 °C for 16 months [27]. Parasitic eggs are very resistant in the environment and can even withstand common disinfectants. Boiling is the most effective method to inactivate Echinococcus eggs [21]. Therefore, drinking water is the most common path of echinococcosis infection [28]. Springs, rivers, ponds, and ditches, but also wells and even tap water, can be polluted by Echinococcus eggs in dog feces. The traditional Tibetan lifestyle of many people in the Qinghai-Tibet Plateau is to settle in the winter in permanent residences and to follow a nomadic lifestyle in summer. During this nomadic period, people and dogs share the same water supply, which is not boiled, tap or well water as well as surface water, such as springs and rivers, which are often of poor quality. Echinococcus eggs in dog feces are likely to pollute surface water. Indeed, nomadic herders often prefer pastures with natural water sources to set up tents, and livestock and dog excrement is randomly discharged in the area, polluting the surrounding water sources [29]. Drinking or using contaminated surface water increases the risk of infection. Furthermore, herdsmen traditionally collect cow dungs as fuel, which will be brought into tents for usage [30]. These customs also increase the risk of infection with echinococcosis. Of course, drinking clean water minimizes the risk of infection, and thus tap water is an echinococcosis protective factor [21, 31, 32]. However, it is not compatible with the traditional semi-nomadic way of life.
Although most patients in the non-Qinghai-Tibet Plateau tend to drink cleaner water, economic development in some places is lagging. Water storage is still part of a traditional lifestyle, so water purity cannot be ensured. However, building water pipelines in CE- and AE-endemic areas is challenging because of geographical and climatic factors, particularly on the Qinghai-Tibet Plateau. Depending on local economic and environmental conditions, appropriate actions should be taken to disinfect and treat local household water, improve water source management, and install disinfection or filtration units to enable local populations to access safe domestic water as well as limit the danger of exposure to Echinococcus eggs.
On Qinghai-Tibet Plateau, the presence of many both domestic and feral dogs greatly increases the risk of contamination, in particular for children. Their health awareness is low, and they lack prevention expertise. As aggravating factors, geographical characteristics in endemic areas, adverse climatic conditions, and economic factors make access to clean drinking water problematic, thus increasing the likelihood of infection in children. Most studies revealed the presence of both feral dogs and domestic dogs, particularly on the Qinghai-Tibet Plateau. However, feral dogs are less common in non-Tibetan societies, probably because of different cultural backgrounds [33]. Canines are the ultimate hosts of Echinococcus, and their faeces contain Echinococcus eggs and can contaminate the environment and water sources, as does animal hair [34]. A survey of domestic dogs in an epidemic area showed the presence of positive Echinococcus antigens in 4.25% of dog feces [5]. Feral dogs are also prevalent in CE- and AE-endemic areas [35, 36]. Dog management and control are critical measures in preventing and controlling echinococcosis as the zoonotic risk of CE and AE increases with the number of dogs and time dogs are maintained [21]. Tibet Autonomous Region has implemented comprehensive prevention and control measures focusing on controlling the infectious source of echinococcosis and achieved good results [37]. The Tibetan semi-nomadic way of life is unique and should be maintained. However, it should include efficient control measures related to animal husbandry and dogs; otherwise, echinococcosis will remain a severe human concern [30]. However, these control measures are difficult to implement.
The main source of income in the agricultural and pastoral areas is livestock raising, which uses dogs to look after and protect herds. Cattle and sheep are also intermediate hosts of E. granulosus. During domestic and sporadic slaughtering, the internal organs of livestock are generally fed to dogs along with the parasites they may contain [36]. In-house slaughter represents a 4.67 times higher risk of echinococcosis [38]. Centralized slaughter can successfully cut off this transmission pathway, reducing the risk of dog illness and thus safeguarding the health of residents. The first strategy for preventing and controlling echinococcosis is to decrease or destroy Echinococcus eggs, and the second is to reduce the probability of interaction with Echinococcus eggs [39]. Human proximity to definitive hosts (dogs) and animal intermediate hosts (livestock or small mammals) will increases the potential risk of echinococcosis (CE and AE) [30].
Non-Qinghai-Tibet Plateau is dominated by CE prevalence. The lifestyle of local residents is different from that of residents in the Qinghai-Tibet Plateau, being mainly settled. So they have access to clean tap drinking water. In this case, the main risk factor for CE is the presence of domestic and feral dogs. Because the geographical and natural environment is different from that of the Qinghai-Tibet Plateau, the main risk factors for AE are dogs in the surrounding environment and unclean drinking water.
Canine deworming and health education, particularly for vulnerable communities, are essential to enhance their understanding of the mechanisms of infection and improve inadequate hygiene practices. This study does have some drawbacks. The collection of influencing factors was limited, such as for CE, the infection rate of livestock, and for AE, the infection rate of small rodents.
Conclusion
In this study, the k-means clustering analysis revealed that the populations susceptible to echinococcosis were mostly middle-aged, poorly educated semi-nomadic herdsmen. However, on Qinghai-Tibet Plateau a specific group of patients was young pupils. This is a serious signal that special attention must be paid to this group. We should increase their health education and raise their awareness about avoiding and controlling echinococcosis. Adapting some traditions and lifestyles might be important to reduce the risk of infection. Simultaneously, in light of risk factors such as feral dogs, dog breeding, polluted drinking water, and domestic animal slaughter practices, we should increase management measures, improve relevant health regulations, improve sanitation conditions, and provide adequate technology for water purification, centralized slaughter, monitoring, and deworming.
Availability of data and materials
The original contributions presented in the study are included in the article material; further inquiries can be directed to the corresponding author.
Abbreviations
- AE:
-
Alveolar echinococcosis
- CE:
-
Cystic echinococcosis
- DALYs:
-
Disability-adjusted life years
References
Mcmanus DP, Zhang W, Li J, Bartley PB. Echinococcosis. Lancet. 2003;362:1295–304.
Wang LY, Qin M, Liu ZH, Wu WP, Xiao N, Zhou XN, et al. Prevalence and spatial distribution characteristics of human echinococcosis in China. PLoS Negl Trop Dis. 2021;15:e0009996.
Wu WP, Wang H, Wang Q, Zhou XN, Wang LY, Zheng CJ, et al. A nationwide sampling survey on echinococcosis in China during 2012–2016. Chin J Parasitol Parasit Dis. 2018;36:1–14.
Jiang CP. Today’s regional distribution of echinococcosis in China. Chin Med J. 2002;115:1244–7.
Wang Q, Francis R, Christine B, Philip SC, Xiao YF, Dominique A, et al. Grass height and 525 transmission ecology of echinococcus multilocularis in Tibetan communities. Chin Med J 526 (Engl). 2010;123:61–7.
Thompson RC. Biology and systematics of echinococcus. Adv Parasitol. 2017;95:65–109.
Brunetti E, Kern P, Vuitton DA. Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010;114(1):1–16.
Frider B, Larrieu E, Odriozola M. Long-term outcome of asymptomatic liver hydatidosis. J Hepatol. 1999;30:228–31.
Wen H, Vuitton L, Tuxun T, Li J, Vuitton DA, Zhang W, et al. Echinococcosis: advances in the 21st century. Clin Microbiol Rev. 2019;32:1–39.
Qucuo N, Wu G, He R, Quzhen D, Zhuoga C, Deji S, et al. Knowledge, attitudes and practices regarding echinococcosis in Xizang Autonomous Region, China. BMC Public Health. 2020;20:483.
McManus DP, Gray DJ, Zhang W, Yang Y. Diagnosis, treatment, and management of echinococcosis. BMJ. 2012;344:e3866.
Budke CM, Deplazes P, Torgerson PR. Global socioeconomic impact of cystic echinococcosis. Emerg Infect Dis. 2006;12:296–303.
Torgerson PR, Keller K, Magnotta M, Ragland N. The global burden of alveolar echinococcosis. PLoS Negl Trop Dis. 2010;4:e722.
Yin J, Gongsang Q, Wang L, Li C, Wu X. Identification of vulnerable populations and knowledge, attitude, and practice analysis of echinococcosis in Tibet Autonomous Region of China. Environ Res. 2020;190:110061.
Ministry of Health of the People’s Republic of China. Diagnostic criteria for hydatid disease (WS 257–2006). 2006.
Likas A, Vlassis N, Verbeek JJ. The global k-means clustering algorithm. Pattern Recognit. 2003;36:451–61.
Hartigan JA, Wong MA. Algorithm AS 136: A K-means clustering algorithm. J Roy Stat Soc. 1979;28:100–8.
MacQueen J, editor. Some methods for classification and analysis of multivariate observations. In: Proceedings of the fifth Berkeley symposium on mathematical statistics and probability. Oakland, CA, USA; 1967.
Chen WQ, Zhang YL, GongSang QZ, Wu WP, Han S, Xue CZ, et al. Analysis of hydatid disease cases in Tibet Autonomous Region Chinese. J Parasitol Parasit Dis. 2018;36:43–6.
Li B, GongSang QZ, Xue CZ, Han S, Chen WQ, Yan XL, et al. Epidemiological survey of echinococcosis in Tibet Autonomous Region of China. Infect Dis Poverty. 2019;8:29.
Wang Q, Qiu J, Yang W, Schantz PM, Raoul F, Raoul F, et al. Socioeconomic and behavior risk factors of human alveolar echinococcosis in Tibetan communities in Sichuan, People’s Republic of China. Am J Trop Med Hyg. 2006;74:856–62.
Bingham GM, Budke CM, Larrieu E, Del Carpio M, Mujica G, Slater MR, et al. A community-based study to examine the epidemiology of human cystic echinococcosis in Rio Negro Province. Argentina Acta Trop. 2014;136:81–8.
Martínez GP. Hidatidosis humana: antecedentes generales y situación epidemiológica en Chile, 2001–2009 [Human hydatidosis disease: general background and epidemiological situation in Chile, 2001–2009]. Rev Chilena Infectol. 2011;28:585–91.
Chai JJ. Epidemiological studies on cystic echinococcosis in China–a review. Biomed Environ Sci. 1995;8:122–36.
Wu WT, Wu WP, Guan YY, Han S, Xue CS, Wang X, et al. A case⁃control study on risk factors of cystic echinococcosis in humans in Tibetan areas Chinese. J Schistosomiasis Control. 2018;30:161–4.
Gemmell MA. Taeniidae: modification to the life span of the egg and the regulation of tapeworm populations. Exp Parasitol. 1977;41:314–28.
Veit P, Bilger B, Schad V, Schäfer J, Frank W, Lucius R. Influence of environmental factors on the infectivity of echinococcus multilocularis eggs. Parasitology. 1995;110:79–86.
Dowling PM, Abo-Shehada MN, Torgerson PR. Risk factors associated with human cystic echinococcosis in Jordan: results of a case-control study. Ann Trop Med Parasitol. 2000;94:69–75.
Wang Q, Huang Y, Huang L, Yu WJ, He W, Zhong B, et al. Review of risk factors for human echinococcosis prevalence on the Qinghai-Tibet Plateau, China: a prospective for control options. Infect Dis Poverty. 2014;3:3.
Craig PS, Giraudoux P, Wang ZH, Wang Q. Echinococcosis transmission on the Tibetan Plateau. Adv Parasitol. 2019;104:165–246.
Li TY, Qiu JM, Yang W, Craig PS, Chen XW, Xiao N, et al. Echinococcosis in Tibetan populations, western Sichuan province. China Emerg Infect Dis. 2005;11:1866–73.
Piarroux M, Piarroux R, Knapp J, Bardonnet K, Dumortier J, Watelet J, et al. Populations at risk for alveolar echinococcosis, France. Emerg Infect Dis. 2013;19:721.
Craig PS, Larrieu E. Control of cystic echinococcosis/hydatidosis: 1863–2002. Adv Parasitol. 2006;61:443–508.
Cai QG, Han XM, Yang YH, Zhang XY, Ma LQ, Karanis P, et al. Lasiopodomys fuscus as an important intermediate host for echinococcus multilocularis: isolation and phylogenetic identification of the parasite. Infect Dis Poverty. 2018;7:27.
Budke CM, Campos-Ponce M, Wang Q, Torgerson PR. A canine purgation study and risk factor analysis for echinococcosis in a high endemic region of the Tibetan plateau. Vet Parasitol. 2005;127:43–9.
Vaniscotte A, Raoul F, Poulle ML, Romig T, Dinkel A, Takahashi K, et al. Role of dog behaviour and environmental fecal contamination in transmission of echinococcus multilocularis in Tibetan communities. Parasitology. 2011;138:1316–29.
Wang LY, Gongsang QZ, Pang HS, Qin M, Wang Y, Li JZ, et al. Assessment of echinococcosis control in Tibet Autonomous Region China. Infect Dis Poverty. 2022;11:59.
Conraths FJ, Probst C, Possenti A, Boufana B, Saulle R, La Torre G, et al. Potential risk factors associated with human alveolar echinococcosis: systematic review and meta-analysis. PLoS Negl Trop Dis. 2017;11:e0005801.
Craig PS, Hegglin D, Lightowlers MW, Torgerson PR, Wang Q. Echinococcosis: control and prevention. Adv Parasitol. 2017;96:55–158.
Acknowledgements
Since the National Echinococcosis Control project was launched in 2006; it has been supported by peers in all epidemic areas. We sincerely thank all the participants who participated in the prevention and control activities in all echinococcosis endemic counties in nine epidemic provinces (plus Xinjiang Production and Construction Corps).
Funding
The study was financially supported by the National Natural Science Foundation of China (grant no. 81703281) and NHC Key Laboratory of Echinococcosis Prevention and Control, China (No.2021WZK1006).
Author information
Authors and Affiliations
Contributions
JY, LYW, and WPW conceived and designed the study. LYW and JY administered the project. LYW and WPW supervised the project. LYW and WPW collected the data. LYW, MQ, LG, XXC, JXL, and RF analyzed the data. LYW and MQ wrote the manuscript. RF and LG reviewed and edited the manuscript. All the authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This survey was approved by the Ethics Review Committee of the National Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention. All participants were informed about the content and purpose of the investigation before data collection. The consenters were required to sign the “informed consent form,” and for minor children the informed consents of their guardians were obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, LY., Qin, M., Gavotte, L. et al. Societal drivers of human echinococcosis in China. Parasites Vectors 15, 385 (2022). https://doi.org/10.1186/s13071-022-05480-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13071-022-05480-8