
Abstract
Background
It had been more than 5 years since the first case of Middle East Respiratory Syndrome coronavirus infection (MERS-CoV) was recorded, but no specific treatment has been investigated in randomized clinical trials. Results from in vitro and animal studies suggest that a combination of lopinavir/ritonavir and interferon-β1b (IFN-β1b) may be effective against MERS-CoV. The aim of this study is to investigate the efficacy of treatment with a combination of lopinavir/ritonavir and recombinant IFN-β1b provided with standard supportive care, compared to treatment with placebo provided with standard supportive care in patients with laboratory-confirmed MERS requiring hospital admission.
Methods
The protocol is prepared in accordance with the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) guidelines. Hospitalized adult patients with laboratory-confirmed MERS will be enrolled in this recursive, two-stage, group sequential, multicenter, placebo-controlled, double-blind randomized controlled trial. The trial is initially designed to include 2 two-stage components. The first two-stage component is designed to adjust sample size and determine futility stopping, but not efficacy stopping. The second two-stage component is designed to determine efficacy stopping and possibly readjustment of sample size. The primary outcome is 90-day mortality.
Discussion
This will be the first randomized controlled trial of a potential treatment for MERS. The study is sponsored by King Abdullah International Medical Research Center, Riyadh, Saudi Arabia. Enrollment for this study began in November 2016, and has enrolled thirteen patients as of Jan 24-2018.
Trial registration
ClinicalTrials.gov, ID: NCT02845843. Registered on 27 July 2016.
Similar content being viewed by others


Background
Since the first report of infection with the Middle East Respiratory Syndrome coronavirus (MERS-CoV) was published in 2012, the World Health Organization has been notified of 2123 laboratory-confirmed infections with MERS-CoV from 27 countries and at least 740 reported deaths (case fatality 35%) [1]. There is no specific therapy of proven efficacy available and no potential treatment has been tested in a randomized clinical trial (RCT) for evaluation [2,3,4]. Based on results from in vitro and animal studies of MERS-CoV infection, the guanosine analog ribavirin, in combination with interferon alpha (IFN-α), has been used to treat patients with MERS [5,6,7,8]. However, the concentration of ribavirin required to inhibit MERS-CoV in vitro exceeds peak levels in the blood after therapeutic doses in humans [9,10,11]. Furthermore, retrospective studies with IFN-α2a, IFN-α2b or IFN-β1a in combination with ribavirin have not shown a clear benefit in patients with MERS [6,7,8, 12].
MERS-CoV attenuates the interferon (IFN) response of the innate immune system, and this mechanism is thought to impair the antiviral adaptive type 1 T-helper cell (Th-1) immune response [13,14,15]. In vitro, IFN-α and IFN-β have inhibitory effects on MERS-CoV and on the closely related coronavirus, Severe Acute Respiratory Syndrome (SARS)-CoV, but MERS-CoV appears to be significantly more sensitive than SARS-CoV to IFN effects [15, 16]. Among IFN subtypes, IFN-β1b causes the greatest in vitro inhibition of MERS-CoV, and has a significantly lower ratio of the half-maximal effective concentration (EC) to the maximal plasma concentration (EC50:Cmax) than IFN-α2a, IFN-α2b or IFN-β1a, indicating potentially greater efficacy [9, 11]. This observation may also partially explain the lack of clear benefit associated with the use of IFN-α2a, IFN-α2b or IFN-β1a in combination with ribavirin. Recombinant IFN-β1b (Betaseron®, Bayer, Leverkusen, Germany) is approved for multiple sclerosis [17,18,19].
Based on in vitro data, the combination of lopinavir and ritonavir has been considered as a candidate therapy for MERS. Lopinavir and ritonavir are antiretroviral protease inhibitors used in combination for the treatment of human immunodeficiency virus (HIV) infection and have limited side effects [20]. The combination of lopinavir/ritonavir (Kaletra®, Abbott Laboratories, Chicago, IL, USA) has also been used for the treatment of SARS. In one study, the combination of lopinavir/ritonavir used in 41 patients with SARS was associated with significantly fewer adverse clinical outcomes (acute respiratory distress syndrome or death) 21 days after the onset of symptoms compare to ribavirin alone used in 111 historical controls (2.4% versus 28.8%, p = 0.001) [21]. However, the historical nature of the control comparison does not allow for a valid estimate of efficacy. In a high-throughput screening for antiviral compounds, lopinavir inhibited the replication of MERS-CoV at levels below those that occur in the circulation after a single oral dose of lopinavir/ritonavir (400 mg lopinavir with 100 mg ritonavir), suggesting that the drug can achieve therapeutic levels in vivo [16, 22]. The effects of lopinavir/ritonavir, IFN-β1b and mycophenolate mofetil (MMF), all of which have shown viral inhibitory effects in vitro, have been tested in common marmosets with severe MERS-CoV infection [23]. The animals treated with lopinavir/ritonavir or IFN-β1b had improved clinical, radiological, pathological and viral-load outcomes compared with untreated animals. By contrast, treatment with MMF resulted in severe or fatal disease, with higher mean viral loads than in untreated animals. Untreated animals and MMF-treated animals had a mortality of 67% by 36 h compared to 0–33% among animals treated with lopinavir/ritonavir or IFN-β1b [23].
In one case from the 2015 Korean MERS outbreak, lopinavir/ritonavir used in combination with ribavirin and IFN-α2a resulted in defervescence, virological clearance and survival [24]. In another case from Greece, lopinavir/ritonavir combined with IFN and ribavirin was started on day 13 of a MERS illness and was followed 2 days later by clearance of viremia, although viral ribonucleic acid (RNA) persisted in the respiratory secretions until the fourth week of illness and the patient subsequently died [25]. During the Korean outbreak of MERS, most patients that developed respiratory illness received triple antiviral therapy composed of pegylated interferon (IFN)-α, ribavirin, and lopinavir/ritonavir; however, data about the efficacy of this approach are lacking [26]. These findings, together with the availability and safety profiles of lopinavir/ritonavir and IFN-β1b, suggest that the combination of these agents has potential efficacy for the treatment of patients with MERS.
The objective of the MIRACLE trial (the MERS-CoV Infection tReated with A Combination of Lopinavir/ritonavir and intErferon-β1b) is to assess the efficacy of administering a combination of lopinavir/ritonavir and recombinant IFN-β1b to hospitalized adults with laboratory-confirmed MERS. The study is designed as recursive, two-stage, group sequential, multicenter, randomized, placebo-controlled, double-blind trial. We report the study protocol according to the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) template [27].
Methods
Study design
The study is a recursive, two-stage, group sequential, multicenter, randomized, placebo-controlled, double-blind trial [28]. The trial is initially designed with 2 two-stage components with two interim analyses and one final analysis. The first two-stage component is designed to adjust sample size and determine futility stopping, but not efficacy stopping. The second two-stage component is designed to determine efficacy stopping and possibly readjustment of sample size to maintain conditional power at the final analysis.
Study population
Inclusion criteria at eligibility assessment
-
1.
Adult (defined as ≥ 18 years of age)
-
2.
Laboratory confirmation of MERS-CoV infection by reverse-transcription polymerase chain reaction (RT-PCR) from any diagnostic sampling source, and
-
3.
New organ dysfunction that is judged to be related to MERS including: hypoxia defined as requirement of supplemental oxygen to maintain oxygen saturations > 90%, hypotension (systolic blood pressure < 90 mmHg) or the need for vasopressor/inotropic medication, renal impairment (increase of creatinine by 50% from baseline, glomerular filtration rate reduction by > 25% from baseline or urine output of < 0.5 ml/kg for 6 h – risk stage by RIFLE criteria) [29], neurological pathology (reduction of Glasgow Coma Scale by 2 or more, i.e., 13 or lower of 15 points), thrombocytopenia (<150,000 platelets/mm3) or gastrointestinal symptoms that require hospitalization (e.g., severe nausea, vomiting, diarrhea or/and abdominal pain).
Exclusion criteria at eligibility assessment
-
1.
Suicidal ideation based on history (contraindication to IFN-β1b)
-
2.
Known allergy or hypersensitivity reaction to lopinavir/ritonavir or to recombinant IFN-β1b, including, but not limited to, toxic epidermal necrolysis, Stevens-Johnson syndrome, erythema multiforme, urticaria or angioedema
-
3.
Elevated alanine aminotransferase (ALT) more than five-fold the upper limit in the hospital’s laboratory
-
4.
Use of medications that are contraindicated with lopinavir/ritonavir and that cannot be replaced or stopped during the study period, such as CYP3A inhibitors (see Table 1)
Table 1 Lopinavir/ritonavir interactions with drugs commonly used in the intensive-care unit -
5.
Pregnancy – eligible and consenting female participants of childbearing age will be tested for pregnancy before enrollment in the study
-
6.
Known HIV infection, because of concerns about the development of resistance to lopinavir/ritonavir if used without combination with other anti-HIV drugs, or
-
7.
Patient likely to be transferred to a non-participating hospital within 72 h.
Trial intervention
Informed consent will be obtained from eligible patients or their substitute decision-makers (for patients lacking decision-making capacity). All patients who provide informed consent will be randomly allocated into one of two study groups.
Intervention group
The intervention group will receive the standard of care as well as lopinavir/ritonavir and recombinant IFN-β1b. Lopinavir/ritonavir (400 lopinavir mg/100 mg ritonavir) will be administered every 12 h for 14 days in tablet form. For patients who are unable to take medications by mouth, the lopinavir/ritonavir (400 lopinavir mg/100 mg ritonavir) will be administered as a 5-ml suspension every 12 h for 14 days via a pre-existing or newly placed nasogastric tube. IFN-β1b will be administered as 0.25-mg/ml subcutaneous injections on alternate days for 14 days (for a total of seven doses).
Control group
The control group will receive standard of care as well as placebo treatment for 14 days at the same frequency as the intervention group, to maintain blinding. One placebo will be given every 12 h and will comprise a sucrose tablet or capsule, or 5 ml of normal saline via nasogastric tube for patients who are unable to take medications by mouth. Patients in the control group will receive 1 ml of normal saline by subcutaneous injection on alternate days.
Co-interventions
Patients in both study arms will receive standard supportive care (e.g., oral/and or intravenously administered fluids according to basal daily requirements or blood pressure support, oral or parenteral nutrition, venous thromboembolism prophylaxis, antibiotic therapy for infections, supplemental oxygen or mechanical ventilation for hypoxia or ventilation needs) at the discretion of the treating teams. Recommendations regarding current standards of care that are consistent with best clinical practices and World Health Organization guidelines will be provided to the treating teams. Data on the use of antimicrobials and corticosteroids, and aspects of respiratory, cardiovascular and renal support will be collected but not protocolized. All patients will be tested for HIV on enrollment; however, results of testing may be delayed > 24 h for some patients; therefore, we will not delay randomization while waiting HIV status. In patients who are discovered to be HIV positive, the intervention will be discontinued and outcome data will be collected as per protocol, as these patients will be included in the intention-to-treat analysis. We will have a separate on-treatment analysis that will not include these patients. Treatment of HIV infection will be as per the treating team.
Randomization, allocation and blinding
Randomization
Patients will be randomly assigned to one of the two intervention arms by a variable-size block, computer-generated randomization procedure, which will ensure that the two arms contain equal numbers of patients. Randomization will be stratified according to center and according to whether the patients require mechanical ventilation (invasive or non-invasive) at the time of enrollment.
Allocation
Patient allocation will follow a concealed process using sealed, fully opaque, numbered envelopes.
Blinding
The intervention will be blinded for the research team (principal investigator, co-investigators, research coordinators and the Steering Committee), treating team (physicians, bedside nurses and clinical pharmacists), outcome assessors (including the laboratory personnel) and study patients. Pharmacists who prepare the study medication, dosing nurses (who administer the medication) and the study statistician will not be blinded. This approach was chosen because placebos that exactly match the medications in appearance are not available.
Study drug preparation and administration
Storage and handling
Lopinavir/ritonavir and recombinant IFN-β1b will be stored in a secure area in the pharmacy at room temprature or refrigerator at 2–8 °C according to standard hospital procedures and the product monograph. A temperature log with daily minimum and maximum temperature readings will be kept by the site pharmacist. Any temperature excursion will be reported immediately to an unblinded project officer from the sponsor, King Abdullah International Medical Research Center, Riyadh, Saudi Arabia. The sodium chloride (0.9%) ampoules and the starch capsules will be stored in a restricted area at room temperature.
Study drug composition and dispensing
At patient randomization by the site investigator or by appropriately delegated study personnel, a sealed envelope containing the patient allocation will be delivered to the pharmacy. The unblinded pharmacist will open the envelope and dispense the study drug in a tamperproof sealed box to blind the treatment assignment. The sealed, opaque box will be labeled to include the following information: name and number of clinical trial protocol, patient study number and site number. The box will only be opened by the unblinded study nurse.
Administration
Unblinded dosing nurses, who will not be responsible for the direct clinical care of the patients, nor other study procedures including assessment of the study outcomes, will administer the treatment. A second un-blinded nurse will check the treatment regimen for each patient according to local hospital regulations for medication administration. The dosing nurses will maintain blinding by the following measures: (1) pulling the screens around the patients’ bed areas while the dose is administered and ensuring that no members of the treating team are present; (2) discarding any labels and the used syringe in a way that ensures that the identity of the medication is not revealed; and (3) avoiding any discussion regarding the study drug with other hospital staff, except the unblinded pharmacist.
Duration of the intervention
The study interventions will continue for 14 days according to the protocol. Medications will be discontinued in patients who are well enough to be discharged from the hospital, even if this occurs before 14 days have elapsed.
Frequency and duration of follow-up
Patients will be followed daily until discharge from hospital or day 28, whichever comes first (Fig. 1). After day 28, the patients will be followed only to document their ICU, hospital, 90-day mortality and length of stay. Collection of this information may require telephone interviews with patients or next of kin. Figure 1 shows the schedule of enrollment, intervention and assessment for the MIRACLE trial according to the SPIRIT template. The SPIRIT Checklist is given in Additional file 1.

Schedule of enrollment, intervention and assessment for the MIRACLE trial according to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) template [27]. Arrows indicate periods of continuous or daily collection or assessment, whereas “X” indicates collection on specific days. * ± 2 days except D0 and D3. ‡Assessed by the clinical pharmacist. §Tests on sputum, tracheal aspirate, broncheoalveolar lavage and nasopharyngeal swab to be continued twice weekly until two consecutive tests are negative. ||Mandatory for intubated patients, optional for non-intubated patients. ¶Hemoglobin, white blood cells, neutrophils, lymphocytes and platelets. #Blood urea nitrogen, creatinine, potassium, sodium, chloride, bicarbonate, glucose and albumin. ∞Serum bilirubin, gamma-glutamyl transferase, alanine transaminase and aspartate aminotransferase. **Serum thyroxine, triiodothyronine and thyroid-stimulating hormone. Abbreviations: ACTH adrenocorticotropic hormone, MERS-CoV Middle East Respiratory Syndrome coronavirus, SOFA Sequential Organ Failure Assessment
MERS-CoV RT-PCR testing
Diagnostic RT-PCR will be preformed per each hospital protocol in its own hospital laboratory or in the reference laboratory of the Saudi Ministry of Health. Additionally, respiratory and blood samples will be sent to King Abdullah International Research Center for semi-quantitative viral-load testing. The testing procedure includes extracting ribonucleic acid (RNA) from respiratory and serum specimens using the MagNA Pure 96 Viral NA Kit (Roche Applied Science, Indianapolis, IN, USA). The extracted nucleic acids will be tested by rRT-PCR targeting the upstream MERS-CoV envelope protein gene (upE) and open-reading frame 1a (ORF1a) regions of the MERS-CoV genome on a LightCycler 480 System (Roche Diagnostics, Mannheim, Germany) [30]. A positive control for ORF1a and upE rRT-PCR is performed according to the manufacturer’s instructions. We will document cycle thresholds (Ct) for upE and ORF1a which indicate the start of exponential amplification. For diagnostic purposes, we consider a cycle threshold (Ct) of < 35 the cutoff for upE and ORF1a in line with the cutoff used by the Saudi Arabia Ministry of Health reference laboratory. If Ct values are ≥ 35, the test will be repeated using different samples, preferably from the lower respiratory tract, to avoid false-positive results. We will use Ct values as semi-quantitative measures for viral RNA load.
Study outcomes
Primary outcome
-
1.
90-day mortality
Secondary clinical outcomes
-
1.
Mortality in the ICU, mortality in the hospital and 28-day mortality
-
2.
Sequential Organ Failure Assessment (SOFA) scores at baseline and on study days 1, 3, 7, 14, 21 and 28
-
3.
Organ support, according to the number of days within the first 28 days after enrollment when patients do not receive specific forms of support:
- (a)
Supplemental oxygen-free days
- (b)
Renal replacement therapy-free days
- (c)
Vasopressor-free days
- (d)
Invasive or non-invasive mechanical ventilation-free days
- (e)
Organ support-free days (that is, days free of invasive mechanical ventilation, renal replacement therapy and vasopressors)
- (f)
Extracorporeal circulation support-free days
- (a)
-
4.
ICU-free days and hospital length of stay:
- (a)
ICU-free days are the number of days when patients are not being cared for in the ICU during the first 28 days after enrollment. Patients who die within 28 days will be assigned the value “0”
- (b)
The hospital length of stay will be calculated as the number of days between admission and discharge from the hospital. Because of the competing risk effect of death on length of stay, length of stay will be also reported for survivors alone
- (a)
Secondary laboratory outcomes
-
1.
Viral replication kinetics will be calculated by determining viral RNA loads as reflected by Ct values by semi-quantitative PCR in serial samples of upper and lower respiratory tract secretions and blood, collected twice per week. Quantitative PCR, which may be more sensitive than Ct values, will be used if it becomes available during the trial
-
2.
Time to clearance from the lower respiratory tract will be determined from the results of RT-PCR analyses of lower respiratory tract secretions or nasopharyngeal swabs in non-intubated patients who are unable to give sputum samples; clearance will be defined as two negative RT-PCR results not followed by a positive one. Patients who die before clearance will be censored at the time of death
-
3.
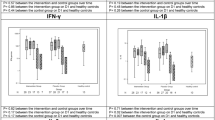
Planned sub-studies will examine cytokine, chemokine and immune responses in serially collected blood samples. A detailed protocol of this sub-study will be published separately
Safety outcomes
-
1.
Safety outcomes will be assessed from serious adverse event reports. The following serious adverse events will be documented at any time during the study period:
- (a)
acute pancreatitis (defined as having two of the following three features: (1) abdominal pain consistent with acute pancreatitis; (2) serum lipase or amylase at least three times greater than the upper limit of normal; and (3) characteristic findings of acute pancreatitis on contrast-enhanced computed tomography) [31] or magnetic resonance imaging
- (b)
elevation of ALT to more than five-fold upper normal limit
- (c)
anaphylaxis
- (d)
bleeding diathesis (INR > 3 without anticoagulant therapy)
- (a)
-
2.
The following data regarding adverse drug reactions will be assessed with the treating team and recorded daily for 14 days and then at 21 days and 28 days after enrollment:
- (a)
Allergic or sensitivity/hypersensitivity reactions, including rash, urticaria, tongue edema, bronchospasm, dyspnea and skin necrosis at the injection site
- (b)
Gastrointestinal signs or symptoms, including nausea, vomiting, abdominal pain and diarrhea
- (c)
Neurological symptoms, including fatigue, headache, insomnia, psychosis, depression and mania
- (a)
Functional outcomes
Data will be collected at baseline before the current illness and at 90 days and may require telephone interviews with the patients or next of kin to determine the patients’ status according to the Karnofsky Performance Scale, which is a scale from 100 (indicating “Normal,” no complaints; no evidence of disease) to 0 (indicating death) [32].
Safety measures
Drug interactions
A clinical pharmacist and the treating physician will evaluate each patient at the time of enrollment and daily throughout the study period until day 14 to identify any interactions between the investigated treatments and other drugs, and they will take action accordingly. Table 1 summarizes common medications that may interact with lopinavir/ritonavir and a suggested action plan.
Liver function tests
Elevated liver enzymes are common in MERS infection due to the liver involvement in the disease. Based on analysis of our historical data, liver enzymes were not more elevated in patients treated with ribavirin and IFN-α. Based on HIV literature, aminotransferase elevation levels (more than five times the upper limit of normal) occur in 3 to 10% of patients taking lopinavir/ritonavir-containing antiretroviral regimens [33]. These laboratory abnormalities are usually asymptomatic and self-limited and often resolve even without discontinuation of the drug [33]. Clinically apparent hepatotoxicity due to lopinavir/ritonavir occurs, but is rare, with symptoms or jaundice appear usually after 1 to 8 weeks of starting therapy [33]. The hepatotoxicity is usually self-limited; although fatal cases have been reported [33]. The treating team should discontinue or minimize concomitant use of any medication that has hepatotoxic potential.
Rules regarding premature discontinuation of treatment
The study intervention will be suspended if the subject develops any of above defined serious adverse events occurred: (1) acute pancreatitis; (2) elevation of ALT to more than five-fold the upper normal limit; (3) anaphylaxis; and (4) bleeding diathesis. These events will be reviewed by at least two people with a third as necessary, all of whom are blinded to the intervention allocation, to adjudicate these events by looking at the study data/clinical records. In case of premature discontinuation of treatment, other aspects of the study procedures, such as data collection and laboratory testing, will be continued and patient data will be included in the intention-to-treat analysis.
Unblinding
Breaking of blinding can be occur in the event that the treating team believes that there is a very strong reason to know the study drug allocation and after discussion with the study principal investigator. In all such cases, the adverse event necessitating emergency unblinding will be reported as a serious adverse event.
Serious adverse events
Any unexpected, medical occurrence that results in death, prolonged hospitalization, persistent or significant disability or incapacity, which is judged to be causally related to the study intervention, will be reported as a serious adverse event to the Institutional Review Board and the Data Safety Monitoring Board. Potential serious adverse events for the trial are defined above and include (1) acute pancreatitis; (2) severe elevation of ALT to more than five-fold the upper normal limit; (3) anaphylaxis; and (4) bleeding diathesis.
Study management
Steering Committee
The Steering Committee, led by the principal investigator, will be responsible for overseeing the conduction of the trial, providing training for new sites, ensuring compliance with the study procedures, addressing challenges that occur at all sites, reviewing serious adverse events and formulating the statistical analysis plan.
Data Safety Monitoring Board
The Data Safety Monitoring Board, which is responsible for reviewing reports regarding the safety of the study patients and protocol adherence, may make recommendations to continue or terminate the study on the basis of the results from the interim analysis. The board will meet at the beginning of the study and at 6-monthly intervals thereafter, or as needed.
Quality control and assurance
Several procedures to ensure data quality and protocol compliance are undertaken including: (1) Training sessions for the study team in the participating centers prior to study commencement; (2) Startup meetings for all sites, either on site or remotely; and (3) Monitoring visits before, during and at the close out of the study.
Study drug distribution to other centers
The Investigational Drug Unit at King Abdullah International Medical Research Center will distribute the study medication and the placebo to other centers. Randomization and blinding will be performed at the local pharmacy of each hospital according to the procedures described above.
Ethical issues
The MIRACLE study is approved by the Scientific Committee and the Institutional Review Boards of the participating sites and registered at the Saudi Food and Drug Authority (SFDA).
The study will be conducted in accordance with the ethical principles of the Declaration of Helsinki and the International Council for Harmonization–Good Clinical Practice guidelines. Informed consent will be obtained from patients or their substitute decision-makers. Site invistigators will explain the objectives of the trial and its potential risks and benefits to patients when possible, or to substitute decision-makers, during the process of obtaining consent. No compensation is provided for enrollment in the trial.
Patient personal data are de-identified. Data from all centers will be stored on a secure place at King Abdullah International Medical Research Center, Riyadh. A list of names/hospital numbers and unique study identification (ID) will be kept in a separate location to the trial data, which has only the associated unique subject ID attached to it.
Statistical analysis
Baseline clinical and demographic characteristics will be summarized and reported using descriptive statistics. Categorical variables will be reported as numbers and percentages, and will be compared using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables will be reported as means and standard deviations or as medians and interquartile ranges, and will be compared using Student’s t test or the Mann-Whitney U test, as appropriate.
The primary analysis will be conducted according to the intention-to-treat principle and will be unadjusted. Per-protocol analysis will be performed and reported separately. The primary analysis will examine the difference in primary outcome between groups and will be reported as absolute risk reduction, with a 95% confidence interval. We do not anticipate imbalances between the two groups. Secondary analysis will be conducted using multiple logistic regression analysis in which death within 90 days will be modeled as the dependent variable and a set of baseline variables that are strongly believed to affect the outcome of MERS-CoV infection will be included as independent variables. Those variables will include at minimum age, community-acquired versus hospital-acquired infection, mechanical ventilation, center, and SOFA score [34]. The multivariable analysis will also include clinically important and unequally distributed baseline variables between the two groups (p < 0.05). Median survival time will be summarized and reported using Kaplan-Meier curves and will be compared between the study groups using the log-rank test. Statistical tests for variables other than the primary outcome will be performed using a two-sided alpha value of 5% to denote significance level.
If patient numbers permits (e.g., no fewer than five patients in subgroups of interest), stratified analysis will be carried out between the following subgroups:
- 1.
Patients with and without mechanical ventilation at the time of randomization
- 2.
Patients with different Acute Physiology and Chronic Health Evaluation II (APACHE II) disease-severity scores at the time of randomization stratified to high (above median) and low (below median) APACHE II scores
- 3.
Patients receiving and those not receiving vasopressors at the time of randomization
- 4.
Patients with ≤ 7 and > 7 days between onset of symptoms to enrollment
- 5.
Patients receiving and those not receiving renal replacement therapy at randomization
Interim analysis and continuous study planning
Because of the uncertainty surrounding the recruitment rate and the efficacy level of the treatment, the trial is designed as recursive, two-stage, group sequential randomized trial [28]. The trial is designed initially to have 2 two-stage components with two interim analyses and one final analysis (Fig. 2). The first two-stage component is designed to determine futility stopping and adjust sample size, but not efficacy stopping. The second two-stage component is designed to determine efficacy stopping and possibly readjustment of sample size to maintain conditional power at the final analysis. A classic two-group design requires a total of 194 subjects (97 subjects per group) to have a 80% power at a significant level of 2.5% (one-sided test) to detect 20% absolute risk reduction in 90-day mortality among subjects receiving treatment (20%) compared to the control group (40%). The trial will start the first two-stage design with 136 subjects (68 subjects per group). We will conduct the first interim analysis when the total subject with 90 days of follow-up reaches 34 subjects (17 per group), which is about 17.5% of the total sample size needed for classical design. We use the method of summing of stage-wise p value to determine the one-sided stopping boundaries in the first two-stage design listed in Table 2. At the first interim analysis we will use the stage-wise p values obtained from the chi-square test for difference in proportion to determine whether the trial will be stopped for futility or not. Should the trial continue, sample size re-estimation based on the observed effect size will be determined using the following formula assuming a conditional power of 80%:

Schematic illustration of the MIRACLE trial design with 2 two-stage components with two interim analyses and one final analysis. Raw p values are obtained from the one-sided chi-square for difference in proportion at each interim analysis
Based on the estimated sample size, we will recalculate the conditional error and set the parameters for the second of the two stages. At the second interim analysis, should the trial continue for efficacy, sample size readjustment will be made based on the previous formula and new boundaries will be calculated for the final-stage analysis.
Upon completion, the results of the trial is planned to be submitted to peer-reviewed journal. Authorship will follow the Uniform Requirements for Manuscripts Submitted to Biomedical Journals [35].
Discussion
This study will be the first randomized controlled trial of a treatment for MERS-CoV infection. Although this type of study provides the best method for determining treatment efficacy during disease outbreaks [36, 37], conducting a randomized controlled trial is logistically challenging [37, 38] since the distribution of MERS cases is sporadic and unpredictable, both geographically and temporally, necessitating the involvement of several centers in the trial to ensure adequate recruitment. This requirement contributes greatly to the planning and administration associated with the trial.
To overcome the uncertainty in recruitment rate and efficacy of the trial’s treatment we designed the trial using recursive, two-stage adaptive design, which is a relatively new method for group sequential trials [28]. The approach is based on the conditional error principle which allows for continuous adjustment of the trial parameters using data observed during prior stages without inflating type I error [39]. Another advantage of this method is the flexibility in setting the timing and the number of needed interim analyses. Such flexibility is necessary in situations where recruitment rate is unpredictable and sudden flux in patient recruitment could happen at any time.
For many emerging infectious diseases, including MERS, patients are often treated with therapeutics on the basis of minimal evidence. For example, patients with MERS have been treated with ribavirin and IFN-α despite the lack of clinical trials exploring the effectiveness of this treatment combination. If these patients had been included in a properly designed study, conclusive evidence might have been generated. Performing such a trial meets a critical need.
Some limitations to our study design should be noted. Complete blinding was not feasible because of the unavailability of appropriate placebo; therefore, the study is unblinding to the dosing nurses and the dispensing pharmacist, both of whom are not otherwise involved in the patient care. However, blinding will be maintained to all other members of the clinical and research team. Because of the sporadic and unpredictable nature of the disease, the number of patients from some sites may be low.
Trial status
The MIRACLE trial has already been approved by the Institutional Review Boards at eight hospitals and by the Scientific Advisory Board at the Ministry of Health in Saudi Arabia and the Saudi Food and Drug Authority. Enrollment for this study began in November 2016, and has enrolled thirteen patients as of Jan 24-2018. At present, eight sites have completed the regulatory requirements and are actively screening for eligible patients; 12 other centers are in progress.
Abbreviations
- ALT:
-
Alanine aminotransferase
- APACHE II:
-
Acute Physiology and Chronic Health Evaluation II
- Ct:
-
Threshold cycle
- EC:
-
Effective concentration
- HIV:
-
Human immunodeficiency virus
- IFN:
-
Interferon
- IFN-α:
-
Interferon alpha
- IFN-β1b:
-
Interferon beta-1b
- MERS-CoV:
-
Middle East Respiratory Syndrome coronavirus
- MIRACLE trial:
-
the MERS-CoV Infection tReated with A Combination of Lopinavir/ritonavir and intErferon β1b
- MMF:
-
Mycophenolate mofetil
- RT-PCR:
-
Reverse-transcription polymerase chain reaction
- SARS:
-
Severe Acute Respiratory Syndrome
- SPIRIT:
-
Standard Protocol Items: Recommendations for Interventional Trials
References
World Health Organization: Middle East respiratory syndrome coronavirus (MERS-CoV). http://www.who.int/emergencies/mers-cov/en/. Accessed 14 Jan 2018.
Arabi YM, Balkhy HH, Hayden FG, Bouchama A, Luke T, Baillie JK, Al-Omari A, Hajeer AH, Senga M, Denison MR, et al. Middle East Respiratory Syndrome. N Engl J Med. 2017;376(6):584–94.
Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367(19):1814–20.
Mo Y, Fisher D. A review of treatment modalities for Middle East Respiratory Syndrome. J Antimicrob Chemother. 2016;71(12):3340–50.
Falzarano D, de Wit E, Rasmussen AL, Feldmann F, Okumura A, Scott DP, Brining D, Bushmaker T, Martellaro C, Baseler L, et al. Treatment with interferon-alpha2b and ribavirin improves outcome in MERS-CoV-infected rhesus macaques. Nat Med. 2013;19(10):1313–7.
Shalhoub S, Farahat F, Al-Jiffri A, Simhairi R, Shamma O, Siddiqi N, Mushtaq A. IFN-alpha2a or IFN-beta1a in combination with ribavirin to treat Middle East respiratory syndrome coronavirus pneumonia: a retrospective study. J Antimicrob Chemother. 2015;70(7):2129–32.
Khalid M, Al Rabiah F, Khan B, Al Mobeireek A, Butt TS, Al ME. Ribavirin and interferon-alpha2b as primary and preventive treatment for Middle East respiratory syndrome coronavirus: a preliminary report of two cases. Antivir Ther. 2015;20(1):87–91.
Omrani AS, Saad MM, Baig K, Bahloul A, Abdul-Matin M, Alaidaroos AY, Almakhlafi GA, Albarrak MM, Memish ZA, Albarrak AM. Ribavirin and interferon alfa-2a for severe Middle East respiratory syndrome coronavirus infection: a retrospective cohort study. Lancet Infect Dis. 2014;14(11):1090–5.
Hart BJ, Dyall J, Postnikova E, Zhou H, Kindrachuk J, Johnson RF, Olinger Jr GG, Frieman MB, Holbrook MR, Jahrling PB, et al. Interferon-beta and mycophenolic acid are potent inhibitors of Middle East respiratory syndrome coronavirus in cell-based assays. J Gen Virol. 2014;95(Pt 3):571–7.
Falzarano D, de Wit E, Martellaro C, Callison J, Munster VJ, Feldmann H. Inhibition of novel beta coronavirus replication by a combination of interferon-alpha2b and ribavirin. Sci Rep. 2013;3:1686.
Chan JF, Chan KH, Kao RY, To KK, Zheng BJ, Li CP, Li PT, Dai J, Mok FK, Chen H, et al. Broad-spectrum antivirals for the emerging Middle East respiratory syndrome coronavirus. J Infect. 2013;67(6):606–16.
Al-Tawfiq JA, Momattin H, Dib J, Memish ZA. Ribavirin and interferon therapy in patients infected with the Middle East respiratory syndrome coronavirus: an observational study. Int J Infect Dis. 2014;20:42–6.
Lau SK, Lau CC, Chan KH, Li CP, Chen H, Jin DY, Chan JF, Woo PC, Yuen KY. Delayed induction of proinflammatory cytokines and suppression of innate antiviral response by the novel Middle East respiratory syndrome coronavirus: implications for pathogenesis and treatment. J Gen Virol. 2013;94(Pt 12):2679–90.
Faure E, Poissy J, Goffard A, Fournier C, Kipnis E, Titecat M, Bortolotti P, Martinez L, Dubucquoi S, Dessein R, et al. Distinct immune response in two MERS-CoV-infected patients: can we go from bench to bedside? PLoS One. 2014;9(2):e88716.
Zielecki F, Weber M, Eickmann M, Spiegelberg L, Zaki AM, Matrosovich M, Becker S, Weber F. Human cell tropism and innate immune system interactions of human respiratory coronavirus EMC compared to those of severe acute respiratory syndrome coronavirus. J Virol. 2013;87(9):5300–4.
de Wilde AH, Raj VS, Oudshoorn D, Bestebroer TM, van Nieuwkoop S, Limpens RW, Posthuma CC, van der Meer Y, Barcena M, Haagmans BL, et al. MERS-coronavirus replication induces severe in vitro cytopathology and is strongly inhibited by cyclosporin A or interferon-alpha treatment. J Gen Virol. 2013;94(Pt 8):1749–60.
Jankovic SM. Injectable interferon beta-1b for the treatment of relapsing forms of multiple sclerosis. J Inflamm Res. 2010;3:25–31.
Hurwitz BJ, Jeffery D, Arnason B, Bigley K, Coyle P, Goodin D, Kaba S, Kirzinger S, Lynch S, Mandler R, et al. Tolerability and safety profile of 12- to 28-week treatment with interferon beta-1b 250 and 500 microg QOD in patients with relapsing-remitting multiple sclerosis: a multicenter, randomized, double-blind, parallel-group pilot study. Clin Ther. 2008;30(6):1102–12.
Gottesman MH, Friedman-Urevich S. Interferon beta-1b (betaseron/betaferon) is well tolerated at a dose of 500 microg: interferon dose escalation assessment of safety (IDEAS). Mult Scler. 2006;12(3):271–80.
Huang X, Xu Y, Yang Q, Chen J, Zhang T, Li Z, Guo C, Chen H, Wu H, Li N. Efficacy and biological safety of lopinavir/ritonavir based anti-retroviral therapy in HIV-1-infected patients: a meta-analysis of randomized controlled trials. Sci Rep. 2015;5:8528.
Chu CM, Cheng VC, Hung IF, Wong MM, Chan KH, Chan KS, Kao RY, Poon LL, Wong CL, Guan Y, et al. Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings. Thorax. 2004;59(3):252–6.
Abbott Laboratories. Product Information: Kaletra®. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021226s030lbl.pdf. Accessed 14 Jan 2018.
Chan JF, Yao Y, Yeung ML, Deng W, Bao L, Jia L, Li F, Xiao C, Gao H, Yu P, et al. Treatment with lopinavir/ritonavir or interferon-beta1b improves outcome of MERS-CoV infection in a nonhuman primate model of common marmoset. J Infect Dis. 2015;212(12):1904–13.
Kim UJ, Won EJ, Kee SJ, Jung SI, Jang HC. Combination therapy with lopinavir/ritonavir, ribavirin and interferon-alpha for Middle East respiratory syndrome. Antivir Ther. 2016;21(5):455–9.
Spanakis N, Tsiodras S, Haagmans BL, Raj VS, Pontikis K, Koutsoukou A, Koulouris NG, Osterhaus AD, Koopmans MP, Tsakris A. Virological and serological analysis of a recent Middle East respiratory syndrome coronavirus infection case on a triple combination antiviral regimen. Int J Antimicrob Agents. 2014;44(6):528–32.
Min CK, Cheon S, Ha NY, Sohn KM, Kim Y, Aigerim A, Shin HM, Choi JY, Inn KS, Kim JH, et al. Comparative and kinetic analysis of viral shedding and immunological responses in MERS patients representing a broad spectrum of disease severity. Sci Rep. 2016;6:25359.
Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gotzsche PC, Krleza-Jeric K, Hrobjartsson A, Mann H, Dickersin K, Berlin JA, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–7.
Chang, M. Adaptive Design Theory and implementation using SAS and R, 2nd ed. Chapman and Hall/CRC. 2014. Pp. 153–180.
Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P, Acute Dialysis Quality Initiative workgroup. Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8(4):R204–212.
Corman VM, Eckerle I, Bleicker T, Zaki A, Landt O, Eschbach-Bludau M, van Boheemen S, Gopal R, Ballhause M, Bestebroer TM, 39, et al. Detection of a novel human coronavirus by real-time reverse-transcription polymerase chain reaction. Euro Surveill. 2012;17(39).
Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS, Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–11.
O'Toole DM, Golden AM. Evaluating cancer patients for rehabilitation potential. West J Med. 1991;155(4):384–7.
U.S. National Library of Medicine. LiverTox. https://livertox.nlm.nih.gov//Lopinavir.htm. Accessed 14 Jan 2018.
Almekhlafi GA, Albarrak MM, Mandourah Y, Hassan S, Alwan A, Abudayah A, Altayyar S, Mustafa M, Aldaghestani T, Alghamedi A, et al. Presentation and outcome of Middle East respiratory syndrome in Saudi intensive care unit patients. Crit Care. 2016;20(1):123.
International Committee of Medical Journal E. Uniform requirements for manuscripts submitted to biomedical journals. N Engl J Med. 1997;336(4):309–15.
Arabi Y, Deeb AM, Aqeel H, Balkhy H. PubMed-cited research articles on the Middle East respiratory syndrome. Ann Thorac Med. 2016;11(2):112–3.
Ippolito G, Lanini S, Brouqui P, Di Caro A, Vairo F, Fusco FM, Krishna S, Capobianchi MR, Kyobe-Bosa H, Puro V, et al. Non-randomised Ebola trials—lessons for optimal outbreak research. Lancet Infect Dis. 2016;16(4):407–8.
Macklin R, Cowan E. Conducting research in disease outbreaks. PLoS Negl Trop Dis. 2009;3(4):e335.
Schafer H, Muller HH. Modification of the sample-size and the schedule of interim analyses in survival trials based on data inspections. Stat Med. 2001;20:3741–51.
Acknowledgements
We would like to acknowledge Maria D Van Kerkhove, PhD, MERS-CoV Technical Lead, High Threat Pathogens, Global Infectious Hazards Management, Health Emergencies Program, World Health Organization, Geneva, Switzerland for her support the MERS therapeutic program.
We would like to acknowledge the Data Safety Monitoring Board (DSMB) Chair and members:
Greg S Martin, MD (Chair)
Professor of Medicine
Associate Division Director, Critical Care Division of Pulmonary,
Allergy, Critical Care and Sleep
Emory University School of Medicine
Section Chief and Director, Medical and Coronary Intensive Care
Grady Memorial Hospital
David A Schoenfeld, PhD (Member)
Professor of Medicine, Harvard Medical School
Professor in the Department of Biostatistics,
Harvard School of Public Health
Sharon L Walmsley, MSc, MD, FRCPC (Member)
Senior Scientist, Toronto General Research Institute (TGRI)
Shannon Carson, MD (Member)
Professor of Medicine
Division Chief, Pulmonary Diseases and Critical Care Medicine
University of North Carolina at Chapel Hill School of Medicine
The MIRACLE trial group
Riyadh, Kingdom of Saudi Arabia:
King Abdulaziz Medical City: Yaseen M. Arabi, Adel Alothman, Hanan H Balkhy, Abdulaziz Al-Dawood, Sameera AlJohani, Shmeylan Al Harbi, Suleiman Kojan, Majed Al Jeraisy, Ahmad M Deeb, Jesna Jose, Mohamed A Hussein, Mohammed Al Muhaidib, Sadat Musharaf, Hala Al Anizi, Reggie Dael
Ministry of Health: Abdullah M Assiri, Mohammad AlMazroa
Prince Mohammed bin Abdulaziz Hospital: Ayed Asiri, Ziad A Memish, Sameeh S Ghazal, Sarah H Alfaraj, Fahad Bafaqeeh
King Saud Medical City: Abdulrahman Al Harthy, Mohammed Al Sulaiman, Ahmed Mady
Prince Sultan Military Medical City: Yasser Mandourah, Ghaleb A Almekhlafi, Nisreen Murad Sherbeeni, Fatehi Elnour Elzein, Reema Muhammed, Shatha Al Samirrai, Shatha Awad, Rylen Cabio Cabal, Bander Al Onazi, Maha Aljuhani, Melven Vince, Abdulrauf Ahmad Malibary
King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia: Abdullah Almotairi, Mushira Al Enani, Alaa Alqurashi, Fatimah Alenezi, Nada Alkhani
King Faisal Specialist Hospital and Research Center, Riyadh, Kingdom of Saudi Arabia: Khalid A. Maghrabi.
Jeddah, Kingdom of Saudi Arabia
King Abdulaziz Medical City: Fahad Al-Hameed, Asim AlSaedi, Abdulhakeem Thaqafi, Ohoud Al Oraabi, Jalal Rifai, Pansy Elsamadisi, Medhat S Hendy, Sara AbuBaker Basher
King Abdullah Medical Complex: Muhammed Abduldhaher, Wael Bajhamoum
King Faisal Specialist Hospital and Research Center, Jeddah, Kingdom of Saudi Arabia: Ismael Qushmaq
King Fahad Armed Forces Hospital: Sarah Shalhoub
Alahsa, Kingdom of Saudi Arabia
King Abdulaziz Hospital: Yusri Taha, Javed Memon, Shahinaz Bashir, Ibraheem Al-Dossary, Saleh Al Mekhloof
King Fahad Hospital: Bader Al-Muhainy
Dammam, Kingdom of Saudi Arabia
Dammam Medical Complex: Shehab Suliman
Al Khobar, Kingdom of Saudi Arabia
King Fahad Hospital of the University-Dammam University: Mohammed S Alshahrani.
Abha, Kingdom of Saudi Arabia
Aseer Central Hospital: Ali Al Bshabshe
Al-Madinah Al-Monawarah, Kingdom of Saudi Arabia
King Fahad Hospital: Ayman Kharaba, Ahmad Al Jabri
Ohoud Hospital: Ayman Kharaba, Magdy Farid, Alawi Alaidarous, Wael Alseraihi, Husam Shahada, Jinish Shimi
Taif, Kingdom of Saudi Arabia
King Faisal Hospital: Bader Alharthi, Osama Yasin
Buraidah, Kingdom of Saudi Arabia
Buraidah Central Hospital: Mohammed Alkathlan
Toronto, Canada
University of Toronto: Robert A Fowler
Charlottesville, VA, USA
University of Virginia School of Medicine: Frederick G Hayden
Funding
The study sponsor does not have any role in the study design, collection, management, analysis or interpretation of the data, or in writing the report. King Abdullah International Medical Research Center, Ministry of National Guard Health Affairs MNGHA, Mail Code: 1515 PO Box 22490 Riyadh 11426, Kingdom of Saudi Arabia
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Consortia
Contributions
YA conception and design, trial sites management, analytical plan, drafting of the manuscript, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. AA conception and design, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. HB conception and design, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. AD conception and design, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. SJ conception and design, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. SH conception and design, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. SK conception and design, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. MJ conception and design, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. AMD conception and design, trial sites management, drafting the manuscript, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. AMA trial sites management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. FH trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. AS trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. YM trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. GM trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. NMS trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. FEZ trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. JM trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. YT trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. AM trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. KM trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. IQ trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. AB trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. AK trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. SS trial site management, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. JJ analytical plan, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. RAF conception and design, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. FGH conception and design, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. MAH analytical plan, critical revision of the manuscript for important intellectual content, approval of the final version to be published and agreement to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The MIRACLE study is approved by the Scientific Committee and the Institutional Review Board at King Abdulaziz Medical City (RC15/142) and registered at the Saudi Food and Drug Authority (SFDA). The approval of the Ethics Committees and the SFDA will be secured from each participated sites before starting patient recruitment. Patients who meet the eligibility criteria or substitute decision-makers (for patients lacking decision-making capacity) of eligible patients will be approached to obtain informed consent for enrollment.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
SPIRIT 2013 Checklist: recommended items to address in a clinical trial protocol and related documents*. (DOC 120 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Arabi, Y.M., Alothman, A., Balkhy, H.H. et al. Treatment of Middle East Respiratory Syndrome with a combination of lopinavir-ritonavir and interferon-β1b (MIRACLE trial): study protocol for a randomized controlled trial. Trials 19, 81 (2018). https://doi.org/10.1186/s13063-017-2427-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-017-2427-0