
Abstract
Background
Negative symptoms of psychosis do not respond to the traditional therapy with first- or second-generation antipsychotics and are among main causes of a decrease in quality of life observed in individuals suffering from the disorder. Minocycline, a broad-spectrum tetracyclic antibiotic displaying neuroprotective properties has been suggested as a new potential therapy for negative symptoms. In the two previous clinical trials comparing minocycline and placebo, both added to the standard care, patients receiving minocycline showed increased reduction in negative symptoms. Three routes to neuroprotection by minocycline have been identified: neuroprotection against grey matter loss, anti-inflammatory action and stabilisation of glutamate receptors. However, it is not yet certain what the extent of the benefit of minocycline in psychosis is and what its mechanism is. We present a protocol for a multi-centre double-blind randomised placebo-controlled clinical trial entitled The Benefit of Minocycline on Negative Symptoms of Psychosis: Extent and Mechanism (BeneMin).
Methods
After providing informed consent, 226 participants in the early phase of psychosis will be randomised to receive either 100 mg modified-release capsules of minocycline or similar capsules with placebo for 12 months in addition to standard care. The participants will be tested for outcome variables before and after the intervention period. The extent of benefit will be tested via clinical outcome measures, namely the Positive and Negative Syndrome Scale score, social and cognitive functioning scores, antipsychotic medication dose equivalent and level of weight gain. The mechanism of action of minocycline will be tested via blood screening for circulating cytokines and magnetic resonance imaging with three-dimensional T1-weighted rapid gradient-echo, proton density T2-weighted dual echo and T2*-weighted gradient echo planar imaging with N-back task and resting state. Eight research centres in UK and 15 National Health Service Trusts and Health Boards will be involved in recruiting participants, performing the study and analysing the data.
Discussion
The BeneMin trial can inform as to whether in minocycline we have found a new and effective therapy against negative symptoms of psychosis.
The European Union Clinical Trial Register: EudraCT 2010-022463-35 with the registration finalised in July 2011. The recruitment in the trial started in January 2013 with the first patient recruited in March 2013.
Similar content being viewed by others


Background
Negative symptoms in psychosis
Psychosis leads to a significant decrease in a person’s quality of life [1], with negative symptoms contributing the most to impaired functional outcome [2]. Negative symptoms - reduction in emotional and social responsiveness, motivation, speech and movement [3] - respond the least to known antipsychotic treatments among all psychotic symptoms [4]. Their initial severity, together with duration of untreated psychosis (DUP) and cognitive impairments, is the best predictor of an individual’s subsequent impairment in quality of social and occupational functioning [5]. Their positive correlation with DUP links their aetiology to a neuropathic process progressing with continuance of untreated psychosis [6-11]. This hypothesis has led to an interest in neuroprotection during early stages of psychosis as a potential therapeutic target for negative symptoms.
Efficacy of minocycline for negative symptoms of psychosis
A broad-spectrum tetracyclic antibiotic, minocycline has neuroprotective properties, which could prevent the accumulation of negative symptoms in psychosis [12-15] while improving the prognosis of neurodegenerative diseases and traumatic or ischaemic central nervous system (CNS) insults [16-19]. Due to its lipophilic properties, it has exceptional potential for blood-brain barrier penetration [20]. It is also marked by its relatively low toxicity [21].
Two double-blind randomised placebo-controlled studies of minocycline as a neuroprotective agent for negative symptoms of psychosis have been completed [14,15]. The first was a 2-centre study in Brazil and Pakistan supervised by the University of Manchester with 144 participants [14]. The second, completed in Tel Aviv, Israel, recruited 70 relapsed patients with schizophrenia [15]. Both studies found significant treatment effects on negative symptoms with adjunctive minocycline. In the first trial, significant treatment effects were observed at 6 months, and in the second trial at 3 months. Furthermore, the 2-centre trial demonstrated that therapeutic effects were sustained at 12 months. No other trials investigating the efficacy of minocycline for negative symptoms have been registered in UK or US databases. However, to assess the extent and mechanism of the benefit of minocycline for negative symptoms in psychosis, a trial with a larger cohort is needed.
Mechanism of action of minocycline on negative symptoms
Although the effectiveness of minocycline in treating negative symptoms has been identified, its mechanism of action remains unresolved [22]. Three possible mechanisms of action have been posited:
-
1)
Neuroprotection against grey matter loss: minocycline may directly prevent neurodegeneration of grey matter in individuals with psychosis. Its neuroprotective properties have been shown in stroke [21,23], Parkinson’s disease [24,25], cerebral ischaemia, amyotrophic lateral sclerosis, Huntington’s disease and multiple sclerosis [26]. In psychosis, loss of grey matter occurs early in the course of the disease [27-30], is associated with DUP [31] and predicts diminished functional outcome [32]. By preventing grey matter loss, minocycline may limit negative symptoms.
-
2)
Anti-inflammatory action: the anti-inflammatory properties [33,34] of minocycline may prevent neural changes associated with the action of microglia and cytokines in psychosis [35]. The inflammatory response as a mechanism of schizophrenia has been suggested by studies demonstrating microglial activation [35,36]. The gene variants associated with risk of schizophrenia have been linked to increased levels of circulating cytokines [37]. A correlation between negative symptoms and levels of IL-10 cytokine has been observed in untreated psychosis [38]. Increased levels of IL-6 appears in medication-naïve patients with first episode of psychosis [39] and acutely relapsed inpatients [40], whereas elevated levels of IL-6 at the age of 9 doubles the risk of developing psychosis later in life [41]. Minocycline may reduce cytokine levels during psychosis thereby limiting negative symptoms.
-
3)
Stabilisation of N-methyl-D-aspartate (NMDA) glutamate receptors: minocycline may improve impaired function of the NMDA glutamate receptor which is thought to display impairment in schizophrenia [42]. Ketamine, which blocks NMDA receptors and causes dysfunctional release of glutamate [43,44], evokes schizophrenia-like negative symptoms in healthy individuals [45]. Minocycline can block ketamine action [46], thus potentially stabilising glutamate release in NMDA receptors [47]. Minocycline may limit negative symptoms either through direct action on glutamate release or through prevention of glutamate neurotoxicity on neuronal branching and glial cells [48]. Although not observable in vivo, this can be examined by the association between NMDA receptors and working memory [49,50].
The three mechanisms of action of minocycline may operate separately or jointly. Each represents a potential target for neuroprotectection, effective only when neurodegenerative processes are active and their adverse effects limitable. Thus, minocycline is likely to be observed as being most effective in the early stages of psychosis.
Benefits and risks of treatment with minocycline
The treatment of psychosis with minocycline may benefit patients by reducing their negative symptoms and, consequently, their difficulties in social and occupational function [5]. This treatment may also reduce the dose of antipsychotic drugs (APDs) necessary to stabilise a patient’s health, thus decreasing potential side-effects of APDs such as weight gain [4]. Finally, new targets for the treatment of psychosis may be discovered [51], which could elucidate the pathophysiology of psychosis and potential biomarkers of increased risk of developing it.
Treatment with minocycline has been associated with vestibular disturbances, gastro-intestinal upset and fatigue [52-54]. Nevertheless, our previous study [14] did not find any such link. Minocycline use has also been associated with the development of a systemic lupus erythematosus - like syndrome [55] with, however, an estimated incidence of 8.8 cases per 100,000 person-years [56]. Patches of discolouration on teeth and skin have also been observed during long-term therapy with minocycline [57,58]. In our previous study [14], three people in each treatment arm reported hyper-pigmentation, but only those in the minocycline arm withdrew from the trial. This was the only noted side-effect withdrawal.
The risks and side-effects observed during minocycline treatment are less severe than those associated with the available antipsychotic drugs, which include extrapyramidal symptoms [59-61], metabolic problems and sedation [62-68]. It is estimated that adding minocycline to standard treatment will have similar effect-size as was observed with a benefit of second-generation APDs over older APDs [62,69].
Rationale and aims of the BeneMin trial
Finding an effective treatment for negative symptoms in psychosis is of paramount importance due to their role in post-morbid functional outcome [2]. Minocycline has been identified as a potential agent for reducing negative symptoms [14,15]. Therefore, in BeneMin we will investigate the extent and mechanism of action of minocycline on negative symptoms in psychosis. Additionally, we will test whether characteristics such as premorbid and current IQ, DUP and cytokine genotype predict the response to minocycline.
Effectiveness hypotheses (EHs)
-
EH1) Added to the standard therapy, minocycline administered during the acute phase of psychosis limits development of negative symptoms in comparison to placebo.
-
EH2) Minocycline reduces side-effects associated with standard therapy such as weight gain in comparison to placebo.
-
EH3) Reduction of negative symptoms leads to improvement in function and life quality in patients treated with minocycline in comparison to placebo.
Mechanistic hypotheses (MHs)
-
MH1) In comparison to placebo, minocycline reduces grey matter degeneration, which occurs particularly during the early acute phase of the disease. The reduction in grey matter degeneration is observed mainly in the frontal lobes and is associated with reduction of negative symptoms.
-
MH2) In comparison to placebo, minocycline diminishes inflammatory action in the CNS thereby reducing negative symptoms. Decreased numbers of circulating cytokines in peripheral blood, and potentially reduced grey and white matter neurodegeneration and micro lesions in the CNS, are observed as the result of minocycline treatment.
-
MH3) In comparison to placebo, minocycline improves function of NMDA glutamate receptors and restores optimal levels of glutamate in the CNS, observed through improved cortical function of working memory. The improvement may be a direct result of minocycline action and may cease after the treatment stops or continue through the neuroprotective action of optimal glutamate levels.
Methods
Study design
BeneMin is a double-blind, randomised, placebo-controlled clinical trial investigating the extent and mechanism of action of minocycline on negative symptoms of psychosis in addition to standard APD therapy. Participants in an acute psychotic phase will be randomly allocated either to the minocycline or to the placebo arm and continue to receive the assigned treatment for 12 months. Both participants and investigators will be blind to treatment group, which will be guaranteed by a direct data-entry, digital database (OpenCDMS system). Separately, participants will be asked to donate fully-anonymised DNA for genotyping of the interleukin 6 (IL-6) gene [70] and for future investigations. The study will be conducted at eight research centres, and led by the University of Manchester (Table 1).
The EHs will be tested via clinical outcome variables: levels of negative and positive symptoms of psychosis, observed side-effects and subsequent quality of life. The MHs will be examined via biomarker outcome variables obtained through blood screening for circulating cytokines and magnetic resonance imaging (MRI). In addition to treatment effectiveness, mediators of treatment response such as DUP, cognitive function and IL-6 gene variants will be assessed.
A pre-post treatment design will be used with baseline measurements of the outcome variables taken before commencement of treatment (screening and randomisation visits) and repeated soon after the treatment has finished (month 12 visit). Clinical outcome variables will also be measured between the pre- and post-treatment assessments (month 2, 6 and 9 visits) to capture possible early therapeutic effects of minocycline. The last assessment will be performed 3 months after the participant has finished their treatment (that is 15 months post-randomisation).
Participants
Eligibility criteria
The BeneMin trial will recruit participants in an acute phase of psychosis within 5 years from their first diagnosis. The detailed inclusion and exclusion criteria of the participants are presented in Figure 1.

Eligibility and withdrawal criteria for participants of BeneMin.
Sample size and recruitment settings
We aim to enrol a total of 226 eligible participants among the 8 research centres. The predicted number of participants remaining in the trial at each stage is presented in the CONSORT diagram in Figure 2. The calculations are based on our previous study of minocycline [14] and a calibration study we performed before this trial [71]. The number of participants was chosen to ensure feasibility of the analysis of post-treatment MRI scans. To meet our recruitment aims we will collaborate with Local Research Networks of the English National Institute for Health Research and Scottish Mental Research Networks. The patients will be recruited via 15 National Health Service (NHS) Trusts and Health Boards (Table 1).

CONSORT diagram with predicted numbers of participants at each stage of the trial.
Suitable candidates will first be approached by delegated members of their clinical teams, who will assess each candidate’s eligibility and ask for their permission to be contacted by a project’s research assistant (RA). Eligible candidates will receive the BeneMin patient information leaflet explaining the trial. After expressing interest they will be approached by the RA who will again verify eligibility. Subsequently, the RA will obtain the candidate’s informed consent for participation in the trial, having verified that the candidate fully understands what is involved. Separate consent will be obtained for donating DNA to the bio-bank at the University of Manchester.
Withdrawal
At any time a participant can withdraw their consent for participation without giving reasons. The participant will be given an opportunity to discuss the reason for withdrawal and any adverse events (AE). If possible, the participant will be assessed by the investigator. Any potential AE will be followed up by the resident medical officer (RMO). If the participant withdraws their consent at any time beyond 6 months of treatment they will be asked to complete the full post-treatment assessment, followed 3 months later by the post-trial assessment. Their results will be included in the main analysis. The detailed withdrawal criteria are presented in Figure 1.
Randomisation procedure
After stratification by the research centre, permuted block randomisation integrated with the OpenCDMS system will be used to allocate participants to the treatment arm. After an investigator has requested randomisation for a participant, the OpenCDMS will use the algorithm to allocate the participant to the treatment arm. Subsequently, it will notify a local pharmacy regarding the serial number of a medication kit to use. Participant’s allocation to the study arm will be known only to the OpenCDMS system.
Planned intervention
Participants will take capsules containing either 100 mg minocycline (modified-release) or matching placebo, 2 per day for the first 2 weeks and then 3 per day for the reminder of the 12-month treatment period in addition to standard therapy. The maximum dose of modified-release minocycline is 3 × 100 mg per 24 hours. Minocycline and placebo will be manufactured, controlled and distributed to the Trusts’ pharmacies by Catalent, Bolton, UK, in accordance with the requirements of the Medicines and Healthcare Products Regulatory Agency (MHRA).
Clinical outcome measures
We will test hypotheses of minocycline efficacy by assessing changes in primary and secondary clinical outcome measures over treatment.
Primary clinical outcome
Severity of negative symptoms of psychosis as measured by the negative symptoms subscale of the Positive and Negative Syndrome Scale (PANSS), an instrument commonly used to assess the efficacy of treatment in schizophrenia [72] consisting of a positive symptoms subscale, a negative symptoms subscale and a general psychopathology subscale [73].
Secondary clinical outcomes
-
1)
Body weight and body mass index [74] as a measure of weight gain, a side-effect of the standard APD therapy.
-
2)
Severity of global and positive symptoms of psychosis as measured by the full PANSS and the PANSS positive symptoms subscale.
-
3)
General and social function as measured by:
-
Global Assessment of Functioning from the Diagnostic and Statistical Manual, fourth edition (DSM-IV) [75,76], a scale assessing psychological, social and occupational function on a hypothetical continuum of health and illness;
-
the Social Functioning Scale [77], a self-rating scale assessing social functioning in domains such as social engagement, interpersonal behaviour, pro-social activities, independence or employment.
-
-
4)
Cognitive function as measured by:
-
a short Wechsler Adult Intelligence Scale III for patients with schizophrenia [78], consisting of the information, block design, arithmetic and digit-symbol subtests. This will provide a measure of current IQ and processing speed [79];
-
the Wechsler Test of Adult Reading [80], a reading test which estimates premorbid IQ [81];
-
Verbal fluency requiring individuals to generate words in response to phonetic or semantic criteria [82];
-
the Auditory-Verbal Learning Task [83-85], a test of word list learning and recall.
-
-
5)
APD dose expressed in chlorpromazine equivalent units [86], assessing the dose of APD required for the patient’s stabilisation.
Biomarker outcome measures
We will examine the mechanism of action of minocycline by assessing changes in primary and secondary biomarker outcome measures over treatment. The biomarker outcomes will be measured via cytokine blood screening and MRI of the brain.
Cytokine blood screening
A blood sample from the participant will be collected into an EDTA tube during a screening visit. Portions of plasma will be separated from the sample for measurement of the cytokine markers associated with inflammatory response in previous studies, namely, IL-6 [87], interleukin-1 receptor antagonist (IL-1RA) [88], monocyte chemotactic protein 1 (MCP-1/CCL2) [89] and C-reactive protein (CRP) [90]. Measurements of IL-6, IL-1RA and MCP-1 will follow a method applied in previous studies of stroke [91,92] and will use multiplex (Luminex®, Manchester, UK) assays. For assessment of CRP level, a sensitive immunoassay will be used [93]. The lowest value among the markers will be classified as the baseline measure of cytokine concentration. Successive blood samples will be collected, and the cytokine tests repeated at month 6, post-treatment (month 12) and post-trial (month 15) visits.
Multi-centre magnetic resonance imaging
Three MRI sequences will be performed for each participant pre-treatment (randomisation visit) and post-treatment (12 month visit): three-dimensional T1-weighted rapid gradient-echo (MPRAGE/SPGR); proton density T2-weighted dual echo (PD/T2); and T2*-weighted gradient echo planar imaging (EPI) with N-back task and resting state. MPRAGE/SPGR, a high-resolution structural scan, will be used to assess volume and, thus, neurodegeneration of grey matter. PD/T2 will measure the volume of grey and white matter and of neuro-inflammatory lesions, and will be applied to perform multi-channel texture analysis [94], thus supporting the measurements of neuro-inflammation. EPI N-back via blood-oxygenation-level-dependent (BOLD) contrast will be used to test the neural function associated with the working memory network (dorsolateral-prefrontal, anterior cingulate and parietal cortices) [95] and, thus, NMDA receptors [49,50], whereas EPI resting state will be applied to observe the default network (medial temporal, medial prefrontal and posterior cingulate cortices) [96,97]. Both sequences will be used to examine functional connectivity, and be merged at acquisition into one sequence to test endogenous neural dynamics recovery from cognitive effort [98].
N-back task
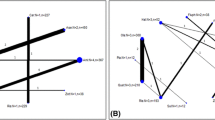
In the N-back task, a well-established method for observing the working memory network [99], the participant presses a button corresponding to the number observed N images previously. The numbers will range from 1 to 4 and the participant will hold a 4-button response box in their right hand. The task will consist of 3 types of blocks, 0-back, 1-back, 2-back, each repeated 5 times in quasi-randomised fashion (the same randomised pattern for each participant). Each block will contain an instruction image (3,750 ms) followed by 15 quasi-randomised trials comprising an image presenting the number (250 ms) and a blank image (1,500 ms) (Figure 3). The response can be given when either the number or the blank image are presented. Reaction times and response accuracy are recorded. After the task has finished an image will appear instructing the participant to close their eyes for the remaining part of the sequence.

N-back task and resting state diagram.
Multi-centre MRI reproducibility
Multi-centre imaging studies are an effective way to reach a target sample size in a clinical trial within a manageable time-frame. However, due to technical and setting differences between MRI scanners, the question of reproducibility and comparability of data arises. In BeneMin the MRI data will be collected in six MRI centres (Table 1) via six 3T MRI scanners, including two Philips Achieva (Philips Medical Systems, Best, Netherlands), two Siemens Trim Trio, one Siemens Verio (Siemens Medical Systems, Erlangen, Germany) and one GE Signa (General Electric, Milwaukee, WI, USA). Due to technical differences between scanners, a direct replication of scanning parameters would not result in functionally equivalent MRI protocols. Therefore, to develop BeneMin MRI protocols we have applied expertise established by the Alzheimer’s disease neuroimaging initiative (ADNI) [100], a multi-centre imaging project aiming at standardisation of MRI across sites and manufacturers, and conducted a calibration study [71] prior to the trial. The calibration study, in which 12 healthy volunteers were scanned repeatedly in 5 different MRI centres with a protocol similar to ours, showed that between-centre differences accounted for 10% of variation in structural MRI and less than 10% in functional MRI, whereas centre-by-individual interaction was on the level of < 5%. In BeneMin the specifications for each sequence are:
-
1)
MPRAGE/SPGR: voxel size of approximately 1 × 1 × 1 mm3, phase encode on the anterior-posterior plane, whole brain recorded;
-
2)
PD/T2: voxel size of approximately 1 × 1 × 3 mm3, phase encode on the right-left plane, whole brain recorded;
-
3)
EPI: TR = 2,000 ms, 748 three-dimensional volumes, voxel size of approximately 3 × 3 × 4.5 mm3, slices aligned to AC-PC axis, phase encode on the anterior-posterior plane, whole brain recorded.
These parameters have been fixed as their variations cannot easily be compensated during analysis. After these specifications were incorporated, each MRI centre developed the remaining parameters of the local BeneMin MRI sequences based on standardised protocols of ADNI complemented by the centre’s expertise. The protocols thus developed will be used in BeneMin, and are presented in Table 2.
Primary biomarker outcomes
-
1)
Medical prefrontal grey matter volume (MH1).
-
2)
Circulating cytokine IL-6 concentration (MH2).
-
3)
Dorsolateral-prefrontal cortex BOLD response, accuracy and functional connectivity in N-back task (MH3).
Secondary biomarker outcomes
-
1)
Total and other regional grey matter volumes (MH1).
-
2)
Volume and multi-channel features of grey and white matter as measured by PD/T2 and of neuro-inflammatory lesions, and concentration of the remaining cytokine markers (MH2).
-
3)
Functional connectivity and the distribution of Hurst exponent of fMRI noise in resting state (MH3).
Side-effects and adverse events
Possible side-effects and potential co-morbidities will be recorded. Depression will be assessed with self-rating Calgary Depression Scale for Schizophrenia [101], extrapyramidal symptoms with the Simpson-Angus Scale [102], the Barnes Akathisia Rating Scale [103], the Abnormal Involuntary Movements Scale [104] and APD subjective side-effects with the Antipsychotic Non-Neurological Side-Effects Rating Scale [105]. The seven-point adherence to treatment scale will be also used [106]. Additionally, any AE such as occurrence of an undesirable medical condition or deterioration of an existing medical concern will be recorded throughout the treatment duration and the post-trial period.
Assessment schedule
Each participant will undergo seven assessment sessions, which will include the screening, the pre- and post-treatment assessments, and the sessions between onset and completion of treatment. The detailed measurements taken during each session are presented in Table 3.
Analysis
Statistical analysis
A single round of analysis will be undertaken after all outcome results have been collected. Treatment effects will be assessed using the intention-to-treat method unless a significant amount of non-adherence to treatment is observed, in which case the complier-average causal effect method will be applied. In both cases non-adherence will be accounted for, since both methods allow for missing data via either inverse probability weights [107,108] or maximum likelihood estimation [109,110], and non-adherence is likely to correlate with withdrawals. Group differences in outcomes and mediators of treatment response will be assessed via a random effects model for longitudinal data, whereas MHs will be tested with instrumental variable methods [111].
MRI analysis
All MRI scans will be visually inspected for quality and possible acquisition artefacts. Subsequently, each scan will undergo standardised modality-specific temporal and spatial pre-processing:
-
1)
MPRAGE/SPGR and PD/T2: brain tissue extraction, segmentation via scan-specific tissue priors, non-linear registration to the Montreal Neurological Institute 152 (MNI) standard space [112], smoothing with an isotropic Gaussian kernel;
-
2)
EPI: motion and slice-timing correction, brain tissue extraction, non-linear co-registration with MNI-registered MPRAGE/SPGR, smoothing with an isotropic Gaussian kernel, intensity normalisation, high pass temporal filter.
For both MPRAGE/SPGR and PD/T2, voxel-based morphometry analysis will be performed [113], with additional lesion count in PD/T2 [114]. Texture features identified as neuro-inflammation markers in multiple sclerosis [94] will be measured in PD/T2. In EPI a general linear model will be used to model the BOLD signal [115]. Additionally, for the EPI resting state, the Hurst exponent will be extracted [116]. Group comparisons for all measures will be performed for the whole brain and for the regions of interest defined as belonging to positive and negative task networks [95-97] and located via MNI Atlases [117]. A mixed effects model for repeated measures will be used to evaluate treatment effectiveness defined as interaction between treatment arm and time. Additionally, a partial least squares model will be applied to identify brain structures and activation patterns associated with the extent of symptomatic change. Furthermore, seed-based correlations of voxel time-series will be used in EPI to establish treatment effects on functional connectivity of the positive and negative task networks [118]. All MRI analyses will be performed via non-parametric testing, with appropriate corrections for multiple comparisons [119].
Ethics approval and research sponsor
The study design and the described procedures have been approved by the National Research Ethics Service Committee North West - Greater Manchester Central (REC reference number: 11/NW/0218). The following local Research and Development departments of NHS Trusts and Health Boards after being presented with the aforementioned approval agreed to host the study: the Manchester Mental Health and Social Care Trust Research and Innovation Office, the Greater Manchester West Mental Health NHS Foundation Trust Research and Development Office, the Pennine Care NHS Foundation Trust Quality Assurance, Research and Innovation Unit, the Lancashire Care NHS Foundation Trust Research Department, the Cheshire and Wirral Partnership NHS Foundation Trust Academic Unit, the Cambridgeshire and Peterborough NHS Foundation Trust Research and Development Department, the Norfolk and Suffolk NHS Foundation Trust Research and Development Office, the UCL/UCLH Joint Research Office, the North Central London Research Consortium, the South London and Maudsley/IoPPN Research and Development Office, the NHS Lothian Academic and Clinical Central Office for Research and Development, the NHS Fife Research and Development Resource Centre and the Birmingham and Solihull Mental Health Foundation NHS Trust Research and Development Department. The Manchester Mental Health and Social Care Trust is the research sponsor and will be responsible for monitoring, audit and pharmacovigilance of the trial. The trial has the approval of MHRA.
Discussion
Minocycline has the potential to improve the treatment of negative symptoms in psychosis and thereby protect premorbid levels of functioning and consequently the quality of life for many patients. The medication has low toxicity and is not expensive to manufacture, hence it could be a straightforward addition to standard care. Furthermore, minocycline may reduce the dose of antipsychotic drugs necessary to stabilise a patient’s condition and thus limit side-effects associated with standard antipsychotic therapy.
Therapy with minocycline can potentially prevent irreparable neurodegenerative changes observed in the early stages of psychosis, which are proposed as a cause of negative symptoms. If the mechanism of action of minocycline is revealed, new targets for therapy of psychosis will be established and novel medications with clinical properties associated with the mechanism may be developed. Discovering the mechanism could also elucidate a neural basis of psychosis itself.
BeneMin as a multi-site clinical trial will evaluate the extent and mechanism of efficacy of minocycline for negative symptoms in a manageable time-frame. However, the multi-site character of BeneMin raises an issue of reproducibility and comparability of the data. Therefore, standardisation of procedures such as MRI and compatible training for the data collectors will be of key importance. On the other hand, recruiting participants from many geographical locations increases ecological validity of the sample which in turn helps with generalisation of the findings.
Trial status
The trial is ongoing. Participants are currently being recruited.
Abbreviations
- ADNI:
-
Alzheimer’s disease neuroimaging initiative
- AE:
-
adverse event
- APD:
-
antipsychotic drug
- BOLD:
-
blood-oxygenation-level-dependent
- CNS:
-
central nervous system
- CRP:
-
C-reactive protein
- DSM-IV:
-
Diagnostic and Statistical Manual, fourth edition
- DUP:
-
days of untreated psychosis
- EHs:
-
effectiveness hypotheses
- EPI:
-
echo planar imaging
- IL-1RA:
-
interleukin-1 receptor antagonist
- IL-6:
-
interleukin 6
- MCP-1:
-
monocyte chemotactic protein 1
- MHs:
-
mechanisitic hypotheses
- MHRA:
-
The Medicine and Healthcare Products Regulatory Agency
- MNI:
-
Montreal Neurological Institute
- MRI:
-
magnetic resonance imaging
- NHS:
-
The National Health Service
- NMDA:
-
N-methyl-D-aspartate
- PANSS:
-
The Positive and Negative Syndrome Scale
- PIC:
-
patient information centre
- RA:
-
research assistant
- RMO:
-
resident medical officer
References
Patterson TL, Kaplan RM, Grant I, Semple SJ, Moscona S, Koch WL, et al. Quality of well-being in late-life psychosis. Psychiatry Res. 1996;63:169–81.
Barnes TR, Leeson VC, Mutsatsa SH, Watt HC, Hutton SB, Joyce EM. Duration of untreated psychosis and social function: 1-year follow-up study of first-episode schizophrenia. Br J Psychiatry. 2008;193:203–9.
American Psychiatric Association., American Psychiatric Association. DSM-5 Task Force. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Association; 2013.
Leucht S, Pitschel-Walz G, Abraham D, Kissling W. Efficacy and extrapyramidal side-effects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials. Schizophr Res. 1999;35:51–68.
Ho B-C, Nopoulos P, Flaum M, Arndt S, Andreasen NC. Two-year outcome in first-episode schizophrenia: predictive value of symptoms for quality of life. Am J Psychiatr. 1998;155:1196–201.
Drake RJ, Haley CJ, Akhtar S, Lewis SW. Causes and consequences of duration of untreated psychosis in schizophrenia. Br J Psychiatry. 2000;177:511–5.
Marshall M, Lewis S, Lockwood A, Drake R, Jones P, Croudace T. Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: a systematic review. Arch Gen Psychiatry. 2005;62:975–83.
McGlashan TH. Duration of untreated psychosis in first-episode schizophrenia: marker or determinant of course? Biol Psychiatry. 1999;46:899–907.
Melle I, Larsen TK, Haahr U, Friis S, Johannesen JO, Opjordsmoen S, et al. Prevention of negative symptom psychopathologies in first-episode schizophrenia: two-year effects of reducing the duration of untreated psychosis. Arch Gen Psychiatry. 2008;65:634–40.
Perkins DO, Gu H, Boteva K, Lieberman JA. Relationship between duration of untreated psychosis and outcome in first-episode schizophrenia: a critical review and meta-analysis. Am J Psychiatr. 2005;162:1785–804.
Waddington J, Youssef H, Kinsella A. Sequential cross-sectional and 10-year prospective study of severe negative symptoms in relation to duration of initially untreated psychosis in chronic schizophrenia. Psychol Med. 1995;25:849–57.
Miyaoka T, Yasukawa R, Yasuda H, Hayashida M, Inagaki T, Horiguchi J. Possible antipsychotic effects of minocycline in patients with schizophrenia. Prog Neuro-Psychopharmacol Biol Psychiatry. 2007;31:304–7.
Miyaoka T, Wake R, Furuya M, Liaury K, Ieda M, Kawakami K, et al. Minocycline as adjunctive therapy for patients with unipolar psychotic depression: an open-label study. Prog Neuro-Psychopharmacol Biol Psychiatry. 2012;37:222–6.
Chaudhry IB, Hallak J, Husain N, Minhas F, Stirling J, Richardson P, et al. Minocycline benefits negative symptoms in early schizophrenia: a randomised double-blind placebo-controlled clinical trial in patients on standard treatment. J Psychopharmacol. 2012;26:1185–93.
Levkovitz Y, Mendlovich S, Riwkes S, Braw Y, Levkovitch-Verbin H, Gal G, et al. A double-blind, randomized study of minocycline for the treatment of negative and cognitive symptoms in early-phase schizophrenia. J Clin Psychiatry. 2010;71:138.
Elewa HF, Hilali H, Hess DC, Machado LS, Fagan SC. Minocycline for short-term‐term neuroprotection. Pharmacotherapy. 2006;26:515–21.
Stirling DP, Koochesfahani KM, Steeves JD, Tetzlaff W. Minocycline as a neuroprotective agent. Neuroscientist. 2005;11:308–22.
Wells JE, Hurlbert RJ, Fehlings MG, Yong VW. Neuroprotection by minocycline facilitates significant recovery from spinal cord injury in mice. Brain. 2003;126:1628–37.
Zhang W, Narayanan M, Friedlander RM. Additive neuroprotective effects of minocycline with creatine in a mouse model of ALS. Ann Neurol. 2003;53:267–70.
Saivin S, Houin G. Clinical pharmacokinetics of doxycycline and minocycline. Clin Pharmacokinet. 1988;15:355–66.
Sakata H, Niizuma K, Yoshioka H, Kim GS, Jung JE, Katsu M, et al. Minocycline-preconditioned neural stem cells enhance neuroprotection after ischemic stroke in rats. J Neurosci. 2012;32:3462–73.
Koistinaho J, Koistinaho M. Minocycline, a tetracycline derivative, as a potential protective agent for acute stroke. In: Immunological mechanisms and therapies in brain injuries and stroke. New York: Springer; 2014. p. 275–85.
Fan X, Lo EH, Wang X. Effects of minocycline plus tissue plasminogen activator combination therapy after focal embolic stroke in type 1 diabetic rats. Stroke. 2013;44:745–52.
Dixit A, Srivastava G, Verma D, Mishra M, Singh PK, Prakash O, et al. Minocycline, levodopa and MnTMPyP induced changes in the mitochondrial proteome profile of MPTP and maneb and paraquat mice models of Parkinson’s disease. Biochim Biophys Acta (BBA) - Mol Basis Dis. 2013;1832:1227–40.
Inamdar AA, Chaudhuri A, O’Donnell J. The protective effect of minocycline in a paraquat-induced Parkinson’s disease model in Drosophila is modified in altered genetic backgrounds. Park Dis. 2012;2012:1–16.
Kim H-S, Suh Y-H. Minocycline and neurodegenerative diseases. Behav Brain Res. 2009;196:168–79.
Whitford TJ, Grieve SM, Farrow TF, Gomes L, Brennan J, Harris AW, et al. Progressive grey matter atrophy over the first 2–3 years of illness in first-episode schizophrenia: a tensor-based morphometry study. Neuroimage. 2006;32:511–9.
Chua SE, Cheung C, Cheung V, Tsang JT, Chen EY, Wong JC, et al. Cerebral grey, white matter and csf in never-medicated, first-episode schizophrenia. Schizophr Res. 2007;89:12–21.
Theberge J, Williamson KE, Aoyama N, Drost DJ, Manchanda R, Malla AK, et al. Longitudinal grey-matter and glutamatergic losses in first-episode schizophrenia. Br J Psychiatry. 2007;191:325–34.
Pantelis C, Velakoulis D, McGorry PD, Wood SJ, Suckling J, Phillips LJ, et al. Neuroanatomical abnormalities before and after onset of psychosis: a cross-sectional and longitudinal MRI comparison. Lancet. 2003;361:281–8.
Malla AK, Bodnar M, Joober R, Lepage M. Duration of untreated psychosis is associated with orbital–frontal grey matter volume reductions in first episode psychosis. Schizophr Res. 2011;125:13–20.
Cahn W, Van Haren N, Pol HH, Schnack H, Caspers E, Laponder D, et al. Brain volume changes in the first year of illness and 5-year outcome of schizophrenia. Br J Psychiatry. 2006;189:381–2.
Bastos LFS, Merlo LA, Rocha LTS, Coelho MM. Characterization of the antinociceptive and anti-inflammatory activities of doxycycline and minocycline in different experimental models. Eur J Pharmacol. 2007;576:171–9.
Wang J, Wei Q, Wang C-Y, Hill WD, Hess DC, Dong Z. Minocycline up-regulates Bcl-2 and protects against cell death in mitochondria. J Biol Chem. 2004;279:19948–54.
Monji A, Kato T, Kanba S. Cytokines and schizophrenia: microglia hypothesis of schizophrenia. Psychiatry Clin Neurosci. 2009;63:257–65.
van Berckel BN, Bossong MG, Boellaard R, Kloet R, Schuitemaker A, Caspers E, et al. Microglia activation in recent-onset schizophrenia: a quantitative < i > (R)</i > −[< sup > 11</sup > C] PK11195 positron emission tomography study. Biol Psychiatry. 2008;64:820–2.
Paul-Samojedny M, Kowalczyk M, Suchanek R, Owczarek A, Fila-Danilow A, Szczygiel A, et al. Functional polymorphism in the interleukin-6 and interleukin-10 genes in patients with paranoid schizophrenia - a case–control study. J Mol Neurosci. 2010;42:112–9.
van Kammen D, McAllister C, Kelley M. Relationship between immune and behavioral measures in schizophrenia. Vienna: Springer; 1997.
Upthegrove R, Manzanares-Teson N, Barnes NM. Cytokine function in medication-naive first episode psychosis: a systematic review and meta-analysis. Schizophr Res. 2014;155:101–8.
Miller BJ, Buckley P, Seabolt W, Mellor A, Kirkpatrick B. Meta-analysis of cytokine alterations in schizophrenia: clinical status and antipsychotic effects. Biol Psychiatry. 2011;70:663–71.
Khandaker GM, Pearson RM, Zammit S, Lewis G, Jones PB. Association of serum interleukin 6 and C-reactive protein in childhood with depression and psychosis in young adult life a population-based longitudinal study. JAMA Psychiatry. 2014;71:1121–8.
Olney JW, Newcomer JW, Farber NB. NMDA receptor hypofunction model of schizophrenia. J Psychiatr Res. 1999;33:523–33.
Hirota K, Lambert DG. Ketamine: its mechanism(s) of action and unusual clinical uses. 1996.
Deakin JW, Lees J, McKie S, Hallak JE, Williams SR, Dursun SM. Glutamate and the neural basis of the subjective effects of ketamine: a pharmaco–magnetic resonance imaging study. Arch Gen Psychiatry. 2008;65:154–64.
Newcomer JW, Farber NB, Jevtovic-Todorovic V, Selke G, Melson AK, Hershey T, et al. Ketamine-induced NMDA receptor hypofunction as a model of memory impairment and psychosis. Neuropsychopharmacology. 1999;20:106–18.
Choi SH, Lee DY, Chung ES, Hong YB, Kim SU, Jin BK. Inhibition of thrombin‐induced microglial activation and NADPH oxidase by minocycline protects dopaminergic neurons in the substantia nigra in vivo. J Neurochem. 2005;95:1755–65.
Monte AS, de Souza GC, McIntyre RS, Soczynska JK, dos Santos JV, Cordeiro RC, et al. Prevention and reversal of ketamine-induced schizophrenia related behavior by minocycline in mice: possible involvement of antioxidant and nitrergic pathways. J Psychopharmacol. 2013;27:1032–43.
Goff DC, Coyle JT. The emerging role of glutamate in the pathophysiology and treatment of schizophrenia. Am J Psychiatr. 2001;158:1367–77.
Lee I, Kesner RP. Differential contribution of NMDA receptors in hippocampal subregions to spatial working memory. Nat Neurosci. 2002;5:162–8.
Lisman JE, Fellous J-M, Wang X-J. A role for NMDA-receptor channels in working memory. Nat Neurosci. 1998;1:273–5.
Correll CU, Hauser M, Auther AM, Cornblatt BA. Research in people with psychosis risk syndrome: a review of the current evidence and future directions. J Child Psychol Psychiatry. 2010;51:390–431.
Fanning WL, Gump DW, Sofferman RA. Side effects of minocycline: a double-blind study. Antimicrob Agents Chemother. 1977;11:712–7.
Goulden V, Glass D, Cunliffe W. Safety of long‐term high‐dose minocycline in the treatment of acne. Br J Dermatol. 1996;134:693–5.
Smith K, Leyden JJ. Safety of doxycycline and minocycline: a systematic review. Clin Ther. 2005;27:1329–42.
Gough A, Chapman S, Wagstaff K, Emery P, Elias E. Minocycline induced autoimmune hepatitis and systemic lupus erythematosus-like syndrome. BMJ. 1996;312:169–72.
Garner SE, Eady A, Bennett C, Newton JN, Thomas K, Popescu CM. Minocycline for acne vulgaris: efficacy and safety. Cochrane Database Syst Rev. 2012;8, CD002086.
Good M, Hussey D. Minocycline: stain devil? Br J Dermatol. 2003;149:237–9.
White SW, Besanceney C. Systemic pigmentation from tetracycline and minocycline therapy. Arch Dermatol. 1983;119:1–2.
Miller CH, Mohr F, Umbricht D, Woerner M, Fleischhacker WW, Lieberman JA. The prevalence of acute extrapyramidal signs and symptoms in patients treated with clozapine, risperidone, and conventional antipsychotics. J Clin Psychiatry. 1998;59(2):69–75.
Casey DE. Neuroleptic drug-induced extrapyramidal syndromes and tardive dyskinesia. Schizophr Res. 1991;4:109–20.
Yang S, Yang YK, Chong M, Yang Y, Chang W, Lai C. Risk of extrapyramidal syndrome in schizophrenic patients treated with antipsychotics: a population-based study. Clinical Pharmacology & Therapeutics. 2007;81:586–94.
Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373:31–41.
Haddad PM, Sharma SG. Adverse effects of atypical antipsychotics. CNS Drugs. 2007;21:911–36.
Henderson DC. Atypical antipsychotic-induced diabetes mellitus. CNS Drugs. 2002;16:77–89.
Kane JM, Sharif ZA. Atypical antipsychotics: sedation versus efficacy. J Clin Psychiatry. 2007;69:18–31.
Miller DD. Atypical antipsychotics: sleep, sedation, and efficacy. Prim Care Companion J Clin Psychiatry. 2004;6:3.
Nasrallah HA, Newcomer JW. Atypical antipsychotics and metabolic dysregulation: evaluating the risk/benefit equation and improving the standard of care. J Clin Psychopharmacol. 2004;24:S7–14.
Tschoner A, Engl J, Laimer M, Kaser S, Rettenbacher M, Fleischhacker W, et al. Metabolic side effects of antipsychotic medication. Int J Clin Pract. 2007;61:1356–70.
Lieberman JA, Tollefson G, Tohen M, Green AI, Gur RE, Kahn R, et al. Comparative efficacy and safety of atypical and conventional antipsychotic drugs in first-episode psychosis: a randomized, double-blind trial of olanzapine versus haloperidol. Am J Psychiatr. 2003;160:1396–404.
Ferguson-Smith AC, Chen Y-F, Newman MS, May LT, Sehgal PB, Ruddle FH. Regional localization of the interferon-β2B-cell stimulatory factor 2/hepatocyte stimulating factor gene to human chromosome 7p15-p21. Genomics. 1988;2:203–8.
Suckling J, Barnes A, Job D, Brennan D, Lymer K, Dazzan P, et al. The neuro/PsyGRID calibration experiment. Hum Brain Mapp. 2012;33:373–86.
Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel RR. What does the PANSS mean? Schizophr Res. 2005;79:231–8.
Kay SR, Flszbein A, Opfer LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13:261.
Keys A, Fidanza F, Karvonen MJ, Kimura N, Taylor HL. Indices of relative weight and obesity. J Chronic Dis. 1972;25:329–43.
Hall RC. Global assessment of functioning: a modified scale. Psychosomatics. 1995;36:267–75.
Startup M, Jackson MC, Bendix S. The concurrent validity of the Global Assessment of Functioning (GAF). Br J Clin Psychol. 2002;41:417–22.
Birchwood M, Smith J, Cochrane R, Wetton S, Copestake S. The Social Functioning Scale. The development and validation of a new scale of social adjustment for use in family intervention programmes with schizophrenic patients. Br J Psychiatry. 1990;157:853–9.
Blyler CR, Gold JM, Iannone VN, Buchanan RW. Short form of the WAIS-III for use with patients with schizophrenia. Schizophr Res. 2000;46:209–15.
Leeson VC, Barnes TR, Harrison M, Matheson E, Harrison I, Mutsatsa SH, et al. The relationship between IQ, memory, executive function, and processing speed in recent-onset psychosis: 1-year stability and clinical outcome. Schizophr Bull. 2010;36:400–9.
Green RE, Melo B, Christensen B, Ngo L-A, Monette G, Bradbury C. Measuring premorbid IQ in traumatic brain injury: an examination of the validity of the Wechsler Test of Adult Reading (WTAR). J Clin Exp Neuropsychol. 2008;30:163–72.
Wechsler D. Wechsler test of adult reading: WTAR. New York: Psychological Corporation; 2001.
Joyce E, Collinson S, Crichton P. Verbal fluency in schizophrenia: relationship with executive function, semantic memory and clinical alogia. Psychol Med. 1996;26:39–49.
Lezak MD. Neuropsychological assessment. New York: Oxford University Press; 2004.
Rey A. L’examen clinique en psychologie. 1958.
Schmidt M. Rey auditory verbal learning test: a handbook. Los Angeles: Western Psychological Services; 1996.
Woods SW. Chlorpromazine equivalent doses for the newer atypical antipsychotics. J Clin Psychiatry. 2003;64:663–7.
Yudkin JS, Kumari M, Humphries SE, Mohamed-Ali V. Inflammation, obesity, stress and coronary heart disease: is interleukin-6 the link? Atherosclerosis. 2000;148:209–14.
Dinarello CA. The interleukin-1 family: 10 years of discovery. FASEB J. 1994;8:1314–25.
Carr MW, Roth SJ, Luther E, Rose SS, Springer TA. Monocyte chemoattractant protein 1 acts as a T-lymphocyte chemoattractant. Proc Natl Acad Sci. 1994;91:3652–6.
Koenig W, Sund M, Fröhlich M, Fischer H-G, Löwel H, Döring A, et al. C-reactive protein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men results from the MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Augsburg Cohort Study, 1984 to 1992. Circulation. 1999;99:237–42.
Emsley H, Smith C, Georgiou R, Vail A, Hopkins S, Rothwell N, et al. A randomised phase II study of interleukin-1 receptor antagonist in acute stroke patients. J Neurol Neurosurg Psychiatry. 2005;76:1366–72.
Emsley HC, Smith CJ, Gavin CM, Georgiou RF, Vail A, Barberan EM, et al. Clinical outcome following acute ischaemic stroke relates to both activation and autoregulatory inhibition of cytokine production. BMC Neurol. 2007;7:5.
Holt I, Cooper R, Denton J, Meager A, Hopkins S. Cytokine inter-relationships and their association with disease activity in arthritis. Rheumatology. 1992;31:725–33.
Zhang J, Tong L, Wang L, Li N. Texture analysis of multiple sclerosis: a comparative study. Magn Reson Imaging. 2008;26:1160–6.
Klingberg T, O’Sullivan BT, Roland PE. Bilateral activation of fronto-parietal networks by incrementing demand in a working memory task. Cereb Cortex. 1997;7:465–71.
Fransson P, Marrelec G. The precuneus/posterior cingulate cortex plays a pivotal role in the default mode network: evidence from a partial correlation network analysis. Neuroimage. 2008;42:1178–84.
Greicius MD, Krasnow B, Reiss AL, Menon V. Functional connectivity in the resting brain: a network analysis of the default mode hypothesis. Proc Natl Acad Sci. 2003;100:253–8.
Barnes A, Bullmore ET, Suckling J. Endogenous human brain dynamics recover slowly following cognitive effort. PLoS One. 2009;4:e6626.
Owen AM, McMillan KM, Laird AR, Bullmore E. N‐back working memory paradigm: a meta‐analysis of normative functional neuroimaging studies. Hum Brain Mapp. 2005;25:46–59.
Jack CR, Bernstein MA, Fox NC, Thompson P, Alexander G, Harvey D, et al. The Alzheimer’s disease neuroimaging initiative (ADNI): MRI methods. J Magn Reson Imaging. 2008;27:685–91.
Addington D, Addington J, Maticka-Tyndale E. Specificity of the Calgary Depression Scale for schizophrenics. Schizophr Res. 1994;11:239–44.
Simpson G, Angus J. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand. 1970;45:11–9.
Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry. 1989;154:672–6.
Lane RD, Glazer WM, Hansen TE, Berman WH, Kramer SI. Assessment of tardive dyskinesia using the Abnormal Involuntary Movement Scale. J Nerv Ment Dis. 1985;173:353–7.
Yusufi B, Mukherjee S, Aitchison K, Dunn G, Page E, Barnes T. Reliability of the antipsychotic non-neurological side effects rating scale (ANNSERS). J Psychopharmacol. 2005;19:A10.
Hayward P. Medication self-management: a preliminary report on an intervention to improve medication compliance. J Ment Health. 1995;4:511–8.
Everitt B, Pickles A. Statistical aspects of the design and analysis of clinical trials. London: World Scientific; 2004.
Heyting A, Tolboom J, Essers J. Statistical handling of drop‐outs in longitudinal clinical trials. Stat Med. 1992;11:2043–61.
Dunn G, Maracy M, Dowrick C, Ayuso-Mateos J, Dalgard O, Page H, et al. The Outcomes of Depression International (ODIN) Group (2003). Estimating psychological treatment effects from an RCT with both non-compliance and loss to follow-up. Br J Psychiatry. 2003;183:323–31.
Dunn G, Maracy M, Tomenson B. Estimating treatment effects from randomized clinical trials with noncompliance and loss to follow-up: the role of instrumental variable methods. Stat Methods Med Res. 2005;14:369–95.
Emsley R, Dunn G, White IR. Mediation and moderation of treatment effects in randomised controlled trials of complex interventions. Stat Methods Med Res. 2010;19:237–70.
Jenkinson M, Smith S. A global optimisation method for robust affine registration of brain images. Med Image Anal. 2001;5:143–56.
Douaud G, Smith S, Jenkinson M, Behrens T, Johansen-Berg H, Vickers J, et al. Anatomically related grey and white matter abnormalities in adolescent-onset schizophrenia. Brain. 2007;130:2375–86.
De Stefano N, Matthews P, Filippi M, Agosta F, De Luca M, Bartolozzi M, et al. Evidence of early cortical atrophy in MS Relevance to white matter changes and disability. Neurology. 2003;60:1157–62.
Zarahn E, Aguirre GK, D’Esposito M. Empirical analyses of BOLD fMRI statistics. Neuroimage. 1997;5:179–97.
Suckling J, Ohlssen D, Andrew C, Johnson G, Williams SC, Graves M, et al. Components of variance in a multicentre functional MRI study and implications for calculation of statistical power. Hum Brain Mapp. 2008;29:1111–22.
Mori S, Wakana S, Van Zijl PC, Nagae-Poetscher L. MRI atlas of human white matter. 2005.
Rissman J, Gazzaley A, D’Esposito M. Measuring functional connectivity during distinct stages of a cognitive task. Neuroimage. 2004;23:752–63.
Winkler AM, Ridgway GR, Webster MA, Smith SM, Nichols TE. Permutation inference for the general linear model. Neuroimage. 2014;92:381–97.
Acknowledgements
The project is funded by the Efficacy and Mechanisms Evaluation (EME) Programme, an MRC and NIHR partnership (–grant number 09/100/23). EMJ is supported by the National Institute for Health Research University College London Hospitals Biomedical Research Centre. Minocycline and placebo are manufactured, controlled and distributed to the Trusts’ pharmacies by Catalent, UK. The authors would like to thank Dr Roger J Tait of the Behavioural and Clinical Neuroscience Institute (University of Cambridge) for his advice and insight on MRI analysis.
Disclaimer
The views expressed in this publication are those of the authors and not necessarily those of the MRC, NHS, NIHR or the Department of Health.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
In the last three years, TREB has received honoraria for speaking at educational meetings and been a member of a scientific advisory board for Sunovion and Otsuka/Lundbeck. PBJ has been a member of scientific advisory boards for Roche and Otsuka. SML has received personal fees from Jansen, Roche and Sunovion, and research grants from Abbvie, Roche and Pfizer. None of this funding was used to finance the present study or to cover the article processing charge. All the other authors declare no competing interest.
Authors’ contributions
DML designed compatible MRI experiments for all research centres involved in the study, trained all RAs in MRI procedures, designed MRI analysis and wrote the article. JS participated in designing of the study, supervised recruitment of participants and execution of the study at the University of Cambridge, supervised designing of the MRI experiment and critically revised the manuscript. TREB participated in designing of the study and critically revised the manuscript. IBC participated in designing of the study, supervised recruitment of participants and execution of the study at the Lancashire Early Intervention Services. PD participated in designing of the study, supervised recruitment of participants and execution of the study at the King’s College London. NH participated in designing of the study, supervised recruitment of participants and execution of the study at the Lancashire Early Intervention Services. PBJ provided advice on describing inflammation hypothesis in the article, participated in designing of the study and recruitment of participants at the University of Cambridge. EJ participated in designing of the study, designed the sessions measuring cognitive function of the participants, supervised recruitment of participants and execution of the study at the University College London and critically revised the manuscript. SML participated in designing of the study, supervised recruitment of participants and execution of the study at the University of Edinburgh. RU critically revised the manuscript, supervised recruitment of participants and execution of the study at the University of Birmingham. BD conceived the study, participated in designing it, supervised the teams in all the research centres, supervised recruitment of participants and execution of the study at the University of Manchester and critically revised the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Lisiecka, D.M., Suckling, J., Barnes, T.R. et al. The benefit of minocycline on negative symptoms in early-phase psychosis in addition to standard care - extent and mechanism (BeneMin): study protocol for a randomised controlled trial. Trials 16, 71 (2015). https://doi.org/10.1186/s13063-015-0580-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-015-0580-x