
Abstract
Background
Metabolic homeostasis is substantially disrupted in critical illness. Given the pleiotropic effects of vitamin D, we hypothesized that metabolic profiles differ between critically ill patients relative to their vitamin D status.
Methods
We performed a metabolomics study on biorepository samples collected from a single academic medical center on 65 adults with systemic inflammatory response syndrome or sepsis treated in a 20-bed medical ICU between 2008 and 2010. To identify key metabolites and metabolic pathways related to vitamin D status in critical illness, we first generated metabolomic data using gas and liquid chromatography mass spectroscopy. We followed this by partial least squares-discriminant analysis to identify individual metabolites that were significant. We then interrogated the entire metabolomics profile using metabolite set enrichment analysis to identify groups of metabolites and pathways that were differentiates of vitamin D status. Finally we performed logistic regression to construct a network model of chemical-protein target interactions important in vitamin D status.
Results
Metabolomic profiles significantly differed in critically ill patients with 25(OH)D ≤ 15 ng/ml relative to those with levels >15 ng/ml. In particular, increased 1,5-anhydroglucitol, tryptophan betaine, and 3-hydroxyoctanoate as well as decreased 2-arachidonoyl-glycerophosphocholine and N-6-trimethyllysine were strong predictors of 25(OH)D >15 ng/ml. The combination of these five metabolites led to an area under the curve for discrimination for 25(OH)D > 15 ng/ml of 0.82 (95% CI 0.71–0.93). The metabolite pathways related to glutathione metabolism and glutamate metabolism are significantly enriched with regard to vitamin D status.
Conclusion
Vitamin D status is associated with differential metabolic profiles during critical illness. Glutathione and glutamate pathway metabolism, which play principal roles in redox regulation and immunomodulation, respectively, were significantly altered with vitamin D status.
Similar content being viewed by others


Background
Low vitamin D status is common in the intensive care unit (ICU) [1,2,3]. Several observational studies in critically ill cohorts suggest that vitamin D status is associated with important clinical outcomes [1,2,3]. In particular, low vitamin D status is associated with increased risk of sepsis and with worse outcomes in patients with sepsis [4, 5]. Moreover, recent studies support vitamin D as a potential therapeutic agent in hospitalized patients [6, 7].
Vitamin D has broad biological effects on nuclear transcription, cell cycle regulation, differentiation, and apoptosis [8]. Vitamin D metabolic enzymes and vitamin D receptors have a wide tissue distribution, reflecting the involvement of vitamin D in the metabolism and function of many cell types [9]. Indeed, differential metabolic profiles are demonstrated in ambulatory patients who respond to vitamin D supplementation relative to those who do not [10, 11]. Since metabolic homeostasis is often disrupted in critical illness, substantial alterations of several intrinsic pathways can be expected in septic patients [12]. Only a limited number of metabolomic studies have been published to date in experimental sepsis models [13], pediatric sepsis [14], and critically ill adults [15].
While some existing data support anti-inflammatory and immune modulating effects related to vitamin D supplementation [16], and while metabolomic approaches are used to understand the pleiotropic effects of Vitamin D [17, 18], there is limited understanding of the metabolic alterations associated with low vitamin D status in critical illness. Therefore, we analyzed metabolite profiles with regard to vitamin D status in a prospective study of adult patients with systemic inflammatory response syndrome (SIRS) and sepsis [19]. We hypothesized that the metabolomic profile of patients with severe critical illness near the time of ICU admission is influenced by vitamin D status and that this metabolic difference in turn can illuminate important biologic pathways that may contribute to pathogenesis and prognosis.
Methods
Study design and patients
The Registry of Critical Illness (RoCI) is a registry of adult medical ICU patients based at the Brigham and Women’s Hospital (Boston, MA, USA), created to record patient data and store samples for plasma, RNA/DNA analysis, and protein isolation. The protocol for patient recruitment has been previously described at length [19]. Between September 2008 and May 2010, 90 medical ICU patients had metabolic profiling: 29 of these patients satisfied SIRS criteria, 30 satisfied criteria for sepsis, and 31 satisfied criteria for sepsis and acute respiratory distress syndrome (ARDS) [20]. Patients were not selected with regard to risk of death or any known metabolic feature. We conducted a sub-analysis involving 65 RoCI patients who had been selected for metabolic profiling, and in whom plasma was available for measuring 25(OH)D levels (Additional file 1, Fig. 1).

Flow chart of the cohort. ARDS acute respiratory distress syndrome, SIRS systemic inflammatory response syndrome, RoCI Registry of Critical Illness
Demographic and physiologic data were collected from the clinical record as described previously [19]. In addition to data collected by the RoCI, additional data on all patients were compiled through a well-described computerized registry, called the Research Patient Data Registry (RPDR) [21] as outlined in Additional file 1.
Plasma 25(OH)D level was measured using plasma samples from the same day as the plasma sample that was used for metabolic profiling. All 25(OH)D levels were measured via the competitive chemiluminescence immunoassay (CLIA) using the DiaSorin LIAISON 25-OH Vitamin D Total assay [22, 23]. Serum 25(OH)D levels were dichotomized a priori into low (≤15 ng/ml) and normal (>15 ng/ml) groups based on large studies performed by our group in the ICU under study, which consistently found differential outcomes at this cut point [2,3,4, 24].
Metabolomic profiling identified 411 metabolites for the complete RoCI cohort (N = 90 plasma samples within 72 hours of ICU admission) using Metabolon, Inc. [20]. Gas and liquid chromatography mass spectroscopy (GC-MS, LC-MS) were performed as described previously [25, 26]. We removed metabolites with the lowest IQR of variability in the RoCI data, leaving 308 metabolites. All metabolite concentrations were log2 transformed to normalize the data, which were utilized for all of the models and all of the metabolite data analyses. Details on metabolomic sample processing have been previously described at length [20].
We utilized MetaboAnalyst 3.0 software (www.metaboanalyst.ca) to identify key metabolism alterations related to vitamin D status [27]. We identified the group of metabolites that best discriminate between individuals with low and normal vitamin D status using partial least squares-discriminant analysis (PLS-DA) (Fig. 2) and identified the metabolites responsible for the overall discrimination ability (Fig. 3). PLS-DA model validation was determined by permutation tests based on separation distance. In each permutation, a PLS-DA model was built between the data and the permuted class labels using the optimal number of components determined by cross-validation for the model based on the original class assignment [28]. Metabolite set enrichment analysis [29] was then performed by mapping the metabolite data on the Human Metabolome Database (HMDB) [30]. Significantly enriched metabolites were identified using the global test [31] and the “betweenness centrality” measure to estimate metabolite importance followed by an assessment of pathway importance of each identified metabolite [32]. P values were adjusted for multiple testing using the Holm-Bonferroni method [33].

Partial least squares-discriminant analysis (PLS-DA). Cross-validated PLS-DA score plot for comparison of the global metabolite profiles of 24 patients with 25(OH)D ≤ 5 ng/ml (red) and 41 patients with 25(OH)D >15 ng/ml (green) shows the separation achieved according to vitamin D status. The p value based on permutation is 0.033 (66/2000). Colored circles represent 95% confidence intervals. Colored dots represent individual samples: 4.5% and 5.3% are the scores of component 1 and component 2, respectively, in the PLS-DA analysis

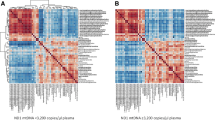
Vitamin D deficiency biomarker identification by global metabolomics. To relate vitamin D status to the blood metabolite data, we used random forest (RF) predictors. An RF importance measure was used to rank metabolites according to their prognostic importance for vitamin D status. The colored boxes on the right indicate the relative concentrations of the corresponding metabolite in the vitamin D groups. Metabolite classes (amino acid metabolic, carbohydrate metabolism, lipid metabolism) are indicated by the colored circles
Similar to our previous work, single metabolite associations were evaluated using multivariable logistic regression models [20]. Specifically, for each metabolite we performed logistic regression with 25(OH)D >15 ng/ml as the outcome, after adjustment for age, gender, race, malignancy status, sepsis, and renal function (as estimated by glomerular filtration rate-modification of diet in renal disease (GFR-MDRD)). Additionally, for each metabolite we performed logistic regression with 28-day mortality as the outcome, after adjustment for Acute Physiology and Chronic Health Evaluation II (APACHE II) scores. Analyses were performed using STATA 14.1MP (College Station, TX, USA). A network of protein-protein and metabolite-protein interactions was then generated using the Search Tool for Interactions of Chemicals (STITCH) database, version 4.0 [34, 35]. STITCH active prediction methods are based on neighborhood, gene fusion, co-occurrence, co-expression, experiments, databases, text mining, and predictions, with a required confidence threshold (score) of 0.40 [34, 35].
Results
Table 1 shows the demographic characteristics of the study cohort. Most patients were male (58%) and white (83%). The mean (SD) age at ICU admission was 55 (15) years. The mean (SD) 25(OH)D concentration was 20 (16) ng/ml, and 63% of cohort patients were diagnosed with sepsis. The mean APACHE II score was 26 (10). The 28-day mortality within the cohort was 35%. There were no significant differences between patients with 25(OH)D ≤ 15 ng/ml relative to those 25(OH)D > 15 ng/ml regarding any key baseline characteristic or for 28-day mortality.
Primary outcome
Metabolomic profiles differed in critically ill patients with 25(OH)D ≤ 15 ng/ml relative to those with levels >15 ng/ml. The supervised PLS-DA showed that the two different groups were well-clustered, with specific metabolic profiles for each (Fig. 2). Group membership (25(OH)D ≤ 15 ng/ml vs. >15 ng/ml) is illustrated by the 95% confidence ellipses calculated from PLS-DA scores. The permutation test with a p value of 0.033 indicates that the classification of global metabolite profiles by 25(OH)D is significantly different.
We utilized the random forest (RF) learning algorithm to select relevant variables for vitamin D status classification by estimating the importance of each metabolite to vitamin D status. In the RF analysis the “mean decrease accuracy” indicates how much a certain metabolite contributes to separation of the 25(OH)D groups, and the overall “predictive accuracy” is indicative of the accuracy for a set of metabolites to discriminate vitamin D status [32]. RF analysis of blood-targeted metabolomics data defined a set of 15 metabolites that constitute the best predictors of vitamin D status (Fig. 3). In particular, increased 1,5-anhydroglucitol, tryptophan betaine and 3-hydroxyoctanoate and decreased 2-arachidonoylglycerophosphocholine and N-6-trimethyllysine were strong predictors of 25(OH)D >15 ng/mL. These metabolites are products of carbohydrate, amino acid, lipid, lipid and amino acid metabolism, respectively. We found that in logistic regression, the combination of these 5 metabolites produced an area under the curve (AUC) for discrimination for 25(OH)D > 15 ng/ml of 0.82 (95% CI 0.71–0.93).
We next sought to identify differential biologically meaningful metabolite pathways in the cohort with regard to vitamin D status. Metabolite set enrichment analysis identified metabolites that were significantly enriched in patients with 25(OH)D > 15 ng/ml, with the strongest enrichment identified for glutathione metabolism (p = 0.020) and glutamate metabolism (p = 0.039). The metabolite sets related to glutathione metabolism (inclusive of cysteinylglycine, pyroglutamine, and L-cysteine) and glutamate metabolism (inclusive of glutamate and α-ketoglutarate) were enriched with regard to vitamin D status more than expected by chance (Additional files 2 and 3).
Twenty metabolites were associated with vitamin D status at a nominal significance level (p < 0.05) in the RoCI cohort, after adjusting for age, race, malignancy status, sepsis, and renal function (Table 2). Seven of these metabolites were associated with vitamin D status and 28-day mortality: (1) glucuronate; (2) 1-palmitoyl-glycerophosphoinositol; (3) bilirubin (E,E) isomer; (4) pyroglutamine; (5) 2-hydroxybutyrate; (6) biliverdin; and (7) tryptophan (Table 2, Additional file 4). Network modeling of chemical-protein interactions was then utilized to illustrate the importance of the relationship between 25(OH)D and the metabolism of bilirubin, fatty acid derivatives, and bile acids through glucuronidation (Fig. 4).

Network of metabolite-protein interactions inferred by metabolomics analysis. The names of the seven metabolites associated with vitamin D status and 28-day mortality (listed in Table 2), in addition to “vitamin D”, were used as input to generate a network of protein-protein and metabolite-protein interactions using the Search Tool for Interactions of Chemicals (STITCH) database. Network nodes are represented as either cylinders (chemicals) or circles (proteins, i.e. predicted functional partners), where nodes are colored if they are directly linked to the input, or white if they are of a higher iteration/depth (i.e. inferred by the network). Lines between nodes (edges) indicate predicted functional links, where stronger associations are represented by thicker lines; protein-protein interactions are shown in blue, chemical-protein interactions are shown in green, and interactions between chemicals are shown in red. Links between chemicals are not used to extend the network
Discussion
In the present study, our goal was to investigate whether vitamin D status in the early course of severe critical illness was associated with differences in the metabolic profiles of critically ill patients. Utilizing several analytic strategies, we demonstrated that the metabolic profile of critically ill patients differs based on their vitamin D status and there is evidence that metabolites related to vitamin D status are most prominently related to glutathione and glutamate metabolism and glucuronidation.
In humans, 25(OH)D is the major circulating form of vitamin D3. Steady-state plasma 25(OH)D concentrations represent a balance between formation and clearance activities, which are mediated by phase I and phase II oxidation and conjugation processes. Variation in the efficiency of these detoxification reactions contributes to variability in circulating plasma concentrations of 25(OH)D, thereby altering the activity of this prohormone. Based on the results of this metabolomic profiling study, we have identified two important phase II metabolism pathways for glutamate, glucuronidation and glutathione cycling that are associated with vitamin D homeostasis in critically ill ICU patients.
By MSEA, we identified the overlapping pathways for glutathione and glutamate metabolism as the most highly enriched pathways in our metabolite data. Pyroglutamine, a cyclic metabolite of glutamine and component of the glutathione cycle, was identified in PLS-DA analysis as a classifier of vitamin D status (Fig. 3). Glutathione, a major cellular thiol antioxidant, is a cofactor of the enzymatic detoxification of oxygen radicals [36, 37]. In vitro data suggest that vitamin D upregulates cellular glutathione [36]. Furthermore, in community-dwelling adults, serum 25(OH)D levels are associated with increased circulating glutathione [38]. Though the redox state of reduced/oxidized glutathione (GSH/GSSG) is closely regulated, it decreases with tissue injury, inflammation, sepsis, and toxin exposure [39,40,41]. Oxidative stress is well-described in patients with sepsis, with supporting evidence for production of reactive oxygen species (ROS) and associated damage [42]. In patients with sepsis, inflammatory response initiation via oxidative stress occurs through redox pathway activation of nuclear factor κB (NFκB) and expression of a substantial number of genes involved in the immune response and cell survival [43, 44].
Glutamate, a highly concentrated intracellular amino acid is important for biosynthesis of multiple amino acids, nucleic acids, nucleotides and metabolites [45]. Though glutamate has a low concentration in plasma [46] it has an important role in peripheral organs and tissues as an extracellular signal mediator [47]. More germane to the severely ill cohort under study, ionotropic glutamate receptors are expressed on T cells and B cells. Dendritic cells and macrophages and glutamate serve as an immunomodulator in the initiation and development of T-cell-mediated immunity in peripheral tissues [48, 49]: α-ketoglutarate, a Krebs cycle intermediate, is produced in a glutamine-dependent fashion and regulates the T helper 1 cell and regulatory T cell generation balance [50].
Glucuronidation is crucial for the hepatic and renal metabolism of compounds, including bile acids, steroids, bilirubin, and fatty acids, to facilitate their elimination from the body and to improve the disposition and activity of drugs and hormones across tissues. Glucuronidation is an essential chemical reaction for rendering 1, 25(OH)2D3 (the most metabolically active vitamin D metabolite) to a water-soluble, biologically inactive form, but may also serve as a reservoir for enterohepatic circulation [51]. This conjugation reaction is performed by UDP glucuronosyltransferase (UGT) enzymes in the liver. In addition to glucuronate, we also identified bilirubin and biliverdin as important metabolite predictors of vitamin D status. Bilirubin, a metabolite of the heme end product biliverdin, is glucuronidated by UGT1A isoforms, chiefly UGT1A1, in addition to UGT1A4.
While UGTs catalyze the conjugation of a wide variety of endogenous substrates, recent studies have identified UGT1A4 as the primary catalyst of 25(OH)D glucuronidation in vivo [52]. Failure to recycle glucuronides could contribute to low vitamin D status through promoting the metabolism of 25(OH)D to its inactive, polar forms, which are more readily excreted, thereby reducing its levels in the systemic circulation. In addition, as UGT enzymes are highly polymorphic, and “gain-of-function” variants with high substrate clearance activity have been described in humans [52, 53], inter-individual variation in 25(OH)D levels due to variable UGT1A4 activity could contribute to lower 25(OH)D levels in circulation. Because homozygous carriers of UGT1A4*3 demonstrate enhanced 25(OH)D glucuronidation activity, patients with this genotype might be expected to have lower circulating levels of 25(OH)D and may therefore be at greater risk of low vitamin D status [52, 53]. In addition to UGT1A4, UGT1A1 was also predicted by network modeling of chemical-protein interactions for all seven metabolites, in addition to vitamin D metabolites, to co-interact with 1,25(OH)2D3, bilirubin, and glucuronic acid (Fig. 4). A specific role for UGT1A1 in glucuronidation of vitamin D has not been investigated but may contribute to vitamin D status in critically ill patients.
Two additional metabolites, 1-palmitoyl-glycerophosphoinositol and 2-hydroxybutyrate, were also associated with 25(OH)D plasma levels (Table 2). While little is known about the specific roles of 1-palmitoyl-glycerophosphoinositol in vitamin D metabolism, this compound belongs to the glycerophosphoinositol family and, along with pyroglutamine and 2-hydroxyisobutyrate (a derivative of 2-hydroxybutyrate), was associated with anti-hypertensive and lipid-lowering drugs in serum samples from a study of 1762 participants in the Cooperative Health Research in the Region of Augsburg (KORA) study [54].
The present study is not without potential limitations. Metabolites were measured early in the ICU course of severe critical illness, from a relatively small number of patients, at a single time point, and from a single biofluid (plasma). As the timing of plasma collection was within 72 hours of ICU admission and not at a uniform time point, the potential for variability and switches in metabolic pathways during the course of critical illness cannot be excluded. Our observational study included patients who were critically ill for various reasons, creating a heterogeneous study sample with high severity of illness. Further, selection bias may be present as we are analyzing only a subset of patients in the RoCI cohort. Without a control population of healthy vitamin-D-sufficient individuals, we do not have comparative metabolomic information on vitamin D status in the critically ill relative to the control. We are unable to account for the impact of race on metabolic profiles as our cohort was mostly white. Though we do have information on nutrition status, we do not have information related to nutrition intake, body mass index (BMI) or alcohol intake at the time metabolomic profiles were obtained. As our study was performed on a convenience sample, our results may not be generalizable to all critical care patients. Our bioinformatics approaches, while robust, are not without risk of introducing sources of bias. Although PLS-DA is well-suited for metabolomic data with much larger numbers of predictors than observations and multi-collinearity [55], it may be subject to over-fitting; to limit this, we performed cross-validation and permutation testing [56, 57]. Our measurement of 25(OH)D in a critically ill population with a mean estimated GFR of 59.6 ml/minute may not accurately account for the biologically active form of vitamin D. Our data do not allow for the distinction between metabolites that may be on a causal pathway or simply confounders of the association between vitamin D and outcome. Further, though aging is noted to be an important factor in metabolic homeostasis [25, 58] our study age range cannot account for such alterations. Finally, we cannot fully account for potential confounding, reverse causation, and the lack of a randomly-distributed exposure [59].
Conclusion
In summary, vitamin D status is associated with differential metabolic profiles in early severe critical illness. Glutathione and glutamate metabolism, which play principal roles in redox regulation and immunomodulation, respectively, were significantly altered with vitamin D status.
Abbreviations
- APACHE II:
-
Acute Physiology and Chronic Health Evaluation II
- ARDS:
-
Acute respiratory distress syndrome
- AUC:
-
Area under the curve
- GFR:
-
Glomerular filtration rate
- ICU:
-
Intensive care unit
- IL:
-
Interleukin
- PLS-DA:
-
Partial least squares-discriminant analysis
- RF:
-
Random forest
- RoCI:
-
Registry of Critical Illness
- SIRS:
-
Systemic inflammatory response syndrome
- STITCH:
-
Search Tool for Interactions of Chemicals
- UGT:
-
Glucuronosyltransferase
References
Lee P, Eisman JA, Center JR. Vitamin D deficiency in critically ill patients. N Engl J Med. 2009;360(18):1912–4.
Braun AB, Gibbons FK, Litonjua AA, Giovannucci E, Christopher KB. Low serum 25-hydroxyvitamin D at critical care initiation is associated with increased mortality*. Crit Care Med. 2012;40(1):63–72.
Braun A, Chang D, Mahadevappa K, Gibbons FK, Liu Y, Giovannucci E, Christopher KB. Association of low serum 25-hydroxyvitamin D levels and mortality in the critically ill*. Crit Care Med. 2011;39(4):671–7.
Moromizato T, Litonjua AA, Braun AB, Gibbons FK, Giovannucci E, Christopher KB. Association of low serum 25-hydroxyvitamin D levels and sepsis in the critically ill. Crit Care Med. 2014;42(1):97–107.
de Haan K, Groeneveld AB, de Geus HR, Egal M, Struijs A. Vitamin D deficiency as a risk factor for infection, sepsis and mortality in the critically ill: systematic review and meta-analysis. Crit Care. 2014;18(6):660.
Amrein K, Litonjua AA, Moromizato T, Quraishi SA, Gibbons FK, Pieber TR, Camargo Jr CA, Giovannucci E, Christopher KB. Increases in pre-hospitalization serum 25(OH)D concentrations are associated with improved 30-day mortality after hospital admission: a cohort study. Clin Nutr. 2016;35(2):514–21.
Amrein K, Schnedl C, Holl A, Riedl R, Christopher KB, Pachler C, Urbanic Purkart T, Waltensdorfer A, Munch A, Warnkross H, et al. Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vitamin D deficiency: the VITdAL-ICU randomized clinical trial. JAMA. 2014;312(15):1520–30.
Ingraham BA, Bragdon B, Nohe A. Molecular basis of the potential of vitamin D to prevent cancer. Curr Med Res Opin. 2008;24(1):139–49.
Christopher KB. Vitamin D, supplementation in the ICU patient. Curr Opin Clin Nutr Metab Care. 2015;18(2):187–92.
O’Sullivan A, Gibney MJ, Connor AO, Mion B, Kaluskar S, Cashman KD, Flynn A, Shanahan F, Brennan L. Biochemical and metabolomic phenotyping in the identification of a vitamin D responsive metabotype for markers of the metabolic syndrome. Mol Nutr Food Res. 2011;55(5):679–90.
Elnenaei MO, Chandra R, Mangion T, Moniz C. Genomic and metabolomic patterns segregate with responses to calcium and vitamin D supplementation. Br J Nutr. 2011;105(1):71–9.
Kiehntopf M, Nin N, Bauer M. Metabolism, metabolome, and metabolomics in intensive care: is it time to move beyond monitoring of glucose and lactate? Am J Respir Crit Care Med. 2013;187(9):906–7.
Izquierdo-Garcia JL, Nin N, Ruiz-Cabello J, Rojas Y, de Paula M, Lopez-Cuenca S, Morales L, Martinez-Caro L, Fernandez-Segoviano P, Esteban A, et al. A metabolomic approach for diagnosis of experimental sepsis. Intensive Care Med. 2011;37(12):2023–32.
Mickiewicz B, Vogel HJ, Wong HR, Winston BW. Metabolomics as a novel approach for early diagnosis of pediatric septic shock and its mortality. Am J Respir Crit Care Med. 2013;187(9):967–76.
Antcliffe D, Gordon AC. Metabonomics and intensive care. Crit Care. 2016;20:68.
Christopher KB. Vitamin D, and critical illness outcomes. Curr Opin Crit Care. 2016;22(4):332–8.
Finkelstein JL, Pressman EK, Cooper EM, Kent TR, Bar HY, O’Brien KO. Vitamin D status affects serum metabolomic profiles in pregnant adolescents. Reprod Sci. 2015;22(6):685–95.
Nelson SM, Panagiotou OA, Anic GM, Mondul AM, Mannisto S, Weinstein SJ, Albanes D. Metabolomics analysis of serum 25-hydroxy-vitamin D in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention (ATBC) Study. Int J Epidemiol. 2016;45(5):1458–68.
Dolinay T, Kim YS, Howrylak J, Hunninghake GM, An CH, Fredenburgh L, Massaro AF, Rogers A, Gazourian L, Nakahira K, et al. Inflammasome-regulated cytokines are critical mediators of acute lung injury. Am J Respir Crit Care Med. 2012;185(11):1225–34.
Rogers AJ, McGeachie M, Baron RM, Gazourian L, Haspel JA, Nakahira K, Fredenburgh LE, Hunninghake GM, Raby BA, Matthay MA, et al. Metabolomic derangements are associated with mortality in critically ill adult patients. PLoS One. 2014;9(1):e87538.
Murphy SN, Chueh HC. A security architecture for query tools used to access large biomedical databases. Proc AMIA Symp. 2002:552 − 56
Ersfeld DL, Rao DS, Body JJ, Sackrison Jr JL, Miller AB, Parikh N, Eskridge TL, Polinske A, Olson GT, MacFarlane GD. Analytical and clinical validation of the 25 OH vitamin D assay for the LIAISON automated analyzer. Clin Biochem. 2004;37(10):867–74.
Wagner D, Hanwell HE, Vieth R. An evaluation of automated methods for measurement of serum 25-hydroxyvitamin D. Clin Biochem. 2009;42(15):1549–56.
Braun AB, Litonjua AA, Moromizato T, Gibbons FK, Giovannucci E, Christopher KB. Association of low serum 25-hydroxyvitamin D levels and acute kidney injury in the critically ill*. Crit Care Med. 2012;40(12):3170–9.
Lawton KA, Berger A, Mitchell M, Milgram KE, Evans AM, Guo L, Hanson RW, Kalhan SC, Ryals JA, Milburn MV. Analysis of the adult human plasma metabolome. Pharmacogenomics. 2008;9(4):383–97.
Sreekumar A, Poisson LM, Rajendiran TM, Khan AP, Cao Q, Yu J, Laxman B, Mehra R, Lonigro RJ, Li Y, et al. Metabolomic profiles delineate potential role for sarcosine in prostate cancer progression. Nature. 2009;457(7231):910–4.
Xia J, Sinelnikov IV, Han B, Wishart DS. MetaboAnalyst 3.0–making metabolomics more meaningful. Nucleic Acids Res. 2015;43(W1):W251–257.
Westerhuis JA, Hoefsloot HCJ, Smit S, Vis DJ, Smilde AK, van Velzen EJJ, van Duijnhoven JPM, van Dorsten FA. Assessment of PLSDA cross validation. Metabolomics. 2008;4(1):81–9.
Xia J, Wishart DS. MSEA: a web-based tool to identify biologically meaningful patterns in quantitative metabolomic data. Nucleic Acids Res. 2010;38(Web Server issue):W71–77.
Wishart DS, Jewison T, Guo AC, Wilson M, Knox C, Liu Y, Djoumbou Y, Mandal R, Aziat F, Dong E, et al. HMDB 3.0–The Human Metabolome Database in 2013. Nucleic Acids Res. 2013;41(Database issue):D801–7.
Goeman JJ, van de Geer SA, de Kort F, van Houwelingen HC. A global test for groups of genes: testing association with a clinical outcome. Bioinformatics. 2004;20(1):93–9.
Houtkooper RH, Argmann C, Houten SM, Canto C, Jeninga EH, Andreux PA, Thomas C, Doenlen R, Schoonjans K, Auwerx J. The metabolic footprint of aging in mice. Sci Rep. 2011;1:134.
Holm S. A simple sequentially rejective multiple test procedure. Scand J Stat. 1979;6:65–70.
Kuhn M, Szklarczyk D, Pletscher-Frankild S, Blicher TH, von Mering C, Jensen LJ, Bork P. STITCH 4: integration of protein-chemical interactions with user data. Nucleic Acids Res. 2014;42(Database issue):D401–7.
Szklarczyk D, Franceschini A, Wyder S, Forslund K, Heller D, Huerta-Cepas J, Simonovic M, Roth A, Santos A, Tsafou KP, et al. STRING v10: protein-protein interaction networks, integrated over the tree of life. Nucleic Acids Res. 2015;43(Database issue):D447–52.
Jain SK, Micinski D. Vitamin D upregulates glutamate cysteine ligase and glutathione reductase, and GSH formation, and decreases ROS and MCP-1 and IL-8 secretion in high-glucose exposed U937 monocytes. Biochem Biophys Res Commun. 2013;437(1):7–11.
Biolo G, Antonione R, De Cicco M. Glutathione metabolism in sepsis. Crit Care Med. 2007;35(9 Suppl):S591–95.
Alvarez JA, Chowdhury R, Jones DP, Martin GS, Brigham KL, Binongo JN, Ziegler TR, Tangpricha V. Vitamin D status is independently associated with plasma glutathione and cysteine thiol/disulphide redox status in adults. Clin Endocrinol (Oxf). 2014;81(3):458–66.
Jones DP. Redefining oxidative stress. Antioxid Redox Signal. 2006;8(9-10):1865–79.
Pacht ER, Timerman AP, Lykens MG, Merola AJ. Deficiency of alveolar fluid glutathione in patients with sepsis and the adult respiratory distress syndrome. Chest. 1991;100(5):1397–403.
Iyer SS, Jones DP, Brigham KL, Rojas M. Oxidation of plasma cysteine/cystine redox state in endotoxin-induced lung injury. Am J Respir Cell Mol Biol. 2009;40(1):90–8.
Chuang CC, Shiesh SC, Chi CH, Tu YF, Hor LI, Shieh CC, Chen MF. Serum total antioxidant capacity reflects severity of illness in patients with severe sepsis. Crit Care. 2006;10(1):R36.
Arnalich F, Garcia-Palomero E, Lopez J, Jimenez M, Madero R, Renart J, Vazquez JJ, Montiel C. Predictive value of nuclear factor kappaB activity and plasma cytokine levels in patients with sepsis. Infect Immun. 2000;68(4):1942–5.
Paterson RL, Galley HF, Dhillon JK, Webster NR. Increased nuclear factor kappa B activation in critically ill patients who die. Crit Care Med. 2000;28(4):1047–51.
Yelamanchi SD, Jayaram S, Thomas JK, Gundimeda S, Khan AA, Singhal A, Keshava Prasad TS, Pandey A, Somani BL, Gowda H. A pathway map of glutamate metabolism. J Cell Commun Signal. 2016;10(1):69–75.
Darmaun D, Matthews DE, Bier DM. Glutamine and glutamate kinetics in humans. Am J Physiol. 1986;251(1 Pt 1):E117–26.
Hinoi E, Takarada T, Ueshima T, Tsuchihashi Y, Yoneda Y. Glutamate signaling in peripheral tissues. Eur J Biochem. 2004;271(1):1–13.
Ganor Y, Levite M. Glutamate in the immune system: glutamate receptors in immune cells, potent effects, endogenous production and involvement in disease. In: Levite M, editor. Nerve-driven immunity: neurotransmitters and neuropeptides in the immune system. Vienna: Springer; 2012. p. 121–61.
Pacheco R, Gallart T, Lluis C, Franco R. Role of glutamate on T-cell mediated immunity. J Neuroimmunol. 2007;185(1-2):9–19.
Klysz D, Tai X, Robert PA, Craveiro M, Cretenet G, Oburoglu L, Mongellaz C, Floess S, Fritz V, Matias MI, et al. Glutamine-dependent alpha-ketoglutarate production regulates the balance between T helper 1 cell and regulatory T cell generation. Sci Signal. 2015;8(396):ra97.
Hashizume T, Xu Y, Mohutsky MA, Alberts J, Hadden C, Kalhorn TF, Isoherranen N, Shuhart MC, Thummel KE. Identification of human UDP-glucuronosyltransferases catalyzing hepatic 1alpha,25-dihydroxyvitamin D3 conjugation. Biochem Pharmacol. 2008;75(5):1240–50.
Wang Z, Wong T, Hashizume T, Dickmann LZ, Scian M, Koszewski NJ, Goff JP, Horst RL, Chaudhry AS, Schuetz EG, et al. Human UGT1A4 and UGT1A3 conjugate 25-hydroxyvitamin D3: metabolite structure, kinetics, inducibility, and interindividual variability. Endocrinology. 2014;155(6):2052–63.
Henderson A, Lawson AS. Frequency distribution and 95% range of a variety of commonly measured blood constituents in healthy Nepalese donors. J Trop Med Hyg. 1985;88(1):21–4.
Altmaier E, Fobo G, Heier M, Thorand B, Meisinger C, Romisch-Margl W, Waldenberger M, Gieger C, Illig T, Adamski J, et al. Metabolomics approach reveals effects of antihypertensives and lipid-lowering drugs on the human metabolism. Eur J Epidemiol. 2014;29(5):325–36.
Perez-Enciso M, Tenenhaus M. Prediction of clinical outcome with microarray data: a partial least squares discriminant analysis (PLS-DA) approach. Hum Genet. 2003;112(5-6):581–92.
Xia J, Wishart DS. Web-based inference of biological patterns, functions and pathways from metabolomic data using MetaboAnalyst. Nat Protoc. 2011;6(6):743–60.
Bijlsma S, Bobeldijk I, Verheij ER, Ramaker R, Kochhar S, Macdonald IA, van Ommen B, Smilde AK. Large-scale human metabolomics studies: a strategy for data (pre-) processing and validation. Anal Chem. 2006;78(2):567–74.
Chaleckis R, Murakami I, Takada J, Kondoh H, Yanagida M. Individual variability in human blood metabolites identifies age-related differences. Proc Natl Acad Sci U S A. 2016;113(16):4252–9.
Ho PM, Peterson PN, Masoudi FA. Evaluating the evidence: is there a rigid hierarchy? Circulation. 2008;118(16):1675–84.
Acknowledgements
This manuscript is dedicated to the memory of our dear friend and colleague Nathan Edward Hellman, MD, PhD. The authors thank Shawn Murphy and Henry Chueh and the Partners Health Care Research Patient Data Registry group for facilitating use of their database.
Funding
Dr. Rogers is supported by a grant from the Parker B. Francis foundation (http://www.francisfellowships.org/); Dr. McGeachie is supported by K12 HL089990; Dr. Gazourian is supported by T32 HL7118 and T32 HL007680; Dr. Fredenburgh is supported by K08 GM083207; Dr. Baron is supported by R01 HL091957, R01 HL112747, and P01 108801; Dr. Choi is supported by P01 HL108801, R01 HL079904, and R01 HL112747; Dr. Lasky-Su is supported by R01 HL123915; and Kenneth Christopher is supported by the A.S.P.E.N. Rhoads Research Foundation and R01 GM115774.
Availability of data and materials
The dataset supporting the conclusions of this article is not available.
Author information
Authors and Affiliations
Contributions
JL-S participated in the design of the study, helped to draft the manuscript, and helped to revise the manuscript; AD participated in the design of the study, ran the model, analyzed output data, and helped to draft the manuscript; AAL participated in the design of the study and helped to draft the manuscript; AJR assembled input data and participated in the design of the study, and helped to draft the manuscript; MJMcG assembled input data and participated in the design of the study, and helped to revise the manuscript; RMB recruited cohort patients, assembled input data and helped to draft the manuscript; LG recruited cohort patients, assembled input data and helped to draft the manuscript; DB-B assembled input data and helped to draft the manuscript; LEF recruited cohort patients, assembled input data, and helped to draft the manuscript; AMKC recruited cohort patients, assembled input data, and helped to draft the manuscript; KMM participated in the design of the study, assembled input data, and helped to draft the manuscript; SAQ participated in the design of the study and helped to draft the manuscript; KA participated in the design of the study and helped to draft the manuscript; KBC conceived of the study, participated in its design and coordination, assembled input data, wrote code, ran the model, analyzed output data, and drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Authors’ information
Not applicable.
Ethics approval and consent to participate
Approval for the study was granted by the Partners Human Research Committee Institutional Review Board, the ethics governing body for Brigham and Women’s Hospital. Written informed consent was obtained from all subjects or their legal surrogates.
Consent for publication
Not applicable.
Competing interests
None of the authors have any competing interests in the manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Supplemental methods. (DOC 100 kb)
Additional file 2: Figure S1.
Glutathione pathway metabolite member normalized concentrations from pathway analysis by global metabolomics in plasma from 24 patients with 25(OH)D ≤15 ng/ml (red) and 41 patients with 25(OH)D >15 ng/ml (green). (PPTX 53 kb)
Additional file 3: Figure S2.
Glutamate metabolism pathway metabolite member normalized concentrations from pathway analysis by global metabolomics in plasma from 24 patients with 25(OH)D ≤15 ng/ml (red) and 41 patients with 25(OH)D >15 ng/ml (green). (PPTX 46 kb)
Additional file 4: Table S1.
Mortality and 25(OH)D associated metabolites by logistic regression analysis. (DOC 35 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lasky-Su, J., Dahlin, A., Litonjua, A.A. et al. Metabolome alterations in severe critical illness and vitamin D status. Crit Care 21, 193 (2017). https://doi.org/10.1186/s13054-017-1794-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-017-1794-y