
Abstract
Background
Acute kidney injury (AKI) is a multifactorial syndrome, but knowledge about its pathophysiology and possible genetic background is limited. Recently the first hypothesis-free genetic association studies have been published to explore individual susceptibility to AKI. We aimed to replicate the previously identified associations between five candidate single nucleotide polymorphisms (SNP) in apoptosis-related genes BCL2, SERPINA4, SERPINA5, and SIK3 and the development of AKI, using a prospective cohort of critically ill patients with sepsis/septic shock, in Finland.
Methods
This is a prospective, observational multicenter study. Of 2567 patients without chronic kidney disease and with genetic samples included in the Finnish Acute Kidney Injury (FINNAKI) study, 837 patients had sepsis and 627 patients had septic shock. AKI was defined according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria, considering stages 2 and 3 affected (severe AKI), stage 0 unaffected, and stage 1 indecisive. Genotyping was done using iPLEXTM Assay (Agena Bioscience). The genotyped SNPs were rs8094315 and rs12457893 in the intron of the BCL2 gene, rs2093266 in the SERPINA4 gene, rs1955656 in the SERPINA5 gene and rs625145 in the SIK3 gene. Association analyses were performed using logistic regression with PLINK software.
Results
We found no significant associations between the SNPs and severe AKI in patients with sepsis/septic shock, even after adjustment for confounders. Among patients with septic shock (252 with severe AKI and 226 without AKI (149 with KDIGO stage 1 excluded)), the SNPs rs2093266 and rs1955656 were significantly (odds ratio 0.63, p = 0.04276) associated with stage 2–3 AKI after adjusting for clinical and demographic variables.
Conclusions
The SNPs rs2093266 in the SERPINA4 and rs1955656 in the SERPINA5 were associated with the development of severe AKI (KDIGO stage 2–3) in critically ill patients with septic shock. For the other SNPs, we did not confirm the previously reported associations.
Similar content being viewed by others


Background
In critically ill patients, the incidence of acute kidney injury (AKI) is high - 39% in the recent prospective, observational, multicenter study, the Finnish Acute Kidney Injury (FINNAKI) study, which was conducted in Finnish intensive care units (ICUs) [1]. In other prospective studies in critically ill patients the incidence of AKI is reported as 24–66% [2, 3]. Although the pathophysiology of AKI has been investigated, there is no single explanation for the condition due to the multifactorial nature of the syndrome. Sepsis is the most common factor predisposing to AKI in the critically ill. In patients with sepsis the incidence of AKI is 31–53% [4–6] and in patients with septic shock it is even higher, at 47–61% [7, 8]. The previously identified risk factors for septic AKI, such as age, sex, and baseline comorbidities, have failed to reliably predict individual risk of septic AKI [9]. Thus, it is plausible that genetic variability between individuals may explain a significant part of the risk.
Genetic predisposition to AKI has been previously studied in candidate genes, by testing associations between single nucleotide polymorphisms (SNP) from candidate genes and a phenotype. Our recent systematic review confirmed that despite some positive associations there are no conclusive data [10]. A study by Frank et al. [11] provided one of the very first hypothesis-free approaches to septic AKI; it comprised 887 patients in septic shock defined according to American College of Chest Physicians/Society of Critical Care Medicine (ACCP/SCCM) criteria [12], who were genotyped using a large-scale genotyping microarray. In this study, five SNPs were associated with AKI after validating the results in an additional sample. Interestingly, the associated SNPs are in the apoptosis pathway genes. The SNP rs8094315 and SNP rs12457893 are located in the intron of B-cell CLL/lymphoma 2 (BCL2) –gene. The SNPs rs2093266 in the serpin peptidase inhibitor, clade A (alpha-1 antiproteinase, antitrypsin), member 4 (SERPINA4) gene and SNP rs1955656 in the serpin peptidase inhibitor, clade A (alpha-1 antiproteinase, antitrypsin), member 5 (SERPINA5) gene are in complete linkage disequilibrium (LD). There was also association between the SNP rs625145 in the salt-inducible kinase family 3 (SIK3) gene and AKI. In this study we aimed to replicate the aforementioned findings [9] in a prospective cohort of critically ill patients with sepsis.
Methods
Study population
This study is a predetermined genetic study of the prospective, observational, multicenter FINNAKI study, in which patients were recruited from 17 Finnish ICUs. Details of the FINNAKI study have been published elsewhere [1] and are presented in Additional file 1. The Ethics Committee of the Department of Surgery in Helsinki University Hospital approved the study. An informed separate written consent for genetic samples was obtained from the patient or next of kin at the initiation, with the option of deferred consent. The main study ended on 1 February 2012, and recruitment was extended until 30 April 2012 to achieve an adequate number of patients with sepsis. The study was conducted according to the Declaration of Helsinki.
Data collection
We collected the study-specific data items (approximately 80% of the data) on admission and daily until day 5 or ICU discharge using an electronic case report form (CRF). Data comprised previous and current health status, medication, risk factors for AKI, laboratory values and operations preceding ICU admission, sepsis and related organ dysfunctions, and focus of infection. Presence of AKI and/or sepsis was screened until ICU discharge or day 5 at the latest if the patient was still in the ICU. Routine data were collected with the help of the Finnish Intensive Care Consortium, which consists of 25 ICUs nationwide.
Definitions
For staging of AKI, plasma creatinine was measured daily and urine output hourly. We defined and staged AKI according to the new Kidney Disease: Improving Global Outcomes (KDIGO) AKI criteria [13]. We sought to compare patients with a severe phenotype of AKI (KDIGO stage 2–3) to patients with no AKI. Thus, we excluded patients with KDIGO stage-1 AKI from the current analysis because their phenotype may be seen as indecisive. We defined sepsis and septic shock according to the ACCP/SCCM definitions [12], a definition also used in the previous report [11].
Blood sampling and DNA extraction
Whole blood was collected at enrollment and after separation of plasma, stored at -80 °C for subsequent DNA extraction. DNA was isolated on a Chemagic 360 instrument (Perkin Elmer, Baesweiler, Germany), based on magnetic bead technology, using a Chemagic DNA Blood10k Kit according to the manufacturer’s instructions. DNA concentrations were determined using UV light and PicoGreen methods, and samples were diluted into 10 ng/μl for genotyping.
Genotype analysis
Genotyping was performed at the Technology Centre of the Institute for Molecular Medicine Finland (FIMM), University of Helsinki. The genotyping was done using Agena MassARRAY® system and the iPLEXTM Gold Assay (Agena BioscienceTM, San Diego, CA, USA). This method has excellent success (>95%) and accuracy (100%) [14]. Genotyping reactions were performed on 20 ng of dried genomic DNA in 384-well plates according to the manufacturer’s recommendations and using their reagents [15]. Both polymerase chain reaction (PCR) and extension primers were designed using MassARRAY Assay Design software (Agena BioscienceTM) (Additional file 2). The data were collected using the MassARRAY Compact System (Agena BioscienceTM) and the genotypes were called using TyperAnalyzer software (Agena BioscienceTM).
We examined genotyping quality by a detailed quality control procedure consisting of success rate check, duplicated samples, water controls, and Hardy-Weinberg equilibrium (HWE) testing. In addition, the genotype calls were checked manually and corrected when necessary. Genotyping personnel were blinded to the clinical status of the patients.
Statistical analysis
We compared the clinical and demographic variables to test for significant differences between groups using the Fisher exact test for categorical variables and the Mann-Whitney U test for continuous variables. We present data as medians and interquartile ranges, or absolute values and percentages. Statistical analyses of the demographic and clinical variables were performed using the SPSS Statistics version 22 (IBM Corp., Armonk, NY, USA).
Associations between AKI and SNP were adjusted for clinical characteristics that differed significantly between patients with and without AKI. In addition to the univariate analysis we performed multivariate analysis using logistic regression by entering variables, selecting characteristics with a p value <0.2 in univariate analysis. The percentage of missing data was 15.9%. The missing data were imputed on the assumption of being unaffected for categorical variables and on the median for continuous variables.
Genetic association tests were performed using logistic regression and the PLINK software [16]. As in the previous study an additive genetic model was assumed. However, confirmatory tests were performed using recessive and dominant genetic models. In the primary analysis patients with sepsis and AKI (KDIGO stage 2–3) were compared to patients with sepsis but no AKI. Secondary analyses were performed including cases and controls from the entire cohort, and was performed separately only in those with septic shock. As this was a replication study, we considered all p values <0.05 significant.
Power calculations
Power calculations were made using Genetic Power Calculator [17], assuming allele frequencies and odds ratios from the validation cohort from the study by Frank et al. [11], and with the assumption of 299 patients and 354 controls, a prevalence of AKI of 39,% and a type I error rate of 0.005. For detailed power calculations for each SNP see Additional file 3.
Results
Patients
We prospectively enrolled 2968 ICU patients in the FINNAKI genetic study, as presented in the study flowchart (Fig. 1). After excluding ineligible patients, there were 2567 critically ill patients, of whom 837 (32.6%) had sepsis. Of these, 299 (35.7% of the 837) patients developed KDIGO stage 2–3 AKI and 354 (42.3% of 837) patients with no AKI served as controls (Fig. 1, orange dashed line). Thus, the genetic associations were studied among 653 patients with sepsis, of whom 478 (73.2%) had septic shock. Among patients with septic shock, 252 (40.2% of 627) had severe AKI and 226 (36.0% of 627) did not have AKI (Fig. 1, red dashed line). In the entire genetic cohort, there were 601 (23.4% of 2567) patients who developed KDIGO stage 2–3 AKI and 1545 (60.2% of 2567) patients who did not develop AKI (Fig. 1, blue dashed line).

Study flowchart. AKI acute kidney injury, KDIGO Kidney Disease: Improving Global Outcomes, FINNAKI Finnish Acute Kidney Injury study
The baseline characteristics of the patients with sepsis who did and did not have AKI are presented in Table 1. The baseline characteristics of the patients with septic shock who did and did not have AKI are presented in Table 2. The baseline characteristics of the entire cohort are presented in Additional file 4.
Genetic associations
All of the polymorphisms tested were in HWE. None of the five SNPs investigated, rs8094315 (odds ratio (OR) 1.10, p = 0.48), rs12457893 (OR 1.02, p = 0.87), rs2093266 (OR 0.77, p = 0.15), rs1955656 (OR 0.77, p = 0.15), and rs625145 (OR 0.88, p = 0.38), was significantly associated with AKI in our analysis in patients with sepsis in the additive genetic model (Table 3). The SNPs rs2093266 and rs1955656 are in complete linkage disequilibrium (LD) and thus present identical results.
In logistic regression analysis in patients with sepsis, higher body mass index (BMI), not having chronic obstructive pulmonary disease (COPD), use of non-steroidal anti-inflammatory drugs (NSAID) as daily medication, administration of contrast medium prior to ICU admission, simplified acute physiology score II (SAPS II) without renal or age components, and source of infection were significantly associated with KDIGO stage 2–3 AKI (Additional file 5). Adjustment for these clinical and demographic factors in the patients with sepsis did not change the results for genetic association, which were not statistically significant (Table 3).
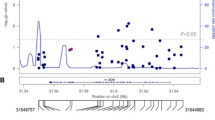
In patients with septic shock, none of the investigated SNPs was significantly associated with AKI in univariate analysis (Table 4). After adjusting for clinical and demographic variables that remained significant in logistic regression (BMI, use of NSAID as daily medication, arteriosclerosis, COPD, administration of contrast medium prior to ICU admission, administration of colloids prior to ICU admission, SAPS II without age or renal components, operative admission, and source of infection (Additional file 6)) SNPs rs2093266 and rs1955656 were significantly associated with AKI (OR 0.63, 95% CI 0.40 to 0.98, p = 0.043, for each) (Table 4, Fig. 2). The carriers of the minor alleles of these SNPs (A and A, respectively) had a decreased risk of developing AKI. This association was in the same direction as in the previous report. The minor allele frequencies of all investigated SNPs in patients with septic shock are presented in Fig. 2.

Minor allele frequencies of all polymorphisms studied in patients with septic shock (n = 478). Patients (red) had severe acute kidney injury (AKI) (Kidney Disease: Improving Global Outcomes (KDIGO) stage 2 or 3 AKI, n = 252) and controls (blue) were ICU patients without AKI. The p values shown above the bars are for the multivariate tests of association between the polymorphisms and AKI. *Significant p values
When the same analyses were performed in the entire genetic cohort, there was no evidence of association between any of the SNPs and AKI in univariate or multivariate models when adjusting for clinical and demographic variables that remained significant in logistic regression (Additional files 7 and 8).
Using recessive and dominant genetic models did not change the results: SNPs rs8094315, rs12457893 and rs625145 were not associated with AKI in any of the subgroups studied. The protective association with SNPs rs2093266 and rs1955656 prevailed in patients in septic shock in the dominant adjusted model (OR 0.59, p = 0.034, for each) (Additional file 9). The self-assessed quality score of the study was 9/10 [18] (Additional file 10).
Discussion
In this study we confirmed the previously reported association between AKI and two polymorphisms, rs2093266 and rs1955656 in apoptosis-related genes SERPINA 4 and SERPINA5 in patients with septic shock. Both in our study and in the original study the minor alleles of these SNPs provided protection from AKI. The association signal was seen in both additive and dominant genetic models but not in the recessive model, suggesting that merely one protective allele is sufficient.
Our study was based on a previous report suggesting that polymorphisms within apoptosis-related genes may be associated with the development of AKI. In this study comprising 887 patients with septic shock, AKI was associated with five SNPs [11]. To our knowledge this is the first successful replication of two of these SNPs. There was no evidence in our cohort of significant association between AKI and the other three polymorphisms tested, rs8094315, rs12457893, and rs625145.
The SNP rs2093266 is located in an intronic region of SERPINA4 gene encoding kallistatin, a serine proteinase inhibitor that has multiple regulatory roles in biological processes [19, 20]. In kallistatin there are two functional domains, an active site and a heparin-binding site, through which it regulates several signaling and biological pathways. Along with its functions in relation to apoptosis, it has anti-inflammatory, antioxidant, vasodilator and angiogenesis inhibiting functions [21]. All these mechanisms are relevant in septic AKI and could thus explain the better outcome.
In recent mouse model studies, Kallistatin has been associated with attenuated inflammation and organ injury and decreased mortality in established sepsis [22], and with improved survival in sepsis-related acute lung injury [23]. Of note, it may also have a renoprotective role against diabetic nephropathy [24]. rs1955656 in SERPINA5 is strongly correlated with rs2093266 and as suspected before, this association with AKI could be driven by rs2093266. Notably, the product of SERPINA5 is known to inhibit activated protein C. This protein C inhibitor (PCI) plays a role in tumor growth and metastasis through its effect on blood coagulation, but it has also been suggested to inhibit the anti-inflammatory activity of activated protein C [25, 26]. This inflammatory function could possibly explain the protection against septic AKI.
Of the other three SNPs studied, two (rs8094315 and rs12457893) are located in the introns of the apoptosis-related gene BCL2 encoding an integral outer mitochondrial membrane protein BCL2 that blocks the apoptotic death of certain cells [27]. The SNP rs625145 is in SIK3, coding for a member of the AMP-activated protein kinase family that affects the regulation of several genes. This protein is found to suppress inflammatory molecule gene expression in macrophages stimulated with lipopolysaccharides (LPS) [28].
There is no definite consensus on the pathophysiology of AKI, and until recently the most common approach has been to test for association with known genetic variants. These variants have often come up in another phenotype, commonly chronic kidney disease, and, thus, may serve as poor markers of AKI [29, 30]. So far, the most studied polymorphisms are within inflammatory mediator genes [10].
Apoptosis-related genes are good candidates for AKI because there is some evidence that apoptosis is an important mechanism in septic AKI. In a murine model of septic AKI the pathophysiology appears to differ from that of ischemia-reperfusion insult, lacking signs of tubular cell injury by necrosis but showing a substantial number of tubular cells undergoing apoptosis [31]. Lerolle et al. found that in post-mortem kidney biopsies of patients who died of septic shock (n = 19) there was a marked increase in apoptosis and capillary leukocytic infiltration in comparison with patients with trauma and ICU controls [32]. However, there were contradicting results in a separate sample of post-mortem kidney biopsies in patients who died of sepsis [33]. The nature of septic AKI alone appears to be diverse, with temporal and individual variation, and the role of apoptosis is inconclusive [34].
We also tested the association between the five SNPs and development of AKI in all patients with sepsis, but the results were negative. The phenotype of septic shock differs from that of sepsis without shock, reflecting a more severe form of illness and a greater risk of death. Thus, we can speculate that the associations between SNPs and AKI detected in these patients, although not generalizable to the septic cohort, can predict better survival for the carriers of the protective allele in terms of AKI.
The strength of our study is that it was a prospective, relatively large, multicenter study comprising consecutive patients. In addition we used the KDIGO criteria to provide a robust phenotype of AKI and critically ill patients without AKI as controls to increase the power of our study.
There are some important limitations in our study. First, 171 genetic samples (5.8%) could not be analyzed due to failure in the DNA isolation phase or to rejection of samples because of a low genotyping success rate. Second, we did not collect data ont ethnicity. However, 99.9% of Finnish-speaking inhabitants are Caucasian. Third, individual genetic susceptibility factors can be expected to increase the AKI risk with values just exceeding an OR of 1 [35]. In our power calculations we used the ORs reported in the original study, and, thus, our study might have been underpowered to replicate the results for BCL2 and SIK3. Fourth, we did not adjust the p values for multiple testing, in this replication of positive findings.
Finally, in contrast to the previous study [11] we excluded patients with chronic kidney disease. Furthermore, we aimed to strengthen the phenotype by comparing patients without AKI to patients with more severe AKI (KDIGO stage 2–3), thus excluding those with KDIGO stage 1. We reasoned that this group would include patients with only KDIGO stage-1 urine output (not included in [11]) criteria, whose phenotype clearly differs from that of more severe acute kidney.
These findings provide some interesting questions for future research. The functions of the SNPs rs2093266 in the SERPINA4 and rs1955656 in the SERPINA5 for the protein products are yet to be determined. If further studies can provide independent evidence supporting the role of these SNPs in AKI susceptibility, information about the genotype of either of these SNPs may add to the battery of risk-predicting tools. However, the effect size of the SNPs is too small for the genotype information to work as an independent biomarker in a clinical setting.
Conclusions
In this study we aimed to replicate the previous findings associating polymorphisms within apoptosis-related genes to AKI. We found that SNPs rs2093266 in the SERPINA4 and rs1955656 in the SERPINA5 were associated with KDIGO stage 2–3 AKI in critically ill patients in septic shock.
Abbreviations
- ACCP/SCCM:
-
American College of Chest Physicians/Society of Critical Care Medicine
- ACE:
-
Angiotensin-converting enzyme
- AKI:
-
Acute kidney injury
- AMP:
-
Adenosine monophosphate
- ARB:
-
Angiotensin receptor blocker
- BCL2:
-
B-cell CLL/lymphoma 2
- BMI:
-
Body mass index
- COPD:
-
Chronic obstructive pulmonary disease
- CRF:
-
Case report form
- DNA:
-
Deoxyribonucleic acid
- FIMM:
-
Institute for Molecular Medicine Finland
- FINNAKI:
-
Finnish Acute Kidney Injury
- HWE:
-
Hardy-Weinberg equilibrium
- ICU:
-
Intensive care unit
- KDIGO:
-
Kidney Disease: Improving Global Outcomes
- LD:
-
Linkage disequilibrium
- LPS:
-
Lipopolysaccharide
- NSAID:
-
Non-steroidal anti-inflammatory drug
- OR:
-
Odds ratio
- PCI:
-
Protein C inhibitor
- SAPS II:
-
Simplified acute physiology score II
- SERPINA4:
-
Serpin peptidase inhibitor, clade A (alpha-1 antiproteinase, antitrypsin), member 4
- SERPINA5:
-
Serpin peptidase inhibitor, clade A (alpha-1 antiproteinase, antitrypsin), member 5
- SIK3:
-
Salt-inducible kinase family 3
- SNP:
-
Single nucleotide polymorphism(s)
References
Nisula S, Kaukonen KM, Vaara ST, Korhonen AM, Poukkanen M, Karlsson S, Haapio M, Inkinen O, Parviainen I, Suojaranta-Ylinen R, Laurila JJ, Tenhunen J, Reinikainen M, Ala-Kokko T, Ruokonen E, Kuitunen A, Pettila V, FINNAKI Study Group. Incidence, risk factors and 90-day mortality of patients with acute kidney injury in Finnish intensive care units: the FINNAKI study. Intensive Care Med. 2013;39(3):420–8.
Medve L, Antek C, Paloczi B, Kocsi S, Gartner B, Marjanek Z, Bencsik G, Kanizsai P, Gondos T. Epidemiology of acute kidney injury in Hungarian intensive care units: a multicenter, prospective, observational study. BMC Nephrol. 2011;12:43. doi:10.1186/1471-2369-12-43.
Piccinni P, Cruz DN, Gramaticopolo S, Garzotto F, Dal Santo M, Aneloni G, Rocco M, Alessandri E, Giunta F, Michetti V, Iannuzzi M, Belluomo Anello C, Brienza N, Carlini M, Pelaia P, Gabbanelli V, Ronco C, NEFROINT Investigators. Prospective multicenter study on epidemiology of acute kidney injury in the ICU: a critical care nephrology Italian collaborative effort (NEFROINT). Minerva Anestesiol. 2011;77(11):1072–83.
Poukkanen M, Vaara ST, Pettilä V, Kaukonen K-M, Korhonen A-M, Hovilehto S, Inkinen O, Laru-Sompa R, Kaminski T, Reinikainen M, Lund V, Karlsson S. FINNAKI sg. Acute kidney injury in patients with severe sepsis in Finnish Intensive Care Units. Acta Anaesthesiol Scand. 2013;57(7):863–72.
Lopes JA, Jorge S, Resina C, Santos C, Pereira A, Neves J, Antunes F, Prata MM. Acute kidney injury in patients with sepsis: a contemporary analysis. Int J Infect Dis. 2009;13(2):176–81.
Bagshaw SM, George C, Bellomo R, ANZICS Database Management Committee. Early acute kidney injury and sepsis: a multicentre evaluation. Crit Care. 2008;12(2):R47.
Plataki M, Kashani K, Cabello-Garza J, Maldonado F, Kashyap R, Kor DJ, Gajic O, Cartin-Ceba R. Predictors of acute kidney injury in septic shock patients: an observational cohort study. Clin J Am Soc Nephrol. 2011;6(7):1744–51.
Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C, Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294(7):813–8.
Hoste EA, Clermont G, Kersten A, Venkataraman R, Angus DC, De Bacquer D, Kellum JA. RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care. 2006;10(3):R73.
Vilander LM, Kaunisto MA, Pettilä V. Genetic predisposition to acute kidney injury - a systematic review. BMC Nephrol. 2015;16(1):1–10.
Frank AJ, Sheu CC, Zhao Y, Chen F, Su L, Gong MN, Bajwa E, Thompson BT, Christiani DC. BCL2 genetic variants are associated with acute kidney injury in septic shock*. Crit Care Med. 2012;40(7):2116–23.
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. DEfinitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644–55.
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
Lahermo P, Liljedahl U, Alnaes G, Axelsson T, Brookes AJ, Ellonen P, Groop PH, Hallden C, Holmberg D, Holmberg K, Keinanen M, Kepp K, Kere J, Kiviluoma P, Kristensen V, Lindgren C, Odeberg J, Osterman P, Parkkonen M, Saarela J, Sterner M, Stromqvist L, Talas U, Wessman M, Palotie A, Syvanen AC. A quality assessment survey of SNP genotyping laboratories. Hum Mutat. 2006;27(7):711–4.
Jurinke C, van den Boom D, Cantor CR, Koster H. Automated genotyping using the DNA MassArray technology. Methods Mol Biol. 2002;187:179–92.
Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MA, Bender D, Maller J, Sklar P, de Bakker PI, Daly MJ, Sham PC. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet. 2007;81(3):559–75.
Purcell S, Cherny SS, Sham PC. Genetic Power Calculator: design of linkage and association genetic mapping studies of complex traits. Bioinformatics. 2003;19(1):149–50.
Clark MF, Baudouin SV. A systematic review of the quality of genetic association studies in human sepsis. Intensive Care Med. 2006;32(11):1706–12.
Silverman GA, Bird PI, Carrell RW, Church FC, Coughlin PB, Gettins PG, Irving JA, Lomas DA, Luke CJ, Moyer RW, Pemberton PA, Remold-O’Donnell E, Salvesen GS, Travis J, Whisstock JC. The serpins are an expanding superfamily of structurally similar but functionally diverse proteins. Evolution, mechanism of inhibition, novel functions, and a revised nomenclature. J Biol Chem. 2001;276(36):33293–6.
Chao J, Miao RQ, Chen V, Chen LM, Chao L. Novel roles of kallistatin, a specific tissue kallikrein inhibitor, in vascular remodeling. Biol Chem. 2001;382(1):15–21.
Chao J, Bledsoe G, Chao L. Protective role of kallistatin in vascular and organ injury. Hypertension. 2016;68(3):533–41.
Li P, Guo Y, Bledsoe G, Yang ZR, Fan H, Chao L, Chao J. Kallistatin treatment attenuates lethality and organ injury in mouse models of established sepsis. Crit Care. 2015;19:200. doi:10.1186/s13054-015-0919-4.
Lin WC, Chen CW, Huang YW, Chao L, Chao J, Lin YS, Lin CF. Kallistatin protects against sepsis-related acute lung injury via inhibiting inflammation and apoptosis. Sci Rep. 2015;5:12463.
Yiu WH, Wong DW, Wu HJ, Li RX, Yam I, Chan LY, Leung JC, Lan HY, Lai KN, Tang SC. Kallistatin protects against diabetic nephropathy in db/db mice by suppressing AGE-RAGE-induced oxidative stress. Kidney Int. 2016;89(2):386–98.
Akita N, Ma N, Okamoto T, Asanuma K, Yoshida K, Nishioka J, Shimaoka M, Suzuki K, Hayashi T. Host protein C inhibitor inhibits tumor growth, but promotes tumor metastasis, which is closely correlated with hypercoagulability. Thromb Res. 2015;135(6):1203–8.
Hayashi T, Nishioka J, Kamada H, Asanuma K, Kondo H, Gabazza EC, Ido M, Suzuki K. Characterization of a novel human protein C inhibitor (PCI) gene transgenic mouse useful for studying the role of PCI in physiological and pathological conditions. J Thromb Haemost. 2004;2(6):949–61.
Hetts SW. To die or not to die: an overview of apoptosis and its role in disease. JAMA. 1998;279(4):300–7.
Sanosaka M, Fujimoto M, Ohkawara T, Nagatake T, Itoh Y, Kagawa M, Kumagai A, Fuchino H, Kunisawa J, Naka T, Takemori H. Salt-inducible kinase 3 deficiency exacerbates lipopolysaccharide-induced endotoxin shock accompanied by increased levels of pro-inflammatory molecules in mice. Immunology. 2015;145(2):268–78.
Doi K, Noiri E, Nakao A, Fujita T, Kobayashi S, Tokunaga K. Functional polymorphisms in the vascular endothelial growth factor gene are associated with development of end-stage renal disease in males. J Am Soc Nephrol. 2006;17(3):823–30.
Tong Z, Yang Z, Patel S, Chen H, Gibbs D, Yang X, Hau VS, Kaminoh Y, Harmon J, Pearson E, Buehler J, Chen Y, Yu B, Tinkham NH, Zabriskie NA, Zeng J, Luo L, Sun JK, Prakash M, Hamam RN, Tonna S, Constantine R, Ronquillo CC, Sadda S, Avery RL, Brand JM, London N, Anduze AL, King GL, Bernstein PS, Watkins S, Genetics of Diabetes and Diabetic Complication Study Group, Jorde LB, Li DY, Aiello LP, Pollak MR, Zhang K. Promoter polymorphism of the erythropoietin gene in severe diabetic eye and kidney complications. Proc Natl Acad Sci USA. 2008;105(19):6998–7003.
Lee SY, Lee YS, Choi HM, Ko YS, Lee HY, Jo SK, Cho WY, Kim HK. Distinct pathophysiologic mechanisms of septic acute kidney injury: role of immune suppression and renal tubular cell apoptosis in murine model of septic acute kidney injury. Crit Care Med. 2012;40(11):2997–3006.
Lerolle N, Nochy D, Guerot E, Bruneval P, Fagon JY, Diehl JL, Hill G. Histopathology of septic shock induced acute kidney injury: apoptosis and leukocytic infiltration. Intensive Care Med. 2010;36(3):471–8.
Takasu O, Gaut JP, Watanabe E, To K, Fagley RE, Sato B, Jarman S, Efimov IR, Janks DL, Srivastava A, Bhayani SB, Drewry A, Swanson PE, Hotchkiss RS. Mechanisms of cardiac and renal dysfunction in patients dying of sepsis. Am J Respir Crit Care Med. 2013;187(5):509–17.
Morrell ED, Kellum JA, Pastor-Soler N, Hallows KR. Septic acute kidney injury: molecular mechanisms and the importance of stratification and targeting therapy. Crit Care. 2014;18(5):501.
Frazer KA, Murray SS, Schork NJ, Topol EJ. Human genetic variation and its contribution to complex traits. Nat Rev Genet. 2009;10(4):241–51.
Acknowledgements
We thank the FINNAKI Study Group: Central Finland Central Hospital: Raili Laru-Sompa, Anni Pulkkinen, Minna Saarelainen, Mikko Reilama, Sinikka Tolmunen, Ulla Rantalainen, Marja Miettinen; East Savo Central Hospital: Markku Suvela, Katrine Pesola, Pekka Saastamoinen, Sirpa Kauppinen; Helsinki University Central Hospital: Ville Pettilä, Kirsi-Maija Kaukonen, Anna-Maija Korhonen, Sara Nisula, Suvi Vaara, Raili Suojaranta-Ylinen, Leena Mildh, Mikko Haapio, Laura Nurminen, Sari Sutinen, Leena Pettilä, Helinä Laitinen, Heidi Syrjä, Kirsi Henttonen, Elina Lappi, Hillevi Boman; Jorvi Central Hospital: Tero Varpula, Päivi Porkka, Mirka Sivula, Mira Rahkonen, Anne Tsurkka, Taina Nieminen, Niina Prittinen; KantaHäme Central Hospital: Ari Alaspää, Ville Salanto, Hanna Juntunen, Teija Sanisalo; Kuopio University Hospital: Ilkka Parviainen, Ari Uusaro, Esko Ruokonen, Stepani Bendel, Niina Rissanen, Maarit Lång, Sari Rahikainen, Saija Rissanen, Merja Ahonen, Elina Halonen, Eija Vaskelainen; Lapland Central Hospital: Meri Poukkanen, Esa Lintula, Sirpa Suominen; Länsi Pohja Central Hospital: Jorma Heikkinen, Timo Lavander, Kirsi Heinonen, Anne-Mari Juopperi; Middle Ostrobothnia Central Hospital: Tadeusz Kaminski, Fiia Gäddnäs, Tuija Kuusela, Jane Roiko; North Karelia Central Hospital: Sari Karlsson, Matti Reinikainen, Tero Surakka, Helena Jyrkönen, Tanja Eiserbeck, Jaana Kallinen; Satakunta Hospital District: Vesa Lund, Päivi Tuominen, Pauliina Perkola, Riikka Tuominen, Marika Hietaranta, Satu Johansson; South Karelia Central Hospital: Seppo Hovilehto, Anne Kirsi, Pekka Tiainen, Tuija Myllärinen, Pirjo Leino, Anne Toropainen; Tampere University Hospital: Anne Kuitunen, Ilona Leppänen, Markus Levoranta, Sanna Hoppu, Jukka Sauranen, Jyrki Tenhunen, Atte Kukkurainen, Samuli Kortelainen, Simo Varila; Turku University Hospital: Outi Inkinen, Niina Koivuviita, Jutta Kotamäki, Anu Laine; Oulu University Hospital: Tero Ala-Kokko, Jouko Laurila, Sinikka Sälkiö; Vaasa Central Hospital: Simo-Pekka Koivisto, Raku Hautamäki, Maria Skinnar. We also thank the Institute for DeCode (Reykjavik, Iceland) for DNA extraction, Molecular Medicine Finland (FIMM, Helsinki, Finland) for genotyping, Tieto Healthcare and Welfare Ltd (Helsinki, Finland) for the FINNAKI study database management, and Martin Sigurdsson MD, PhD for his insightful comments on the manuscript.
Funding
This study was supported by grants TYH 2013343 and 2016243 from the Helsinki University Hospital research funding (VP) and a grant from the Sigrid Juselius Foundation (VP).
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article and its additional files.
Authors’ contributions
LV contributed to the data analysis and interpretation of the data and drafted the manuscript. MK contributed to the data analysis and interpretation of the data and participated in editing and finalizing the manuscript. SV contributed to the data analysis and interpretation of the data, contributed to the data acquisition and database access, and participated in editing and finalizing the manuscript. VP conceived the study, contributed to its design and coordination, and participated in editing and finalizing the manuscript. All authors reviewed and revised the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The Ethics Committee of the Department of Surgery in Helsinki University Hospital approved the study (reference number 18/13/03/02/2010). Separate informed written consent for genetic samples was obtained from the patient or next of kin at the initiation, with the option of deferred consent.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional files
Additional file 1:
FINNAKI study enrollment and inclusion of patients. Report of the enrollment period and inclusion and exclusion criteria. (DOC 22 kb)
Additional file 2:
Primer sequences. Polymerase chain reaction (PCR) 1 and 2 and extension primer sequences. (DOC 30 kb)
Additional file 3:
Detailed power calculations for each SNP, for power to report the additionional risk given known minor allele frequencies and risk ratios. (DOC 22 kb)
Additional file 4:
Demographic and baseline characteristics of the entire cohort according to the presence of acute kidney injury: the main demographic and baseline characteristics of the patients included in the FINNAKI genetic study. (DOC 86 kb)
Additional file 5:
Logistic regression (the “enter” method) in patients with sepsis (n = 653) in differing demographic variables, missing data imputed. Number (N) of imputed values and percentages of the cohort are given. Results of logistic regression in patients with sepsis showing that higher BMI, not having COPD, use of NSAID as daily medication, administration of contrast medium prior to ICU admission, SAPS II score without renal or age components, and source of infection were significantly associated with KDIGO stage 2–3 AKI. (DOC 54 kb)
Additional file 6:
Logistic regression (“enter” method) in patients with septic shock (n = 478) in differing demographic variables, missing data imputed. Number (N) of imputed values and percentages of the cohort are given. Results of logistic regression in patients with septic shock showing that BMI, use of NSAID as daily medication, arteriosclerosis, COPD, administration of contrast medium prior to ICU admission, administration of colloids prior to ICU admission, SAPS II without age or renal components, operative admission, and source of infection were significantly associated with KDIGO stage 2–3 AKI. (DOC 53 kb)
Additional file 7:
Association between acute kidney injury and the polymorphisms studied in all genotyped patients (n = 2146) (additive genetic model). Association between acute kidney injury and the studied polymorphisms in all genotyped patients was tested in univariate and multivariate models. No significant associations are reported. (DOC 35 kb)
Additional file 8:
Logistic regression (“enter” method) in all genotyped patients (n = 2146) in differing demographic variables, missing data imputed. Number (N) of imputed values and the percentages of the cohort are given. Logistic regression in all genotyped patients showed that BMI, chronic liver disease, use of NSAID as daily medication, use of warfarin as daily medication, administration of contrast medium prior to ICU admission, administration of colloids prior to ICU admission, administration of albumin prior to ICU admission, maximum white blood cell count, minimum platelet count, SAPS II without age or renal components, operative admission, and source of infection were significantly associated with KDIGO stage 2–3 AKI. (DOC 72 kb)
Additional file 9:
Association between acute kidney injury and the studied polymorphisms, recessive and dominant genetic models. Association between acute kidney injury and the polymorphisms studied in septic patients, patients with septic shock and all genotyped patients, recessive and dominant genetic models. Univariate and multivariate associations are reported. In dominant genetic model in patients with septic shock the SNPs rs2093266 and rs1955656 were significantly associated with KDIGO stage 2–3 AKI after adjustment. (DOC 89 kb)
Additional file 10:
Fulfillment of quality criterion by Clark et al. for genetic association studies, which were originally validated for AKI studies by Lu et al., and were later adapted by Vilander et al. Self-assessment of the study quality criteria is shown. (DOC 45 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Vilander, L.M., Kaunisto, M.A., Vaara, S.T. et al. Genetic variants in SERPINA4 and SERPINA5, but not BCL2 and SIK3 are associated with acute kidney injury in critically ill patients with septic shock. Crit Care 21, 47 (2017). https://doi.org/10.1186/s13054-017-1631-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-017-1631-3