
Abstract
Introduction
Neurocritical care patients are at high risk for stress-related upper gastrointestinal (UGI) bleeding. The aim of this meta-analysis was to evaluate the risks and benefits of stress ulcer prophylaxis (SUP) in this patient group.
Methods
A systematic search of major electronic literature databases was conducted. Eligible studies were randomized controlled trials (RCTs) in which researchers compared the effects of SUP (with proton pump inhibitors or histamine 2 receptor antagonists) with placebo or no prophylaxis in neurocritical care patients. The primary outcome was UGI bleeding, and secondary outcomes were all-cause mortality and nosocomial pneumonia. Study heterogeneity was sought and quantified. The results were reported as risk ratios/relative risks (RRs) with 95 % confidence intervals (CIs).
Results
We included 8 RCTs comprising an aggregate of 829 neurocritical care patients. Among these trials, one study conducted in a non–intensive care unit setting that did not meet our inclusion criteria was ultimately included based on further evaluation. All studies were judged as having a high or unclear risk of bias. SUP was more effective than placebo or no prophylaxis at reducing UGI bleeding (random effects: RR 0.31; 95 % CI 0.20–0.47; P < 0.00001; I 2 = 45 %) and all-cause mortality (fixed effects: RR 0.70; 95 % CI 0.50–0.98; P = 0.04; I 2 = 0 %). There was no difference between SUP and placebo or no prophylaxis regarding nosocomial pneumonia (random effects: RR 1.14; 95 % CI 0.67–1.94; P = 0.62; I 2 = 42 %). The slight asymmetry of the funnel plots raised the concern of small trial bias, and apparent heterogeneity existed in participants, interventions, control treatments, and outcome measures.
Conclusions
In neurocritical care patients, SUP seems to be more effective than placebo or no prophylaxis in preventing UGI bleeding and reducing all-cause mortality while not increasing the risk of nosocomial pneumonia. The robustness of this conclusion is limited by a lack of trials with a low risk of bias, sparse data, heterogeneity among trials, and a concern regarding small trial bias.
Trial registration
International Prospective Register of Systematic Reviews (PROSPERO) identifier: CRD42015015802. Date of registration: 6 Jan 2015.
Similar content being viewed by others


Introduction
Stress ulcer and stress-related upper gastrointestinal (UGI) bleeding is common in critically ill patients. The reported incidence of overt UGI bleeding ranges from 0.1 % to 4 % among all intensive care unit (ICU) patients and was up to 15 % among patients who received no prophylaxis, which was associated with worsened outcomes [1, 2].
Both the American Society of Health-System Pharmacists (ASHP) and the Surviving Sepsis Campaign guidelines recommend stress ulcer prophylaxis (SUP) with either histamine 2 receptor antagonists (H2RAs) or proton pump inhibitors (PPIs) as standard care in patients with a high risk of stress-related UGI bleeding [3, 4]. However, the rationale and level of evidence for this recommendation have been questioned by the findings of some recent randomized controlled trials (RCTs) and meta-analyses [1, 5–7]. Even though two recent meta-analyses showed that PPIs were more effective than H2RAs in preventing UGI bleeding in critically ill patients without increasing the risk of nosocomial pneumonia [8, 9], one meta-analysis and trial sequential analysis comparing the use of SUP versus no prophylaxis or placebo found that the quality and quantity of evidence for the use of SUP in adult ICU patients is low and that there is no firm evidence for benefit or harm of SUP [5].
Neurocritical care patients, however, are a unique subgroup. Neurological injury is an acknowledged risk factor for UGI bleeding, and the ASHP guidelines also recommend SUP for ICU patients with either an inability to obey simple commands or a Glasgow Coma Scale (GCS) score ≤10 [3]. The risk is potentiated by other major risk factors, including mechanical ventilation, hypotension, and coagulopathy [1]. Neurological injury, combined with severe physiological stress and critical illness, has been shown to increase the morbidity and mortality associated with stress-related UGI bleeding in the setting of acute neurological diseases, including traumatic brain injury (TBI) [10–14], spontaneous intracerebral hemorrhage (ICH) [15, 16], ischemic stroke [17–19], spinal cord injury [20, 21], central nervous system (CNS) infections, and so forth [22, 23].
Therefore, the findings of a meta-analysis including heterogeneous critically ill patients may not necessarily apply, and uncertainty over whether routine SUP is indicated in neurocritical care patients exists among clinicians. New evidence from one RCT favors the prophylactic use of PPIs over H2RAs or placebo in critically ill neurosurgical patients with ICH [16], which has emerged after a report of the most recent meta-analysis on this topic in general ICU patients [5]. We performed a systematic review and meta-analysis to weigh the risks of SUP against the benefits to answer the following research question: Is SUP with PPIs or H2RAs in neurocritical care patients superior to placebo or no prophylaxis in terms of UGI bleeding, all-cause mortality, and nosocomial pneumonia?
Methods
This systematic review was conducted mainly using the methodology recommended by the Cochrane Collaboration [24], despite some necessary adaptations customized to the topic, and the review was prepared according to the PRISMA statement [25]. The protocol is published in the International Prospective Register of Systematic Reviews (PROSPERO identifier: CRD42015015802).
Eligibility criteria
Types of studies
RCTs were eligible for inclusion.
Population
The study population was adult patients (age ≥18 years, without an upper limit) who received critical care for at least one of the following conditions: TBI, subarachnoid hemorrhage, ICH, ischemic stroke, anoxic brain injury, spinal cord injury, CNS infections, or other acute neurological injuries.
Intervention
The intervention was patients receiving SUP with at least one intervention group of PPIs or H2RAs.
Control
The control group was patients receiving placebo or no prophylaxis.
Outcome
UGI bleeding was the primary outcome of this meta-analysis. All-cause mortality and nosocomial pneumonia were secondary outcomes. The outcome measures were used as defined by the authors of the original trials.
We included studies regardless of language of publication and publication status. We excluded studies in animals, in pediatric patients, and those in which the authors reported only non-patient-centered outcomes such as gastric pH and gastric colonization. For RCTs involving mixed populations but not presenting separate data for neurocritical care patients, the pooled results were included only if >75 % of patients had a neurocritical care diagnosis [26].
Search strategy
MEDLINE, Embase, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews were searched from their inception date until the first week of February 2015. To identify RCTs involving neurocritical care patients, the Boolean operator “AND” was used to combine four search concepts: stress ulcer, SUP, neurocritical care, and clinical trials. These concepts were created using a combination of National Library of Medicine Medical Subject Headings terms and keywords, and they were combined using the Boolean operator “OR” (Additional file 1: Appendix).
A separate search was also performed to identify clinical trials involving general critical care patients with heterogeneous diagnostic categories in multisystem ICUs (Additional file 1: Appendix). Previously published meta-analyses were used to identify relevant articles [1, 5–9, 27]. We reviewed the retrieved studies to determine if separate results were reported specifically for neurocritical care patients.
Study selection
The retrieved records were reviewed independently and in duplicate by two authors (BL and SL). By screening of the titles, abstracts, and keywords, studies that were obviously not relevant were excluded. The remaining studies were assessed in full text. Disagreements were resolved by consensus.
Data extraction
Two authors (BL and SL) extracted the data independently and in duplicate using a data extraction form, which was developed according to the recommendations of the Cochrane Collaboration. The form was tested in several studies and well-customized to the topic of the present review. The extracted information included trial characteristics (title, author, year of publication, country, trial design, duration, publication status, funding), the characteristics of the trial participants (number, age, sex, diagnosis, Acute Physiology and Chronic Health Evaluation II score, GCS score, other clinical parameters, duration of follow-up, dropout rates, inclusion criteria, risk factors for UGI bleeding, type of nutrition), exclusion criteria, type of intervention and/or control (name, dosing, duration, route of administration, comparator), and outcomes (clinically important bleeding, overt bleeding, occult bleeding, pneumonia, mortality, ICU length of stay, adverse events). Attempts were made to contact all the primary authors of the publications for missing data elements, and more than half responded with useful additional information [13, 15, 16, 22, 28].
Risk of bias assessment
Risk of bias was assessed independently and in duplicate by two authors (BL and AY), using the tool recommended by the Cochrane Collaboration, including domains of random sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, baseline imbalance, and other bias [24]. Disagreements were resolved by consensus. The overall risk of bias for an individual trial was categorized as “low” (if the risk of bias was low in all domains), “unclear” (if the risk of bias was unclear in at least one domain, with no high risk of bias domains), or “high” (if the risk of bias was high in at least one domain) [24].
Statistical analysis
Statistical analysis was performed using RevMan 5.3 software. The risk ratio/relative risk (RR) of each outcome measure was calculated with 95 % confidence interval (CI). Statistical heterogeneity was assessed by the I 2 statistic [24]. I 2 values of approximately 25 %, 50 %, and 75 % represent low, moderate, and high heterogeneity, respectively [9]. Substantial heterogeneity was predefined as P < 0.10 with I 2 > 50 %. We used a fixed effects model if the I 2 statistic was 0; otherwise, we used a random effects model. A test of interaction (with a P value <0.05 considered significant) was performed for each of the subgroups to examine the difference in effect size between two subgroups. Publication bias was assessed by funnel plot asymmetry [29].
Subgroup analyses
To address heterogeneity potentially influencing estimated intervention effects, several strategies were used. Extensive subgroup analyses were conducted, including four predefined subgroup analyses: (1) lower (low or unclear) versus higher (high) risk of bias trials (possible smaller in trials with lower risk of bias [30]); (2) adequate versus inadequate random sequence generation, allocation concealment, and blinding (possibly smaller in trials with adequate random sequence generation, allocation concealment, and blinding [30]); (3) use of PPIs versus H2RAs (possibly larger in trials using PPIs [8, 9]); and (4) placebo trials versus no prophylaxis trials (possibly larger in trials using no prophylaxis [31]). We also conducted three post hoc subgroup analyses: (1) presence of enteral nutrition versus no enteral nutrition (possible larger intervention effect and increased risk of nosocomial pneumonia in trials using enteral nutrition [7]), (2) patients with TBI versus patients with ICH (possible different intervention effect), and (3) trials conducted in Asian versus non-Asian countries (possibly larger in Asian countries [32]). A post hoc random effects model was preferred even if statistical heterogeneity was not significant when apparent clinical and/or methodological diversity was judged to exist.
Results
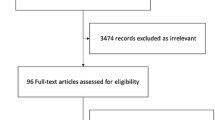
The study selection process is summarized in Fig. 1. Eight studies involving an aggregate of 829 patients were included [11–16, 28]. The main reasons for exclusion were not involving and/or reporting neurocritical care patients and not including a placebo or no prophylaxis group. It is noteworthy that one study conducted in a non-ICU setting but consisting of patients who were critically ill with acute neurological injuries (median GCS 6, range 3–8) and underwent emergency neurosurgery and actually were under critical care perioperatively was also included [22]. Because this trial was a relatively large study with all included patients having a high risk of developing stress ulcers, and despite the appropriateness of excluding patients who underwent nonelective neurosurgery being debatable per se, the results were included in the main analysis. This is a protocol deviation, as we did include patients receiving perioperative critical care outside an ICU. A sensitivity analysis was done to validate the results by excluding the trial conducted in a non-ICU setting.

Study flow diagram. H2RA histamine 2 receptor antagonist, ICU intensive care unit, PPI proton pump inhibitor
Characteristics of included trials
The characteristics of the eight included trials are summarized in Table 1. The definition of primary outcome varied among the trials, with one reporting clinically important UGI bleeding [22], six reporting overt UGI bleeding [11–16], and one reporting seemingly overt UGI bleeding without a specified definition [28].
Participants
In 5 trials all eligible patients were included in the study analysis [12–14, 22, 28], and in 3 trials 111 (24.3 %) of 457 patients were excluded from the analysis due to loss to follow-up and other reasons, including enrollment error, missing data/procedures, lack of consent, bleeding not related to stress ulcer, and early death [11, 15, 16]. Of the 829 patients included in the analysis in all 8 trials, 288 from 4 trials had TBI [11–14], 440 had ICH [11, 15, 16, 28], and the remainder were emergency neurosurgical patients (69 had cerebrovascular disease not specified, 29 had brain tumors, 3 had CNS infections, and 10 had hydrocephalus) [22]. The mean ages of the patients ranged from 29.6 to 61.0 years, and the male-to-female ratio was 1.71:1 (523 vs. 306, respectively). GCS scores were reported in six trials, and the mean GCS score ranged from 5 to 9.8 [11, 12, 14–16, 22]. For each trial, patients’ baseline characteristics in all intervention and control groups were well-balanced. In four trials, patients received enteral nutrition [13, 15, 22, 28].
Interventions and controls
Six trials used H2RA as an intervention [11–15, 22] (one trial used both H2RA and sucralfate as interventions, but the sucralfate group was not included in this meta-analysis), and two trials used more than one intervention (both PPI and H2RA) [16, 28]. The route of administration was intravenous in six trials [11–16], orally in one trial [28], and either orally or intravenously in one trial [22]. Regarding control treatment, placebo was used as a comparator in seven trials [12–16, 22, 28] and no prophylaxis was used in one trial [11].
Risk of bias assessment
No trials were judged to have a low risk of bias in all domains. Three trials had unclear risk of bias [13, 14, 22], and the remaining five trials had a high risk of bias [11, 12, 15, 16, 28] (Fig. 2). It is noteworthy that our judgments regarding the risk of bias in some studies differed from previous systematic reviews [5]. The variation may result from different information identified in the study reports and different interpretation of the tool [33]. The statements supporting our judgment for each included study are provided in Additional file 2. The main reasons for high risk of bias were inadequate blinding or incomplete outcome data. No trials met the criteria of adequate random sequence generation, allocation concealment, and blinding. Therefore, one of the predefined subgroup analyses of trials with adequate versus inadequate random sequence generation, allocation concealment, and blinding could not be done.

Risk of bias summary of review authors’ judgments about each risk of bias item for each included study. Red high risk, green low risk, yellow unclear
Outcome measures
UGI bleeding
UGI bleeding data were available in all eight trials [11–16, 22, 28]. The median duration of follow-up ranged from 2 to 20 days. SUP in neurocritical care patients resulted in a lower incidence of UGI bleeding than treatment with placebo or no prophylaxis (11 % vs. 33 %; random effects: RR 0.31; 95 % CI 0.20–0.47; P < 0.00001; P = 0.09 for heterogeneity; I 2 = 45 %) (Fig. 3). Subgroup analyses showed no significant heterogeneity among the included trials regarding different interventions (P = 0.42 for interaction of PPIs vs. H2RAs) (Table 2) or different neurological pathologies (P = 0.52 for interaction of TBI vs. ICH) (Table 2). However, more complex neurological care conditions than our subgroup analyses could cover were observed across the trials in the areas of disease states and brain injury severity, which may influence the pathophysiology of stress ulcer and the benefits of SUP and thus have compromised the our results. Visual inspection of a funnel plot showed slight asymmetry at the bottom of the funnel plot (Additional file 3: Figure S1).

Forest plot of stress ulcer prophylaxis (SUP) and upper gastrointestinal bleeding. CI confidence interval, M-H Mantel–Haenszel method
All-cause mortality
Mortality data were available in 5 trials involving 381 patients [11–13, 15, 16]. The duration of follow-up ranged from 3 to 30 days, and the median time to the final follow-up assessment for mortality was 20 days. There was a statistically significant decrease in all-cause mortality of patients receiving SUP versus placebo or no prophylaxis (23 % vs. 30 %; fixed effects: RR 0.70; 95 % CI 0.50–0.98; P = 0.04; P = 0.62 for heterogeneity; I 2 = 0 %) (Fig. 4). A post hoc random effects model considering possible clinical heterogeneity showed results consistent with the main analysis (random effects: RR 0.71; 95 % CI 0.51–0.99; P = 0.04), as well as all the subgroup analyses regarding all-cause mortality (data not shown). Visual inspection of a funnel plot showed slight asymmetry (Additional file 4: Figure S2).

Forest plot of stress ulcer prophylaxis (SUP) and all-cause mortality. CI confidence interval, M-H Mantel–Haenszel method
Nosocomial pneumonia
In 4 trials involving 521 patients, researchers reported the incidence of nosocomial pneumonia [14–16, 22]. However, only two of the four trials included explicit definitions of this outcome (they were still different between the two) [14, 22]. The proportion of patients receiving SUP who developed nosocomial pneumonia varied between studies, ranging from 4 % to 37 %. The incidence of nosocomial pneumonia was no greater among patients receiving SUP than among those receiving placebo or no prophylaxis (20 % vs. 17 %; random effects: RR 1.14; 95 % CI 0.67–1.94; P = 0.62; P = 0.16 for heterogeneity; I 2 = 42 %) (Fig. 5). Either the lack or the variation in definitions of outcome measures, different disease severity, and complex neurological care conditions may account for the possible heterogeneity and thus may have compromised the results. Visual impression revealed a similar slight asymmetry in a funnel plot (Additional file 5: Figure S3).

Forest plot of stress ulcer prophylaxis (SUP) and nosocomial pneumonia. CI confidence interval, M-H Mantel–Haenszel method
Subgroup and sensitivity analyses
We found no significant subgroup heterogeneity regarding UGI bleeding, all-cause mortality, or nosocomial pneumonia when we compared trials with higher (high) versus lower (low/unclear) risk of bias, intervention drugs (PPIs vs. H2RAs), comparator types (placebo vs. no prophylaxis), presence of nutrition versus no enteral nutrition, diagnosis (TBI vs. ICH), and study location (Asia vs. non-Asian). The results, including P values for interactions, are summarized in Table 2.
In sensitivity analysis, exclusion of the trial conducted in a non-ICU setting but involving critically ill patients who underwent emergency neurosurgeries had little impact on the results [22]. Specifically, UGI bleeding (random effects: RR 0.28; 95 % CI 0.16–0.47; P < 0.00001; I 2 = 50 %) was significantly reduced and risk of nosocomial pneumonia (random effects: RR 0.94; 95 % CI 0.49–1.78; P = 0.84; I 2 = 37 %) was not increased, consistent with the main analysis.
Discussion
In this meta-analysis, SUP with either H2RAs or PPIs in adult neurocritical care patients was more effective than placebo or no prophylaxis in reducing UGI bleeding and all-cause mortality without increasing the risk of nosocomial pneumonia. However, the main results were limited by the lack of trials with low risk of bias, sparse data, heterogeneity among trials, and concern regarding small trial bias.
UGI bleeding
The mechanisms responsible for stress ulcerations are complex, including multiple factors affecting the imbalance between mucosal protection and gastric acid production. Compared with general ICU patients, critically ill neurosurgical and neurological patients are more vulnerable to stress-related UGI bleeding, as they have increased acid secretion caused by stress-triggered vagal stimulation of the stomach through CNS pathways [18, 23, 34] and impaired mucosal protection resulting from compromised mucosal microcirculation [35]. In addition, the presence of elevated intracranial pressure (ICP) can be found in any mechanism of cerebral injury, which is a well-known contributing factor in stress ulcer formation [15, 16, 23, 36]. These risk factors related to neurological injury could be potentiated by other risk factors, including mechanical ventilation, hypotension, and coagulopathy, which are common in neurocritical care patients as well [1, 23]. Indeed, several studies have shown that neurocritical care patients have increased morbidity and mortality associated with stress-related UGI bleeding [10–23]. In addition, because this increased risk of UGI bleeding is a consequence of elevated ICP, cerebral ischemia, sympathetic hyperactivity, and the inflammatory response that exist in almost all neurocritical care patients [23], it is unlikely that one specific type of neurological injury (such as TBI vs. ICH) predisposes patients to a higher risk than another. Therefore, neurocritical care patients in general warrant special attention to this issue in practice.
The present meta-analysis of UGI bleeding showed a benefit of SUP over placebo or no prophylaxis. However, this apparent benefit of SUP should be conservatively interpreted because (1) the pooled analysis may be influenced by the relatively lower quality of the included trials, as no trial in this meta-analysis was judged to be of low risk of bias in all domains and no single trial had adequate random sequence generation, allocation concealment, and blinding; (2) the slight asymmetry of the funnel plot raised the concern of small trial bias; (3) apparent heterogeneity in participants, interventions, control treatments, and outcome measures did exist among the included studies; and (4) the size of this meta-analysis is small, and thus its power is limited. Taken together, the effect size of benefit with SUP may have been biased toward a larger effect.
All-cause mortality
Stress-related UGI bleeding has been shown to be a strong predictor of mortality in critically ill patients, which is associated with a mortality rate of 50–77 % and is as much as four times higher than that of patients without UGI bleeding [37]. Our pooled analysis of all-cause mortality showed a benefit of SUP in neurocritical care patients, and the robustness of the findings was confirmed by the sensitivity analyses. Despite these observations, however, it is still elusive whether stress-related UGI bleeding is a contributing cause of mortality or simply a marker of disease severity. Because the median duration of follow-up for mortality was only 20 days, the long-term outcome of patients who may or may not have benefited from SUP is unknown. Additionally, a genuine benefit of SUP on mortality might be questioned concerning the similar bias that existed in the analysis of UGI bleeding.
Nosocomial pneumonia
One of the proposed complications of SUP is an increased vulnerability to nosocomial pneumonia. However, we could not find any benefit or harm of SUP on the risk of nosocomial pneumonia. The overall higher risk of bias of the trials and sparse data warrant cautious interpretation of the results. Though not significant, as shown by subgroup analyses, between-trial heterogeneity was observed, which is possibly due to (1) clinical variability in participants, interventions, and control treatments; (2) unclear or inconsistent definitions of nosocomial pneumonia [14–16, 22]; and (3) inherent bias associated with adverse effect outcomes in RCTs, as they are not always foreseeable and may not have been adequately addressed in the original studies [24].
Protocol deviations
There are a few protocol deviations in this meta-analysis compared with the original published protocol in PROSPERO. We did not perform Egger’s test and meta-regression, because there were fewer than ten trials included and in that case the statistical power of these tests is very confined [24]. We included a trial conducted in a non-ICU setting with perioperative critically ill patients [22], and to explore the impact of this protocol deviation we performed a sensitivity analysis by excluding this trial. Although the intention is that a meta-analysis should adhere to the published protocol, changes in protocol are sometimes necessary to adapt to unanticipated circumstances, such as problems with participant recruitment, data collection, and unexpected event rates.
Relationship to other reviews
Recent systematic reviews with meta-analyses indicated a benefit of PPIs over H2RAs in reducing the risk of UGI bleeding without affecting the risk of nosocomial pneumonia, death, or ICU length of stay for general critical care patients [8, 9]. However, the authors of these reviews have overlooked one important question: whether SUP with PPIs or H2RA has any benefit over placebo or no prophylaxis. There is a possibility that even though PPIs are better than H2RAs, neither may be better than placebo or no prophylaxis. In that case, the conclusions of the superior effects of PPIs may be of limited or no clinical significance.
Indeed, the authors of one recent systemic review using meta-analysis and trial sequential analysis questioned this issue by assessing the efficacy and safety of SUP versus placebo or no prophylaxis in general critical care patients [5]. The results revealed that SUP with PPIs or H2RAs was not statistically significantly different from placebo or no prophylaxis in terms of mortality, GI bleeding, and pneumonia. Yet, our results support the effectiveness and safety of SUP with PPIs or H2RAs in reducing the morbidity and mortality of stress-related UGI bleeding in neurocritical care patients. The difference could be attributed to three factors. First and foremost, the trial eligibility criteria varied significantly between the two reviews. Krag et al.’s [5] review included critically ill patients from medical, surgical, and mixed ICUs with various primary diagnoses and different disease states and severity. In contrast, our review included only neurocritical care patients with primary pathologies, all of which were related to CNS and comparable risks, and these patients were in general at greater risk for stress-related UGI bleeding and associated complications, as discussed above. Second, owing to the update of RCTs on SUP in critical ill patients, we included three recently published trial results [15, 16, 28] not included in Krag et al.’s review [5]. In addition, we included a trial conducted in a non-ICU setting that consisted of critically ill patients with acute and severe neurological injuries who underwent emergency neurosurgery and were under critical care perioperatively. This trial was excluded from Krag et al.’s review simply because it was not in an ICU setting; however, we decided to include it based on the evaluation of the characteristics of the patients and the actual level of care they received. Third, the statistical methods used were different. We did not perform a trial sequential analysis to challenge the meta-analysis, partially because an anticipated RR reduction of 20 % for intervention effect with an event proportion of 21 % in the control arm is somewhat too rigorous. However, the lack of a trial sequential analysis may limit the robustness of our results.
Strengths and limitations of the review
The robustness of our findings is supported by general compliance with the recommendations of the Cochrane Collaboration for intervention reviews for RCTs, despite some necessary adaptations customized to the present topic.
However, our meta-analysis also has many limitations, such as the clinical and methodological heterogeneity, protocol deviations, sparse data, and concerns regarding small trial bias. Thus, the generalizability of the results may be compromised. In addition, our findings should not necessarily be applied to patients undergoing elective neurosurgical procedures, because these patients were not included in our analysis.
Implications for future practice and research
The meta-analysis encouraged the use of SUP in neurocritical care patients by providing evidence that SUP with PPIs or H2RAs yields a reduction in stress-related UGI bleeding and all-cause mortality and does not increase the risk of nosocomial pneumonia compared with placebo or no prophylaxis. Recommendations in current guidelines that advocate SUP for patients with high risk of stress-related UGI bleeding [3, 4] are supported by this meta-analysis. However, there are no clear recommendations on the monitoring and discontinuation of SUP in critical ill patients to date, and this needs to be addressed in future investigations.
The overall high or unclear risk of bias of the trials and sparse data in this meta-analysis highlight the lack of firm evidence for the benefits of SUP in neurocritical care patients. Larger, well-designed RCTs with low risk of bias are thus warranted for the safety and effective care of patients. In addition, among all neurocritical care patients, almost all RCTs have been targeted at patients with TBI and ICH; patients with other acute neurological conditions, such as ischemic stroke, spinal cord injury, and aneurysmal subarachnoid hemorrhage, should be taken into consideration.
Conclusions
This meta-analysis provides a comprehensive summary of available trial information for clinicians and guideline developers. Our results suggest that SUP, compared with placebo or no prophylaxis, may significantly lower the risk of UGI bleeding and all-cause mortality in neurocritical care patients without influencing the risk of nosocomial pneumonia. The robustness of this conclusion is limited by the lack of trials with low risk of bias, sparse data, heterogeneity among trials, and concern regarding small trial bias. Cost-effectiveness analysis and larger, well-designed RCTs are warranted among neurocritical care patients to allow firm conclusions to be drawn about the magnitude of the beneficial effect and its clinical relevance.
Key messages
-
Stress ulcer prophylaxis with proton pump inhibitors or histamine 2 receptor antagonists seems to be more effective than placebo or no prophylaxis in reducing the morbidity and mortality of stress-related upper gastrointestinal bleeding in neurocritical care patients.
-
Stress ulcer prophylaxis seems to reduce all-cause mortality while not increasing the risk of nosocomial pneumonia in neurocritical care patients.
-
The robustness of these conclusions is limited by the lack of trials with low risk of bias, sparse data, heterogeneity among trials, and concern regarding small trial bias.
Abbreviations
- AKI:
-
acute kidney injury
- ASHP:
-
American Society of Health-System Pharmacists
- AVM:
-
arteriovenous malfunction
- CI:
-
confidence interval
- CNS:
-
central nervous system
- CT:
-
computed tomography
- CVD:
-
cardiovascular disease
- EN:
-
enteral nutrition
- FOBT:
-
fecal occult blood test
- GCS:
-
Glasgow Coma Scale
- GI:
-
gastrointestinal
- GOBT:
-
gastric occult blood test
- H2RA:
-
histamine 2 receptor antagonist
- ICH:
-
intracerebral hemorrhage
- ICP:
-
intracranial pressure
- ICU:
-
intensive care unit
- IV:
-
intravenous
- MV:
-
mechanical ventilation
- NA:
-
not available
- NG:
-
nasogastric
- PO:
-
per os
- PPI:
-
proton pump inhibitor
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- PUD:
-
peptic ulcer disease
- RCT:
-
randomized controlled trial
- RR:
-
risk ratio/relative risk
- SUP:
-
stress ulcer prophylaxis
- TBI:
-
traumatic brain injury
- UGI:
-
upper gastrointestinal
References
Krag M, Perner A, Wetterslev J, Moller MH. Stress ulcer prophylaxis in the intensive care unit: is it indicated? A topical systematic review. Acta Anaesthesiol Scand. 2013;57(7):835–47.
Cook DJ, Fuller HD, Guyatt GH, Marshall JC, Leasa D, Hall R, et al. Risk factors for gastrointestinal bleeding in critically ill patients. N Engl J Med. 1994;330(6):377–81.
ASHP Therapeutic Guidelines on Stress Ulcer Prophylaxis. ASHP Commission on Therapeutics and approved by the ASHP Board of Directors on November 14, 1998. Am J Health Syst Pharm. 1999;56(4):347–79.
Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637.
Krag M, Perner A, Wetterslev J, Wise MP, Hylander Møller M. Stress ulcer prophylaxis versus placebo or no prophylaxis in critically ill patients: a systematic review of randomised clinical trials with meta-analysis and trial sequential analysis. Intensive Care Med. 2014;40(1):11–22.
Lin PC, Chang CH, Hsu PI, Tseng PL, Huang YB. The efficacy and safety of proton pump inhibitors vs histamine-2 receptor antagonists for stress ulcer bleeding prophylaxis among critical care patients: a meta-analysis. Crit Care Med. 2010;38(4):1197–205.
Marik PE, Vasu T, Hirani A, Pachinburavan M. Stress ulcer prophylaxis in the new millennium: a systematic review and meta-analysis. Crit Care Med. 2010;38(11):2222–8.
Alhazzani W, Alenezi F, Jaeschke RZ, Moayyedi P, Cook DJ. Proton pump inhibitors versus histamine 2 receptor antagonists for stress ulcer prophylaxis in critically ill patients: a systematic review and meta-analysis. Crit Care Med. 2013;41(3):693–705.
Barkun AN, Bardou M, Pham CQ, Martel M. Proton pump inhibitors vs. histamine 2 receptor antagonists for stress-related mucosal bleeding prophylaxis in critically ill patients: a meta-analysis. Am J Gastroenterol. 2012;107(4):507–21.
Kamada T, Fusamoto H, Kawano S, Noguchi M, Hiramatsu K. Gastrointestinal bleeding following head injury: a clinical study of 433 cases. J Trauma. 1977;17(1):44–7.
Reusser P, Gyr K, Scheidegger D, Buchmann B, Buser M, Zimmerli W. Prospective endoscopic study of stress erosions and ulcers in critically ill neurosurgical patients: current incidence and effect of acid-reducing prophylaxis. Crit Care Med. 1990;18(3):270–4.
Burgess P, Larson GM, Davidson P, Brown J, Metz CA. Effect of ranitidine on intragastric pH and stress-related upper gastrointestinal bleeding in patients with severe head injury. Dig Dis Sci. 1995;40(3):645–50.
Halloran LG, Zfass AM, Gayle WE, Wheeler CB, Miller JD. Prevention of acute gastrointestinal complications after severe head injury: a controlled trial of cimetidine prophylaxis. Am J Surg. 1980;139(1):44–8.
Metz CA, Livingston DH, Smith JS, Larson GM, Wilson TH, Larson GM, et al. Impact of multiple risk factors and ranitidine prophylaxis on the development of stress-related upper gastrointestinal bleeding: a prospective, multicenter, double-blind, randomized trial. Crit Care Med. 1993;21(12):1844–9.
Misra UK, Kalita J, Pandey S, Mandal SK, Srivastava M. A randomized placebo controlled trial of ranitidine versus sucralfate in patients with spontaneous intracerebral hemorrhage for prevention of gastric hemorrhage. J Neurol Sci. 2005;239(1):5–10.
Liu BL, Li B, Zhang X, Fei Z, Hu SJ, Lin W, et al. A randomized controlled study comparing omeprazole and cimetidine for the prophylaxis of stress-related upper gastrointestinal bleeding in patients with intracerebral hemorrhage. J Neurosurg. 2013;118(1):115–20.
O’Donnell MJ, Kapral MK, Fang J, Saposnik G, Eikelboom JW, Oczkowski W, et al. Gastrointestinal bleeding after acute ischemic stroke. Neurology. 2008;71(9):650–5.
Schaller BJ, Graf R, Jacobs AH. Pathophysiological changes of the gastrointestinal tract in ischemic stroke. Am J Gastroenterol. 2006;101(7):1655–65.
Hamidon BB, Raymond AA. The risk factors of gastrointestinal bleeding in acute ischaemic stroke. Med J Malaysia. 2006;61(3):288–91.
Fabian TC, Boucher BA, Croce MA, Kuhl DA, Janning SW, Coffey BC, et al. Pneumonia and stress ulceration in severely injured patients: A prospective evaluation of the effects of stress ulcer prophylaxis. Arch Surg. 1993;128(2):185–92.
Leramo OB, Tator CH, Hudson AR. Massive gastroduodenal hemorrhage and perforation in acute spinal cord injury. Surg Neurol. 1982;17(3):186–90.
Chan KH, Lai ECS, Tuen H, Ngan JHK, Mok F, Fan YW, et al. Prospective double-blind placebo-controlled randomized trial on the use of ranitidine in preventing postoperative gastroduodenal complications in high-risk neurosurgical patients. J Neurosurg. 1995;82(3):413–7.
Schirmer CM, Kornbluth J, Heilman CB, Bhardwaj A. Gastrointestinal prophylaxis in neurocritical care. Neurocrit Care. 2012;16(1):184–93.
Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions, version 5.1.0 [updated March 2011]. Oxford, UK: The Cochrane Collaboration; 2011.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Kramer AH, Roberts DJ, Zygun DA. Optimal glycemic control in neurocritical care patients: a systematic review and meta-analysis. Crit Care. 2012;16:R203.
Huang J, Cao Y, Liao C, Wu L, Gao F. Effect of histamine-2-receptor antagonists versus sucralfate on stress ulcer prophylaxis in mechanically ventilated patients: a meta-analysis of 10 randomized controlled trials. Crit Care. 2010;14:R194.
Zhang YH, Wu P, Wu S. [Combined use of GM1 with proton-pump inhibitors or H2-receptor antagonists for treatment of spontaneous intracerebral hemorrhage with upper digestive tract hemorrhage]. World Chin J Digestology. 2014;22(26):3958–62. Chinese.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Wood L, Egger M, Gluud LL, Schulz KF, Juni P, Altman DG, et al. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: meta-epidemiological study. BMJ. 2008;336(7644):601–5.
Krogsbøll LT, Hróbjartsson A, Gøtzsche PC. Spontaneous improvement in randomised clinical trials: meta-analysis of three-armed trials comparing no treatment, placebo and active intervention. BMC Med Res Methodol. 2009;9:1.
Leontiadis GI, Sharma VK, Howden CW. Proton pump inhibitor treatment for acute peptic ulcer bleeding. Cochrane Database Syst Rev. 2006;1:CD002094.
Hartling L, Hamm MP, Milne A, Vandermeer B, Santaguida PL, Ansari M, et al. Testing the risk of bias tool showed low reliability between individual reviewers and across consensus assessments of reviewer pairs. J Clin Epidemiol. 2013;66(9):973–81.
Hernandez DE. Neuroendocrine mechanisms of stress ulceration: focus on thyrotropin-releasing hormone (TRH). Life Sci. 1986;39(4):279–96.
Yang YX, Lewis JD. Prevention and treatment of stress ulcers in critically ill patients. Semin Gastrointest Dis. 2003;14(1):11–9.
Cushing H. Peptic ulcer and the interbrain. Surg Gynecol Obstet. 1932;55:1–34.
Sesler JM. Stress-related mucosal disease in the intensive care unit: an update on prophylaxis. AACN Adv Crit Care. 2007;18(2):119–28.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors made substantial contributions to the study conception and design, acquisition of data, or analysis and interpretation of data. All authors reviewed the protocol before study initiation. BL and SL performed the background literature review, literature search, study selection, and critical appraisal of the studies and were primarily responsible for drafting the manuscript. BL and AY performed the statistical analysis and interpretation of data. JS conceived of the study, participated in its design and coordination, provided close guidance throughout the process, and helped to draft the manuscript. All authors read and approved the final manuscript.
Bolin Liu, Shujuan Liu and Anan Yin contributed equally to this work.
Additional files
Additional file 1:
Appendix. (DOCX 106 kb)
Additional file 2:
Risk of bias table. (DOCX 109 kb)
Additional file 3: Figure S1.
Funnel plot: UGI bleeding. (EPS 81 kb)
Additional file 4: Figure S2.
Funnel plot: all-cause mortality. (EPS 81 kb)
Additional file 5: Figure S3.
Funnel plot: nosocomial pneumonia. (EPS 84 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Liu, B., Liu, S., Yin, A. et al. Risks and benefits of stress ulcer prophylaxis in adult neurocritical care patients: a systematic review and meta-analysis of randomized controlled trials. Crit Care 19, 409 (2015). https://doi.org/10.1186/s13054-015-1107-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-015-1107-2