
Abstract
Background
The five-year overall survival (OS) of advanced-stage ovarian cancer remains nearly 25-35%, although several treatment strategies have evolved to get better outcomes. A considerable amount of heterogeneity and complexity has been seen in ovarian cancer. This study aimed to establish gene signatures that can be used in better prognosis through risk prediction outcome for the survival of ovarian cancer patients. Different studies’ heterogeneity into a single platform is presented to explore the penetrating genes for poor or better survival. The integrative analysis of multiple data sets was done to determine the genes that influence poor or better survival. A total of 6 independent data sets was considered. The Cox Proportional Hazard model was used to obtain significant genes that had an impact on ovarian cancer patients. The gene signatures were prepared by splitting the over-expressed and under-expressed genes parallelly by the variable selection technique. The data visualisation techniques were prepared to predict the overall survival, and it could support the therapeutic regime.
Results
We preferred to select 20 genes in each data set as upregulated and downregulated. Irrespective of the selection of multiple genes, not even a single gene was found common among data sets for the survival of ovarian cancer patients. However, the same analytical approach adopted. The chord plot was presented to make a comprehensive understanding of the outcome.
Conclusions
This study helps us to understand the results obtained from different studies. It shows the impact of the heterogeneity from one study to another. It shows the requirement of integrated studies to make a holistic view of the gene signature for ovarian cancer survival.
Similar content being viewed by others


Background
Several treatment strategies evolved to make the outcome of ovarian cancer better [1]. But the five-year overall survival (OS) of the advanced stage of the disease remains nearly 25-35% [2]. A considerable amount of heterogeneity and complexity has been seen in ovarian cancer (OC) [3]. Genetic alterations (BRCA gene mutations, DNA damage, TP53 mutations, chromosomal instability) and alterations in RNA and miRNA expression characterised the high grade serous ovarian cancer (HGSOC) [4]. Simultaneously, genes such as TRIM44 and CENPK [5] were identified, and these were significantly associated with the prognosis of ovarian cancer patients. However, only a few prognostic signatures have been developed [5]. Hence, there was a need to study the disparities among different studies and accumulate that in a single platform to understand the penetrating genes for poor or better survival of ovarian cancer patients.
The predicting tool needs to be robust and flexible to accommodate gene signature and provides treatment outcomes. Individual-level risk prediction score generated by the rigorous statistical model always served the purpose. It was not only about the model development; moreover, the statistical model compatible with suitable data fulfilled the mission. Omics data only support individual-level risk score prediction or personalised medicine by coupling with survival outcomes. So the survival outcome and omic data come together to support the personalised medicine and generate the individual-level risk score. Omic data were having several thousand gene expression defined as high dimensional data. The joint work of survival data and high dimensional data is not new [6]. There are several challenges in high-dimensional data [7], where many of the problems were solved, and many of them were not. Separately, survival analysis challenged with different methodology [8].
Mostly oncology domain presented with follow-up observations like recurrence, response and death. The time-to-occurrence of the event plays a crucial role in this direction.
This work is prepared by applying the risk prediction model in the survival - high dimensional ovarian cancer data.
The Cox proportional hazards (PH) regression model is defined as
where h(t) is defined as the hazard function, (t) appear for the survival time, X is the covariate vector, the coefficient β measures the impact which is effect size and the h0(t) is known as the baseline hazard [9].
When there are multiple coefficients and covariates,
the quantities of exp(β) are called as the hazard ratios, and here a value of βi greater than zero or the hazard ratio greater than one depicts that the value of the ith covariate will increase and overall the event hazard will increase and thus the survival length will decrease.
It was anticipated that while the initial treatment was given, a patient may be no longer censored. The dimension reduction was the common challenge to work with high dimensional data, and it was not easy to obtain any unique, robust estimator [10]. The dimensional reduction has been extended in this line as the linear models [11]. The most widely used methods are linear and ridge regression model. By reducing the dimension, it becomes compatible with a penalised estimator of the Lasso. However, it was not stable for a large number of variables in microarray data [12]. The survival modelling with high-dimensional covariates becomes complicated. It required to look first about clustering the gene expression data and looks at clustered data by the Cox PH model.
Recently gene signatures have been commonly adopted for cancer patients. It helps to determine the best therapy in the context of personalised medicine [13], and it was confirmed by the clinically validating procedure [14]. Over the years, the selection of gene signature and further adoption in cancer prediction took a lead role in cancer research. However, it was challenging to identify the reliable gene signature due to variable selection challenges. Commonly the selected gene signature was found inconsistent from study to study [15]. Because the model used to select gene signature from one study also varies from others [15]. It raised the contradictory outcomes between the studies [13]. This signature was concerned with the reliability and benefits of using it as reliable for clinical practice.
Several environmental factors may influence the study. Given the relatively small sample size, conclusions were preliminary lacked due to power and generated with less accuracy of prediction [15]. Sometimes, the prevalence of the clinical outcome also reduced the replicability [16].
Recent studies showed that due to the low frequencies of some molecular types become inappropriate to predict for the new patients correctly. It would be worth testing how well the method performs in different laboratories. The laboratory wise variation in gene signature accuracy prediction was observed.
Data processing technique also play a crucial role to obtain different outcomes. Particularly, the normalization steps for data processing was crucial [16].
It required to create of the training data set before validation. Perhaps, result bias also generated due to the small sample size.
It could happen in some situations and thus requires a more detailed look on the microarray chip [17].
It becomes challenging to maintain consistency if the new study performs into a new platform to boost up the prediction capacity. The gene expression measured by next-generation sequencing was different “from microarray measurements. It needs to derive a methodology from boosting up the clinical prediction capacity for a specific platform.
Different statistical methods have been developed to integrate data from different studies towards agreement on a conclusion where the horizontal integration was useful for a conclusive remark [18].
This study aimed to establish a gene signature which can be helpful in better prognosis through risk prediction model in the high dimensional-survival ovarian cancer data obtained from the NCBI’s Gene Expression Omnibus database (https://www.ncbi.nlm.nih.gov.in/geo/).
Methods
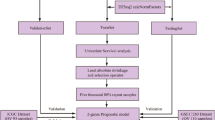
A total of 6 high dimensional-survival ovarian cancer data sets was obtained to understand the gene expression and the process followed by them, to conclude for better prognosis through a risk prediction model. An integrative approach of multiple data sets was made to find out the gene to make the influence of poor/better survival by considering different data sets. The Cox PH model was used to obtain significant genes that had an impact on ovarian cancer patients, emphasising the importance of the effect size. The gene signatures were prepared by splitting over-expressed and under-expressed genes together after the gene selection. The chord plot data visualisation technique was used to formalise the recommendations for routine clinical practice. The data visualisation techniques were prepared to predict the overall survival, and it could support the therapeutic regime.
Identification of differentially expressed genes in ovarian Cancer
In this study, data was retrieved about gene expression from studies conducted on the NCBI’s Gene Expression Omnibus database (https://www.ncbi.nlm.nih.gov.in/geo/) to identify relevant data sets which contain the gene profile of ovarian cancer. Data sets with accession number GSE14764, 22283 probes ID of 80 patients [19]; accession number GSE17260, 41000 probes ID of 110 patients [20]; accession number GSE19829, 12558 probes ID of 42 patients [21]; accession number GSE30161, 54613 probes ID of 58 patients [22]; accession number GSE49997, 32878 probes ID of 194 patients [23] and accession number GSE63885, 54613 probes ID of 75 patients [24] were chosen for the study.
Genes selection
The data sets were filtered with p-value < 0.05 by univariate Cox PH model. A number of probes were selected, and the VIMP function in the ‘party’ package in R was used to obtain the most significant probes. The correlated genes were separated by VIMP function in R. The hazard ratio (HR), and confidence intervals were considered to select the probes. Later, the positive probes having HR > 1 and negative probes having HR < 1 were selected to create the adjacency matrix. The adjacency matrix was generated from the positive and negative probes, which was used to create the chord plot (a circular visualisation to show relations between genes by links).
Data set obtained from the Gene Expression Omnibus (GEO) database under the accession number GSE14764. It consisted of 22,283 probes of 80 patients. Initially, the data set was filtered with p-value < 0.05 by univariate Cox PH model, where a total of 531 probes were selected. The VIMP function obtained the most significant 100 probes. The correlated genes were separated by the VIMP function. The HR and confidence intervals were considered to select 100 probes.
In the next step, the positive probes having HR > 1 and negative probes having HR < 1 were selected for the adjacency matrix. The adjacency matrix of 10 *10 was generated from the positive and negative probes, which was used to create the chord plot. A similar approach was used for all the data sets.
Generating global p-value
Suppose n number of univariate statistical tests were performed. The statistics obtained from each step were presented as Xi. Now, n number of the statistical test will generate X1, X2, ……Xn. The statistics was presented as vector \(\overline{X}=\left({X}_1,{X}_{2,\dots \dots }{X}_n\right)\). The statistics obtained from each test followed certain distribution as \(\overline{X}\) presented a random variable. The P-value obtained for each step of the test defined as pi. The minimum P value of all the test was presented as mini(pi). This similar set up works in multivariate analysis. In our situation, a total of 20 genes were selected by the univariate Cox PH model. The set of genes further determined in the multivariate set up to create mini(pi).
The mini(pi) was presented as a global P-value, which is given in Fig. 1. Global significance level pmin associated with the single experiment-wise statistic was obtained from the proportion of values at least as small as the observed mini(pi) .If pmin < = 0.05 then the experiment (at least one of the steps in the clustering process) was significant at the 5\% level [25] (Fig. 2).

Forest Plot and Chord Plot for overexpressed and underexpressed genes obtained on GSE14764

Forest Plot and Chord Plot for overexpressed and underexpressed genes obtained on GSE14764
Clustering effect
To assess the benefits of clustering, we compared the statistical significance for the entire experiment, which involved the tests at each step created by clustering; that is, we compared the global p-value, pmin, with the significance level, p0, of the statistic prior to clustering. When pmin < p0, the results were more significant, and the clustering was beneficial. But if pmin > p0 then the smallest p-value has a high probability of occurring by chance.
In our study, the ‘ggforest’ function was used with the survminer package for the preparation of the Forest Plot for the Cox PH model. For instance, the Gene Expression Omnibus (GEO) database under the accession number GSE14764 consists of 22,283 probes, and 80 patients and the univariate data analysis were performed. However, all the significant genes showed a non-significant p-value. But, the overall p-value obtained by the Global p-value observed with the highly significant p-value.
Genes links by data visualisation
The circular visualisation method was used to show the relations between genes by links by the chord plots. The “circlize” package in R software was used, and the Chord diagram was formed in a straight forward and highly customised way. For creating the chord diagrams, we first computed a concordance matrix for each dataset. The row and column names of each matrix contained the result as upregulated and down-regulated genes leading to death. Each concordance cell was assigned a value as 0, 1, or 2 by calculating risk towards death due to the respective high values of upregulated and low values of down-regulated genes. Proportions of risk were partitioned as < 25%, more significant than 25 and < 50%, > 50%.
Chord plot showed that the links were straight forward to show the relations between genes (Fig. 2). The width of the links was also observed as proportional to the strength of the relation. The colours of links provided the visual linkage among the genes. The width of sectors represents total strength for the gene, which connects to other gene or was connected from other genes. The forest plot and chord plot for overexpressed and under-expressed genes obtained on GSE14764 consisting of 22,283 probes and 80 patients were done for obtaining the global p-value, and similar plots for additional 5 data sets was done.
Results
As shown in the Table 1, a total of 20 genes from each data sets was selected. With the statistical analysis, we were able to found out the upregulated and down-regulated genes that showed up with the hazard ration (HR) and the p-value. In this study, the results obtained describes that the upregulated genes with the HR > 1 are making difficulties for survival and the down-regulated genes with the hazard ratio HR < 1.
The results obtained on GSE14764, the genes obtained were ARCN1, UBR5, MTMR2, TAT1, IFNA1, BCR, DYNLT3, GTPBP1, SEMA3E and PAX9, which were upregulated genes and ANAPC5, RPL13A, KDM2A, EDA, TWISTNB, CCL1, BAI1, LSM6, PRMT2 and SHOX2 were down-regulated genes. The genes were ranked based on their HR and Confidence Intervals. The expression of SEMA3 family members was frequently associated with overall patient survival. SEMA3E primarily associated with a poor prognosis of survival. Results reveal an undiscovered role of SEMA3E in promoting pancreatic cancer pathogenesis, suggesting that SEMA3E as a suitable prognostic marker and therapeutic target for pancreatic cancer [26]. PAX9 an independent prognostic factor for the surgical treatment of ESCC and a possible predictor of radiation sensitivity [27]. MTMR2 an essential promoter in gastric cancer invasion and metastasis by inactivating IFNA1/STAT1 signalling and acts as a new prognostic indicator and a potential therapeutic target for gastric cancer [28].
UBR5 a key regulator of cell signalling relevant to broad areas of cancer biology [29]. DYNLT3 exerts pro-tumoral effects on Ovarian cancer through promoting cell proliferation, migration and invasion. DYNLT3 a potential prognostic predictor in ovarian cancer [30]. GTPBP1, a regulator and adaptor of the exosome-mediated mRNA turnover pathway [31]. CCL1 significantly correlated with the infiltration of immunosuppressive FoxP3+ Treg that were known to negatively affect survival negatively. Thus, CCL1 serves as a prognostic marker and novel therapeutic target in breast cancer [32]. High KDM2A levels were correlated with poor prognosis in NSCLC patients. They were suggesting that KDM2A may be a promising therapeutic target in NSCLC [33]. PR (PRDI-BFI and RIZ) domain-containing (PRDM) proteins have been shown to be important in several types of human cancer [34]. RPL13A, the most suitable reference gene for analysing the transcription profile of ovarian cancer cells following treatment with PTX and HCPT [35]. Levels of BAI1 mRNA steadily downregulated in cells lines, primary glioma specimens and from lung adenocarcinoma in brain metastases [36]. PRMT2 were significantly high in malignant breast tissues than in normal tissues of breast [37].
Genes under data set GSE17260 were grouped YWHAB, SEC22B, EIF3J, MMP1, BNIP2, FAM126B, DTWD1, CU674465, TBC1D15 and PHF20 as upregulated, and down-regulated genes were ZNF341, PRR3, TBXA2R, OPALIN, SERINC5, AQP10, FAM95B1, MIDN, RABL2A and NKPD1. The gene YWHAE was found associated with tumour size, lymph node metastasis, and poor patient survival in patients with breast cancer [38]. SEC22B was observed closely related to tumorigenesis with types of mutation. The gene fusion of SEC22B confirmed in aggressive breast cancers and mantle cell lymphoma [39]. EIF3J-AS1 gene was found correlated with prognostic features, including tumour size, vascular invasion and tumour stage, which takes crucial expert roles in hepatocellular carcinoma (HCC) progression [40]. High MMP1 expression associates with worse OS in breast cancer patients after systematic therapy [41].
In the case of Cancer epigenetics, DTWD1 was down-regulated in gastric cancer cell lines and primary gastric carcinoma tissues. DTWD1 functions as a tumour suppressor play an important role in the pathogenesis of many cancers, including gastric cancer [42]. The stimulator of IFN genes mediated DNA sensing pathway plays an important role in the innate immune response to pathogen infection, autoimmunity, and cancer, which was regulated by TBC1D15, mitochondrial dynamics mediators [43]. Plant homeodomain finger protein 20 (PHF20) was highly expressed in primary human gliomas, and its expression was found to be associated with tumour grade, which relates to glioblastoma [44]. There was an increase in overall cancer incidence among patients with primary immunodeficiencies of ZNF341 [45]. Thromboxane synthases were differentially expressed in human breast cancer. TBXA2R thus has a significant prognostic value in clinical breast cancer [46]. FAM95B1 significantly correlates with cervical lymph node metastasis. Cervical lymph node metastasis was an important prognostic indicator for papillary thyroid carcinoma (PTC) and affects treatment strategies (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6388952/) and tumour staging.
On analysis of GSE18929, genes such as Hsp40, HELZ, STX3, FTL, NPC1, PMM1, TPP1, RBL2, CREG1 and AKAP11 were upregulated genes, and the down-regulated genes were ANAPC15, MANF, BAX, CDC34, IL23A, NCL, PEX10, PHGDH, DNPH1 and SSNA1. Hsp40 was the probes in cancerous lung tissues; it was also shown that levels of Hsp40 increased in the serum of cancer patients [47]. The roles of Syntaxin 3(STX3) acts as an oncogenic protein in human breast cancer [48]. Ferritin Light Chain (FTL) completes with long noncoding RNA to regulate chemoresistance and metastasis of colorectal cancer, which was a leading cause of cancer deaths [49]. NPC1 family of proteins plays an essential role in molecular mechanisms in breast cancer cells which was associated with constitutive activation of autophagy [50]. Expressed gene PMM1, located on chromosome bands, helps differentiate gene expression before and after radiation of subcutaneous fibroblasts, identifying breast cancer patients resistant to radiation-induced fibrosis [51]. A rare variant of TPP1 confers an increased risk of colorectal cancer through interrupting TPP1-TIN2 interaction [52]. RBL2/p130, a member of the retinoblastoma family of proteins, a well-known tumour suppressor gene in the Rb family, found inactivated in numerous cancers, has growth-suppressive properties and also deregulates in various types of cancer, especially in Pancreatic adenocarcinoma (PDAC), one of the most aggressive malignancies in humans [53].
CREG1, the cellular repressor of E1A-stimulated genes, a downstream effector of KRAS which identifies in Glycoproteomic Approach as a positive regulator of CREG1 in Non-small Cell Lung Cancer Cells [54]. The AKAP gene was related to tumour heterogeneity in breast cancer tumours which relates to the primary tumour [55]. The adenomatous polyposis coli (APC) play a rate-limiting role in the majority of sporadic colorectal cancers. Loss of APC function triggers the chain of molecular and histological changes [56]. MANF levels were associated with the status of liver cirrhosis, advanced tumour-node-metastasis (TNM) stage, and tumour size [57]. Frameshift mutations were seen present in both BAX alleles in some MMP+ colon tumour cell lines and in primary tumours. Inactivating BAX mutations during the progression of colorectal MMP+ tumours and the wild-type BAX gene plays a suppressor role in a p53-independent pathway for colorectal carcinogenesis [58]. CDC34 changes expressions of Proteasome and Ubiquitin Genes in Human Renal Cancer Cells (https://cancerres.aacrjournals.org/content/51/24/6677.short). NCL was commonly overexpressed in human breast tumours, and it was expression correlates with NCL dependent miRNAs [59]. Phosphoglycerate dehydrogenase (PHGDH) plays an essential role in cancer-specific metabolic reprogramming [60]. The crystal structure of rat DNPH1, a potential target for anti-cancer therapies, suggested that various analogues of AMP can inhibit this enzyme [61].
Results obtained on GSE30161 were grouped CDHR3, STK25, NADK2, HELQ, USF3, HKR1, MAGOH, TLE4, TRIO and POSTN as upregulated, and the down-regulated genes were WNT16, CYP2E1, CAPN3, EP400, CIB2, DUSP4, ZDHHC2, CCT6B, LOC101929607 and FOXJ1. The glutamine-dependent survival and sensitivity to ER stress in USF3-deficient cells provided adjunct preventive interventions for both sporadic cancers as well as cancer predisposition syndromes [62]. HKR1 mRNA expression levels in lung cancers were higher, and that high expression levels in lung cancers were found to be associated with antemortem platinum drug administration [63]. MAGOHB, the top gene dependency in cells with hemizygous MAGOH deletion. MAGOH and MAGOHB as reciprocal paralog dependencies across cancer types suggest a rationale for targeting the MAGOHB-IPO13 axis in cancers [64]. TLE4 promote colorectal cancer progression through activation of the signalling pathway. TLE4 in colorectal cancer (CRC) tissues were significantly higher than that in their matched adjacent intestine epithelial tissues. TRIO gene promotes Colorectal Cancer Invasion and Metastasis. TRIO pY2681, one of the downstream effectors in colorectal cancer and can be a prognostic marker, helping to determine the therapeutic modality of patients with colorectal cancer [65].
The vascular endothelial growth factor was found to be a significant regulator of breast cancer angiogenesis, the effects of which were transmitted through the kinase domain receptor (KDR). Up-regulation of KDR by periostin (POSTN) induces angiogenesis which was an important step in the development of cancer [66]. Gastric cancer was a multi-step, multi-factor, and elaborated process that was associated with gene abnormal gene expression. Great significant modification occurred in tumoral tissues, and the gene expression increased significantly in tumoral tissue observed due to upregulation of WNTt16 gene expression in gastric cancer, which was one of the most severe and lethal kinds of cancer in the world [67]. Investigation of the association between cancer development risk and cytochrome P4502E1 (CYP2E1) gene polymorphism was significant [68]. A novel fusion gene, EP400-PHF1, was discovered in ossifying fibromyxoid tumour; its relation to this type of tumour has been uncertain because the EP400-PHF1 fusion gene has been successfully detected in only 1 case [69]. CIB2, significantly down-regulated in ovarian cancer, and low CIB2 expression was associated with poor prognosis in ovarian cancer patients [70]. Dual-specificity protein phosphatase 4 (DUSP4), a negative regulator of extracellular-regulated kinase activity, was a potential mediator of resistance to chemotherapy and a tumour suppressor. Clarification was done for the association between DUSP4 gene expression and clinical outcome in patients with colorectal cancer [71]. Zinc finger, DHHC-type containing 2 (ZDHHC2), proposed as a putative tumour/metastasis suppressor gene and was often aberrantly decreased in human cancers. ZDHHC2 expression pattern and its clinical significance have not yet been investigated in gastric adenocarcinoma [72]. Forkhead box (FOX) proteins were a large family of transcriptional regulators, which control a variety of biological processes leading to alteration of cell fate. Thus, the development and progression of ovarian cancer, which was the most lethal of all gynaecological malignancies, and the Identification of novel prognostic and therapeutic targets for ovarian cancer was crucial. As four FOX proteins, including FOXO1, FOXO3a, FOXJ1 and FOXB1, were the likely targets of NANOG in embryonic stem cells [73].
On thorough analysis of GSE49997, we found LTBP2, ACTA2, WBP4, LOC283241, CYB561D2, CTSK, NAP1L5, DCN, ZBTB7 KIF1A were the upregulated genes, and down-regulated genes were COL16A1, RFX4, RPP38, BCR, ADRA1D, TTN, ZEB2, CDH1, KLC2 and FAP. The resulting genes were not exceptional as they have been previously termed as less or more effective in cancer oncology. The genes which were being termed as an essential marker for significant prognosis of cervical cancer were ADRA1D, LTBP2 whereas KLC2 protein-protein was termed for poor prognosis in early NsCLC patients [74]. RFX4 was considered as a target for GMB treatment. As a result, it depicts to be a risk factor for stemness of GSCs and malignance of Flioma. On comparing the lower express ZBTB7 with the higher, which exhibited lower overall and recurrence-free survival, hence ZBTB7 may be necessary for the initiation and progression of TCC (Urothelial carcinoma, also known as transitional cell carcinoma) [75]. ACTA2 can be considered as a prognostic biomarker and therapeutic target for metastatic lung cancer [76]. CTSK, in the case of ovarian cancer, shows association with metastases and inferior overall prognosis of EOC (Epithelial ovarian cancer) [77].
NAP1L1 was overexpressed while promoting the proliferation of p57 promoter Methylation. Cervical cancer has been seen initiated and progressed by an oncogene COL6A1. It was leading to a poor prognosis of cervical cancer [78]. TTN-AS1 paves a path for new treatment strategies in Cervical cancer patients, and it shows a significant correlation with FIGO stage, poor differentiation, lymph node metastasis and poor overall survival of CC patients [79]. Upregulated Zeb2 has an association with the progression of cancer. It was found to be relatively higher in colon cancer cell lines but seen reduced in healthy human colonic epithelial cell lines [80]. CDH1 shows the correlation with cervical cancer carcinogenesis as well as histological subtypes [81]. HGSOC, the most common and lethal form of ovarian cancer, Upregulation of FAP was found in advanced stage HGSOC patients, showing association with poor prognosis via FN1 pathway, the association of FAP network shows FN1 can be a potential downstream gene leading to HGSOC survival [82]. Whereas downregulation of STK25 triggers a mechanism by which tumour cells functionally impair the hippo tumour tumour-suppressor pathway [83].
Results obtained on GSE63885 were grouped OR7C1, ZSWIM1, PITPNA, DLL3, LOC92249, CLASP1, MBNL1, C21orf84, GP2 and C19orf20 as upregulated genes and downregulated genes were DGCR8, MMP1, GOLGA8G, CCNE1, ADK, BCL2L12, LOC149478, SPPL2B, PTPN2, SRP72. The genes were ranked based on their HR and Confidence Intervals.OR7C1, a novel marker for colon CICs and a target of potent CIC-targeting immunotherapy [84]. `The activation sensitive nature of ZSWIM1 expression shows that it plays a novel role in the development or function of T helper cells, which primarily mediate anti-tumour immunity [85]. A therapeutic strategy for the treatment of cancer could be idealised on targeting the PITPNA-AS1-associated signalling, which mediates the effects of c-MET on the proliferation, apoptosis and cell cycle in cervical cancer cells [86]. DLL3 localised to the plasma membrane of tumour cells and acted as a reliable biomarker to predict cancer progression and a poor clinical outcome. Pre- and clinical trial results indicated that membrane DLL3, a potential target for preventing tumour growth [87].
Endothelial cell (EC) branching was critically dependent upon the dynamic nature of the microtubule (MT) cytoskeleton. CLASP1 knockdown results were significantly faster and longer-lived MT growth specifically within EC branches, and thereby identify CLASP1 as a critical regulator of MT dynamics within EC branches. MLL-rearranged signatures revealed that muscleblind-like 1 (MBNL1) was one of the most consistently overexpressed genes in MLL-rearranged leukaemia compared to other leukaemias [88]. Mediated by miR-27b, DGCR8 functions as oncogene in Ovarian cancer [89]. MMP-1, differentially regulated in breast cancer tissues and served a role in breast cancer invasion and metastasis. Hence, it was considered as a diagnostic marker and drug target for breast cancer [90]. CCNE1 gene was targeted by miR-16-1 in Cervical Cancer cells [91]. BCL2L12 expression and stimulated proliferation and engrafting of leukaemia cells suggested CD82 and BCL2L12 as promising therapeutic targets in AML [92]. It was anticipated that the absence of SPPL2a/b critically affects disease-relevant pathways in the brain but also other organ systems when mice were challenged in a certain way [93]. PTPN21 overexpression was an early step in urothelial cancer progression. It was a novel biomarker and possible therapeutic target for bladder cancer [94]. SRP72, a novel gene involved in radio resistance [95].
Discussion
As of now, we have seen that ovarian cancer is the most common gynaecological oncological malignant tumour. It is the leading factor for the cause of death among women worldwide due to its late diagnosis and poor prognosis. Like any other cancer, it exhibits complexity and heterogeneity drug response and overall survival. Our investigation for the gene expression for ovarian cancer reveals that there were a number of upregulated and downregulated genes that were useful in disease diagnosis for an individual, as we have already mentioned about them earlier.
Ovarian carcinoma contributed to the highest mortality rate for any kind of gynaecological malignancies. It was investigated that the molecular markers can predict the death outcome of ovarian cancer independently along with clinical predictors [19]. In a study [20], it was shown that 110 patients from the Japanese population had advanced-stage serous ovarian cancer, where 93(84.5%) patients were in stage-III and rested in stage-IV. After having primary surgery, all the patients were treated with platinum/ taxane-based chemotherapy. The median duration of overall survival was found to be 31 months, and the total of 88-gene expression profile was found significant by ridge Cox proportional model. The clinical factors were explored in predicting cancer progression [20]. Furthermore, Jazaeri and Konstantinopolous in their studies showed about the gene expression profile of BRCAness, which was prepared from the publicly available microarray data set that included tumour expression data from 61 patients with pathologically confirmed EOC, including 34 with BRCA germline mutations (n = 18, BRCA1; n = 16, BRCA2), and 27 without either mutation (i.e., sporadic cancers). The hierarchical clustering was used to define the BRCA-like (BL) and non-BRCA-like (NBL)). Similar to our study, Ferris(2012) attempted the multi-gene molecular predictors to forecast the response of 55 ovarian cancer patients. They studied the overall survival and multi-gene molecular predictor. The predicted responders and the non-responders with a median survival of 55.4 months vs 32.1 months respectively showed a significant difference which was demonstrated by the combination predictors. Finally, it was concluded that the COXEN single and the combination was a drug predictor that successfully stratified the platinum resistance and taxane response in ovarian cancer [22].
In our study, we performed the overall survival and death as an outcome of interest to select the genes, whereas, in a study performed by Pils (2012), it was given that the RNA from the fresh frozen tumour was separated by ABI PRISM 6100 Nucleic Acid PrepStation (Applied Biosystems, Carlsbad, CA, USA). The correlation analysis of the clinicopathologic parameters was examined through chi-square test, t-test and Fisher’s exact test where the progression-free survival and overall survival; were measured. And, a total of 194 ovarian cancer patient’s clinic pathological and microarray data was selected to select the influencing genes on disease survival [23].
Conclusions
Ovarian cancer is the leading cause and adding to the disease burden all over the world. We discovered the expression of the number of genes to understand the effectiveness or harmfulness of those upregulated and down-regulated genes for the better prognosis of cancer. With the use of integrative data analysis, insight on the gene to make the influence of better survival was done. The results obtained with individual studies show little replicability, even with similar clinical outcomes. Study design and small sample size are critical limitations to deal with heterogeneity. The individual study may lead to low sensitivity because of the small sample size. The performance of sensitivity steadily decreases with an increase in heterogeneity of a gene effect. Besides, it was possible to combine multiple studies and improvise variable selection. It leads to higher prediction power by adopting power from different studies.
This study shows how to combine the effects of the same variable from the studies and make an impact on clinical prediction. The gene signature variability makes impacts on prediction. Besides, it was possible to combine the positive and negative genes and convert them into an adjacency matrix to prepare the chord plot, and that after processing the variable selection. Data obtained from multiple sources are subject to additional processing to obtain it in an equal platform. Finally, we provide applications on public domain data to select the gene signature. The achievement of the gene signature in the chord plot relies upon the over and under-expressed genes together.
Availability of data and materials
Data is publicly available.
References
Agarwal R, Kaye SB. Ovarian cancer: strategies for overcoming resistance to chemotherapy. Nat Rev Cancer. 2003;3(7):502–16.
Colombo P-E, Fabbro M, Theillet C, Bibeau F, Rouanet P, Ray-Coquard I. Sensitivity and resistance to treatment in the primary management of epithelial ovarian cancer. Crit Rev Oncol Hematol. 2014;89(2):207–16.
Kroeger PT Jr, Drapkin R. Pathogenesis and heterogeneity of ovarian cancer. Curr Opin Obstet Gynecol. 2017;29(1):26.
Network, T.: institution. participants are arranged by area of contribution and then by, sites d, bell d, berchucka, birrer m, chien j, cramer dw, dao f, dhir r, et al. Integrated genomic analyses of ovarian carcinoma. Nature. 2011;474:609–15.
Wang S, Jia M, He Z, Liu X-S. Apobec3b and apobec mutational signature as potential predictive markers for immunotherapy response in non-small cell lung cancer. Oncogene. 2018;37(29):3924–36.
Witten DM, Tibshirani R. Survival analysis with high-dimensional covariates. Stat Methods Med Res. 2010;19(1):29–51.
Johnstone IM, Titterington DM. Statistical challenges of high-dimensional data: The Royal Society Publishing; 2009. https://royalsocietypublishing.org/doi/full/10.1098/rsta.2009.0159.
Perera M, Dwivedi AK. Statistical issues and methods in designing and analyzing survival studies. Cancer Rep. 2020;3(4):1176.
Putter H, Fiocco M, Geskus RB. Tutorial in biostatistics: competing risks and multi-state models. Stat Med. 2007;26(11):2389–430.
Rosenwald A, Wright G, Chan WC, Connors JM, Campo E, Fisher RI, et al. The use of molecular profiling to predict survival after chemotherapy for diffuse large-b-cell lymphoma. N Engl J Med. 2002;346(25):1937–47.
Jolliffe IT. Principal components in regression analysis. Principal Component Anal. 2002:167–98. https://link.springer.com/book/10.1007/b98835.
Fan J, Li R. Variable selection via nonconcave penalized likelihood and its oracle properties. J Am Stat Assoc. 2001;96(456):1348–60.
Swisher EM, Taniguchi T, Karlan BY. Molecular scores to predict ovarian cancer outcomes: a worthy goal, but not ready for prime time; 2012.
Chibon F. Cancer gene expression signatures-the rise and fall? Eur J Cancer. 2013;49(8):2000–9.
Waldron L, Haibe-Kains B, Culhane AC, Riester M, Ding J, Wang XV, et al. Comparative meta-analysis of prognostic gene signatures for late-stage ovarian cancer. J Natl Cancer Inst. 2014;106(5).
Lusa L, McShane LM, Reid JF, De Cecco L, Ambrogi F, Biganzoli E, et al. Challenges in projecting clustering results across gene expression-proffling datasets. J Natl Cancer Inst. 2007;99(22):1715–23.
McCall MN, Bolstad BM, Irizarry RA. Frozen robust multiarray analysis (frma). Biostatistics. 2010;11(2):242–53.
Richardson S, Tseng GC, Sun W. Statistical methods in integrative genomics. Annu Rev Stat Appl. 2016;3:181–209.
Denkert C, Budczies J, Darb-Esfahani S, Györffy B, Sehouli J, Köonsgen D, et al. A prognostic gene expression index in ovarian cancer|validation across different independent data sets. J Pathol. 2009;218(2):273–80.
Yoshihara K, Tajima A, Yahata T, Kodama S, Fujiwara H, Suzuki M, et al. Gene expression proffle for predicting survival in advanced-stage serous ovarian cancer across two independent datasets. PLoS One. 2010;5(3):9615.
Jazaeri AA, Yee CJ, Sotiriou C, Brantley KR, Boyd J, Liu ET. Gene expression proffles of brca1-linked, brca2-linked, and sporadic ovarian cancers. J Natl Cancer Inst. 2002;94(13):990–1000.
Ferriss JS, Kim Y, Duska L, Birrer M, Levine DA, Moskaluk C, et al. Multi-gene expression predictors of single drug responses to adjuvant chemotherapy in ovarian carcinoma: predicting platinum resistance. PLoS One. 2012;7(2):30550.
Pils D, Hager G, Tong D, Aust S, Heinze G, Kohl M, et al. Validating the impact of a molecular subtype in ovarian cancer on outcomes: a study of the ovcad consortium. Cancer Sci. 2012;103(7):1334–41.
Lisowska KM, Olbryt M, Student S, Kujawa KA, Cortez AJ, Simek K, et al. Unsupervised analysis reveals two molecular subgroups of serous ovarian cancer with distinct gene expression proffles and survival. J Cancer Res Clin Oncol. 2016;142(6):1239–52.
Hoh J, Wille A, Ott J. Trimming, weighting, and grouping snps in human case-control association studies. Genome Res. 2001;11(12):2115–9.
Raposo TP, Susanti S, Ilyas M. Investigating tns4 in the colorectal tumor microenvironment using 3d spheroid models of invasion. Adv Biosyst. 2020;4(6):2000031.
Zhang L, Cao H, He T, Yang J, Tao H, Wang Y, et al. Overexpression of prdm13 inhibits glioma cells via rho and gtp enzyme activation protein. Int J Mol Med. 2018;42(2):966–74.
Wagner KW, Alam H, Dhar SS, Giri U, Li N, Wei Y, et al. Kdm2a promotes lung tumorigenesis by epigenetically enhancing erk1/2 signaling. J Clin Invest. 2013;123(12):5231–46.
Choo K-B, Huang C-J, Chen C-M, Han C-P, Au L-C. Jun-b oncogene aberrations in cervical cancer cell lines. Cancer Lett. 1995;93(2):249–53.
Kuehnemuth B, Piseddu I, Wiedemann GM, Lauseker M, Kuhn C, Hofmann S, et al. Ccl1 is a major regulatory t cell attracting factor in human breast cancer. BMC Cancer. 2018;18(1):1–6.
Woo K-C, Kim T-D, Lee K-H, Kim D-Y, Kim S, Lee H-R, et al. Modulation of exosome-mediated mrna turnover by interaction of gtp-binding protein 1 (gtpbp1) with its target mrnas. FASEB J. 2011;25(8):2757–69.
Zhou L, Ye M, Xue F, Lu E, Sun L-Z, Zhu X. Effects of dynein light chain tctex-type 3 on the biological behavior of ovarian cancer. Cancer Manag Res. 2019;11:5925.
Jiang L, Liu J-Y, Shi Y, Tang B, He T, Liu J-J, et al. Mtmr2 promotes invasion and metastasis of gastric cancer via inactivating ifn/stat1 signaling. J Exp Clin Cancer Res. 2019;38(1):1–16.
Tan B, Wang J, Song Q, Wang N, Jia Y, Wang C, et al. Prognostic value of pax9 in patients with esophageal squamous cell carcinoma and its prediction value to radiation sensitivity. Mol Med Rep. 2017;16(1):806–16.
Liang Y, Zeng D, You Y, Ma B, Li X, Chen T. Designing dihydrofolate reductase inhibitors as x-ray radiosensitizers to reverse radioresistance of cervical cancer. ACS Med Chem Lett. 2020;11(7):1421–8.
Kaur B, Brat DJ, Calkins CC, Van Meir EG. Brain angiogenesis inhibitor 1 is differentially expressed in normal brain and glioblastoma independently of p53 expression. Am J Pathol. 2003;162(1):19–27.
Zhong J, Cao R-X, Zu X-Y, Hong T, Yang J, Liu L, et al. Identification and characterization of novel spliced variants of prmt2 in breast carcinoma. FEBS J. 2012;279(2):316–35.
Yang Y-F, Lee Y-C, Wang Y-Y, Wang C-H, Hou M-F, Yuan S-SF. Ywhae promotes proliferation, metastasis, and chemoresistance in breast cancer cells. Kaohsiung J Med Sci. 2019;35(7):408–16.
Robinson DR, Kalyana-Sundaram S, Wu Y-M, Shankar S, Cao X, Ateeq B, et al. Functionally recurrent rearrangements of the mast kinase and notch gene families in breast cancer. Nat Med. 2011;17(12):1646–51.
Yang X, Yao B, Niu Y, Chen T, Mo H, Wang L, et al. Hypoxia-induced lncrna eif3j-as1 accelerates hepatocellular carcinoma progression via targeting mir-122-5p/ctnnd2 axis. Biochem Biophys Res Commun. 2019;518(2):239–45.
Shen C-J, Kuo Y-L, Chen C-C, Chen M-J, Cheng Y-M. Mmp1 expression is activated by slug and enhances multi-drug resistance (mdr) in breast cancer. PLoS One. 2017;12(3):0174487.
Ma Y, Yue Y, Pan M, Sun J, Chu J, Lin X, et al. Histone deacetylase 3 inhibits new tumor suppressor gene dtwd1 in gastric cancer. Am J Cancer Res. 2015;5(2):663.
Feldman DE, Chen C, Punj V, Machida K. The tbc1d15 oncoprotein controls stem cell self-renewal through destabilization of the numb-p53 complex. PLoS One. 2013;8(2):57312.
Liu T, Zhang T, Zhou F, Wang J, Zhai X, Mu N, et al. Identiffcation of genes and pathways potentially related to phf20 by gene expression proffle analysis of glioblastoma u87 cell line. Cancer Cell Int. 2017;17(1):1–12.
Cekic S, Hartberger JM, Frey-Jakobs S, Huriyet H, Hortoglu MB, Neubauer JC, et al. Cancer tendency in a patient with znf341 deffciency. J Clin Immunol. 2020;40(3):534–8.
Watkins G, Douglas-Jones A, Mansel RE, Jiang WG. Expression of thromboxane synthase, tbxas1 and the thromboxane a2 receptor, tbxa2r, in human breast cancer. In: International Seminars in Surgical Oncology, vol. 2: Springer; 2005. p. 1–8.
Mitra A, Shevde LA, Samant RS. Multi-faceted role of hsp40 in cancer. Clin Exp Metastasis. 2009;26(6):559–67.
Nan H, Han L, Ma J, Yang C, Su R, He J. Stx3 represses the stability of the tumor suppressor pten to activate the pi3k-akt-mtor signaling and promotes the growth of breast cancer cells. Biochim Biophys Acta Mol Basis Dis. 2018;1864(5):1684–92.
Li Z, Liu J, Chen H, Zhang Y, Shi H, Huang L, et al. Ferritin light chain (ftl) competes with long noncoding rna linc00467 for mir-133b binding site to regulate chemoresistance and metastasis of colorectal cancer. Carcinogenesis. 2020;41(4):467–77.
Fluegel ML, Parker TJ, Pallanck LJ. Mutations of a drosophila npc1 gene confer sterol and ecdysone metabolic defects. Genetics. 2006;172(1):185–96.
Schollen E, Pardon E, Heykants L, Renard J, Doggett NA, Callen DF, et al. Comparative analysis of the phosphomannomutase genes pmm1, pmm2 and pmm2 : the sequence variation in the processed pseudogene is a reection of the mutations found in the functional gene. Hum Mol Genet. 1998;7(2):157–64.
Li J, Chang J, Tian J, Ke J, Zhu Y, Yang Y, et al. A rare variant p507l in tpp1 interrupts tpp1-tin2 interaction, inuences telomere length, and confers colorectal cancer risk in chinese population. Cancer Epidemiol Prev Biomarkers. 2018;27(9):1029–35.
Ullah F, Khan T, Ali N, Malik FA, Kayani MA, Shah STA, et al. Promoter methylation status modulate the expression of tumor suppressor (rbl2/p130) gene in breast cancer. PLoS One. 2015;10(8):0134687.
Clark DJ, Mei Y, Sun S, Zhang H, Yang AJ, Mao L. Glycoproteomic approach identiffes kras as a positive regulator of creg1 in non-small cell lung cancer cells. Theranostics. 2016;6(1):65.
Kjällquist U, Erlandsson R, Tobin NP, Alkodsi A, Ullah I, Stffalhammar G, et al. Exome sequencing of primary breast cancers with paired metastatic lesions reveals metastasis-enriched mutations in the a-kinase anchoring protein family (akaps). BMC Cancer. 2018;18(1):1–17.
Fodde R. The apc gene in colorectal cancer. Eur J Cancer. 2002;38(7):867–71.
Liu J, Wu Z, Han D, Wei C, Liang Y, Jiang T, et al. Mesencephalic astrocyte-derived neurotrophic factor inhibits liver cancer through small ubiquitin-related modiffer (sumo) ylation-related suppression of nf-ffb/snail signaling pathway and epithelial-mesenchymal transition. Hepatology. 2020;71(4):1262–78.
Rampino N, Yamamoto H, Ionov Y, Li Y, Sawai H, Reed JC, et al. Somatic frameshift mutations in the bax gene in colon cancers of the microsatellite mutator phenotype. Science. 1997;275(5302):967–9.
Pichiorri F, Palmieri D, De Luca L, Consiglio J, You J, Rocci A, et al. In vivo ncl targeting affects breast cancer aggressiveness through mirna regulation. J Exp Med. 2013;210(5):951–68.
Samanta D, Park Y, Andrabi SA, Shelton LM, Gilkes DM, Semenza GL. Phgdh expression is required for mitochondrial redox homeostasis, breast cancer stem cell maintenance, and lung metastasis. Cancer Res. 2016;76(15):4430–42.
Amiable C, Pochet S, Padilla A, Labesse G, Kaminski PA. N 6-substituted amps inhibit mammalian deoxynucleotide n-hydrolase dnph1. PLoS One. 2013;8(11):80755.
Ni Y, Seballos S, Fletcher B, Romigh T, Yehia L, Mester J, et al. Germline compound heterozygous poly-glutamine deletion in usf3 may be involved in predisposition to heritable and sporadic epithelial thyroid carcinoma. Hum Mol Genet. 2017;26(2):243–57.
Oguri T, Katoh O, Takahashi T, Isobe T, Kuramoto K, Hirata S, et al. The krüppel-type zinc ffnger family gene, hkr1, is induced in lung cancer by exposure to platinum drugs. Gene. 1998;222(1):61–7.
Viswanathan SR, Nogueira MF, Buss CG, Krill-Burger JM, Wawer MJ, Malolepsza E, et al. Genome-scale analysis identiffes paralog lethality as a vulnerability of chromosome 1p loss in cancer. Nat Genet. 2018;50(7):937–43.
Sonoshita M, Itatani Y, Kakizaki F, Sakimura K, Terashima T, Katsuyama Y, et al. Promotion of colorectal cancer invasion and metastasis through activation of notch-dab1-abl-rhogef protein trio. Cancer discovery. 2015;5(2):198–211.
Försti A, Jin Q, Altieri A, Johansson R, Wagner K, Enquist K, et al. Polymorphisms in the kdr and postn genes: association with breast cancer susceptibility and prognosis. Breast Cancer Res Treat. 2007;101(1):83–93.
Norollahi SE, Alipour M, Rashidy-Pour A, Samadani AA, Larijani LV. Regulatory uctuation of wnt16 gene expression is associated with human gastric adenocarcinoma. J Gastrointest Cancer. 2019;50(1):42–7.
Danko I, Chaschin N. Association of cyp2e1 gene polymorphism with predisposition to cancer development. Exp Oncol. 2005;27(4):248–56.
Endo M, Kohashi K, Yamamoto H, Ishii T, Yoshida T, Matsunobu T, et al. Ossifying ffbromyxoid tumor presenting ep400-phf1 fusion gene. Hum Pathol. 2013;44(11):2603–8.
Zhu W, Jarman KE, Lokman NA, Neubauer HA, Davies LT, Gliddon BL, et al. Cib2 negatively regulates oncogenic signaling in ovarian cancer via sphingosine kinase 1. Cancer Res. 2017;77(18):4823–34.
Saigusa S, Inoue Y, Tanaka K, Toiyama Y, Okugawa Y, Shimura T, et al. Decreased expression of dusp4 is associated with liver and lung metastases in colorectal cancer. Med Oncol. 2013;30(3):620.
Yan S-M, Tang J-J, Huang C-Y, Xi S-Y, Huang M-Y, Liang J-Z, et al. Reduced expression of zdhhc2 is associated with lymph node metastasis and poor prognosis in gastric adenocarcinoma. PLoS One. 2013;8(2):56366.
Siu MK, Wong ES, Kong DS, Chan HY, Jiang L, Wong OG, et al. Stem cell transcription factor nanog controls cell migration and invasion via dysregulation of e-cadherin and foxj1 and contributes to adverse clinical outcome in ovarian cancers. Oncogene. 2013;32(30):3500–9.
Wang M, Zhu X, Sha Z, Li N, Li D, Chen L. High expression of kinesin light chain-2, a novel target of mir-125b, is associated with poor clinical outcome of elderly non-small-cell lung cancer patients. Br J Cancer. 2015;112(5):874–82.
Guo C, Xiong D, Yang B, Zhang H, Gu W, Liu M, et al. The expression and clinical signiffcance of zbtb7 in transitional cell carcinoma of the bladder. Oncol Lett. 2017;14(4):4857–62.
Lee HW, Park YM, Lee SJ, Cho HJ, Kim D-H, Lee J-I, et al. Alpha-smooth muscle actin (acta2) is required for metastatic potential of human lung adenocarcinoma. Clin Cancer Res. 2013;19(21):5879–89.
Fan X, Wang C, Song X, Liu H, Li X, Zhang Y. Elevated cathepsin k potentiates metastasis of epithelial ovarian cancer. Histol Histopathol. 2018;33(7):673–80.
Hou T, Tong C, Kazobinka G, Zhang W, Huang X, Huang Y, et al. Expression of col6a1 predicts prognosis in cervical cancer patients. Am J Transl Res. 2016;8(6):2838.
Chen P, Wang R, Yue Q, Hao M. Long non-coding rna ttn-as1 promotes cell growth and metastasis in cervical cancer via mir-573/e2f3. Biochem Biophys Res Commun. 2018;503(4):2956–62.
Li M-Z, Wang J-J, Yang S-B, Li W-F, Xiao L-B, He Y-L, et al. Zeb2 promotes tumor metastasis and correlates with poor prognosis of human colorectal cancer. Am J Transl Res. 2017;9(6):2838.
Liu G. Cdh1 promoter methylation in patients with cervical carcinoma: a systematic meta-analysis with trial sequential analysis. Future Oncol. 2018;14(1):51–63.
Li M, Cheng X, Rong R, Gao Y, Tang X, Chen Y. High expression of ffbroblast activation protein (fap) predicts poor outcome in high-grade serous ovarian cancer. BMC Cancer. 2020;20(1):1–8.
Lim S, Hermance N, Mudianto T, Mustaly HM, Mauricio IPM, Vittoria MA, et al. Identiffcation of the kinase stk25 as an upstream activator of lats signaling. Nat Commun. 2019;10(1):1–17.
Morita R, Hirohashi Y, Torigoe T, Ito-Inoda S, Takahashi A, Mariya T, et al. Olfactory receptor family 7 subfamily c member 1 is a novel marker of colon cancer-initiating cells and is a potent target of immunotherapy. Clin Cancer Res. 2016;22(13):3298–309.
Ko KK, Powell MS, Hogarth PM. Zswim1: a novel biomarker in t helper cell differentiation. Immunol Lett. 2014;160(2):133–8.
Guo Q, Li L, Bo Q, Chen L, Sun L, Shi H. Long noncoding rna pitpna-as1 promotes cervical cancer progression through regulating the cell cycle and apoptosis by targeting the mir-876-5p/c-met axis. Biomed Pharmacother. 2020;128:110072.
Xiu M-X, Liu Y-M, Kuang, B.-h. The role of dlls in cancer: a novel therapeutic target. Onco Targets Ther. 2020;13:3881.
Pereira AL, Pereira AJ, Maia AR, Drabek K, Sayas CL, Hergert PJ, et al. Mammalian clasp1 and clasp2 cooperate to ensure mitotic ffdelity by regulating spindle and kinetochore function. Mol Biol Cell. 2006;17(10):4526–42.
Itskovich SS, Gurunathan A, Clark J, Burwinkel M, Wunderlich M, Berger MR, et al. Mbnl1 regulates essential alternative rna splicing patterns in mll-rearranged leukemia. Nat Commun. 2020;11(1):1–14.
Wang Q-M, Lv L, Tang Y, Zhang L, Wang L-F. Mmp-1 is overexpressed in triple-negative breast cancer tissues and the knockdown of mmp-1 expression inhibits tumor cell malignant behaviors in vitro. Oncol Lett. 2019;17(2):1732–40.
Zubillaga-Guerrero MI, del Carmen Alarcffon-Romero L, Illades-Aguiar B, Flores-Alfaro E, Bermffudez-Morales VH, Deas J, et al. Microrna mir-16-1 regulates ccne1 (cyclin e1) gene expression in human cervical cancer cells. Int J Clin Exp Med. 2015;8(9):15999.
Nishioka C, Ikezoe T, Takeuchi A, Nobumoto A, Tsuda M, Yokoyama A. The novel function of cd82 and its impact on bcl2l12 via akt/stat5 signal pathway in acute myelogenous leukemia cells. Leukemia. 2015;29(12):2296–306.
Mentrup T, Loock A-C, Fluhrer R, Schroder, B. Signal peptide peptidase and spp-like proteases-possible therapeutic targets? Biochimica et Biophysica Acta (BBA)-molecular. Cell Res. 2017;1864(11):2169–82.
Stebbing J, Lit L, Zhang H, Darrington R, Melaiu O, Rudraraju B, et al. The regulatory roles of phosphatases in cancer. Oncogene. 2014;33(8):939–53.
Prevo R, Tiwana GS, Maughan TS, Buffa FM, McKenna WG, Higgins GS. Depletion of signal recognition particle 72kda increases radiosensitivity. Cancer Biol Ther. 2017;18(6):425–32.
Acknowledgements
The authors are grateful to the gene omnibus repository of the public domain data on ovarian cancer.
Funding
We further confirm that there has been no significant financial support for this work that could have influenced its outcome.
Author information
Authors and Affiliations
Contributions
All authors had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Conceptualization-Akash Pawar, Oindrila Roy Chowdhury,Ruby Chauhan. Analysis- Atanu Bhattacharjee. Interpretation- Sanjay Talole, Akash Pawar, Oindrila Roy Chowdhury, Ruby Chauhan. Drafting- Akash Pawar, Oindrila Roy Chowdhury, Ruby Chauhan. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
1. Statement on ethics approval (or to say it was waived) - We the undersigned declare that this manuscript is original, has not been published before and is not currently being considered for publication elsewhere.
2. Name of the ethics committee and the committee’s reference number - Ethical approval is not applicable. Anonymized data available in public domain repository as secondary sourced is used for this work. As institutional policy, ethical approval is not required for studies involving public domain data. Since no interventions carried on any living being.
3. The research does not involve human participants, human data or tissue or animals a statement. So this is not applicable.
Consent for publication
1. Not Applicable. Anonymized data available in public domain repository as secondary sourced is used for this work. Any individual has not been directly interacted.
2. No face is shown on a photo relating to the individual case. So no consent is needed.
3. The study doesn’t contain any data from an individual person. So it is not applicable.
Competing interests
We wish to confirm that there are no known conflicts of interest associated with this publication.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pawar, A., Chowdhury, O.R., Chauhan, R. et al. Identification of key gene signatures for the overall survival of ovarian cancer. J Ovarian Res 15, 12 (2022). https://doi.org/10.1186/s13048-022-00942-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13048-022-00942-0