
Abstract
Background
Most multi-problem young adults (18–27 years old) have been exposed to childhood maltreatment and/or have been involved in juvenile delinquency and, therefore, could have had Child Protection Service (CPS) interference during childhood. The extent to which their childhood problems persist and evolve into young adulthood may differ substantially among cases. This might indicate heterogeneous profiles of CPS risk factors. These profiles may identify combinations of closely interrelated childhood problems which may warrant specific approaches for problem recognition and intervention in clinical practice. The aim of this study was to retrospectively identify distinct statistical classes based on CPS data of multi-problem young adults in The Netherlands and to explore whether these classes were related to current psychological dysfunctioning and delinquent behaviour.
Methods
Age at first CPS interference, numbers and types of investigations, age at first offence, mention of child maltreatment, and family supervision order measures (Dutch: ondertoezichtstelling; OTS) were extracted from the CPS records of 390 multi-problem young adult males aged 18–27 (mean age 21.7). A latent class analysis (LCA) was conducted and one-way analyses of variance and post-hoc t-tests examined whether LCA class membership was related to current self-reported psychological dysfunctioning and delinquent behaviour.
Results
Four latent classes were identified: (1) late CPS/penal investigation group (44.9%), (2) early CPS/multiple investigation group (30.8%), (3) late CPS interference without investigation group (14.6%), and (4) early CPS/family investigation group (9.7%). The early CPS/family investigation group reported the highest mean anxiousness/depression and substance use scores in young adulthood. No differences were found between class membership and current delinquent behaviour.
Conclusions
This study extends the concept that distinct pathways are present in multi-problem young adults who underwent CPS interference in their youth. Insight into the distinct combinations of CPS risk factors in the identified subgroups may guide interventions to tailor their treatment to the specific needs of these children. Specifically, treatment of internalizing problems in children with an early onset of severe family problems and for which CPS interference is carried out should receive priority from both policy makers and clinical practice.
Similar content being viewed by others

Background
Childhood onset of delinquent behaviour and severe family problems, including child maltreatment and neglect, are associated with a variety of adverse outcomes in young adulthood [1,2,3,4,5,6]. These childhood problems are important risk factors for later delinquent behaviour and hamper psychological functioning [1, 3, 4, 7,8,9,10,11,12,13,14,15,16,17]. So far, childhood risk factors of adulthood problems have been studied either within delinquent populations [1,2,3, 9, 13, 18,19,20,21] or in populations of young adults who experienced maltreatment and out-of-home placements in their childhood [3, 22]. These studies focused predominantly on the severity, age of onset and persistence of delinquent behaviour and on maltreatment and family interferences by, for example, the Child Protection Services (CPS; Dutch: Raad voor de Kinderbescherming). However, such childhood problems are closely interrelated and the presence of multiple problems in childhood drastically increases the probability of adverse adult outcomes [19, 23, 24]. Therefore, studies should focus on combinations of risk factors in young children [13, 25, 26], instead of focusing on single risk factors, and assess to what extent these combinations can predict outcomes later in life. In this way, it may be possible to distinguish among youth risk profiles which may help tailor primary, secondary and tertiary prevention strategies. The present study tackled these issues by retrospectively studying combined risk factors and long-term outcomes of both childhood judicial and civil CPS interferences in multi-problem young adults.
Young adulthood is considered a distinct developmental stage comprising major psychological [27,28,29], social [27] and neurobiological [30] changes that are critical for a healthy transition towards adulthood [31,32,33]. In most cases, young adults (aged 18–27) who experienced severe psychological, family and judicial problems since childhood encounter difficulties during this transition in becoming self-sufficient adults [32,33,34,35]. Previous studies have provided evidence that these vulnerable young adults are at high risk of an accumulation of several problems such as unemployment, psychological problems, early parenthood, and court involvement [34, 36,37,38]. Furthermore, a majority of these young adults suffer from substance use disorder [39, 40], and lack social support [33, 34]. This group with multiple and intertwined problems has been called multi-problem young adults, and is increasingly recognized as warranting specific scientific attention in order to inform and help improve professional support [33, 41]. An important aspect in this respect is to understand the development of the childhood problems that culminate in these multi-problem young adults.
In general, childhood problems as risk factors of later delinquent behaviour and mental health problems are widely studied. These risk factors are often distinguished on the individual and family level [2, 9, 12, 13]. Individual risk factors as intellectual disability, disruptive behaviour, psychological problems and an early onset of substance use are related to the development of antisocial behaviour [2, 42,43,44] later in life, and to mental health problems in adulthood as well [45]. Other risk factors in this respect are low school achievement and truancy [46, 47]. Important risk factors on the family level are inadequate parenting, low social economic status, maltreatment and neglect, mental health problems and substance abuse of parents [12]. All these factors may have contributed in their own unique way to the various problems of young adults.
Many multi-problem young adults have demonstrated delinquent behaviour and severe family problems during childhood [1, 22, 48,49,50] and, therefore, are likely to have underwent CPS interference during their youth. In The Netherlands, there are two main reasons for a child to receive a CPS investigation: to request a civil or a penal measure. It is not uncommon for children to receive multiple CPS interferences during their lives [3]. Therefore, the characteristics of CPS interference differ among children [21, 51,52,53]. Multi-problem young adults are likely to have experienced several judicial, school and family problems simultaneously [19, 23, 24], for which the timing, the number and the intensity of CPS investigations may vary [3]. CPS characteristics can be seen as static risk factors [54] for deviant development since children who underwent CPS interference have an elevated risk of developing delinquent behaviour and mental health problems in young adulthood [1, 3, 8, 21, 48, 55, 56]. The annual arrest rate for young adults who as children had been referred to CPS is more than four times higher than the national rate for 18- to 24-year olds [57] and 50% of this young adult population have experienced mental health problems [57].
Whereas all children who were exposed to severe family problems and/or who were involved in juvenile delinquency have an elevated risk of adult problem behaviour [1, 6, 15, 50, 58,59,60,61], the extent to which these problems persist and evolve into young adulthood differs substantially [7, 61, 62]. This might indicate heterogeneous profiles of the concurrent childhood problems. Several studies investigated and aimed to reduce the heterogeneity of problems within comparable populations of high-risk youths by exploring profiles [9, 13]. A study by Haapasalo found two groups of young adult offenders with CPS interventions: an early onset multiple intervention group and a late onset group who had fewer interventions [3]. A study by Dembo et al. [9] in high-risk youths reported two classes based on self-report data; one with a low prevalence and the other with a high prevalence of problems in family and peer relations, psychological functioning and education [9]. Furthermore, Geluk et al. [13] distinguished three profiles in childhood arrestees, differing in the extent of problems in peer relations, psychological functioning and authority conflicts. So, exploring profiles proved useful in ordering these childhood problems into several homogenous classes concerning the onset, the prevalence and the extent of the problems. However, these studies did not explore specifically if and how these childhood classes may contribute to a deviant development into (young) adulthood.
Although CPS does not provide treatment, CPS interference is directly related to extensive contact with judicial, mental health and social services [48, 63] and CPS may refer their clients to appropriate care, if necessary. However, many (young) adults with a childhood history of CPS interference still experience serious problems, even after repeated intervention [3, 48, 49, 64, 65]. As such, it seems that the effectiveness of current secondary prevention and intervention practices during childhood is limited in this population. Therefore, retrospectively identifying classes of interrelated static risk factors of CPS interference within a relatively unstudied population of multi-problem young adults may prove useful for more effective problem recognition and screening purposes in childhood [26, 54]. Finally, relating these childhood classes to delinquency and mental health problems in young adulthood may give useful indications for the prevention of the escalation of these problems to clinical practice [48, 49].
The present study aims to explore whether groups of CPS characteristics in childhood can be identified within a sample of multi-problem young adults. Furthermore, the associations between class membership and both self-reported delinquency and psychological functioning in young adulthood are investigated. Based on the literature, we expect multi-problem young adults to have a significant prevalence of CPS interference. Within this group we expect to find distinct latent classes differing in the onset, number and intensity of judicial and civil interferences [3] and in the extent of family problems [7, 9]. Lastly, it is hypothesized that classes of CPS interference in youths relate differently to current psychological dysfunctioning and current severity of delinquent behaviour in multi-problem young adults [1, 65, 66].
Methods
Study sample
In 2014–2016 a total of 596 multi-problem young adults were recruited in Rotterdam, The Netherlands. All participants were male, between 18 and 27 years old (mean age 21.7), and had sufficient knowledge of the Dutch language to understand the study procedure and the questionnaires. This study was part of a larger study in which participants were recruited from two sites. The first site was a municipal agency (Dutch: Jongerenloket) where young adults between the ages of 18 and 27 can apply for social welfare. Every year over 4000 intakes are carried out by so-called youth coaches [67]. During this intake, the level of self-sufficiency of the young adult is assessed on eleven life domains with the validated Self-Sufficiency Matrix—Dutch version (SSM-D) [68,69,70], based on the American version of the SSM [71], on a five-point scale with scores ranging from 1 (acute problems) to 5 (completely self-sufficient). Participants were eligible when they adhered to the following definition: (a) a score of 1 or 2 on the domains Income and Daytime Activities, (b) a maximum score of 3 on at least one of the following domains: Addiction, Mental health, Social network, Justice and (c) a minimum score of 3 on the domain Physical health [72]. Eligible young adults were asked to cooperate voluntarily. As a part of a larger study, N = 436 participants were recruited in this way [72]. The second site was multimodal day treatment program New Opportunities (Dutch: De Nieuwe Kans; DNK). Multi-problem young adults also signed up to DNK themselves or were referred to DNK directly by youth care, probation services, mental health services or social organizations. Therefore, additional participants were recruited directly from DNK (N = 160). From the total study sample (N = 596), 99.3% (N = 592) gave informed consent to conduct the register and record research. Of the N = 592, 65.9% (N = 390) was matched to a record in the CPS system.
Procedure
The study was performed by the VU University Medical Center Department of Child and Adolescent Psychiatry and approved by the Medical Ethics Review Committee of VU University Medical Center.Footnote 1 Participants gave informed consent before voluntary participation after a member of the research team had provided oral information accompanied by written information. After informed consent, trained (junior) researchers administered questionnaires.
Interference with CPS was checked in the CPS system Kinderbescherming Bedrijfs Processen Systeem (KBPS) using first names, surname and date of birth of the participants. This resulted in a match of 65.9% (N = 390) of the total sample (N = 592); 34.1% (N = 202) did not match to a record in the system. For a part of the latter group it is uncertain whether they truly never had CPS contact or whether their record has been destroyed, since CPS is legally required to destroy records of clients that reach age 24. This applies to N = 98 of the N = 202 that did not match to a record in the system. For the other N = 104 (51.5% of N = 202), it was certain that they did not have CPS interference, since they were younger than 24 years old. The CPS files consist of all documents received and sent by the CPS concerning the child and a selection of judicial and police report data [73]. Data were extracted from April 2015 to August 2016 by trained (junior) researchers. To test the inter-rater reliability, 19 randomly selected files were scored by two independent raters, showing a substantial inter-rater reliability (κ = 0.72) [74, 75].
Context
The register and record research was conducted at CPS and the data were extracted between April 2015 and August 2016. CPS monitors children between 0 and 18 years old when there are serious concerns regarding their home situation and upbringing. In families with severe parenting problems a child welfare investigator can perform a civil protection investigation of the home environment of the child, at the request of CPS. At the request of the court, CPS mediates when parents break up and disagree about arrangements concerning their children. Moreover, CPS can initiate a judicial or truancy investigation for youth suspected of an offence or truancy. The investigation report with recommendations on (mandatory) service use or a suitable penalization is delivered to the court [73].
Measurements
Socio-demographic characteristics
Socio-demographic characteristics were assessed with a structured self-report questionnaire. Ethnicity was based on the country of birth of the respondent and at least one of his parents. A respondent was classified as non-Dutch if he or one of his parents was not born in The Netherlands [76]. Ethnicity was recoded into a dichotomous variable (Dutch ethnicity vs. other ethnicity). Educational level was classified into three levels: maximum primary education, achievement of junior secondary education and senior secondary education attainment. Family problems in youth were assessed with the single item ‘Did you suffer from problems that existed in the family you grew up with? (Yes/No)’. Police contact of family members in youth was assessed with the single item ‘Did family members you grew up with have police contact? (Yes/No)’. Prior service use was assessed with the single item ‘Did you previously use services? (Yes/No)’. Frequency of service use was assessed with the single item ‘Which services did you have contact with?’ (e.g., youth care, probation services, child protection services). This was recoded into a frequency score defined as the number of self-reported services.
CPS variables
Several variables were obtained from the CPS records. All variables were divided into categories to perform the latent class analysis (LCA), as it is a condition for this analysis to use categorical variables. The variables Age of first CPS report, Type of investigation, Number of investigations, Child maltreatment, Age of onset of delinquent behaviour and Family supervision order were used as indicators to execute the LCA. Age of first CPS report in which date of the first CPS investigation was recoded into four categories: no report, below age 13, 13 or 14 years old, age 15 up to 18. The CPS records provided information on three types of investigations: offence investigation, protection investigation and truancy investigation. Type of investigation was recoded into a variable that contained five categories: no investigation, protection investigation, offence investigation, truancy investigation, several types of investigations. Number of CPS investigations was recoded into three categories: no investigation, one or two investigations, at least three investigations. Child maltreatment was extracted from the record when a professional ascertained child maltreatment (Yes/No). Domestic violence was observed and registered by a professional (Yes/No). The verdict of the court to impose a family supervision order was included in the record (Yes/No). Out-of-home placement was also included in the record in the verdict of the court (Yes/No). Age of onset of delinquent behaviour: the date of the first offence was registered based on the police report. Using this date combined with the date of birth, the age of first offence was computed. This variable was recoded into four categories: no offence, first offence below age thirteen, first offence between 13 and 14 years of age, and first offence at age 15 or older.
Current psychological functioning
The Dutch version of the Adult Self Report (ASR) [77] was assessed orally and filled out by the researcher to obtain current psychological functioning. ASR part VIII consists of 123 items on internalizing and externalizing problems during the previous 6 months. The reliability of the questionnaire is good, with a Cronbach’s α of 0.83. In this study the ASR total problem score and the scores of nine subscales were used as outcome measures. The subscales are: anxious/depressed, withdrawn, somatic complaints (internalizing problems); intrusive, rule-breaking and aggressive behaviour (externalizing problems); thought problems, attention problems and substance use. The prevalence of serious dysfunctioning on all subscales is presented in Table 1. The mean scale scores per class as outcome measure are based on percentile scores [78] (Table 5).
Delinquent behaviour
The frequency and seriousness of delinquent behaviour were investigated orally and filled out by a researcher using the Dutch version [79] of the Self-report Delinquency Scale (SRD) [80]. This questionnaire has 29 items (including two items of violation: fare dodging and lighting fireworks when prohibited) and the internal consistency of the total score is excellent with Cronbach’s α = 0.85 [79, 81]. The questionnaire explored the frequency of offences committed both during the respondent’s lifetime and in the previous 6 months. In addition, the items were also divided into four different offence categories: destruction/public order offences (5 items, Cronbach’s α = 0.64), property offences (11 items, Cronbach’s α = 0.79), aggression/violent offences (8 items, Cronbach’s α = 0.7) and drug offences (3 items, Cronbach’s α = 0.72) [79]. The frequencies per offence category were recoded into dichotomous variables (Yes/No), due to the skewed distribution of the data. Lifetime and previous 6 months’ prevalence are presented in Table 1. Mean scores based on the frequencies of offences in the previous 6 months were used as outcome measure (see Table 5). The 27 items (excluding two items of violation) add up to one total delinquency score reflecting the multiplication of the seriousness of the offences and their frequency. The seriousness is divided into minor and serious offences based on applicable legal penalties; minor offences have a maximum custodial sentence of 48 months (score 1) and serious offences have a minimum custodial sentence of 48 months (score 2) [79, 80].
Data analysis
In order to detect classes of childhood correlates Latent Class Analysis (LCA) was performed. LCA is a useful method for analysing the relationships among observed variables, when each observed variable is categorical, in a heterogeneous population assumed to be comprised of a set of latent classes [82]. LCA was performed with the program Statistical Analysis System (SAS) version 9.3. The six CPS childhood indicators mentioned above were entered into the LCA. Analyses were conducted using PROC LCA 1.2.6 for SAS 9.3 [83]. Good qualification quality was established taking into account the Bayesian information criterion (BIC), entropy and Akaike information criterion (AIC) [82]. The entropy value ranges between 0 and 1; a value approaching 1 indicates a clear description of the classes [84]. Subsequently, item response probability scores on all indicators were used to interpret the classes. Lastly, to explore differences among classes derived from the LCA on current psychological functioning and delinquent behaviour, One-Way Analyses of Variance and Post Hoc t-tests with Bonferroni correction were performed with Statistical Packages for the Social Sciences, version 22 for Windows [85].
Results
Table 1 shows the self-reported socio-demographic and family characteristics, service use, current psychological functioning and delinquent behaviour of multi-problem young adults with CPS interference in youth. It shows that many young adults had problems in youth; 63.2% had problems in their family, 83.3% reported prior service use and 93.3% committed an offence. During the previous 6 months, 53.0% had serious substance use problems and 63.0% committed an offence.
Childhood correlates of the CPS records
Table 2 shows the descriptive results of the childhood CPS correlates in percentages. After referral to CPS, 84.9% of participants were investigated. In 21.0% of the participants the first CPS investigation was below the age of thirteen and 39.0% had their first investigation at age fifteen or older. Almost half of the group (43.9%) had one or two CPS investigations and 41.5% had at least three CPS investigations. Judicial investigations were conducted in 75.0% of the group and protection investigations in 40.0% of participants. Multiple types of investigations were conducted in 32.6% of participants of which 50.0% first had a protection investigation and 40.0% first had a judicial investigation. Truancy investigations rarely occurred separately (1.8%). Child maltreatment was registered in 29.5% of the CPS reports and the CPS records reported domestic violence in 16.4% of the cases. Protection measures taken by the juvenile court were investigated as well; 33.6% of participants underwent a family supervision order and 22.1% an out-of-home placement. In 88.5% of the CPS records childhood delinquency was registered and 23.3% committed their first offence below age 13.
Identification of childhood correlate classes (Latent Class Analysis)
The first step conducted for the LCA involved identifying the number of latent classes that best fit the data on six childhood indicators. Table 3 presents the fit indices after carrying out several class models. Based on the entropy (0.95) and the BIC value (692.03), the four-class models fitted best. The five-class model, however, had the lowest value of the AIC (417.74). Models distinguishing six or more classes all performed worse on all indicators. Based on these findings and the interpretability of the resulting latent class model, we decided that the four-class model had the best fit for these data.
In order to interpret the latent classes, item response probabilities of the indicators were examined for each latent class. Table 4 presents the item-response probabilities and the proportions of the classes.
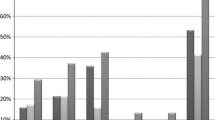
The first class, labelled as the late CPS/penal investigation group (44.9%) (Fig. 1), did not experience maltreatment or a family supervision order in childhood. They all committed at least one offenceFootnote 2 and their first offence was at age 13 or 14. Their first judicial CPS report was executed at age fifteen or older (late CPS interference) and they had a maximum of two, solely judicial, reports.

1-Late CPS/penal investigation group
A majority of the second class, labelled as the early CPS/multiple investigation group (30.8%) (Fig. 2), experienced maltreatment in childhood which often resulted in at least one family supervision order pronounced by the court. They had their first report at a young age, below age 13 (early CPS interference) and had three or more CPS investigations, due to various causes (judicial and/or family and/or truancy investigations), since they often committed their first offence below age thirteen.

2-Early CPS/multiple investigation group
The third class, labelled as the late CPS interference without investigation group (14.6%) (Fig. 3), did not experience any severe family problems such as maltreatment or family supervision orders. If they committed an offence, it was at age 15 or older (late CPS interference). CPS decided mostly not to investigate the child and they often did not have any reports in their record.

3-Late CPS interference without investigation group
The fourth class, labelled as the early CPS/family investigation group (9.7%) (Fig. 4), had early CPS interference below age thirteen (early CPS interference), due to severe family problems such as maltreatment which resulted mostly in at least one family supervision order. CPS decided to investigate their situations once or twice, which were specifically protection investigations. Participants in this group were not likely to commit any offence.

4-Early CPS/family investigation group
Table 5 presents results of the ANOVA and post hoc comparisons between LCA class membership on current psychological functioning. There was a significant difference among classes on anxious/depressive problems (p = 0.035), a borderline significant difference on intrusive problems (p = 0.056) and a significant difference on substance use (p = 0.029). The post hoc test showed that participants of the early CPS/family investigation group reported significantly more anxious/depressive problems than participants of the early CPS/multiple investigation group (p = 0.022). Moreover, the early CPS/family investigation group reported more substance abuse than the late CPS interference without investigation group (borderline significant; p = 0.056).
No significant differences among LCA classes were found on self-reported current delinquent behaviour (Table 5).
Discussion
The purpose of this study was twofold. The first aim was to retrospectively identify distinct classes in multi-problem young adults based on childhood CPS characteristics. This resulted in four latent classes: a late CPS/penal investigation group (44.9%), an early CPS/multiple investigation group (30.8%), a late CPS interference without investigation group (14.6%) and an early CPS/family investigation group (9.7%). The second aim was to explore whether these classes differed on current young adult psychological functioning and delinquent behaviour. The early CPS/family investigation group reported significantly more problematic anxiousness/depression problems than the other groups. Substance use differed significantly among groups, although post hoc tests only revealed borderline significant differences. No differences in current delinquent behaviour were reported among the classes.
In our sample of multi-problem young adults, 65.9% had one or more CPS interference(s) during their childhood versus 1% of the total population of Dutch children in 2016 [86]. Furthermore, 29.5% in the current sample underwent maltreatment versus 3% of Dutch youth that was in danger of any type of maltreatment in 2010 [87]. Thus, the prevalence of CPS interferences and severe family problems is, as expected, clearly higher in this population of multi-problem young adults than in the general population. One should note, however, that these percentages are not completely comparable, since the prevalence in the current study was not limited to 1 year. The high prevalence of CPS interference in multi-problem young adults matches their self-reported problems in childhood quite adequately: 83.3% reported service use in their youth and 63.2% reported family problems. As expected, multi-problem young adults also experience heterogeneous problems in their current functioning. This extends findings in other studies [88,89,90] that argue that different forms of problem behaviour (such as mental health problems, delinquency and substance use) with an onset in childhood are interrelated and may be seen as symptoms of a general disposition toward deviant behaviour through life, by some referred to as problem behaviour syndrome (PBS) [91]. How PBS is expressed may vary over time and across contexts. For children with PBS, the transition to adulthood typically occurs in the context of severe family problems and interference by multiple justice/care/and child welfare systems [41, 66]. Therefore, they may experience a differential pathway into adulthood in which more tailor-made specialized care is needed to support their adopting adult responsibilities such as independent living [41]. This way, they may be prevented from growing into multi-problem young adults. Our first findings underline the importance of gaining more insight into the childhood onset of the problem heterogeneity of multi-problem young adults in order to enhance effective tailor-made intervention.
The present study confirmed several distinct classes of risk factors for adult problem behaviour in addition to earlier studies [3, 9, 13]. Dembo et al. 9 and Geluk et al. 13 identified two and three classes, respectively, differing in the extent of problem behaviour; Haapasalo [3] reported two classes differing in age of onset and number of CPS interventions. A first distinction in the identified classes in the current study indeed occurred between early (below age 13) and late (from age 15) CPS involvement. The early CPS/multiple investigation group had the earliest onset of delinquent behaviour (below age 13). Several studies show that early onset delinquents are more at risk for problems in young adulthood, such as mental health problems, substance abuse, drug related and violent delinquent behaviour, than later onset delinquents [20, 61]. Furthermore, the early CPS/multiple investigation group underwent the most CPS investigations and is, therefore, also comparable to the early onset group in the Haapasalo study [3], in which the offenders demonstrated more problems during their youth and were in greater need of CPS interventions such as placement in foster care.
Regarding the long term outcomes of childhood CPS interference specifically, the early CPS/family investigation group reported the most anxious/depression problems and the most substance abuse in young adulthood. Maltreatment, family supervision and other severe family problems in childhood have repeatedly been shown to be robust risk factors for mental health problems in (young) adulthood [7, 16]. For example, according to Thornberry et al. [15], childhood maltreatment is indeed strongly related to later substance abuse and internalizing problems. Although the early CPS/family investigation was the smallest identified group (9.7%), they seem to have followed the most adverse developmental pathway into young adulthood. It is possible that CPS failed to provide appropriate interventions for this group, since the CPS involvement was not as intensive as for the early onset/multiple investigation group. Moreover, the early CPS/family group was the only group that did not engage in delinquent behaviour in childhood/adolescence. This may have caused them to stay unnoticed for a longer period of time. However, traumatic events in the child’s family environment may have already occurred long before the first CPS interference and are associated with an increased likelihood of adverse adult outcomes [7, 16]. Besides a broader focus on the problems of the child itself, children with solely civil CPS interference may benefit from more attention to treatment of the problems of the parents. Interventions could be aimed at strengthening their parenting capabilities and resources. Adopting such a ‘two-generation approach’ has shown promising results in preventing family and childhood problems from growing worse [92].
No significant differences among classes in current delinquent behaviour were found among groups. The late CPS/penal group was the largest group in our sample (44.9%); their first CPS investigation was at age 15 or older and the age of onset of their delinquent behaviour varied between ages 13 and 15. All multi-problem young adults showed a strong tendency for persisting in and/or developing criminal behaviour into adulthood, notwithstanding their distinct childhood histories. Moreover, since the group without CPS investigations also reported delinquent behaviour in adulthood, all forms of CPS interference (even marginal contact) should be considered risk factors for later antisocial behaviour. In addition, the late CPS/penal children proved to be a group without severe family problems, at least according to the CPS data. Steinberg [17] noted that adolescent onset offenders often manifest less severe patterns of family pathology and mental health problems than life course persistent offenders [61]. In our sample, both late onset CPS groups indeed reported fewer mental health problems in young adulthood than the early onset groups. A follow-up study should be conducted to explore whether these differences in problem behaviour among groups still persist into (middle) adulthood. Finally, since all groups persisted in their delinquent behaviour, children with CPS interference should be targeted as a high-risk population in need of specialized interventions aimed at reducing the criminogenic risk factors associated with recidivism.
Limitations
Like any other study, this study has some limitations. First, the CPS record investigation in the current study was not performed using a validated instrument, because an applicable instrument was not available. However, CPS investigations are standardized and in order to optimize and monitor the quality of the data, inter-rater reliability was analysed and found to be substantial. Second, registered offence data, and in particular data on the first offence, is likely to be under reported, as a minority of juvenile delinquents is actually convicted [24]. Still, in this sample officially recorded and self-reported delinquency data are, while not exactly similar, quite comparable, both showing a high prevalence of delinquent behaviour. Third, in this study, self-report questionnaires were also used to investigate socio-demographic characteristics and psychological functioning. To achieve good reliability, a validated self-report psychological functioning questionnaire is used and anonymity and privacy of participants was emphasized before and during the assessment of questionnaires. Fourth, a majority of 87.4% of participants in this study have a non-Dutch ethnicity. In our case, non-Dutch ethnicity refers to an amalgam of cultural backgrounds, for example Surinamese, Antillean, Moroccan and Turkish. However, due to small sample sizes per ethnic subgroup, it was not possible to perform separate analyses. Fifth, generalizability of study results to an international context is not straightforward, because of different service system organizations. In Great-Britain and the United States of America, for example, child protection service and the judicial youth system are more separate systems than in The Netherlands [93, 94]. Scandinavian countries have more comparable systems to the Dutch system, although those systems are more based on prevention. For instance, in Sweden voluntary and involuntary services are not divided as in The Netherlands [95]. And lastly, LCA is an exploratory data-driven method and the findings per class represent probabilities on latent indicators.
Conclusions
This study adds to the concept that even in a highly complex sample of multi-problem young adults who underwent CPS interference in their youth distinct developmental pathways, at least for mental health problems, can be distinguished. Although this exploratory study was not intended to produce definite ideas on how the underlying latent subgroups may experience differential treatment effects, our findings do suggest that members of the groups might benefit from interventions specifically tailored to their differing patterns of problems. The development of specific secondary and tertiary prevention programmes for children with an early onset of CPS interference and severe family problems should receive priority from both policy makers and clinical practice. In addition, evidence based interventions should be developed to prevent problem behaviour of all children that underwent CPS interference in their youth to prevent mental health problems and the persistence of delinquent behaviour into (young) adulthood.
Notes
Registration number: 2013.422—NL46906.029.13.
Those who committed no offence in youth, have not (yet) experienced the onset of delinquency. Therefore, the category ‘no offence’ is mentioned in Table 4. For classes 1 and 2 this translates into all respondents in these classes having committed at least one offence.
Abbreviations
- AIC:
-
akaike information criterion
- ANOVA:
-
analysis of variance
- ASR:
-
adult self report
- BIC:
-
Bayesian information criterion
- CAU:
-
care as usual
- CPS:
-
Child Protection Services
- Df:
-
degrees of freedom
- DNK:
-
New Opportunities (Dutch: De Nieuwe Kans)
- KBPS:
-
Kinderbescherming Bedrijfs Processen System (CPS system)
- LCA:
-
latent class analysis
- M:
-
mean
- SAS:
-
Statistical Analysis System
- SD:
-
standard deviation
- SPSS:
-
Statistical Packages for the Social Sciences
- SRD:
-
Self-Report Delinquency Scale
- SSM-D:
-
Self-Sufficiency Matrix-Dutch Version
References
Barrett DE, Katsiyannis A, Zhang D, Zhang D. Delinquency and recidivism: a Multicohort, Matched-Control Study of the Role of Early Adverse Experiences, Mental Health Problems, and Disabilities. J Emot Behav Disord. 2014;22:3–15.
Barrett DE, Katsiyannis A. Juvenile offending and crime in early adulthood: a large sample analysis. J Child Fam Stud. 2016;25:1086–97.
Haapasalo J. Young offenders’ experiences of Child Protection Services. J Youth Adolesc. 2000;29:355–71.
Edwards VJ, Holden GW, Felitti VJ, Anda RF. Relationship between multiple forms of childhood maltreatment and adult mental health in community respondents: results from the Adverse Childhood Experiences Study. Am J Psychiatry. 2003;160:1453–60.
Pecora PJ, Kessler RC, O’Brien K, White CR, Williams J, Hiripi E, et al. Educational and employment outcomes of adults formerly placed in foster care: results from the Northwest Foster Care Alumni Study. Child Youth Serv Rev. 2006;28:1459–81.
Braga T, Gonçalves LC, Basto-Pereira M, Maia Â. Unraveling the link between maltreatment and juvenile antisocial behavior: a meta-analysis of prospective longitudinal studies. Aggress Violent Behav. 2017;33:37–50.
Widom CS. The cycle of violence. Science. 1989;244:160–6.
DeGue S, Widom CS. Does out-of-home placement mediate the relationship between child maltreatment and adult criminality? Child Maltreat. 2009;14:344–55.
Dembo R, Wareham J, Poythress N, Meyers K, Schmeidler J. Psychosocial functioning problems over time among high-risk youths. Crime Delinq. 2008;54:644–70.
King DC, Abram KM, Romero EG, Washburn JJ, Welty LJ, Teplin LA. Childhood maltreatment and psychiatric disorders among detained youths. Psychiatr Serv. 2011;62:1430–8.
Haapasalo J, Pokela E. Child-rearing and child abuse antecedents of criminality. Aggress Violent Behav. 1999;4:107–27.
Moffitt TE, Caspi A. Childhood predictors differentiate life-course persistent and adolescence-limited antisocial pathways among males and females. Dev Psychopathol. 2001;13:355–75.
Geluk CAML, Van Domburgh L, Doreleijers TAH, Jansen LMC, Bouwmeester S, Garre FG, et al. Identifying Children at risk of problematic development: latent clusters among childhood arrestees. J Abnorm Child Psychol. 2014;42:669–80.
van Domburgh L, Loeber R, Bezemer D, Stallings R, Stouthamer-Loeber M. Childhood predictors of desistance and level of persistence in offending in early onset offenders. J Abnorm Child Psychol. 2009;37:967–80.
Thornberry TP, Henry KL, Ireland TO, Smith CA. The causal impact of childhood-limited maltreatment and adolescent maltreatment on early adult adjustment. J Adolesc Health. 2010;46:359–65.
Horwitz AV, Widom CS, McLaughlin J, White HR. The impact of childhood abuse and neglect on adult mental health: a Prospective Study. J Health Soc Behav. 2001;42:184–201.
Steinberg L. Adolescence. 10th ed. New York: McGraw-Hill; 2014.
Potter CC, Jenson JM. Cluster profiles of multiple problem youth: mental health problem symptoms, substance use, and delinquent conduct. Crim Justice Behav. 2003;30:230–50.
Van der Geest V, Bijleveld C, Blokland A. Ontwikkelingspaden van delinquent gedrag bij hoog-risicojongeren. Tijdschr. Voor Criminol. 2007;49:351–69.
Odgers CL, Moffitt TE, Broadbent JM, Dickson N, Hancox RJ, Harrington H, et al. Female and male antisocial trajectories: from childhood origins to adult outcomes. Dev Psychopathol. 2008;20:673–716.
Van Domburgh L, Vermeiren R, Blokland AA, Doreleijers TA. Delinquent development in dutch childhood arrestees: developmental trajectories, risk factors and co-morbidity with adverse outcomes during adolescence. J Abnorm Child Psychol. 2009;37:93–105.
Colman RA, Mitchell-Herzfeld S, Kim DH, Shady TA. From delinquency to the perpetration of child maltreatment: examining the early adult criminal justice and child welfare involvement of youth released from juvenile justice facilities. Child Youth Serv Rev. 2010;32:1410–7. https://doi.org/10.1016/j.childyouth.2010.06.010.
Shaw DS, Hyde LW, Brennan LM. Early predictors of boys’ antisocial trajectories. Dev Psychopathol. 2012;24:871–88.
Geest, Van der V, Blokland A, Bijleveld C. Delinquent development in a sample of high-risk youth: shape, content, and predictors of delinquent trajectories from age 12 to 32. J Res Crime Delinq. 2009;46:111–43. http://jrc.sagepub.com/content/46/2/111.abstract.
DeLisi M, Neppl TK, Lohman BJ, Vaughn MG, Shook JJ. Early starters: which type of criminal onset matters most for delinquent careers? J Crim Justice. 2013;41:12–7.
Loeber R, Burke JD. Developmental pathways in Juvenile externalizing and internalizing problems. J Res Adolesc. 2011;21:34–46.
Blokland A, Palmen H, San Van M. Crimineel gedrag in de jongvolwassenheid. Tijdschr Voor Criminol. 2012;54:85–98.
Doreleijers TH, Fokkens JW. Minderjarigen en jongvolwassenen: Pleidooi voor een evidence based strafrecht. Rechtstreeks. 2010;2:9–47.
Lamet W, James C, Dirkzwager A, Van der Laan P. Reclasseringstoezicht en jongvolwassenen. PROCES. 2010;89:371–83.
Crone EA. Executive functions in adolescence: inferences from brain and behavior. Dev Sci. 2009;12:825–30.
Arnett JJ. Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol. 2000;55:469–80.
Arnett JJ. Emerging adulthood : what is it, and What is it good for ? Child Dev Perspect. 2007;1:68–73.
D’Oosterlinck F, Broekaert E, Vander Haeghen C. Probleemjongeren te vroeg het te-huis uit? voor Orthop Kinderpsychiatrie, en Klin Kinderpsychologie. 2006;31:58–68.
Berzin SC. Difficulties in the transition to adulthood: using propensity scoring to understand what makes foster youth vulnerable. Soc Serv Rev. 2008;82:171–96.
Collins ME. Transition to adulthood for vulnerable youths: a review of research and implications for policy. Soc Serv Rev. 2001;72:271–91.
Bullis M, Yovanoff P. Those who do not return: correlates of the work and school engagemtent of formerly incarcerated youth who remain in the community. J Emot Behav Disord. 2002;10:66–78.
Fagan J, Freeman R. Crime and work. Crime Justice. 1999;25:225–90.
Ahrens KR, Garrison MM, Courtney ME. Health outcomes in young adults from foster care and economically diverse backgrounds. Pediatrics. 2014;134:1067–74.
Copeland WE, Miller-Johnson S, Keeler G, Angold A, Costello EJ. Childhood psychiatric disorders and young adult crime: a prospective population-based study. Am J Psychiatry. 2007;164:1668–75.
Arnett JJ. The developmental context of substance use in emerging adulthood. J Drug Issues. 2005;35:235–53.
Osgood DW, Foster EM, Flanagan C, Gretchen RR, Courtney ME, Heuring DH, et al. On your own without a net: the transition to adulthood for vulnerable populations. Osgood DW, Foster EM, Flanagan C, Ruth GR, editors. Chicago: The University of Chicago; 2005.
Fergusson DM, Horwood LJ. Early onset cannabis use and psychosocial adjustment in young adults. Addiction. 1997;92:279–96.
Loeber R, Farrington DP. Young children who commit crime: epidemiology, developmental origins, risk factors, early interventions, and policy implications. Dev Psychopathol. 2000;12:737–62.
Barron P, Hassiotis A, Banes J. Offenders with intellectual disability: a prospective comparative study. J Intellect Disabil Res. 2004;48:69–76.
Mun EY, Windle M, Schainker LM. A model-based cluster analysis approach to adolescent problem behaviors and young adult outcomes. Dev Psychopathol. 2008;20:291–318.
Murray J, Farrington DP. Risk factors for conduct disorder and delinquency: key findings from longitudinal studies. Can J Psychiatry. 2010;55:633–42.
Kearney CA. School absenteeism and school refusal behavior in youth: a contemporary review. Clin Psychol Rev. 2008;28(3):451–7.
Osgood DW, Foster EM, Courtney ME. Vulnerable populations and the transition to adulthood. Futur Child. 2010;20:209–29.
Courtney ME, Dworsky A. Early outcomes for young adults transitioning from out-of-home care in the USA. Child Fam Soc Work. 2006;11:209–19.
Smith CA, Park A, Ireland TO, Elwyn L, Thornberry TP. Long-term outcomes of young adults exposed to maltreatment: the role of educational experiences in promoting resilience to crime and violence in early adulthood. J Interpers Violence. 2013;28:121–56.
Havlicek J, Courtney ME. Maltreatment histories of aging out foster youth: a comparison of official investigated reports and self-reports of maltreatment prior to and during out-of-home care. Child Abus Negl. 2016;52:110–22.
Loman LA. Families frequently encountered by child protection services: a Report on Chronic Child Abuse and Neglect. Missouri: St. Louis; 2006.
Darlington Y, Healy K, Feeney JA. Approaches to assessment and intervention across four types of child and family welfare services. Child Youth Serv Rev. 2010;32:356–64.
Domburgh, Van L, Vermeiren R, Doreleijers TAH. Screening and assessment. In: Loeber R, Slot NW, Laan, van der PH, Hoeve M, editors. Tomorrow’s Crim. Dev. child Delinq. Eff. Interv. Aldershot: Ashgate; 2008. p. 165–78.
Montgomery P, Donkoh C, Underhill K. Independent living programs for young people leaving the care system: the state of the evidence. Child Youth Serv Rev. 2006;28:1435–48.
Kapp SA. Pathways to Prison: life histories of former clients of the child welfare and juvenile justice systems. J Soci Soc Welf. 2000;27:63–74.
International Research Triagle Institute. Adolescents involved with child welfare: a transition to adulthood. Washington D.C.: National Survey of Child and Adolescent Well-Being (NSCAW); 2008.
Fergusson DM, Lynskey MT. Physical punishment/maltreatment during childhood and adjustment in young adulthood. Child Abuse Negl. 1997;21:617–30.
Jonson-Reid M, Kohl PL, Drake B. Child and adult outcomes of chronic child maltreatment. Pediatrics. 2012;129:839–45.
Smith CA, Ireland TO, Thornberry TP. Adolescent maltreatment and its impact on young adult antisocial behavior. Child Abus Negl. 2005;29:1099–119.
Moffitt TE, Caspi A, Harrington H, Milne BJ. Males on the life-course-persistent and adolescence-limited antisocial pathways: follow-up at age 26 years. Dev Psychopathol. 2002;14:179–207.
Mun EY, Windle M, Schainker LM. A model-based cluster analysis approach to adolescent problem behaviors and young adult outcomes. Dev Psychopathol. 2008;20:291–318.
Maschi T, Hatcher SS, Schwalbe CS, Rosato NS. Mapping the social service pathways of youth to and through the juvenile justice system: a comprehensive review. Child Youth Serv Rev. 2008;30:1376–85.
Barnes JC, Boutwell BB. On the relationship of past to future involvement in crime and delinquency: a behavior genetic analysis. J Crim Justice. 2012;40:94–102.
Garland A, Aarons GA, Brown SA, Wood PA, Hough RL. Diagnostic profiles associated with use of mental health and substance abuse services among high-risk youths. Psychiatr Serv. 2003;54:562–4.
Corrales T, Waterford M, Goodwin-Smith I, Wood L, Yourell T, Ho C. Childhood adversity, sense of belonging and psychosocial outcomes in emerging adulthood: a test of mediated pathways. Child Youth Serv Rev. 2016;63:110–9.
Spies H, Tan S, Davelaar M. De Jeugd Maar Geen Toekomst? Naar Een Effectieve Aanpak Van Sociale Uitsluiting. Amsterdam: SWP; 2016.
Fassaert T, Lauriks S, Van De Weerd S, Theunissen J, Kikkert M, Dekker J, et al. Psychometric properties of the Dutch version of the self-sufficiency matrix (SSM-D). Community Ment Health J. 2014;50:583–90.
Fassaert T, Lauriks S, Van De Weerd S, De Wit M, Buster M. Ontwikkeling en betrouwbaarheid van de Zelfredzaamheid-Matrix. Tijdschr voor Gezondheidswetenschappen. 2013;91:169–77.
Bannink R, Broeren S, Heydelberg J, van’t Klooster E, Raat H. Psychometric properties of self-sufficiency assessment tools in adolescents in vocational education. BMC Psychol. 2015;33:10.
Culhane DP, Gross KS, Parker WD, Poppe B, Sykes E. Accountability, cost-effectiveness, and program performance: progress since 1998. Retrieved from http://repository.upenn.edu/spp_papers/114.
Luijks MJ, Bevaart F, Zijlmans J, van Duin L, Marhe R, Doreleijers TA, et al. A multimodal day treatment program for multi-problem young adults: Study protocol of a randomized controlled trial in clinical practice. Trials. 2017;18:1–15.
Het Kwaliteitskader van de Raad voor de Kinderbescherming. Utrecht; 2013.
McHugh ML. Interrater reliabilty: the kappa statistic. Biochem Medica. 2012;22:276–82.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–74.
Keij I. Standaarddefinitie allochtonen. Index: Cent Bur voor Stat; 2000.
Achenbach TM, Rescorla LA. Manual for the ASEBA adult forms and profiles. Burlington: ASEBA; 2003.
Vanheusden K, van der Ende J, Mulder CL, van Lenthe FJ, Verhulst FC, Mackenbach JP. The use of mental health services among young adults with emotional and behavioural problems: equal use for equal needs? Soc Psychiatry Psychiatr Epidemiol. 2008;43:808–15.
van der Laan AM, Blom M. WODC-Monitor Zelfgerapporteerde Jeugd-criminaliteit—Meting 2005. Den Haag: WODC Memorandum; 2006.
van der Laan AM, Blom M, Kleemans ER. Exploring long-term and short-term risk factors for serious delinquency. Eur J Criminol. 2009;6:419–38.
Bosma A, Asscher J, Van der Laan P, Stams J. Procesevaluatie Tools4U. Amsterdam: Kohnstamm Instituut; 2011.
Collins LM, Lanza ST. Latent Class and Latent Transition Analysis. Balding DJ, Cressie NAC, Fitzmaurice GM, Johnstone IM, Molenberghs G, Scott DW, et al., editors. New Jersey: Wiley; 2010.
Lanza ST, Collins LM, Lemmon DR, Schafer JL. PROC LCA: a SAS procedure for latent class analysis. Struct Equ Model Multidiscip J. 2007;14:671–94.
Celeux G, Soromenho G. An entropy criterion for assessing the number of clusters in a mixture model. J Classif. 1996;13:195–212.
Field A. Discovering statistics using SPSS. 3rd ed. chennai: Sage Publications; 2009.
Raad voor de Kinderbescherming. 2016: ongeveer 35.000 kinderen in aanraking met de RvdK. 2017 https://www.kinderbescherming.nl/actueel/nieuws/2017/04/18/2016-ongeveer-35.000-kinderen-in-aanraking-met-de-rvdk Accessed 2017 Jun 30.
Nederlands Jeugdinstituut. Studie cijfers kindermishandeling. 2016. http://www.nji.nl/Kindermishandeling-Probleemschets-Cijfers.
LeBlanc ML, Bouthillier C. A developmental test of the general deviance syndrome with adjudicated girls and boys using hierarchical confirmatory factor analysis. Crim Behav Ment Heal. 2003;13:81–105.
Henry KL, Huizinga DH. School-related risk and protective factors associated with truancy among urban youth placed at risk. J Prim Prev. 2007;28:505–19.
McCluskey CP, Bynum TS, Patchin JW. Reducing chronic absenteeism: an assessment of an early truancy initiative. Crime Delinq. 2004;50:214–34.
Jessor R, Jessor SL. Problem behavior and psychosocial development: A longitudinal study of youth. San Diego: Academic Press; 1977.
Shonkoff JP, Fisher PA. Rethinking evidence-based practice and two-generation programs to create the future of early childhood policy. Dev Psychopathol. 2013;25:1635–53.
Myers JEB. A short history of child protection in America. Fam Law Q. 2008;42:449–63.
HM Government. Working together to safeguard children. 2015. https://www.gov.uk/government/publications/working-together-to-safeguard-children--2.
Berg T, Vink C. Jeugdzorg in Europa—Lessen over strategieën en zorgsystemen uit Engeland, Duitsland. Utrecht: Noorwegen en Zweden; 2009.
Authors’ contributions
TD and AP are the principal investigators and obtained funding for the study. LD coordinate the record and register research and, together with JZ and ML, the data collection during the study. LD and FB drafted the manuscript with important contributions from CP, ML, JZ, RM, AB, TD, and AP. LD and AB together performed the data analysis. All authors read and approved the final manuscript.
Acknowledgements
The data that support the findings of this study are available from VU University Medical Center but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors reasonable request and with permission of VU University Medical Center. We would like to thank the social welfare agency (Jongerenloket) in Rotterdam, DNK, The Child Care and Protection Service for their cooperation with this study.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The study was performed by the VU University Medical Center Department of Child and Adolescent Psychiatry and approved by the Medical Ethics Review Committee of VU University Medical Center (Registration Number: 2013.422—NL46906.029.13). Participants gave informed consent before voluntary participation after a member of the research team had provided oral information accompanied by written information.
Funding
This research project is funded by De Verre Bergen foundation. De Verre Bergen foundation is a venture philanthropy organization that aims to build a better Rotterdam through substantial investments in innovative, impactful social ventures. The financer is not involved in the design of the study nor the drafting of the manuscript. Furthermore, the financer is not and shall not be involved in the subsequent process of data collection, analysis and interpretation. Contact information: Nanne Boonstra, Parklaan 22, 3016 BB Rotterdam, The Netherlands; Tel: 0031 10 209 2000; E-mail: nboonstra@sdvb.com.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
van Duin, L., Bevaart, F., Paalman, C.H. et al. Child Protection Service interference in childhood and the relation with mental health problems and delinquency in young adulthood: a latent class analysis study. Child Adolesc Psychiatry Ment Health 11, 66 (2017). https://doi.org/10.1186/s13034-017-0205-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13034-017-0205-0