
Abstract
Objective
To examine the relationship between a history of childhood abuse and mental health problems in juveniles who sexually offended (JSOs) over and above general offending behavior.
Methods
A sample of 44 JSOs incarcerated in two juvenile detention centers in the Netherlands between May 2008 and March 2014 were examined for childhood abuse history (Childhood Trauma Questionnaire-Short Form) and mental health problems (Massachusetts Youth Screening Instrument-Version 2). Furthermore, the connection between childhood abuse and mental health problems in JSOs was compared to a sample of 44 propensity score matched juveniles who offended non-sexually (non-JSOs).
Results
In JSOs, sexual abuse was related to anger problems, suicidal ideation, and thought disturbance. These associations were significantly stronger in JSOs than in non-JSOs.
Conclusions
Our results suggest that the relationship between childhood abuse and both internalizing and externalizing mental health problems is of more salience for understanding sexual offending than non-sexual offending, and should, therefore, be an important focus in the assessment and treatment of JSOs.
Similar content being viewed by others

Background
Childhood traumatic experiences are a major societal problem, with detrimental consequences for the victim. There is clear evidence that childhood abuse is related to an increased prevalence of mental health problems (e.g., [1–3]). Moreover, childhood abuse is a risk factor for later offending behavior [4]. Although childhood abuse is highly prevalent in juveniles who have sexually offended (JSOs) (e.g., [5]), little attention has been devoted to the direct relation between childhood abuse and mental health problems in this specific group of offenders. More insight into this relationship could be of great importance for the assessment and treatment of JSOs.
Previous studies showed that childhood abuse is highly prevalent in JSOs. Based on information reported in Seto and Lalumière’s meta-analysis [5], the mean prevalence rate for sexual abuse in JSOs was 36.9%,Footnote 1 42.2% for physical abuse, and 48.1% for emotional abuse/neglect. Moreover, JSOs experienced sexual abuse (d = 0.62), physical abuse (d = 0.19), and emotional abuse/neglect (d = 0.28) more often than juveniles who offended non-sexually (non-JSOs) [5].
One hypothesis to explain the higher prevalence of sexual abuse among JSOs compared to non-JSOs is the sexually abused sexual abuser hypothesis (for detailed information see: [5, 6]). According to this hypothesis, juveniles with a history of sexual abuse are at increased risk to engage in sexual offending behavior. Meta-analyses of both adult and juvenile sex offender samples found support for this hypothesis, as sexual abuse histories were relatively more prevalent in offenders who had committed a sex offense than among those who had not [5, 6].
Several explanations have been discussed for the relationship between sexual victimization and later sexual offending. First, sexual abuse victims may be at increased risk for sexual offending vis-à-vis learning (e.g., modeling of their abuser’s behavior) and adoption of positive attitude and beliefs towards sexual behavior between children and adults [7]. Second, sexual abuse may contribute to abnormal or deviant psychosexual development, which in turn may increase risk for sexual offending behavior [6]. Third, the relationship between sexual abuse and sexual offending behavior could be caused indirectly through other third variables, such as mental health problems [6].
With regard to this latter explanation, childhood abuse is related to various mental health problems, including substance abuse, depression, suicidal ideation, anxiety and Post-Traumatic Stress Disorder [8–12]. Because research suggests that a history of childhood abuse is more prevalent among JSOs than non-JSOs [5, 13], one might expect JSOs to have more mental health problems than non-JSOs. In general, JSOs report more internalizing problems (social isolation, anxiety, low self-esteem, thought disturbance) and atypical sexual interests, but fewer externalizing problems, including substance abuse problems, than non-JSOs [5, 13–15]. Hence, it could be hypothesized that the connection between childhood abuse and mental health problems differs among juveniles with and without a history of perpetrating sex offenses.
The aim of the current study is to examine the relationship between childhood abuse and mental health problems in sexual offending behavior, over and above general offending behavior. To do so, we compared the association between childhood abuse and mental health problems in JSOs and non-JSOs. Based on the extant research literature, we hypothesized that there would be a stronger relationship between childhood abuse, especially sexual abuse, and internalizing mental health problems among youth with a history of sexual offending than among youth whose offending histories did not include sexual offenses.
Methods
Participants
The sample included 44 male juveniles who sexually offended (i.e., JSOs) and 44 propensity score matched male juvenile non-sexual offenders (i.e., non-JSOs) incarcerated in two juvenile detention centers in the Netherlands between May 2008 and March 2014. Youth were classified as JSO if their official judicial record showed at least one conviction for a sexual offense (n = 17), if at least one index offense was a sexual offense (n = 26), or if they reported during the assessment that they ever engaged in sexual behavior against someone else’s will (n = 6). Non-JSOs were suspected or convicted of violent (e.g., manslaughter, armed robbery) and/or non-violent (e.g., theft, drug dealing) crimes, but did not have a history of sexual offense perpetration. JSOs and non-JSOs were propensity score matched on age and ethnicity. The age range of the total sample was between 13 and 24 years (33% of the offenders were 18 years or older, and 18% were 19 years or older). The mean age of JSOs and non-JSOs was similar [JSOs: 17.0 (SD = 2.0), non-JSOs: 17.7 (SD = 1.8); t = 1.8; p = .97], as was the proportion of participants who were native Dutch (JSOs: 40.9%, non-JSOs: 22.7%; χ2 = 3.4, p = .11).
Procedure
Assessment was part of a standardized self-report mental health screening procedure in the juvenile detention centers used for clinical purposes. Master students and test assistants with a Master’s degree trained by clinically experienced researchers performed the comprehensive assessments. Juveniles and their parents were informed that all information was also used for scientific research after encryption. The relevant institutional review and scientific boards of the juvenile detention centers approved the study and procedure (for more details, see: [16]).
Instruments
Childhood Trauma Questionnaire-Short Form (CTQ-SF)
The CTQ-SF [17, 18] is a 28-item self-report inventory for juveniles and adults (from age 12 and up) that provide brief, reliable, and valid screening for histories of abuse and neglect [18, 19]. It inquires about five types of maltreatment: (1) emotional abuse (e.g., “I thought that my parents wished I had never been born”), (2) physical abuse (e.g., “People in my family hit me so hard that it left me with bruises or marks”), (3) sexual abuse (e.g., “Someone tried to touch me in a sexual way or tried to make me touch them”), (4) emotional neglect (e.g., “There was someone in my family who helped me feel that I was important or special”) and (5) physical neglect (e.g., “I had to wear dirty clothes”). Three items screen for false-negative trauma reports (e.g., “There was nothing I wanted to change about my family”). Participants are asked to rate whether each item is (1) never, (2) rarely, (3) sometimes, (4) often, or (5) very often true. In the Dutch translation [20], one question about molestation was removed due to low correlation with the sexual abuse subscale and high correlation with physical abuse subscale. Translation of the word “molestation” into Dutch was not linked to sexual abuse per se [21]. Internal consistency of the Dutch CTQ-SF ranged from .89 (emotional abuse) to .95 (sexual abuse), with the exception of physical neglect (.63) [21].
Massachusetts Youth Screening Instrument-Version 2 (MAYSI-2)
The MAYSI-2 [22, 23] is a brief screening tool to identify youth who are at immediate risk for suicide and increased mental health and substance use needs. Although the MAYSI-2 has been developed for juveniles between the age of 12 and 17, it has been suggested that it can be used also with older youths as long as the results are interpreted carefully [24]. It is one of the most widely used screening instruments for mental health problems in the United States [22, 23], and has been implemented by the Dutch Ministry of Justice as part of the standardized mental health screening at entry to all juvenile justice detention centers in the Netherlands. Based on factor analyses, the MAYSI-2 contains seven scales: Alcohol/Drug Use, Angry-Irritable, Anxious-Depressed, Somatic Complaints, Suicide Ideation, Thought Disturbance, and Traumatic Experiences [22, 23, 25, 26]. All scales except for the Traumatic Experiences scale have two cut-off points. The caution cut-off indicates that the score of the youth may have clinical significance; the warning cut-off indicates an exceptionally high score compared to other juveniles in juvenile justice institutions.
The MAYSI-2 has acceptable to good internal consistency for the Alcohol/Drug Use, Angry-Irritable, Anxious-Depressed, Somatic Complaints and Suicide Ideation scales, and poor to acceptable internal consistency for the Thought Disturbance and Traumatic Experiences scale [22, 23, 25, 26]. Good concurrent validity has been demonstrated [23, 26, 28–32].
Statistical analysis
Data were analyzed using International Business Machines Corporation Statistical Package for Social Sciences, version 19 (IBM SPSS 19). The level of significance was set at .01 in order to account for Type I error inflation due to multiple testing. First, differences in childhood trauma scores and mental health scores between JSOs and non-JSOs were examined using t-tests. Second, as our data were not normally distributed, we used Spearman Rho Correlations to examine the relation between childhood abuse and mental health problems in JSOs and general offending juveniles. Third, we compared the strength of the relationship between childhood abuse and mental health problems in JSOs and non-JSOs by calculating the difference between the two independent correlation coefficients using software available from http://quantpsy.org [33]. Although the Fischer r-to-z transformation is a method usually applied to Pearson correlation coefficients, Myers and Sirois [34] showed that this approach performed best in terms of control of Type I error when compared to other strategies. To interpret the magnitude of the correlation coefficients, we followed Cohen’s [35] benchmark of small (r = .10), medium (r = .30) and large (r = .50).
Results
In Table 1, the descriptive statistics for the CTQ-SF and the MAYSI-2 are presented separately for JSOs and non-JSOs. On the CTQ-SF, both JSOs and non-JSOs reported the highest mean scores on the emotional neglect scale and the lowest mean scores on the sexual abuse scale. The caution cut-off scores of the MAYSI-2 indicate that problems with thought disturbance, depression and anxiety, and somatic complaints are highly prevalent in JSOs. A high number of non-JSOs manifested depressed anxious problems and alcohol/drug use problems. With respect to warning cut-off scores, a high number of JSOs reported problems with alcohol/drug use and thought disturbance. Alcohol/drug use problems also were highly prevalent in non-JSOs. There were no significant differences between JSOs and non-JSOs in reported traumatic experiences (CTQ-SF) or mental health problems (MAYSI-2) (see Table 1).
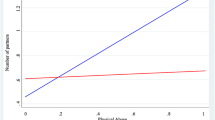
In Table 2, correlations between the scales of the CTQ-SF and the MAYSI-2 are presented for JSOs and non-JSOs. For JSOs, 6 of the 30 correlations were medium or large in magnitude [33], whereas this was the case for only 2 of the 30 correlations for non-JSOs. In JSOs, there were significant and large correlations between sexual abuse and anger problems, suicidal ideation, and thought disturbance, as well as between physical neglect and suicidal ideation. Medium correlations were found for emotional abuse and depressed anxious problems, and the Traumatic Experiences scale of the MAYSI-2. In non-JSOs, medium correlations were found for emotional abuse and the Traumatic Experiences scale of the MAYSI-2, and emotional neglect and suicidal ideation. In comparisons of the differences between the two independent correlations in JSOs and non-JSOs, significantly stronger associations were observed among JSOs for the relationship between sexual abuse and anger problems, suicidal ideation, and thought disturbance.
Discussion
The aim of the current study was to examine the relationship between childhood abuse and mental health problems in sexual offending behavior, over and above offending behavior in general. We found a stronger relationship between childhood sexual abuse and anger problems, suicidal ideation, and thought disturbance in JSOs than in non-JSOs.
In contrast to previous studies [e.g., 5], we did not observe significant differences in history of childhood abuse and current mental health problems between JSOs and non-JSOs. However, our study only included youths in juvenile detention centers, whereas the meta-analysis of Seto and Lalumière [5] included studies with youths sampled throughout different processing points in the juvenile justice system. It has been assumed that the prevalence of mental health problems escalates with increased penetration into “deeper” levels of the juvenile justice system [36]. Based on prevalence studies of mental health problems in juvenile arrestees [37], juveniles brought to court [38], juveniles forensically assessed at the request of the court [39], and incarcerated juveniles [40], Doreleijers [36] hypothesized that the prevalence of mental health problems in youth increases the “deeper” they go into the juvenile justice system. For example, 90% of the incarcerated juveniles reported at least one mental disorder [40]. With such high prevalence rates, statistically significant differences in mental health problems, as well as histories of childhood abuse, become more difficult to identify.
Moreover, it can be argued that, given the objective of the present study, the absence of significant differences between JSOs and non-JSOs in childhood abuse and mental health problems is an advantage, as the relationship of childhood sexual abuse and mental health problems in JSOs compared to non-JSOs is not biased by pre-existing differences between both groups. In line with our hypothesis, we found a relationship between sexual abuse and internalizing mental health problems (i.e., suicidal ideation and thought disturbance) in JSOs, which we did not find in non-JSOs. In addition, we also observed a relationship between sexual abuse in JSOs and externalizing mental health problems (i.e., angry-irritable problems). These results suggest that there is a stronger relation between the degree of sexual abuse and both internalizing and externalizing mental health symptoms in JSOs than there is in non-JSOs.
With regard to the sexually abused sexual abuser hypothesis, we did not find significant differences in experiences of childhood sexual abuse between JSOs and non-JSOs (in contrast to [5, 6]). However, we did find a stronger relationship between childhood sexual abuse and both internalizing and externalizing mental health problems in JSOs than in non-JSOs, indicating that the link between childhood sexual abuse and sexual antisocial behavior might be influenced by mental health problems.
In addition, the relationship between internalizing mental health problems and sexual offending behavior remains incompletely understood. On one hand, internalizing mental health problems may be the result of previously existing problems with sexuality and/or history of sexual abuse. On the other hand, internalizing mental health problems could manifest as a reaction to perpetration of sexual offenses [41, 42]. Hence, as no conclusions can be drawn regarding the causal relationship between internalizing mental health problems and occurrence of sexual offending behavior, future research should investigate the temporal ordering and related causal nexus of internalizing conditions and sexual offense perpetration.
Limitations
Findings of this study must be interpreted in the context of some limitations. First, previous research showed that JSOs constitute a heterogeneous group with differences in childhood abuse and mental health problems [43–45]. Especially JSOs with child victims, when compared to JSOs with adolescent/adult victims, show more childhood abuse, especially sexual abuse, and more mental health problems. We did not examine subgroups given that our sample of JSOs constituted only 44 offenders. Second, we did not assess the extent, frequency and duration of childhood abuse, which also might have influenced our results. Third, the juvenile detention centers in the current study only admitted males. Therefore, our results cannot be generalized to female offender populations. The fourth limitation refers to the reliability of the results. The CTQ-SF and the MAYSI-2 are both self-report instruments. Therefore, our results may have been biased due to social desirability (e.g., on one hand it is conceivable that a history of maltreatment is kept a secret because of shame or loyalty to the perpetrator, but on the other hand it can be suggested that a history of maltreatment is over-reported to gain justification and/or compassion for one’s behavior). Furthermore, as youths were told that their answers would be used for clinical purposes and for evaluation of their interventions, the (lack of) confidentiality could have affected our results. Moreover, retrospective recall bias [46] also may have played a role in the over- or under-reporting of perceived maltreatment; it has been suggested that more recent maltreatment is more accurately recalled than more distal maltreatment. In addition, amplification of the negativity of the maltreatment (e.g., recall of own abuse history when charged with perpetration of a sexual offense) also could lead to over-reporting of maltreatment [47]. Fifth, the internal consistency of the MAYSI-2 scales Thought Disturbance and Traumatic Experiences have been found to be poor to acceptable [22, 23, 25, 27]. Although lower consistency may be explained by the broadness of the constructs measured, this should be taken into account when interpreting the results. Sixth, by lowering the level of statistical significance to .01 we reduced the probability of making a Type I error. As a result, however, the probability of making Type II errors increased (and power reduced), which should also be taken into account. Seventh, the current study was cross-sectional and, therefore, causal relationships between childhood abuse and mental health problems could not be established. Longitudinal studies are needed to establish this relationship. Finally, beyond mental health problems, other variables could have influenced the relationship between childhood (sexual) abuse sexual offending behavior, such as genetic predisposition, various family factors, and peer influences.
Implications
Our results suggest that if a youth with a history of perpetrating a sexual offence reports mental health symptoms, especially internalizing mental health problems such as suicidal ideation and thought disturbance or externalizing mental health problems such as angry-irritable problems, there is stronger reason to suspect these symptoms are related to childhood abuse or neglect, especially sexual abuse, than if a youth without a history of sexual offending reports similar symptoms. As internalizing mental health problems are harder to detect than externalizing mental health problems, it is of great importance to assess both internalizing and externalizing mental health problems in JSOs at entry to juvenile detention centers. Furthermore, as we found a stronger relationship between childhood sexual abuse and both internalizing and externalizing mental health problems in JSOs than in non-JSOs, our results suggest the need for a different focus for treatment of JSOs and non-JSOs. For JSOs, perhaps the treatment needs to focus on dealing with the childhood sexual abuse (e.g., trauma-based therapy) if this is determined to be a key risk factor for future offending for that particular youth. Finally, as there is evidence that the relationship between sexual abuse and sexual offending behavior could be caused indirectly through mental health problems, one aspect of sexual violence risk management among juveniles who have experienced sexual abuse could comprise treatment with a focus on healthy development and behaviors in order to prevent sexual offending behavior.
Notes
We calculated the mean prevalence rates using information in Table 7 in Seto and Lalumière [5, p. 546]. First, we converted the reported percentages of experienced sexual abuse into proportions. Second, we multiplied the proportion of experienced sexual abuse with the number of adolescent sex offenders per study (i.e., estimate of the number of adolescent sex offenders who experienced sexual abuse). Third, we computed the total number of adolescent sex offenders and the total of the newly created variable proportion experienced sexual abuse*number of adolescent sex offenders (i.e., estimate of the total number of adolescent sex offenders who experienced sexual abuse). Fourth, we divided the total proportion experienced sexual abuse*number of adolescent sex offenders (i.e., estimate of the total number of adolescent sex offenders who experienced sexual abuse) by the total number of adolescent sex offenders. The mean prevalence rates for physical abuse and emotional abuse/neglect were calculated using the same method.
References
Kilpatrick DG, Acierno R, Saunders B, Resnick HS, Best CL, Schnurr PP. Risk factors for adolescent substance abuse and dependence: data from a national sample. J Consult Clin Psychol. 2000;68(1):19–30.
Ruchkin V, Henrich CC, Jones SM, Vermeiren R, Schwab-Stone M. Violence exposure and psychopathology in urban youth: the mediating role of posttraumatic stress. J Abnorm Child Psychol. 2007;35:578–93.
Wasserman GA, McReynolds LS. Contributors to traumatic exposure and posttraumatic stress disorder in juvenile justice youths. J Trauma Stress. 2011;24(4):422–9.
Watts SJ, McNulty TL. Childhood abuse and criminal behavior: testing a general strain theory model. J Interpers Violence. 2013;28:3023–40. doi:10.1177/0886260513488696.
Seto MC, Lalumière ML. What is so special about male adolescent sexual offending? A review and test of explanations through meta-analysis. Psychol Bull. 2010;136(4):526–75.
Jespersen AF, Lalumière ML, Seto MC. Sexual abuse history among adult sex offenders and non-sex offenders: a meta-analysis. Child Abuse Negl. 2009;33:179–92.
Burton DL. Male adolescents: sexual victimization and subsequent sexual abuse. Child Adolesc Soc Work J. 2003;20(4):277–96.
Brown J, Cohen P, Johnson JG, Smailes EM. Childhood abuse and neglect: specificity of effects of adolescent and young adult depression and suicidality. J Am Acad Child Adolesc Psychiatry. 1999;38(12):1490–6.
Chartier MJ, Walker JR, Naimark B. Health risk behaviors and mental health problems as mediators of the relationship between childhood abuse and adult health. Am J Public Health. 2009;99(5):847–54.
Collishaw S, Pickles A, Messer J, Rutter M, Shaerer C, Maughan B. Resilience to adult psychopathology following childhood maltreatment: evidence from a community sample. Child Abuse Negl. 2007;31(3):211–29.
Grilo CM, Sanislow C, Fehon DC, Martino S, McGlashan TH. Psychological and behavioral functioning in adolescent psychiatric inpatients who report histories of childhood abuse. Am J Psychiatry. 1999;156:538–43.
King DC, Abram KM, Romero EG, Washburn JJ, Welty LJ, Teplin LA. Childhood maltreatment and psychiatric disorders among detained youths. Psychiatr Serv. 2011;62(12):1430–8.
Van Wijk A, Vermeiren R, Loeber R, ’t Hart-Kerkhoffs L, Doreleijers T, Bullens R. Juvenile sex offenders compared to non-sex offenders: a review of the literature 1995–2005. Trauma Violence Abuse. 2006;7:227–43.
DeLisi M, Drury A, Kosloski A, Caudill J, Conis P, Anderson C, Vaughn M, Beaver K. The cycle of violence behind bars: traumatization and institutional misconduct among juvenile delinquents in confinement. Youth Violence Juv Justice. 2010;8(2):107–21.
Van Wijk APh, Blokland AAJ, Duits N, Vermeiren R, Harkink J. Relating psychiatric disorders, offender and offence characteristics in a sample of adolescent sex offenders and non-sex offenders. Crim Behav Mental Health. 2007;17:15–30.
Vahl P, Colins OF, Lodewijks HPB, Markus MT, Dorelelijers TAH, Vermeiren RRJM. Psychopatic-like traits in detained adolescents: clinical usefulness of self-report. Eur Child Adolesc Psychiatry. 2013. doi:10.1007/s00787-013-0497-4.
Bernstein DP, Fink L. Childhood trauma questionnaire: a retrospective self-report: manual. San Antonio: Pearson, Psychological Corporation; 1998.
Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, Stokes J, Handelsman L, Medrano M, Desmond D, Zule W. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Negl. 2003;27:169–90.
Bernstein DP, Ahluvalia T, Pogge D, Handelsman L. Validity of the childhood trauma questionnaire in an adolescent psychiatric population. J Am Acad Child Adolesc Psychiatry. 1997;36(3):340–8.
Arntz A, Wessel I. Jeugd trauma vragenlijst [Dutch version of the childhood trauma questionnaire]. The Netherlands: Author; 1996.
Thombs BD, Bernstein DP, Lobbestael J, Arntz A. A validation study of the Dutch Childhood Trauma Questionnaire-Short Form: factor structure, reliability, and known-groups validity. Child Abuse Negl. 2009;33:518–23.
Grisso T, Barnum R. Massachusetts youth screening instrument-version 2: user’s manual and technical report. Sarasota, FL: Professional Resource Press; 2006.
Grisso T, Barnum R, Fletcher KE, Cauffman E, Peuschold D. Massachusetts youth screening instrument for mental health needs of juvenile justice youths. J Am Acad Child Adolesc Psychiatry. 2001;40(5):541–8.
Grisso T, Fusco S, Paiva-Salisbury M, Perrault R, Williams V, Barnum R. The Massachusetts youth screening instrument-version 2 (MAYSI-2): comprehensive research review. Worcester, MA: University of Massachusetts Medical School; 2012.
Archer RP, Stredny RV, Mason JA, Arnau RC. An examination and replication of the psychometric properties of the Massachusetts Young Screening Instrument-Second Edition (MAYSI-2) among adolescents in detention settings. Assessment. 2004;11(4):290–302.
Grisso T, Fusco S, Paiva-Salisbury M, Perrauot R, Williams V, Barnum R. The Massachusetts youth screening instrument-version 2 (MAYSI-2): comprehensive research review. Worcester, MA: University of Massachusetts Medical School. www.nysap.us; 2012.
Hayes MA, McReynolds LS, Wasserman GA. Paper and voice MAYSI-2. Format comparability and concordance with the voice DISC-IV. Assessment. 2005;12(4):395–403.
Archer RP, Simonds-Bisbee EC, Spiegel DR, Handel RW, Elkins DE. Validity of the Massachusetts Youth Screening Instrument-2 (MAYSI-2) Scales in juvenile justice settings. J Pers Assess. 2010;92(4):337–48.
Butler MA, Loney BR, Kistner J. The Massachusetts Youth Screening Instrument as a predictor of institutional maladjustment in severe male juvenile offenders. Crim Justice Behav. 2007;35(4):476–92.
Caldwell R, Sturges S, Silver N. Home versus school environments and their influences on the affective and behavioral states of African-American, Hispanic, and Caucasian juvenile offenders. J Child Fam Stud. 2006;16:125–38. doi:10.1007/s10826-006-9073-6.
Chapman JF, Ford JD. Relationships between suicide risk, trauma experiences, and substance use among juvenile detainees. Arch Suicide Res. 2005;12(1):50–61.
Tille J, Rose J. Emotional and behavioral problems of 13-to-18-year-old incarcerated female first-time offenders and recidivists. Youth Violence Juv Justice. 2007;5:426–35. doi:10.1177/1541204007300355.
Preacher KJ. Calculation for the test of the difference between two independent correlation coefficients [Computer software]; 2002. http://quantpsy.org.
Myers L, Sirois MJ. Spearman correlation coefficients, differences between. Wiley StatsRef: Statistics Reference Online; 2006.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New York, NY: Academic Press; 1988.
Doreleijers T. To crazy for words? [Te gek voor woorden?]. In: Borst M, Doreleijers T, Maas B, Schaap R, Taghon G, van Velthooven B, editors. Oppositional and deviant behaviour in secondary education [Oppositioneel en opstandig gedrag in het voortgezet onderwijs]. Garant: Antwerpen–Apeldoorn; 2008. p. 39–66.
Scholte EM. Youths, police and care. Preventive care for juveniles with psychosocial problems [Jeugd, politie en hulpverlening. Preventieve hulp aan jongeren met psychosociale problemem.]. Leuven/Amersfoort: Acco; 1988.
Doreleijers ThAH. Assessment between juvenile justice and care [Diagnostiek tussen jeugdstrafrecht en hulpverlening.]. Gouda: Quint; 1995.
Duits N. Forensic child and adolescent psychiatry [Forensische kinder- en jeugdpsychiatrie]. In: Duits N, Bartels JAC, Gunning WB, editors. Adolescent psychiatry and law [Jeugdpsychiatrie en recht.]. Assen: Van Gorcum; 1997. p. 99–106.
Vreugdenhil J. Psychiatric disorders among incarcerated male adolescents in the Netherlands. Amsterdam: VU University Medical Center Amsterdam; 2003.
Teplin LA, Abram KM, McClelland GM, Dulcan MK, Mericle AA. Psychiatric disorders in youth in juvenile detention. Arch Gen Psychiatry. 2002;59:1133–43.
Vermeiren R. Psychopathology and delinquency in adolescents: a descriptive and developmental perspective. Clin Psychol Rev. 2003;23:277–318.
‘t Hart-Kerkhoffs LA, Jansen LM, Doreleijers TA, Vermeiren R, Minderaa RB, Hartman CA. Autism spectrum disorder symptoms in juvenile suspects of sex offenses. J Clin Psychiatry. 2009;70:266–72.
Hunter JA, Figueredo AJ, Malamuth NM, Becker JV. Juvenile sex offenders: toward the development of a typology. Sex Abuse. 2003;15:27–48.
Hunter JA, Hazelwood RR, Slesinger D. Juvenile-perpetrated sex crimes: patterns of offending and predictors of violence. J Fam Violence. 2000;15(1):82–93.
Widom CS. Does violence beget violence? A critical examination of the literature. Psychol Bull. 1989;106(1):3–28.
Aylwin AS, Studer LH, Reddon JR, Clelland SR. Abuse prevalence and victim gender among adult and adolescent child molesters. Int J Law Psychiatry. 2003;26:179–90.
Authors’ contributions
All listed authors have key responsibility for the material in the article. OC, EM, PV and RV requested and delivered the data that were collected in the two Youth Detention Centers (YDCs). CB and LG analyzed the data and interpreted the data in collaboration with TG, LJ, TD and RV. All authors have been involved in drafting the manuscript or revising it critically for important intellectual content and have given final approval of the version to be published. All authors read and approved the final manuscript.
Acknowledgements
This work was supported by: the Foundation “De Drie Lichten”, Hilversum, The Netherlands; Police Science and Research, Apeldoorn, The Netherlands; and the Dokter Wittenberg Foundation, Deventer, The Netherlands. There was complete freedom to direct the analysis and the reporting, without influence from the sponsor. There was no editorial direction or censorship from the sponsor.
Competing interests
TG is an author of the MAYSI-2 but does not receive financial remuneration from sales of the tool. Furthermore, the authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Boonmann, C., Grisso, T., Guy, L.S. et al. Childhood traumatic experiences and mental health problems in sexually offending and non-sexually offending juveniles. Child Adolesc Psychiatry Ment Health 10, 45 (2016). https://doi.org/10.1186/s13034-016-0127-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13034-016-0127-2