
Abstract
Background
Dystroglycanopathy (α-DG) is a relatively common, clinically and genetically heterogeneous category of congenital forms of muscular dystrophy (CMD) and limb-girdle muscular dystrophy (LGMD) associated with hypoglycosylated α-dystroglycan. To date, mutations in at least 19 genes have been associated with α-DG. One of them, GMPPB, encoding the guanosine-diphosphate-mannose (GDP-mannose) pyrophosphorylase B protein, has recently been associated with a wide clinical spectrum ranging from severe Walker-Warburg syndrome to pseudo-metabolic myopathy and even congenital myasthenic syndromes.
We re-sequenced the full set of known disease genes in 73 Italian patients with evidence of either reduced or nearly absent α-dystroglycan to assess genotype-phenotype correlations in this cohort. We used innovative bioinformatic tools to calculate the effects of all described GMPPB mutations on protein function and attempted to correlate them with phenotypic expressions.
Results
We identified 13 additional cases from 12 families and defined seven novel mutations. Patients displayed variable phenotypes including less typical pictures, ranging from asymptomatic hyperCKemia, to arthrogryposis and congenital clubfoot at birth, and also showed neurodevelopmental comorbidities, such as seizures and ataxic gait, as well as autism-spectrum disorder, which is seldom described in clinical reports of dystroglycanopathies. We also demonstrated that few mutations recur in the Italian GMPPB-mutated population and that alterations of protein stability are the main effects of GMPPB missense variants.
Conclusion
This work adds to the data on genotype-phenotype correlations in α-DG and offers new bionformatic tools to provide the conceptual framework needed to understand the complexity of these disorders.
Similar content being viewed by others

Background
Muscular dystrophies with evidence of reduced glycosylation of the transmembrane glycoprotein α-dystroglycan on skeletal muscle biopsy [1] are collectively termed α-dystroglycanopathy (α-DG) [2,3,4], and they constitute a clinically and genetically heterogeneous group of autosomal recessive muscular dystrophies with variable neurological and ophthalmic involvement.
The phenotypic severity of α-DG patients is extremely variable. At the most severe end of the clinical spectrum we find Walker-Warburg syndrome (WWS), muscle-eye-brain disease and Fukuyama congenital muscular dystrophy. These conditions are characterized by congenital muscular dystrophy (CMD) and severe structural brain and eye abnormalities, leading to early infantile death in WWS [5]. Conversely, individuals at the mildest end of the clinical spectrum may present, sometimes in adulthood, with limb-girdle muscular dystrophy (LGMD), and without associated brain or eye involvement [6].
Mutations in six genes (POMT1, POMT2, POGnT1, FKRP, FKTN, and LARGE) are by far the most common in large Italian and UK cohorts ascertained by low skeletal muscle expression of α-dystroglycan [7, 8], but they account for only about 50% of cases, leaving the rest without a molecular diagnosis. The advent of next-generation sequencing (NGS) methodologies has rapidly expanded the number of α-DG-related genes and subsequently resulted in an expansion of the clinical spectrum observed in affected children and adults [9, 10].
To date, mutations in 19 genes coding for dystroglycan itself or more frequently, for glycosyltransferases and accessory proteins involved in the post-translational modification of α-dystroglycan, are documented to be responsible for the different forms of α-DG. One of them, GMPPB, coding for the guanosine-diphosphate-mannose (GDP-mannose) pyrophosphorylase B protein, seems to be particularly frequent and is associated with a wide spectrum of muscle weakness, ranging from WWS to a mild form of adult-onset LGMD overlapping with different congenital myasthenic syndromes (CMSs) [11,12,13]. More recently pseudo-metabolic features have been described in few patients [14, 15]. Overall, about 81 GMPPB-mutated patients have been described worldwide: 56 with LGMD or overlapping LGMD-CMS phenotypes and the rest presenting features of CMD. To assess the relative frequency of GMPPB variants and contribute to the definition of the associated clinical manifestations, we systematically screened a large Italian population of α-DG patients for mutations. We used new bioinformatics tools to assess how mutations found in this study may affect protein function. We then combined the data from available families to determine mutation frequencies in relation to clinical severity, and thus establish more precise genotype-phenotype correlations.
Methods
This study was approved by the ethics committees of our institutions. The patients were recruited after written informed consent that had been obtained in accordance with national regulations.
All the cases are part of a multicenter study that aims to improve molecular characterization of presently undefined forms of CMD associated with defective glycosylation of α-dystroglycan. For the present work, we collected all genetically undefined patients with low α-dystroglycan levels currently followed at any of the tertiary care centers for pediatric and adult neuromuscular disorders belonging to the Italian CMD network. Cases with milder phenotypes, and a possible diagnosis of LGMD or LGMD-CMS, were also investigated.
We selected, from the overall network population, 105 patients with muscle biopsy-confirmed low α-dystroglycan expression. Prior to our molecular investigations, two expert co-authors (C.F., A.R.) blindly reviewed these patients’ histological and immunohistochemical features. On the basis of their findings, 32 patients, with a reduction of α-dystroglycan likely unrelated to glycosylation defects, or no reduction at all, were excluded. Thus, our study included 73 patients fully meeting the diagnostic criteria for dystroglycanopathy described elsewhere [9].
In this work, past medical history and clinical information, as well as neurophysiological, brain MRI and myoimaging (available only in two patients) are described for the 13 patients in whom we identified bi-allelic mutations in GMPPB. Patients who showed a significant delay in motor abilities and late acquisition of walking (> 24 months) were classified as affected by CMD, whereas those in whom overt clinical manifestations appeared later, as described elsewhere [16], were deemed to present with LGMD. Clinical subcategories of CMD were defined as others have done [17]. Whenever possible patients have since been reassessed and submitted to a detailed clinical re-examination.
Molecular genetic analyses were carried out in all 73 patients and, when available, in their parents and siblings. Genomic DNA was purified from whole blood using standard methodologies and the coding regions of 93 genes linked to CMD, LGMD or related diseases were investigated in a single tube using Dystroplex, an extended NGS testing panel covering at high depth the tested genes and described elsewhere [15, 18]. In all the cases, sequencing was performed with Illumina technology and standard bioinformatics pipelines were applied for quality control, mapping, variant calling and annotation. Publicly available databases (HGMD: http://www.hgmd.cf.ac.uk/ac/index.php; LOVD: http://www.dmd.nl/; 1000G database: http://www.1000genomes.org/; dbSNP database: http://www.ncbi.nlm.nih.gov/SNP/; Sequencing Initiative Suomi (SISu): www.sisuproject.fi; gnomAD; http://gnomad.broadinstitute.org/; ExAC: http://exac.broadinstitute.org/ and EVS: http://evs.gs.washington.edu/EVS/) (last access December 2017) were interrogated to identify previously reported variants and also to determine the frequency of the novel variants observed. The pathogenicity assessment of the target variant was performed according to the guidelines published by the American College of Medical Genetics for the interpretation of sequence variants [19]. Standard in silico tools (Polyphen: http://genetics.bwh.harvard.edu/pph2/; SIFT: sift.jcvi.org/; UMD-Predictor: http://umd-predictor.eu/analysis.php and Mutation taster: http://www.mutationtaster.org/) were used to assess the deleteriousness of missense mutations.
A three-dimensional model of human GMPPB was obtained using a combination of threading and homology modeling methods [20]. The quality of predicted models was assessed using the Qmean server [21] and energy minimization of protein models was carried out using the 3DRefine web server [22]. The effects of GMPPB missense mutations on protein stability and the change in thermodynamic folding stability (the difference in Gibbs free energy between wild-type and mutant, ΔΔG) were calculated using FoldX [23], an algorithm that uses an empirical force field to evaluate the effect of mutations on protein stability. The calculated free energy differences (ΔΔG) [24] indicate the change in structural stability, with negative values indicating amino acid substitutions that tend to increase the thermodynamic structural rigidity of the proteins, and positive values indicating variants that tend to destabilize proteins. The RepairPDB function was applied to the GMPPB wild-type structure before running the BuildModel function of FoldX, and nine independent runs were carried out for each mutation. The prediction error of FoldX is approximately 0.5 kcal/mol, therefore changes in that range are insignificant. UCSF Chimera software (version 1.11) [25] was used for molecular graphics and GraphPad Prism was used for data analysis and curve fitting.
Western blotting (WB) was undertaken as described [26] on a limited number of samples (P1, P2, P3, P6, and P7), depending on material availability. Mouse monoclonal antibodies used on blots were to β-dystroglycan (NCL-b-DG, Leica Biosystems) and laminin α2 (MAb 1922, Chemicon). Western blots were visualized using the Pierce Supersignal detection system according to the manufacturer’s directions. The density of the myosin heavy chain (MHC) band on the Coomassie blue stained, post-blotted gel was a marker for protein loading.
Results
Thirteen patients (8 men and 5 women, age range at last examination 20 months–74 years) from a cohort of 73 Italian α-DG cases showed two predictably pathogenic mutations in GMPPB. The patients’ clinical data are summarized in Table 1. Patient P6 has already been described in detail elsewhere [15]. Patients 9 and 10 are uncle and nephew; the remaining patients are unrelated.
Five patients (P1–P5) presented onset at birth or in the first year of life, and three (P6, P7, P11) during childhood. The other five had adult onset of their muscle weakness (> 18 years). All 13 patients, albeit to different degrees, presented proximal weakness both of the shoulder and the pelvic girdle. Contractures and scoliosis were part of the picture in 4/13 cases, and two patients with congenital onset (P3 and P4) displayed arthrogryposis. Generalized or focal epilepsy (both tonic-clonic and focal seizures with impaired awareness and oromasticatory automatisms) was seen in all the patients with congenital onset, and in one case with childhood onset (P6). All the patients with congenital onset showed intellectual disability and were unable to produce full sentences; P1 has a diagnosis of autism spectrum disorder. Two patients with congenital onset (P2 and P4) showed bilateral cataracts. One case (P1) displayed nystagmus and inward strabismus, with reduction of lateral movement, and upgaze palsy. Two of the LGMD patients (P6 and P7) displayed exercise intolerance and four (P8, P11, P12, P13) easy fatigability; anyway only P8 received pharmacological treatment showing a partial response to pyridostigmine. No respiratory or cardiac involvement was found in this cohort, except for slight heart conduction impairment in three patients (one of whom [P6] carried a diagnosis of Wolf–Parkinson–White syndrome).
The disease was usually progressive over time, however most of the patients who achieved ambulation were still ambulant at the time of diagnosis.
Serum CK levels were increased (ranging from 316 to 38,650 UI/L); muscle biopsy showed features of a muscular dystrophy with abnormal variation in fiber size, necrosis and fibrosis, and in two cases (P5 and P6) it highlighted a myolitic process. Immunohistochemistry with the IIH6 antibody revealed variable degrees of hypoglycosylation of α-dystroglycan. Electromyography was normal in some cases, and otherwise showed mild to moderate myopathic changes. Repetitive nerve stimulation was performed in three LGMD patients (P6, P8 and P13), and only in P8 revealed findings consistent with abnormal neuromuscular transmission in proximal muscles. Brain MRI was available in 6 patients (P1-P6) and showed features previously observed in published GMPPB-mutated patients (Table 1). Muscle MRI was available only in two patients (P1 and P6): the first one, with a CMD phenotype, presented a prevalent involvement of vastus lateralis at thigh level and minimal involvement of soleus at the calves. The second patient with a LGMD phenotype showed minimal involvement of adductor magnus, semimebranosus, semitendinosus and sartorius muscles at thigh level, whereas revealed a mild fatty streaking in soleus and peroneal muscles at calf level.
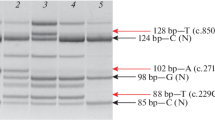
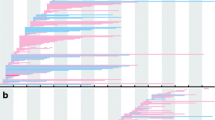
The 13 patients carried 15 different mutations (seven were novel) in GMPPB, including 13 missense variants, one nonsense, and one frameshift (Fig. 1; Table 2). The mutations appear evenly distributed throughout the different domains/inter-domains of the protein and induce distinct alterations in the conformation of the protein (Additional file 1: Figure S1). The predicted ΔΔG values of the different GMPPB mutations were found to range from 5.7 to 13.7 kcal/mol (Fig. 2a), and showed the classical Gaussian distribution previously described for other proteins [24]. The mean of the high destabilizing score (μ = 2.1 kcal/mol, R = 0.96; Fig. 2b) suggested that most GMPPB mutations affect the thermodynamic stability of the protein. In particular, 33% of mutations were recognized as stabilizing (ΔΔG < − 0.46 kcal/mol) and 54% as destabilizing (ΔΔG > 0.46 kcal/mol) (Fig. 2c), while a small percentage appeared to be neutral (− 0.46 < ΔΔG < 0.46 kcal/mol; Fig. 2a, c).

Morbidity map of GMPPB in Italian patients with α-dystroglycanopathy compared to mutations reported in literature. The scheme of the GMPPB protein is illustrated and the mutations identified in this study depicted in bold (novel mutations are in red, published mutations are in black)

Energy changes of missense mutations in GMPPB. a Histogram of calculated free energy changes (ΔΔG) due to missense mutations in GMPPB. Orange-, gray- and green-shaded bars indicate mutated residues falling in the N-terminal catalytic domain, inter-domains and C-terminal LbH domain, respectively. b The ΔΔG distributions of GMPPB missense mutations. The ΔΔG values of mutations were presented in histograms, using 3 kcal/mol bins (the single mutation with ΔΔG = 13.7 kcal/mol was classified into the > 10 kcal/mol bin) and the distribution was fitted to a Gaussian function. c Histogram of the number of mutations (%) plotted against the predicted effect of mutations on GMPPB stability
Finally, we investigated whether mutations with different scores may have different effect on other proteins known to be secondarily affected in GMPPB dystroglycanopathy [26]. WB confirmed a mobility shift of β-dystroglycan in all the patients analyzed and a variable reduction of laminin α2, which was not correlated with the nature of mutations in GMPPB (Fig. 3).

Western blot analysis of patients with mutations in the GMPPB gene. Consistent lower mobility shift of β-dystroglycan (β-DG) and variable expression of laminin α2 (LAMA2) in skeletal muscle biopsies from five patients (P1, P2, P3, P6, and P7) with mutations in the GMPPB gene. Myosin heavy chain (MHC) was used as measure of protein loading. CTRL, control muscle
Discussion
This is the first Italian population study regarding GMPPB-related dystroglycanopathy and encompassing all the previously reported related clinical phenotypes. Only 18% of the patients in our cohort (13/73) harbored pathogenic mutations in GMPPB, and only five presented a CMD phenotype. This latter finding is in line with data from the literature [11, 26,27,28], which indicate that mutations in GMPPB are more common in relatively milder forms of neuromuscular disorders.
No significant clinical findings seemed to emerge in the CMD group, as the features found in these patients, including intellectual disability, ophthalmic involvement, epilepsy and microcephaly, are also typical of other dystroglycanopathies [11]. However, what our study adds to this already broad clinical spectrum is the possible presence of arthrogryposis and congenital clubfoot, particularly in patients with very severe, generalized involvement, as well as nystagmus and upgaze palsy.
Intellectual disability was evident in all the congenital forms, predominantly affecting the language domain. Epilepsy appeared to be related to cognitive impairment and not to the presence of MRI alterations. Autism spectrum disorder emerged as a rare neurodevelopmental comorbidity. At this stage, we cannot totally exclude that an additional variant in neurodevelopmental genes can co-occur, at least in some patients, in a sort of “double trouble” condition. Contrary to the findings of others [14], none of our patients displayed movement disorders such as chorea, whereas ataxia could be part of the clinical picture in line with possible evidence of cerebellar atrophy. On the basis of data from the literature and from our case studies, it can confidently be asserted that mutations in GMPPB predominantly affect the brain in CMD infants. Unless these patients’ clinical and laboratory features are evaluated in a tertiary center specializing in neuromuscular diseases, this might lead to a suspicion of encephalopathy and prevent the condition from being diagnosed early.
The onset of motor manifestations in the LGMD group occurred at different ages and, as previously reported, the extent of weakness was unrelated to the timing of onset of the disease. On the other hand, features such as intellectual disability or epilepsy can be the first manifestations of the disease and are frequent in those patients who have earliest (< 18 years) muscle involvement. None of our LGMD patients displayed cognitive impairment or brain MRI alterations.
The patients with the milder forms manifested easy fatigability or myoglobinuria, or (P8) presented relatively asymptomatic hyperCKemia with subtle weakness, evident only on expert clinical examination. Few cases had overlapping LGMD and CMS features, however we did not specifically set out to identify patients with pathological neurophysiological data, and abnormal neuromuscular transmission in proximal muscles was detected in P8 only after establishing the molecular diagnosis. Contrary to literature data, none of our patients showed facial weakness or ptosis and cataracts were not invariably detected in our patients.
Muscle MRI did not reveal, in our cohort, a striking pattern of muscle involvement maybe in consideration of the different ages and phenotypes displayed by the two patients analyzed (P1 and P6). However, as reported previously [13, 26] we observed a prevalent involvement of posterior compartment of the thigh with a relative atrophy of the anterior compartment, and a minor involvement of the lower limb.
Through this work, we have expanded the array of pathogenic variants associated with GMPPB, and shown that these mutations are widely distributed within the coding exons and located both in the C and in the N-terminal domains (see Additional file 1: Figure S1). In this sample at least, the clinical phenotype did not appear to be related to a specific mutation site within the protein structure. Nonetheless, in an attempt to identify possible genotype-phenotype correlations, we analyzed the allelic frequency of the common variants identified in our population and studied the effects of these mutations on protein stability computing the changes in the thermodynamic folding free energy (ΔΔG). Two mutations (p.R287Q and p.D27H) were found to be common in our study, having an allelic frequency of 15.4 and 11.5%, respectively, rates similar to those reported in the literature [27]. Conversely, p.V330I, found in 3/26 alleles in our study, has only occasionally been reported elsewhere. Interestingly, p.V330I appeared to be pseudo-dominantly inherited in one family (P9 and P10, Additional file 2: Figure S2). We cannot firmly establish whether family members were distantly related and the possibility of an independent inheritance of the p.D27H mutation cannot be excluded.
Examining our data we observed that all the patients carrying p.D27H (P6, P9, P10) showed a mild phenotype as previously described, and this is in keeping with this mutation’s neutral effect on protein stability (Fig. 2a). The reverse is true for p.D287Q whose ΔΔG value predicted a stabilizing effect on the protein. Furthermore, p.R287Q, if combined with the likely destabilizing effect of p. I219T or p.P32L, might predict a severe phenotype (as in P1 or P5, respectively), whereas its association with a neutral variant (e.g. p.G220R in P11 or p.V330I, as in P12) might suggest a less aggressive phenotype. Similar considerations probably apply in the case of association of the most common variant, p.D27H (often seen in LGMD-CMS patients), with the more severe p.P32L mutation.
Consistent with previous findings [26], we observed that patients with GMPPB dystroglycanopathy share the unique biochemical feature of a change in electrophoretic mobility of β-dystroglycan. As there was not apparent correlation between the predicted stability of mutated GMPPB and residual expression of glycosylated α-dystroglycan or secondary reduction of laminin α2 (Fig. 3 and not shown), the finding that β-dystroglycan is equally affected in all patients regardless of the predicted stability of the mutations suggests that the overall retained function of GMPPB may be key to the variability in patients’ phenotype.
Conclusions
To summarize, this study describes a sample of 13 Italian patients carrying a total of 15 different mutations in GMPPB, representing 18% of our study cohort of α-DG patients. Accordingly, GMPPB seems to be one of the more frequent “second generation” α-DG-related genes discovered in the NGS era. Our findings, combined with literature data, show that there are at least three forms of GMPPB-related myopathy: i) CMD, ii) early onset LGMD, and iii) adult onset LGMD, often with evidence of neuromuscular junction involvement. Less severe phenotypes are also observed, such as exercise intolerance and myoglobinuria (in P6) or asymptomatic hyperCKemia (P8). In the absence of information on residual enzyme activity in tissues, combining clinical findings with bioinformatic data on variant stability might allow objective assessment of disease severity.
Abbreviations
- CMD:
-
Congenital muscular dystrophy
- CMS:
-
Congenital myasthenic syndrome
- GMPPB:
-
Guanosine-diphosphate-mannose (GDP-mannose) dyrophosphorylase B gene
- LGMD:
-
Limb-girdle muscular dystrophy
- MRI:
-
Magnetic resonance imaging
- NGS:
-
Next-generation sequencing
- WWS:
-
Walker-Warburg syndrome
- α-DG:
-
alpha-dystroglycanopathy
References
Muntoni F, Brockington M, Blake DJ, Torelli S, Brown SC. Defective glycosylation in muscular dystrophy. Lancet. 2002;360:1419–21.
Toda T, Kobayashi K, Takeda S, Sasaki J, Kurahashi H, Kano H, et al. Fukuyama-type congenital muscular dystrophy (FCMD) and alphadystroglycanopathy. Congenit Anom (Kyoto). 2003;43:97–104.
Brockington M, Muntoni F. The modulation of skeletal muscle glycosylation as a potential therapeutic intervention in muscular dystrophies. Acta Myol. 2005;24:217–21.
Mercuri E, Topaloglu H, Brockington M, Berardinelli A, Pichiecchio A, Santorelli F, et al. Spectrum of brain changes in patients with congenital muscular dystrophy and FKRP gene mutations. Arch Neurol. 2006;63:251–7.
van Reeuwijk J, Brunner HG, van Bokhoven H. Glyc-O-genetics of Walker-Warburg syndrome. Clin Genet. 2005;67:281–9.
Brockington M, Yuva Y, Prandini P, Brown SC, Torelli S, Benson MA, et al. Mutations in the fukutin-related protein gene (FKRP) identify limb girdle muscular dystrophy 2I as a milder allelic variant of congenital muscular dystrophy MDC1C. Hum Mol Genet. 2001;10:2851–9.
Graziano A, Bianco F, D'Amico A, Moroni I, Messina S, Bruno C, et al. Prevalence of congenital muscular dystrophy in Italy: a population study. Neurology. 2015;84:904–11.
Sframeli M, Sarkozy A, Bertoli M, Astrea G, Hudson J, Scoto M, et al. Congenital muscular dystrophies in the UK population: cinical and molecular spectrum of a large cohort diagnosed over a 12-year period. Neuromuscul Disord. 2017;27:793–803.
Bönnemann CG, Wang CH, Quijano-Roy S, Deconinck N, Bertini E, Ferreiro A, et al. Diagnostic approach to the congenital muscular dystrophies. Neuromuscul Disord. 2014;24:289–311.
O'Grady GL, Lek M, Lamande SR, Waddell L, Oates EC, Punetha J, et al. Diagnosis and etiology of congenital muscular dystrophy: we are halfway there. Ann Neurol. 2016;80:101–11.
Carss KJ, Stevens E, Foley AR, Cirak S, Riemersma M, Torelli S, et al. Mutations in GDP-mannose pyrophosphorylase B cause congenital and limb-girdle muscular dystrophies associated with hypoglycosylation of α-dystroglycan. Am J Hum Genet. 2013;93:29–41.
Belaya K, Rodríguez Cruz PM, Liu WW, Maxwell S, McGowan S, Farrugia ME, et al. Mutations in GMPPB cause congenital myasthenic syndrome and bridge myasthenic disorders with dystroglycanopathies. Brain. 2015;138(Pt 9):2493–504.
Oestergaard ST, Stojkovic T, Dahlqvist JR, Bouchet-Seraphin C, Nectoux J, Leturcq F, et al. Muscle involvement in limb-girdle muscular dystrophy with GMPPB deficiency (LGMD2T). Neurol Genet. 2016;2:e112.
Cabrera-Serrano M, Ghaoui R, Ravenscroft G, Johnsen RD, Davis MR, Corbett A, et al. Expanding the phenotype of GMPPB mutations. Brain. 2015;138:836–44.
Panicucci C, Fiorillo C, Moro F, Astrea G, Brisca G, Trucco F, et al. Mutations in GMPPB presenting with pseudometabolic myopathy. JIMD Rep. 2017; https://doi.org/10.1007/8904_2017_25.
Mercuri E, Muntoni F. Muscular dystrophies. Lancet. 2013;381:845–60.
Godfrey C, Clement E, Mein R, Brockington M, Smith J, Talim B, et al. Refining genotype phenotype correlations in muscular dystrophies with defective glycosylation of dystroglycan. Brain. 2007;130:2725–35.
Astrea G, Pezzini I, Picillo E, Pasquariello R, Moro F, Ergoli M, et al. TMEM5-associated dystroglycanopathy presenting with CMD and mild limb-girdle muscle involvement. Neuromuscul Disord. 2016;26:459–61.
Rehm HL, Bale SJ, Bayrak-Toydemir P, Berg JS, Brown KK, Deignan JL, et al. Working Group of the American College of medical genetics and genomics laboratory quality assurance Commitee. ACMG clinical laboratory standards for next-generation sequencing. Genet Med. 2013;15:733–47.
Fiorillo C, Moro F, Yi J, Weil S, Brisca G, Astrea G, et al. Novel dynein DYNC1H1 neck and motor domain mutations link distal spinal muscular atrophy and abnormal cortical development. Hum Mutat. 2014;35:298–302.
Benkert P, Künzli M, Schwede T. QMEAN server for protein model quality estimation. Nucleic Acids Res. 2009;37:W510–4.
Bhattacharya D, Nowotny J, Cao R, Cheng J. 3Drefine: an interactive web server for efficient protein structure refinement. Nucleic Acids Res. 2016;44:W406–9.
Guerois R, Nielsen JE, Serrano L. Predicting changes in the stability of proteins and protein complexes: a study of more than 1000 mutations. J Mol Biol. 2002;320:369–87.
Tokuriki N, Stricher F, Schymkowitz J, Serrano L, Tawfik DS. The stability effects of protein mutations appear to be universally distributed. J Mol Biol. 2007;369:1318–32.
Pettersen EF, Goddard TD, Huang CC, Couch GS, Greenblatt DM, Meng EC, et al. UCSF chimera--a visualization system for exploratory research and analysis. J Comput Chem. 2004;25:1605–12.
Sarkozy A, Torelli S, Mein R, Henderson M, Phadke R, Feng L, et al. Mobility shift of beta-dystroglycan as a marker of GMPPB gene-related muscular dystrophy. J Neurol Neurosurg Psychiatry. 2018; https://doi.org/10.1136/jnnp-2017-316956.
Jensen BS, Willer T, Saade DN, Cox MO, Mozaffar T, Scavina M, et al. GMPPB-associated dystroglycanopathy: emerging common variants with phenotype correlation. Hum Mutat. 2015;36:1159–63.
Raphael AR, Couthouis J, Sakamuri S, Siskind C, Vogel H, Day JW, et al. Congenital muscular dystrophy and generalized epilepsy caused by GMPPB mutations. Brain Res. 2014;1575:66–71.
Acknowledgements
The authors thank Catherine J. Wrenn, who provided expert editorial assistance.
#The Italian Network on Congenital Muscular Dystrophies comprises the following researchers:
Angela Berardinelli1, Giacomo Comi2, Maria Alice Donati3, Maria Teresa Dotti4, Marina Grandis5, Francesca Magri2, Maria A. Maioli6, Alessandro Malandrini4, Francesco Mari3, Roberto Massa7, Luciano Merlini8, Maurizio Moggio2, Lucia O. Morandi9, Olimpia Musumeci10, Marika Pane11, Antonella Pini8, Elena Pegoraro12, Elena M. Pennisi13, Lorenzo Peverelli2, Giulia Ricci14, Carmelo Rodolico10, Lucia Ruggiero15, Michele Sacchini3, Lucio Santoro15, Gabriele Siciliano14, Alessandro Simonati16, Paola Tonin16, Antonio Toscano10.
1 UO Neuropsichiatria Infantile, C. Mondino National Neurological Institute, Pavia, 2 UO Neurology, Maggiore Hospital, and Neuromuscular and Rare Diseases Unit, Dino Ferrari Center, Milan, 3 Meyer Children Hospital, Florence, 4 Neurology, University of Siena, Siena, 5 Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, University of Genoa, Genoa, 6 Neurophysiopathology Multiple Sclerosis Center Hospital Binaghi, Cagliari, 7 UOC Neurology, Policlinico Tor Vergata, Rome, 8 University of Bologna, Bologna, 9 Muscle Cell Biology Lab, Neuromuscular Diseases and Neuroimmunology Unit, Fondazione IRCCS C. Besta, Milan, 10 UOC Neurology and Neuromuscular Diseases, AOU Policlinico G. Martino, Messina, 11 U.O. Neuropsichiatria Infantile, A. Gemelli Hospital, Rome, 12 Department of Neurology, Hospital of Padua, Padua, 13 UOC Neurology, San Filippo Neri, Rome, 14 UO Neurology, AOUP, Pisa, 15 UO Neurology, Policlinico Federico II, Naples, 16 UOC Neurology, Borgo Roma Hospital, Verona.
Funding
This work was partially funded by Regione Toscana FAS SALUTE 2014 (CUP 4042.16092014.066000060 to FMS) and Telethon Foundation grants GUP13004 to AD, GA, CB, EM and LP). FMu and IZ gratefully acknowledge the European Community’s Seventh Framework Programme (FP7/2007–2013) funded grant “Integrated European –omics research project for diagnosis and therapy in rare neuromuscular and neurodegenerative diseases (NEUROMICS)” (grant agreement n° 2012–305121); the Muscular Dystrophy UK Grant on Gene Identification to FMu. FMu is supported by the National Institute for Health Research Biomedical Research Centre at Great Ormond Street Hospital for Children NHS Foundation Trust and University College London; the views expressed in this article are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.. The support of the Muscular Dystrophy UK to the Dubowitz Neuromuscular Centre and of the MRC Neuromuscular Centre Biobank is also gratefully acknowledged.
Availability of data and materials
The dataset supporting the conclusions of this article are included within the article and its additional files.
Author information
Authors and Affiliations
Consortia
Contributions
GA, CF and AD coordinated the collection and elaboration of data. GA and AR drafted the manuscript. CD, RT, FM, FeM, IP, MP, FF, IZ, and WS performed and interpreted the molecular analysis. AR: performed functional in silico studies on selected mutations. RiB and CF reviewed Western blotting in muscle biopsies. CF and AR reviewed the muscle biopsies. CA, CGA, RB, CB, MF, RG, LM, MM, EP, LP, PS and CT, provided patients data. VN and MS reviewed the genetic results. FMS, EB, CB, EM, FMu conceived the study and helped in drafting the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Regione Toscana Pediatric Ethic Review Board.
Consent for publication
Written informed consent was obtained from all subjects or their legal guardians, with explicit consent for future use for research purposes. Signed consent form are available at patients referring centers.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Figure S1. (A) Effects of missense mutations on the structure of GMPPB. The images show the close-up of the different mutation sites with the predicted consequences of the amino acid replacement. Wild-type protein is shown in gray and mutated proteins in magenta. The side chain of wild-type and mutated residues are shown as sticks. Mutated residues located in the N-terminal catalytic domain, inter-domains and C-terminal LbH domain are shown on orange, gray and green backgrounds, respectively. (B) Distribution of missense mutations between the domains and inter-domains of the GMPPB protein reported as number of mutations per amino acid. Orange bar, N-terminal catalytic domain; gray bar, inter-domains; green bar, C-terminal LbH domain. (PDF 8212 kb)
Additional file 2:
Figure S2. Pedigree of the family showing pseudo-dominant inheritance in GMPPB disease. Two patients (uncle and nephew, P9 and P10, respectively) showed onset in early adulthood and similar muscular impairments associated with biallelic mutations (p:Asp27His and p.Val330Ile) in GMPPB. Circles are females and squares are males. Slashed symbols indicate deceased individuals. Numbers in symbols indicate number of siblings. (PDF 7 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Astrea, G., Romano, A., Angelini, C. et al. Broad phenotypic spectrum and genotype-phenotype correlations in GMPPB-related dystroglycanopathies: an Italian cross-sectional study. Orphanet J Rare Dis 13, 170 (2018). https://doi.org/10.1186/s13023-018-0863-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-018-0863-x