
Abstract
Background
Spinocerebellar ataxia type 2 (SCA2) affects several neurological structures, giving rise to multiple symptoms. However, only the natural history of ataxia is well known, as measured during the study duration. We aimed to describe the progression rate of ataxia, by the Scale for the Assessment and Rating of Ataxia (SARA), as well as the progression rate of the overall neurological picture, by the Neurological Examination Score for Spinocerebellar Ataxias (NESSCA), and not only during the study duration but also in a disease duration model. Comparisons between these models might allow us to explore whether progression is linear during the disease duration in SCA2; and to look for potential modifiers.
Results
Eighty–eight evaluations were prospectively done on 49 symptomatic subjects; on average (SD), study duration and disease duration models covered 13 (2.16) months and 14 (6.66) years of individuals’ life, respectively. SARA progressed 1.75 (CI 95%: 0.92–2.57) versus 0.79 (95% CI 0.45 to 1.14) points/year in the study duration and disease duration models. NESSCA progressed 1.45 (CI 95%: 0.74–2.16) versus 0.41 (95% CI 0.24 to 0.59) points/year in the same models. In order to explain these discrepancies, the progression rates of the study duration model were plotted against disease duration. Then an acceleration was detected after 10 years of disease duration: SARA scores progressed 0.35 before and 2.45 points/year after this deadline (p = 0.013). Age at onset, mutation severity, and presence of amyotrophy, parkinsonism, dystonic manifestations and cognitive decline at baseline did not influence the rate of disease progression.
Conclusions
NESSCA and SARA progression rates were not constant during disease duration in SCA2: early phases of disease were associated with slower progressions. Modelling of future clinical trials on SCA2 should take this phenomenon into account, since disease duration might impact on inclusion criteria, sample size, and study duration. Our database is available online and accessible to future studies aimed to compare the present data with other cohorts.
Similar content being viewed by others
Background
The spinocerebellar ataxia type 2 (SCA2) is one of the most common polyglutamine (polyQ) disorders. Caused by a dominant expansion of a CAG repeat tract (CAGexp) at ATXN2, SCA2 is related to a polyQ with more than 32–33 glutamines in ataxin-2 [1]. Disease usually starts in adulthood and clinical picture is not homogeneous. Main symptoms are related to cerebellar dysfunction, and include ataxic gait, cerebellar dysarthria as well as dysmetria [2]. Severe saccade slowing and peripheral neuropathy are very frequent and affect more than 50% of case series [3]. Besides, several other manifestations might appear, such as pyramidal findings, extrapyramidal syndromes (including dystonic movements and parkinsonism), lower motor neuron findings, cognitive deterioration, and others [4,5,6]. ATXN2 expansion explains most but not all variability in age at onset (AO) of symptoms [1], and it was related to presence of some neurological findings such as dystonic movements and parkinsonism [7]. Mean (SD) age at onset was around 30 to 33 (14) years [8, 9] and median survival was 68 [95% CI: 65–70] years, usually after a wheelchair period [10].
Description of disease progression in SCA2 depends on a comprehensive disease-progression model as well as in other SCAs. Several challenges hamper this, such as heterogeneous subphenotypes evolving in time, rarity, and the long duration of disease. Moreover, effects related to genetic or environmental background cannot be discarded. Clinical scales appropriated to the phenotype, description of disease progression in more than one cohort, and anticipating potential drawbacks from data obtained from short duration clinical studies are some of the questions investigators should keep in mind [11].
As stated before, SCA2 symptoms are very heterogeneous. In spite of that, majority of longitudinal studies followed ataxic manifestations only, as measured by Scale for the Assessment and Rating of Ataxia (SARA) [12], SCA Functional-Index (SCAFI) [13], and Composite-Cerebellar-Functional-Score (CCFS) [14]. The natural history (NH) of SARA has been measured a couple of times in SCA2 patients [15,16,17,18,19]. NH of SCAFI and CCFS were described only once for each, with insufficient or non-significant progression rates [18, 20]. An unique study followed up extra-cerebellar findings by using the inventory of non-ataxic symptoms (INAS); however, non satisfactory results were raised [15, 16].
Most longitudinal observations of neurological scales in SCAs used the study entry as the time correspondent to the start of the measurements. First measurements were considered as baseline, abscissa axis was the chronological time since the beginning of study, and the slope of progression was obtained by comparing these data with those obtained at latter observations, usually at fixed intervals [15, 16, 18, 19]. Other studies chose to add age at onset informed by the individual into the model: in these studies, the abscissa axis presented the whole disease duration [21, 22]. If the actual progression rate of the disease is continuous and linear, the slopes obtained by both models should be similar. In contrast, if slopes obtained with these two models are different, this means that progression is not linear and must be further explored.
Our aims were to describe the progression rate of neurological manifestations in a new SCA2 cohort, as measured by the ataxia scales SARA, SCAFI, and CCFS, and by a comprehensive neurologic scale, the Neurological Examination Score for Spinocerebellar Ataxias (NESSCA) [23, 24]; to explore if progression rates are linear during the whole disease duration since onset of gait ataxia; and to look for potential modifiers of disease progression.
Methods
Symptomatic carriers with a molecular diagnosis of SCA2, under care in outpatient clinics of University hospitals of Porto Alegre, Rio de Janeiro, and São Paulo, Brazil, were invited to participate in this study.
Investigators trained in the scales (TLM, ERR, MA, ASPS) applied NESSCA, SARA, SCAFI, CCFS, and mini-mental state examination (MMSE) in the participants at baseline and in a second visit planned to occur 12 months later. Data was registered in protected files.
Independent variables under study were the following: age, gender, age at onset of gait ataxia (AOga), age at onset of first symptom (AOfs), disease duration since start of gait ataxia (DDga), disease duration since start of first symptom (DDfs), and the number of CAG repeats in both alleles. Molecular studies were performed as previously described [6]. Phenotypic subgroups were built according to presence or absence of amyotrophy, parkinsonism, dystonia, and cognitive losses, as previously described [7]. They were used as additional independent variables. Briefly, amyotrophy was considered present if fasciculations in regions other than face, or muscle tissue loss were found (items 8 and 15 of NESSCA) [22 23]. Parkinsonism was present if at least two out of three manifestations were documented - bradykinesia, rigidity, and resting tremor (items 11 and 12 of NESSCA) [23, 25]. Dystonia was considered present if dystonic movements impaired in some degree the voluntary movements (at least 2 points on item 10 of NESSCA) [23]. Cognitive decline was considered present according to Folstein criteria for MMSE [26].
Modeling
Linear growth curve models, i.e., mixed models with intercepts and random slopes, were adjusted to model the relationship between outcomes and time. The annual rate of increase was estimated in two different ways:
-
Study duration model: A mean change per studied year. Points in time included in this model were the study entry (first observation was the baseline), and 12 and 24 months later (follow up observations).
-
Disease duration model: A mean change since the disease onset, according to patient’s report. In this model, at least three time points were of interest: the time of onset of gait ataxia (baseline), the study entry (first observation), and 12 and 24 months later (follow up observations). The progression rate was that estimated to occur during all disease duration.
These different strategies followed the recommendation of Singer and Willett (2003) [27] of investigating alternative temporal specifications. The progression rate obtained during the study duration model was defined as the standard model in the present analysis. If lopes derived from both models were different, the raised hypothesis was that the progression is highly dependent on disease duration, and then a binary variable would be included in the study duration model, according to the apparent effect of disease duration on shifting the progression rate.
A variance component covariance matrix was used for the intercepts and random slopes. Models were fitted in R 3.2.2 software, using lme4 package. P-values were obtained through likelihood ratio tests, using Anova function of car package. Bootstrap replicates were used to produce confidence intervals for the fitted curves.
Ethics approval and consent to participate
The study protocol was approved by the institutional ethical standards committees on human experimentation of all contributing centers (registered as 12–0346 at Comissao de Etica em Pesquisa of our institution, and as 07105712.1.0000.5327 at the Brazilian National platform, Plataforma Brasil). All patients gave written informed consent to participate in the study.
Consent for publication
Not applicable – this report does not contain any individual persons data.
Results
Forty-nine SCA2 symptomatic carriers (27 men) were included in the baseline analysis, and thirty-eight follow-up evaluations were done. Clinical and molecular characteristics at baseline were already described [7]. Table 1 summarizes demographic data, genetic and neurological findings at baseline (all similar between genders). The original database was anonymized and is also available for readers (Additional file 1).
Progression rates
Progression rates were obtained for SARA, NESSCA, CCFS and SCAFI according to the mean change per studied year (study duration model) and to mean change since the disease onset (disease duration model).
SARA progressed 1.75 points/year (95% CI: 0.92–2.57) in the study duration model and only 0.79 points/year (95% CI 0.45 to 1.14) in the disease duration model.
NESSCA progressed 1.45 points/year (CI 95%: 0.74–2.16) in the study duration model and only 0.41 points/year (95% CI 0.24 to 0.59) in the disease duration model.
SCAFI progressed just −0.05 points/year (95% -0.09 to −0.01) in the disease duration model. SCAFI did not present a significant progression in the study duration model, while CCFS did not present significant progressions in both models.
The above results documented that there were differences in the progression rates of SARA and NESSCA when both models were applied. The hypothesis was that the progression rate of these scales was not constant during disease duration. Deltas of SARA and NESSCA observed in one year (the study duration model) were then plotted against disease duration in order to determine a cutoff value for the subsequent stratification of the study duration analysis.
Sixteen out of 38 subjects evaluated in the follow-up had 10 or less years of DD. Figure 1A shows that 2/16 subjects with less than 10 years of disease duration progressed 3 points – and none of them progressed more than that -, whereas 10/22 individuals with more than 10 years of disease duration progressed 3 or more points in SARA scores in one year (chi-square = 4.66, p = 0.031). Age, AO and CAGexp at ATXN2 were similar between these DD groups and did not influence their deltaSARAs (data not shown).

- Differences (deltas) between baseline and follow up observations 12 months later, according to disease duration since onset of gait ataxia. (a) Deltas of SARA scores were lower than 3 in the first 10 years of disease duration (b) Deltas of NESSCA scores during the first 10 years and after 20 years of disease duration were also lower than those observed in 10–20 years of disease duration
Progression rates of SARA were shown in Fig. 2, using the cutoff of 10 years of disease duration to stratify our cohort. Symptomatic SCA2 individuals with less and more than 10 years of disease duration progressed 0.35 and 2.45 points/year in SARA scores (p = 0.013), respectively.

- SARA progression during the study duration, according to disease duration strata
Figure 1B shows that NESSCA progression is also lower in the first 10 years of disease duration than later on. NESSCA progression turned fast after 10 years, and slowed again after 20 years of disease duration. Due to this finding, and in order to examine the effect of disease stage on the slopes, we have studied further NESSCAs from individuals with less than 20 years of disease duration only, by using the cutoff of 10 years of disease duration. Progression rates of NESSCA were shown in Fig. 3. Symptomatic SCA2 individuals with less and more than 10 years of disease duration progressed 1.03 and 2.14 points/year in NESSCA scores (p = 0.191), respectively.

- NESSCA progression during study duration, according to disease duration strata
Modifier factors
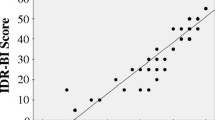
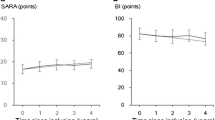
Gender, AOga, AOfs, CAGexp at ATXN2, and presence/absence of amyotrophy, parkinsonism, dystonic manifestations and cognitive decline at baseline, were studied as potential modifier factor of disease progression according to both models (study duration model and disease duration model). None of them produced significant differences in the progression rates - even using the disease duration strata revealed in Figs. 1 ,2, and 3. Figure 4 shows an example of the NESSCA and SARA progression rates obtained in subjects with and without cognitive decline.

- Disease progression as measured by clinical scales in SCA2 individuals according to disease duration model. (a) NESSCA progression. (b) SARA progression. Hatched lines describe progression rates of subjects with cognitive decline, while continuous lines describe progression rates of subjects without cognitive decline
Discussion
Our results showed that progression rates of SARA and NESSCA were not constant during the long disease duration of SCA2 symptomatic patients. At early phases, i.e., in the first 10 years of the disease, progression rates of both scales were slower than in the following years. This phenomenon might be due to the psychometric characteristics of scales or to biological causes. Whatever the reason, the direct use of linear models during prospective longitudinal observations without paying attention to differences in disease duration might keep these non-linear progressions hidden.
At least nine studies followed SCA2 patients with longitudinal observations [15,16,17,18,19, 28,29,30,31]. In most cases where SARA progression was measured, annual worsening was around 1.5 to 1.9 points [15, 16, 18, 19, 30]. The methodology of analysis of two of these former cohorts were similar to that from our group therefore, our results can be compared to those studies [15, 16, 18]. Our observations related to the study duration analysis raised a SARA progression of 1.75 points/year, which is comparable to theirs. However, neither observations related to disease duration (Fig. 1) nor discrepancy of results obtained by the two models has been reported before.
Disease progression of a cohort of 35 SCA2 patients living in France was analysed using mixed models with a random effect for patients and the fixed effects group and time between inclusion and clinical examination [18]. Authors found that SARA worsened 1.3 (0.2) points per year. Factors associated with faster SARA progression were male gender, and patients who were younger at onset. Disease duration and CAGexp did not change SARA progression in that cohort. The Eurosca study included 163 SCA2 patients from several European countries in a longitudinal cohort, and linearity of the progression rate was tested via nested models (likelihood ratio test), followed by an analysis of covariance where the effect of gender, age at onset, disease duration, and repeat length of the expanded allele were tested [15, 16]. SARA worsened 1.40 points per year. Earlier age at onset and longer expanded alleles were associated with faster SARA progression: in the multivariate analysis, age at onset was the only independent factor. Thirty Cuban symptomatic subjects were evaluated four times (baseline, and at 1, 2, and 5 years), in a study that longitudinally followed variations in SARA and in saccades: the exponential progression rate of the SARA score was associated to the CAGexp [19].
Therefore, previous SCA2 cohorts showed effects of gender, early ages at onset or of CAGexp on speeding SARA progression. None detected a difference related to disease duration. In contrast, our cohort showed a trend to associate a faster NESSCA (not SARA) progression to larger CAGexp. These discrepancies can be due to differences in sample sizes - the number of observations impacting on the choice of statistical modeling -, or to truly differences between cohorts with diverse populational origins.
Contrary to previous cohorts, our longitudinal observation was able to pick up a clear effect of disease duration on the slope of progression of SARA and NESSCA. This effect was detected because of the discrepancy between the slopes obtained with the two models: the study duration and the disease duration models. Discrepancy led us to look for deltas distributions (Fig. 1) and a cutoff value was chosen with the empirical data. Both Jacobi et al. [15] and Tezenas du Montcel et al. [18] analysed the data by the study duration, using the time between inclusion and clinical examination as one of the fixed effects. We questioned whether the treatment of disease duration in their model was unable to reveal this variable as a modifier. It is relevant to state that disease duration entered their model as a factor whose interaction with progression rate was tested with a mathematical treatment - either as a continuous or a dichotomous variable, splitted by the median. This procedure fitted totally with the generalized linear mixed model; but it might be insufficient to clarify the problem. A good way to shed light into this problem will be to perform either multicentric studies or a meta-analysis. Our database is available online with the present communication in order to help any of these approaches.
Non linear are as plausible as linear progressions for neurodegenerative diseases and were already clearly proposed for SCA2 [19]. In Huntington disease (HD), another polyQ disorder, progression rates of chorea and of caudate atrophy are not linear. Slopes for caudate atrophy changes with the clinical stage [32]. The annual rate of increase in chorea is greater among individuals with earlier-stage HD than in those with advanced HD [33]. Reasons for non-linearity might include scale limitations and truly natural phenomena. For instance, NESSCA progression seemed to be slower either in the first as well as in the last years of the disease (Fig. 1B). We postulate that the slowdown seen after 20 years of the disease more probably reflects the inability of this scale to measure progression after a certain disease stage. In any case, statistical modeling is an issue for discontinuous deteriorations. In another study, we used markov chains to describe the progression of several neurological findings in SCA3/Machado Joseph disease (SCA3/MJD). Although markov chains are quite uneasy and unfamiliar for clinical researchers, this model disclosed that isolated findings, such as gait ataxia, limb ataxia, dystonic manifestations and others, followed a curvilinear trajectory as the disease progressed [21]. Perhaps the present approach, where the use of mixed models was done in two stracta, splitted by a cutoff for dichotomous (dummy) observations chosen by an immediate, empirical data judged by eye inspection, can be more helpful.
Conclusions
The present study suggested that the speed of progression of scales SARA and NESSCA is not uniform during the disease process in SCA2, varying according to stage of disease. General progression rates of SARA and NESSCA were either similar to others studies in SCA2 (1.7 points per year in the case of SARA) or very like other SCA (1.45 points per year in the case of NESSCA, similar to the progression found in SCA3/MJD), while general progression of SCAFI and CCFS were non significant, at least in the study duration model. Early phases of disease were associated with slower SARA and NESSCA progressions, when compared to phases after 10 years of disease onset. Future clinical trials on SCA2 should take this into account when estimating sample size/study duration. Moreover, we recommend that disease duration should be included in recruitment criteria. Finally, our database is available online and accessible to future studies aimed to compare our cohort with other databases. A meta-analysis would be the best way to elucidate all events that influence the progression of this disease.
Abbreviations
- AO:
-
age at onset
- AOfs:
-
age at onset of first symptom
- AOga:
-
age at onset of gait ataxia
- CAGexp:
-
expanded CAG repeat tract
- CCFS:
-
Composite-Cerebellar-Functional-Score
- DDfs:
-
disease duration since the start of first symptom
- DDga:
-
disease duration since the start of gait ataxia
- HD:
-
Huntington disease
- INAS:
-
inventory of non-ataxic symptoms
- MMSE:
-
mini-mental state examination
- NESSCA:
-
Neurological Examination Score for Spinocerebellar Ataxias
- NH:
-
natural history
- polyQ:
-
polyglutamine
- SARA:
-
Scale for the Assessment and Rating of Ataxia
- SCA:
-
Spinocerebellar ataxia
- SCA2:
-
Spinocerebellar ataxia type 2
- SCA3/MJD:
-
Spinocerebellar ataxia type 3/Machado-Joseph disease
- SCAFI:
-
SCA Functional-Index
- SD:
-
standard deviation
References
Pulst SM. Spinocerebellar Ataxia Type 2. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Fong CT, Mefford HC, Smith RJH, Stephens K, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2016. 1998 Oct 23 [updated 2015 Nov 12].
Magaña JJ, Velázquez-Pérez L, Cisneros B. Spinocerebellar ataxia type 2: clinical presentation, molecular mechanisms, and therapeutic perspectives. Mol Neurobiol. 2013 Feb;47(1):90–104.
Cancel G, Dürr A, Didierjean O, Imbert G, Bürk K, Lezin A, Belal S, Benomar A, Abada-Bendib M, Vial C, Guimarães J, Chneiweiss H, Stevanin G, Yvert G, Abbas N, Saudou F, Lebre AS, Yahyaoui M, Hentati F, Vernant JC, Klockgether T, Mandel JL, Agid Y, Brice A. Molecular and clinical correlations in spinocerebellar ataxia 2: a study of 32 families. Hum Mol Genet. 1997 May;6(5):709–15.
Schöls L, Gispert S, Vorgerd M, Menezes Vieira-Saecker AM, Blanke P, Auburger G, Amoiridis G, Meves S, Epplen JT, Przuntek H, Pulst SM, Riess O. Spinocerebellar ataxia type 2. Genotype and phenotype in German kindreds. Arch Neurol. 1997 Sep;54(9):1073–80.
Bürk K, Globas C, Bosch S, Gräber S, Abele M, Brice A, Dichgans J, Daum I, Klockgether T. Cognitive deficits in spinocerebellar ataxia 2. Brain. 1999;122:769–77.
de Castilhos RM, Furtado GV, Gheno TC, Schaeffer P, Russo A, Barsottini O, Pedroso JL, Salarini DZ, Vargas FR, de Lima MA, Godeiro C, Santana-da-Silva LC, Toralles MB, Santos S, Van der Linden H Jr, Wanderley HY, de Medeiros PF, Pereira ET, Ribeiro E, Saraiva-Pereira ML, Jardim LB. Rede Neurogenetica. Spinocerebellar ataxias in Brazil--frequencies and modulating effects of related genes. Cerebellum. 2014 Feb;13(1):17–28.
Monte T, Pereira FS, Reckziegel ER, Augustin MC, Silva ASP, Locks-Coelho LD, Barsottini O, Pedroso JL, Vargas FR, Saraiva-Pereira ML, Jardim LB, on behalf of Rede Neurogenetica. Neurological phenotypes in spinocerebellar ataxia type 2: role of mitochondrial polymorphism A10398G and other risk factors. Park Relat Disorders 2017 Jun 19. https://doi.org/10.1016/j.parkreldis.2017.06.010 [Epub ahead of print].
Klockgether T, Lüdtke R, Kramer B, Abele M, Bürk K, Schöls L, Riess O, Laccone F, Boesch S, Lopes-Cendes I, Brice A, Inzelberg R, Zilber N, Dichgans J. The natural history of degenerative ataxia: a retrospective study in 466 patients. Brain. 1998 Apr;121(Pt 4):589–600.
Almaguer-Mederos LE, Falcón NS, Almira YR, Zaldivar YG, Almarales DC, Góngora EM, Herrera MP, Batallán KE, Armiñán RR, Manresa MV, Cruz GS, Laffita-Mesa J, Cyuz TM, Chang V, Auburger G, Gispert S, Pérez LV. Estimation of the age at onset in spinocerebellar ataxia type 2 Cuban patients by survival analysis. Clin Genet. 2010 Aug;78(2):169–74.
Monin ML, Tezenas du Montcel S, Marelli C, Cazeneuve C, Charles P, Tallaksen C, Forlani S, Stevanin G, Brice A, Durr A. Survival and severity in dominant cerebellar ataxias. Ann Clin Transl Neurol. 2015 Feb;2(2):202–7.
Yang E, Farnum M, Lobanov V, Schultz T, Verbeeck R, Raghavan N, Samtani MN, Novak G, Narayan V, DiBernardo A. Alzheimer's DiseaseNeuroimaging initiative. Quantifying the pathophysiological timeline of Alzheimer's disease. J Alzheimers Dis. 2011;26(4):745–53.
Schmitz-Hübsch T, du Montcel ST, Baliko L, Berciano J, Boesch S, Depondt C, Giunti P, Globas C, Infante J, Kang JS, Kremer B, Mariotti C, Melegh B, Pandolfo M, Rakowicz M, Ribai P, Rola R, Schöls L, Szymanski S, van de Warrenburg BP, Dürr A, Klockgether T, Fancellu R. Scale for the assessment and rating of ataxia: development of a new clinical scale. Neurology. 2006 Jun 13;66(11):1717–20.
Schmitz-Hübsch T, Giunti P, Stephenson DA, Globas C, Baliko L, Saccà F, Mariotti C, Rakowicz M, Szymanski S, Infante J, van de Warrenburg BP, Timmann D, Fancellu R, Rola R, Depondt C, Schöls L, Zdzienicka E, Kang JS, Döhlinger S, Kremer B, Melegh B, Filla A, Klockgether TSCA. Functional index: a useful compound performance measure for spinocerebellar ataxia. Neurology. 2008 Aug 12;71(7):486–92.
du Montcel ST, Charles P, Ribai P, Goizet C, Le Bayon A, Labauge P, Guyant-Maréchal L, Forlani S, Jauffret C, Vandenberghe N, N’guyen K, le Ber I, Devos D, Vincitorio CM, Manto MU, Tison F, Hannequin D, Ruberg M, Brice A, Durr A. Composite cerebellar functional severity score: validation of a quantitative score of cerebellar impairment. Brain. 2008 May;131(Pt 5):1352–61.
Jacobi H, Bauer P, Giunti P, Labrum R, Sweeney MG, Charles P, Dürr A, Marelli C, Globas C, Linnemann C, Schöls L, Rakowicz M, Rola R, Zdzienicka E, Schmitz-Hübsch T, Fancellu R, Mariotti C, Tomasello C, Baliko L, Melegh B, Filla A, Rinaldi C, van de Warrenburg BP, Verstappen CC, Szymanski S, Berciano J, Infante J, Timmann D, Boesch S, Hering S, Depondt C, Pandolfo M, Kang JS, Ratzka S, Schulz J, Tezenas du Montcel S, Klockgether T. The natural history of spinocerebellar ataxia type 1, 2, 3, and 6: a 2-year follow-up study. Neurology. 2011 Sep 13;77(11):1035–41.
Jacobi H, du Montcel ST, Bauer P, Giunti P, Cook A, Labrum R, Parkinson MH, Durr A, Brice A, Charles P, Marelli C, Mariotti C, Nanetti L, Panzeri M, Rakowicz M, Sulek A, Sobanska A, Schmitz-Hübsch T, Schöls L, Hengel H, Baliko L, Melegh B, Filla A, Antenora A, Infante J, Berciano J, van de Warrenburg BP, Timmann D, Szymanski S, Boesch S, Kang JS, Pandolfo M, Schulz JB, Molho S, Diallo A, Klockgether T. Long-term disease progression in spinocerebellar ataxia types 1, 2, 3, and 6: a longitudinal cohort study. Lancet Neurol. 2015 Nov;14(11):1101–8.
Lee YC, Liao YC, Wang PS, Lee IH, Lin KP, Soong BW. Comparison of cerebellar ataxias: a three-year prospective longitudinal assessment. Mov Disord. 2011 Sep;26(11):2081–7.
Tezenas du Montcel S, Charles P, Goizet C, Marelli C, Ribai P, Vincitorio C, Anheim M, Guyant-Maréchal L, Le Bayon A, Vandenberghe N, Tchikviladzé M, Devos D, Le Ber I, N'Guyen K, Cazeneuve C, Tallaksen C, Brice A, Durr A. Factors influencing disease progression in autosomal dominant cerebellar ataxia and spastic paraplegia. Arch Neurol. 2012 Apr;69(4):500–8. https://doi.org/10.1001/archneurol.2011.2713.
Rodríguez-Labrada R, Velázquez-Pérez L, Auburger G, Ziemann U, Canales-Ochoa N, Medrano-Montero J, Vázquez-Mojena Y, González-Zaldivar Y. Spinocerebellar ataxia type 2: measures of saccade changes improve power for clinical trials. Mov Disord. 2016 Apr;31(4):570–8.
Schmitz-Hübsch T, Fimmers R, Rakowicz M, Rola R, Zdzienicka E, Fancellu R, Mariotti C, Linnemann C, Schöls L, Timmann D, Filla A, Salvatore E, Infante J, Giunti P, Labrum R, Kremer B, van de Warrenburg BP, Baliko L, Melegh B, Depondt C, Schulz J, du Montcel ST, Klockgether T. Responsiveness of different rating instruments in spinocerebellar ataxia patients. Neurology. 2010 Feb 23;74(8):678–84.
Jardim LB, Hauser L, Kieling C, Saute JA, Xavier R, Rieder CR, Monte TL, Camey S, Torman VB. Progression rate of neurological deficits in a 10-year cohort of SCA3 patients. Cerebellum. 2010 Sep;9(3):419–28.
Torman VL, De Vries J, Verbeek D, Brunt E, Kampinga H, Jardim LB. Interrelation between size of CAG-expansion and progression of ICARS scores in a Dutch cohort of SCA3/MJD patients. Abstract presented in the international meeting on spastic Paraparesis and ataxias. Paris. 2016;
Kieling C, Rieder CR, Silva AC, Saute JA, Cecchin CR, Monte TL, Jardim LBA. Neurological examination score for the assessment of spinocerebellar ataxia 3 (SCA3). Eur J Neurol. 2008 Apr;15(4):371–6.
Monte TL, Reckziegel ER, Augustin MC, Silva ASP, Locks-Coelho LD, Barsottini O, Pedroso JL, Vargas FR, Saraiva-Pereira ML, Leotti VB, Jardim LB, Rede Neurogenética NESSCA. Validation and responsiveness of several rating scales in Spinocerebellar ataxia type 2. Cerebellum. 2017 Apr 29; https://doi.org/10.1007/s12311-017-0855-8. [Epub ahead of print]
Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease. A clinico-pathological study of 100 cases. JNNP. 1992;55:181–4.
Folstein MF, Folstein SE, McHugh PR. Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res..Nov;12(3):189–198.
Singer JD, Willett JB. Applied longitudinal data analysis: modeling change and event occurrence. First Ed, Oxford: Oxford University Press; 2003.
Velázquez-Perez L, Rodríguez-Labrada R, Canales-Ochoa N, Sanchez-Cruz G, Fernandez-Ruiz J, Montero JM, Aguilera-Rodríguez R, Diaz R, Almaguer-Mederos LE, Truitz AP. Progression markers of Spinocerebellar ataxia 2. A twenty years neurophysiological follow up study. J Neurol Sci. 2010 Mar 15;290(1–2):22–6.
Velázquez-Pérez L, Rodríguez-Labrada R2, Canales-Ochoa N2, Montero JM2, Sánchez-Cruz G2, Aguilera-Rodríguez R2, Almaguer-Mederos LE2, Laffita-mesa JM2. Progression of early features of spinocerebellar ataxia type 2 in individuals at risk: a longitudinal study. Lancet Neurol 2014 May;13(5):482–489.
Fancellu R, Paridi D, Tomasello C, Panzeri M, Castaldo A, Genitrini S, Soliveri P, Girotti F. Longitudinal study of cognitive and psychiatric functions in spinocerebellar ataxia types 1 and 2. J Neurol. 2013 Dec;260(12):3134–43.
Moriarty A, Cook A, Hunt H, Adams ME, Cipolotti L, Giunti PA. Longitudinal investigation into cognition and disease progression in spinocerebellar ataxia types 1, 2, 3, 6, and 7. Orphanet J Rare Dis. 2016 Jun 22;11(1):82.
Ross CA, Aylward EH, Wild EJ, Langbehn DR, Long JD, Warner JH, Scahill RI, Leavitt BR, Stout JC, Paulsen JS, Reilmann R, Unschuld PG, Wexler A, Margolis RL, Tabrizi SJ. Huntington disease: natural history, biomarkers and prospects for therapeutics. Nat Rev Neurol. 2014 Apr;10(4):204–16.
Dorsey ER, Beck CA, Darwin K, Nichols P, Brocht AF, Biglan KM, Shoulson I. Huntington study group COHORT investigators. Natural history of Huntington disease. JAMA Neurol. 2013 Dec;70(12):1520–30.
Acknowledgements
We are grateful to patients who agreed to participate in this study.
Funding
This work was supported by the following Brazilian agencies: CNPq - Conselho Nacional de Desenvolvimento Científico e Tecnológico - by the Project 78,057/2012–1; FIPE-HCPA – Fundo de Incentivo à Pesquisa do Hospital de Clínicas de Porto Alegre – by the Projects GPPG HCPA 12–0357 and 12–0396; and by INAGEMP - Instituto Nacional de Genética Médica Populacional. MA and LDLC were supported by FAPERGS. ERR, MA, ASPS, MLSP, and LBJ were supported by CNPq.
Availability of data and materials
Our database is available online as a supplemental material.
Author information
Authors and Affiliations
Consortia
Contributions
TLM had an important role in the project’s conception and execution, in the data analysis and in drafting the manuscript. ERR performed neurological evaluations. MA performed neurological evaluations. LDLC performed neurological evaluations and data analysis. ASPS performed neurological evaluations. GVF performed molecular analyses. EPM performed molecular analyses. JLP obtained data and performed neurological evaluations. OPB obtained data and performed neurological evaluations. FRV obtained data and performed neurological evaluations. MLSP performed molecular analyses. SAC interpreted the patient data and modelled statistical analyses. VBL interpreted the patient data, modelled statistical analyses and was a major contributor in writing the manuscript. LBJ had an important role in the project’s conception, obtined funding, analysed the results, and was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the institutional ethical committees of the contributing centers (registered as 12–0346 at Comissao de Etica em Pesquisa of our institution, and as 07105712.1.0000.5327 at the Brazilian National platform, Plataforma Brasil). All patients gave written informed consent to participate in the study.
Consent for publication
Not applicable – this report does not contain any individual persons data.
Competing interests
The authors declare that they don’t have conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Database on the Brazilian SCA2 cohort, by Monte et al 2018, Orphanet Journal of Rare Diseases. (XLSX 224 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Monte, T.L., Reckziegel, E., Augustin, M.C. et al. The progression rate of spinocerebellar ataxia type 2 changes with stage of disease. Orphanet J Rare Dis 13, 20 (2018). https://doi.org/10.1186/s13023-017-0725-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-017-0725-y