
Abstract
Objective
Postoperative delirium (POD) is a common complication along with poor prognosis in geriatric intertrochanteric fracture (ITF) patients. However, the prevention and treatment of POD remain unclear. Previous studies have confirmed that POD is essentially a consequence of neuro-inflammatory responses. Dexamethasone is a glucocorticoid with comprehensive anti-inflammatory effects, while a high dose of dexamethasone correlates with many side effects or even adverse consequences. Thus, this prospective study aims to discuss whether a single preoperative low-dose dexamethasone can reduce the impact of POD on geriatric ITF patients with internal fixation surgery.
Methods
Between June 2020 and October 2022, there were 219 consecutive ITF patients assessed in our department. Of the 219 ITF patients, 160 cases who met the inclusion and exclusion criteria were finally enrolled and randomly allocated to the dexamethasone group and the placebo group (80 geriatric ITF patients in each group) in this prospective study. The patients in the dexamethasone group received intravenous 10 mg (2 ml) dexamethasone while the patients in the placebo group received intravenous 2 ml saline in 30 min before being sent to the operating room, respectively. The baseline characteristics, surgical information, incidence and severity of POD as the efficacy-related outcomes, and infection events and hyperglycemia as safety-related outcomes (adverse events), were collected and analyzed between the two groups. The severity of POD was evaluated by Memorial Delirium Assessment Scale (MDAS) score.
Results
There were no differences in baseline characteristics and surgical information between the dexamethasone group and the placebo group. The dexamethasone group had a lower incidence of POD than the placebo group within the first 5 days after surgery [(9/80, 11.3% vs. 21/80, 26.3%, RR = 0.83, 95% CI 0.71–0.97, P = 0.015]. The dexamethasone group had lower MDAS scores (Mean ± SD) than the placebo group [13.2 ± 1.0 (range 11 to 15) vs. 15.48 ± 2.9 (range 9 to 20), P = 0.011, effect size = 0.514]. There were no differences in infection events and hyperglycemia between the two groups.
Conclusions
A single preoperative low-dose dexamethasone may reduce the incidence and severity of POD in geriatric ITF patients with internal fixation surgery.
Trial registration: ChiCTR2200055281.
Similar content being viewed by others


Introduction
Intertrochanteric fracture (ITF), also commonly known as one kind of hip fracture, is important causes of hospitalization in the elderly. The population aged over 70 years will double in the next three decades, leading to a great number of ITF globally [1, 2]. ITF is typically treated with surgery because conservative treatment is associated with high mortality and poor functional recovery [3]. However, postoperative delirium (POD), defined as an acute disruption in attention, consciousness, and cognition, is a common and serious complication following ITF surgery, with reported incidences varying from 14.3 to 25.0% [4,5,6]. Patients who develop POD are associated with prolonged hospital stays, high medical costs, postoperative cognitive impairment, and increased mortality [7].
Despite the high prevalence and morbidity of POD, the exact pathophysiology is still not fully elucidated. Various mechanisms are proposed to understand POD, of which the most widely recognized one is the neuro-inflammatory mechanism [8, 9]. Concerning ITF, the first trauma, subsequent anesthesia, and following surgery trigger both local and systemic inflammatory responses, which lead to an increase of pro-inflammatory and anti-inflammatory mediators. As a result, this can cause neuronal dysfunction or synaptic impairment, and finally, delirium [10, 11].
Corticosteroids, which are routinely used for the treatment of postoperative complications, are potent suppressors of inflammatory response. The effects of corticosteroids on reducing various inflammatory factors have been confirmed in those patients who underwent surgery [12,13,14]. Therefore, many researchers try to prevent or reduce POD with corticosteroids. Previous studies have demonstrated that preoperative corticosteroids could reduce the risk of POD in hip fractures [15,16,17]. In a double-blind, randomized, placebo-controlled feasible trial, Kluger et al. revealed that a single dose of 20 mg intravenous dexamethasone at hospital admission was associated with a reduced POD severity but not the occurrence in hip fracture patients [17]. However, it is not clear the safety of dexamethasone for patients with acute fractures in such a high dose. Moreover, the timing of dexamethasone used at hospital admission is probably too early for anesthesia and surgery. If the drug efficacy of the hospital admission dose of dexamethasone is gone, supplementary uses are prudent due to increasing the complication risks like infection and hyperglycemia. Hereby, we think that a low-dose dexamethasone intravenously used within 30 min before being sent to the operating room is not only safe for aging patients but also effective to reduce the impact of POD.
Therefore, we hypothesize that a single low dose of 10 mg dexamethasone intravenously administrated within 30 min before being sent to the operating room can reduce the incidence and severity of POD in geriatric ITF patients after internal fixation surgery.
Patients and methods
Study design
This study was a single-center, single-blinded, randomized, placebo-controlled trial, which complied with the Declaration of Helsinki and received ethics approvals from the ethics committees of the Guangzhou First People’s Hospital (Number: K-2020-106-01). All patients provided written informed consent. The study was registered at the Chinese Clinical Trials Registry (Registration number: ChiCTR2200055281). Patients were recruited by orthopedists between June 2020 and October 2022.
Participants
All patients were diagnosed with ITF by X-ray. Inclusion criteria: (1) age over 60 years, (2) required surgical treatment, (3) fracture within three weeks, and (4) capable of complying with the study protocol. Exclusion criteria: (1) systemic or fracture site infection before, (2) multiple traumas or open fractures, (3) stroke within 3 months or acute myocardial infarction within 6 months, (4) active peptic ulcer, (5) pathological fracture or pending fracture diagnosed by radiographic data, (6) chronic organic failure without effective replacement therapy, (7) advanced malignant tumor, (8) severe cognitive disorder (Mini-mental State Examination, MMSE ≤ 9 points) [18], (9) severe malnutrition (body mass index, BMI < 16) or overnutrition (BMI ≥ 35), (10) medication of systemic corticosteroids more than two weeks, and (11) patients who are considered to be inappropriate for participation by researchers.
Randomization
After the initial screening, all the patients were randomized into two groups (the dexamethasone group vs. the placebo group) with an allocation ratio of 1:1. The random number generated via SPSS (IBM SPSS Statistic for Windows, Version 25.0. Armonk, NY: IBM Corp) by a clinical research coordinator who was not involved in the study, and the results were concealed from the researchers. The assignment list was sealed in opaque envelopes, and they were opened to determine dexamethasone or placebo by the researchers after obtaining informed consent.
Baseline variables
Baseline characteristics included gender, age, Body Mass Index (BMI), fracture site, American Society of Anesthesiologists (ASA) classification, comorbidities, pre-injury living condition, Activities of Daily Life (ADL) [19], nutrition status according to Mini-Nutritional Assessment (MNA) [20], preoperative cognitive level according to Mini-Mental State Examination (MMSE) [18], hemoglobin and albumin levels at admission were collected. In addition, surgical data including fixation type, the timing of surgery, surgical time, anesthesia, blood loss, and intraoperative transfusion were collected.
Interventions
All ITF patients received treatments and interventions in the setting of standard Enhanced Recovery After Surgery (ERAS) procedure, of which the management content mainly included three parts included preoperative, intraoperative, and postoperative management. The preoperative management included education programs, auxiliary examination nutrition, nutrition management, pain management, DVT prevention, sleep management, and gastrointestinal management. On the morning of surgery, those patients allocated to the dexamethasone group received intravenous 10 mg (2 ml) dexamethasone (Dexamethasone Sodium Phosphate Injection, Tianjin Pharmacy), while the patients allocated to the placebo group received intravenous 2 ml physiological saline (0.9% sodium chloride injection) in 30 min before being sent to the operating room. The dexamethasone or physiological saline was given by an independent nurse who was not involved in the trial and was blinded to the patient’s outcome. All patients in this study underwent standard anesthesia procedures (including receiving routine sedatives and care) determined by the anesthesiologists who were blinded to patient allocation. Standard endotracheal general anesthesia was induced sequentially with sufentanil (0.5–0.7 μg/kg), cis-atracurium (0.16–0.2 mg/kg), and propofol (2–2.5 mg/kg) was maintained with propofol and sevoflurane. Remifentanil (0.05–2 μg/kg/min) was given intraoperatively as needed at the discretion of the anesthesiologists. Spinal anesthesia was administered with ropivacaine 0.5% (1.5–2.5 ml). Ultrasound-guided psoas compartment block was administered with ropivacaine 0.5% (20–30 ml). The intraoperative part included anesthesia selection, surgery optimization, and temperature management. The postoperative part included pain management, DVT prevention, respiratory management, and functional exercise. A detailed description of the ERAS procedure can be found in Additional file 1. POD was managed according to routine clinical practice. Nonpharmacological measures (such as visual/hearing aids, noise reduction, and avoidance of unnecessary indwelling catheters) were first performed. If the symptoms worsen or do not resolve, pharmacological measures would be considered according to the specialty consultant (0.25–1 mg of oral/intravenous haloperidol is given every 12 h as needed until symptom resolution).
Outcomes measures
The efficacy-related outcomes reported in this study were the incidence and severity of POD in the first 5 days after surgery. Patients were screened for POD using the Nursing Delirium Screening Scale (Nu-DESC) [21], an easy-to-use tool for assessing delirium in routine nursing care without requiring specialized knowledge [15]. The first screening was performed within 8 h after internal fixation surgery, and routine screening was performed twice a day (at 8 h intervals) in the first 5 days after surgery. A score of 2 or above on two consecutive assessments suggested possible POD. Afterward, patients suspected of POD were evaluated using the Memorial Delirium Assessment Scale (MDAS) by one researcher who was blinded to assignment twice a day [22]. It consisted of 10 items with a maximum score of 30, which assessed cognitive function including memory, attention, orientation, psychomotor activity, and so on. POD severity was determined by the average scores of MDAS.
Safety-related outcomes were infection events (including wound infection, postoperative pneumonia, and urinary infection), hyperglycemia, and maximum glucose in the first 3 days postoperatively (Additional file 1).
Sample size
The pre-specified sample size was calculated according to the primary outcome (1-year mortality after surgery) of a randomized, placebo-controlled trial. The incidence of primary outcome was as high as 23% or even 36% in previous studies [23, 24]. We hypothesized that 1-year mortality after surgery in the placebo group and the dexamethasone group was 36% and 15%, respectively. Therefore, we calculated that a total of 160 patients (80 patients in each group) were enough to detect the difference with a 5% type I error and a power of 80% in a two-sided test. The recruitment time was expected to be 16 months (from June 2020 to October 2021). However, affected by the COVID-19, the recruitment and study were extended to Oct 2022.
Statistical analysis
All analyses of related outcomes were performed according to the intention-to-treat principle. Continuous variables were assessed for normal distribution with a Q–Q plot and Kolmogorov–Smirnov test. Students t test were applied for normally distributed continuous variables and the Mann–Whitney U-test for non-normally distributed continuous variables. Chi-squared or Fisher’s exact tests were used to assess differences for categorical variables. Effect sizes for outcome variables were estimated according to the superiority effect size measure, of which the difference ≥ 0.56, ≥ 0.64, and ≥ 0.71 are considered small, medium, and large, respectively [25]. All statistical analyses were performed with SPSS Version 25.0. A p value below 0.05 was considered statistically significant.
Subgroup analyses were done post hoc to explore whether the overall primary outcome differed between groups (including gender, age, ASA, nutrition, cognitive levels, anemia, pain degree, time of surgery, surgery time, and anesthesia). The results are presented as a forest plot with the RRs and 95% CIs as well as p for interaction. The forest plot was generated using the “forestplot” R package in R studio (Version 4.1.2).
Results
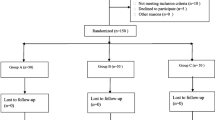
Between June 2020 and October 2022, a total of 219 patients were assessed for eligibility. Seventeen patients (7.76%) who did not meet the inclusion criteria and 42 patients (19.18%) who fulfilled the exclusion criteria were excluded. Finally, 160 patients were randomly assigned to either the dexamethasone group or the placebo group. No patient was withdrawn from the study. The flow chart is presented in Fig. 1

Flow diagram
Baseline characteristics and surgical data between groups did not have statistical differences (Tables 1, 2). Median (IQR) time from admission to intervention (nearly coincide with the time of surgery) in dexamethasone and placebo groups were approximately 89.9 [57.6, 135.6] and 94.3 [66.0, 142.5] hours; the difference was not significant (p = 0.228) (Table 2).
The efficacy-related outcomes and safety-related outcomes are shown in Table 3. The dexamethasone group had a significantly lower accumulated incidence of POD within the first 5 days after surgery compared with the placebo group (11.3%, 9/80 vs. 26.3%, 21/80, RR = 0.83, 95% CI 0.71–0.97, P = 0.015). Moreover, significantly lower MDAS scores (Mean ± SD, range) was also found in the dexamethasone group (13.2 ± 1.0, 11–15) compared with the placebo group (15.48 ± 2.9, 9–20), (P = 0.011, effect size = 0.514). Besides, there is a lower accumulated incidence rate of POD on the fourth day after surgery in the dexamethasone group (11.3%, 9/80, vs. 23.8, 19/80, RR = 0.86, 95% CI 0.74–0.99, P = 0.037) (Table 4). No significant differences were observed in the safety-related outcomes including wound infections, postoperative pneumonia, urinary infections, hyperglycemia, and maximum glucose. The adverse events were shown in Additional file 1.
The incidence and severity of POD in the first 5 days after surgery are presented in Table 4 and Fig. 2. The comparison of POD incidence in the first 5 days after surgery is shown in Table 4. No significant differences were observed in the incidence on each day in the first 5 days after surgery. Although there was a lower incidence of the POD in the first 3 days in the dexamethasone group than in the placebo group (8/80 10.0%, vs. 17/80, 21.3%), the difference did not reach significant (P = 0.05; RR = 0.88, 95% CI 0.76–1.00).

Comparison of incidence and severity of POD between two groups on the five days after surgery
Post hoc subgroup analysis was shown in Fig. 3. No significant interaction effect was observed in the two groups and all the 11 subgroups.

Relative risk for the POD in post hoc subgroups analysis. There were no significant interactions in all the 11 subgroups (P > 0.05 for all comparison)
Discussion
POD is a distributing problem in clinical practice, of which the pathogenesis, preventions, and treatments are still unclear [7]. Furthermore, POD is a complication associated with high prevalence and poor prognosis [26]. This single-blind, randomized control trial indicates that a single preoperative low-dose dexamethasone is beneficial in reducing both the incidence and the severity of POD in geriatric ITF after internal fixation surgery. The results provide theoretical basics for dexamethasone administration in optimizing ERAS clinical pathways of ITF.
Previous studies indicated that the incidence of POD in hip fractures varied from 14.3 to 25.0% [4,5,6]. Our study showed that the incidence of POD was 26.3% (21/80) in the placebo group, which is essentially in accordance with that reported in the literature [4,5,6]. The recognition and diagnosis of POD were great clinical concerns as the opinions divided into which tool is the best for evaluating POD [26,27,28]. In our study, Nu-DESC and MDAS were regarded as the screening measure of POD incidence and quantitative assessment of POD severity, respectively. Nu-DESC is the most useful method with high sensitivity for early diagnosis of POD, which is not required specific training to ensure optimum performance [27, 29]. As the severity of POD could not be assessed by Nu-DESC, MDAS was used as a definitive evaluation of both the incidence and severity of POD for its’ superiority in assessing delirium [28, 29]. The combination of Nu-DESC and MDAS for identifying POD is both efficient and precise. An MDAS score of 7.5 or more indicates delirium or is correlated with cognitive dysfunction after hip fracture [30]. In our study, the MDAS score of patients diagnosed with POD was at least 9 points (9–20), which might indicate a high accuracy in detecting and diagnosing POD.
Infections events and hyperglycemia are associated with the long-term use of high-dose steroids, but there is currently no clear evidence that a single low-dose dexamethasone given preoperatively increases these adverse events. A meta-analysis involving 51 studies confirmed that a single preoperative high-dose, short-acting corticosteroid did not increase the risk of postoperative complications after trauma surgery [31]. In this study, a higher pneumonia rate was found in the dexamethasone group, but the difference was not statistically significant. Prior studies have reported that low-dose dexamethasone used in arthroplasty surgery did not increase infection events [32, 33], yet whether high-dose dexamethasone would result in infection is still debatable and unclear [17, 34, 35]. A recent study concluded that a high dose of preoperative dexamethasone could potentially increase postoperative infection in long-term follow-up in hip fractures [17]. Besides, although no significant difference, higher hyperglycemia rates, and higher maximum glucose were found in the dexamethasone group in this study. Our findings are consistent with prior studies showing that blood glucose was raised after a single perioperative low dose of dexamethasone but there was no apparent increase in adverse effects [33, 35,36,37]. However, some studies have suggested that dexamethasone used in patients with diabetes mellitus should be prudent because of the uncertain effect. Thus, both the correlation between the dose and the infection and the effect of low-dose dexamethasone on patients with diabetes mellitus should be further investigated in future studies for their clinical significance.
The most important finding in this study is a single, preoperative, low-dose dexamethasone significantly reduced both the incidence and severity of POD in the first 5 days after surgery in geriatric ITF patients. The potential mechanism for this finding is dexamethasone reduces some POD-related inflammatory molecules like IL-1β by exerting anti-inflammatory effects [38, 39]. Besides, as the high concentration of endogenous cortisol has been demonstrated previously to be associated with POD [40], there is a possibility that preoperative dexamethasone could reduce endogenous cortisol levels by negative feedback of the hypothalamic‑pituitary‑adrenal axis [41]. But on the other hand, the between-group comparisons of daily POD incidence did not reach statistical significance. The reason for this observation may be partly attributed to the low incidence each day. Besides, the daily POD incidence in our study was the new-onset POD on that day, and the assessment of patients with POD was not consecutive and dynamic. We speculated that it would be lesser helpful for significant differences in daily incidence between the two groups.
There were some differences between our study and previous similar studies [16, 17]. Firstly, the observation duration of POD in this study was increased from 3 to 5 days after surgery to reduce the missed diagnosis of POD [29]. Our study found that the decrease in POD incidence was also observed in the first 3 days after surgery (10.0% vs. 21.3%), attributed to the half-life of dexamethasone being nearly 36–72 h [42]. However, Kluger’s study showed that high-dose dexamethasone could significantly reduce the POD severity but did not affect the POD incidence [17]. That could presumably explain the timing of dexamethasone administration. In Kluger’s study, dexamethasone was given as early as possible following hospital admission to reduce the neuro-inflammatory response to the initial trauma and surgery. However, that was probably too soon for the geriatric patients in such a high dose (20 mg), as both the comorbidities and rapid change of patient condition after fracture might prolong the timing of surgery. Secondly, our current study excluded patients with severe cognitive impairment (as assessed with MMSE) while Kluger’s study excluded the patients with cognitive impairment (as assessed with the 4AT test). However, cognitive impairment might result in a diverse effect on POD incidence as preoperative cognitive impairment is one of the foremost inducing factors for POD [4,5,6]. Then, the time from dexamethasone intervention to surgery varied considerably (0.3–46.8 h) in Kluger’s study, which might probably cause different effects of dexamethasone on initial fracture and subsequent surgery. Finally, the detection of delirium was performed twice a day (at 8 h intervals) in our study while once a day in Kluger’s study, which might reduce the risk of missed diagnosis of POD. Unlike some previous studies, the observation duration of POD in this study increased from 3 to 5 days after surgery to reduce the missed diagnoses in POD, as reported by the European Society of Anesthesiology evidence-based guidelines. Also, five patients with POD were observed in this study on the 4th and 5th day postoperatively, which led to statistical differences in the comparisons of POD accumulated incidence between the two groups in the first 4 or 5 days after surgery.
Although previous studies have reported that advanced age, gender, ASA grade, nutrition, comorbidities, preoperative cognitive disorder, preoperative anemia, pain degree, the timing of surgery, and surgery duration are the risk factors for POD [4,5,6,7, 43, 44], our result showed that there were no significant interactions between the two groups and in the subgroups (all p values for interaction were over 0.05) except for nutrition status. Limited by the sample size and uncertainty of emergency, the prior subgroup design was difficult to complete in a single center. Therefore, the post hoc subgroup analysis was performed to explore the effect of dexamethasone on POD in different subgroups. Our result showed no significant interactions between the dexamethasone and subgroups (all p values for interaction were over 0.05) except for nutrition status. Although no significant interaction effect (P = 0.08), lower POD incidence was observed in patients with malnutrition compared to the patients without malnutrition after dexamethasone intervention (RR = 0.54, 95 CI% 0.32–0.93). The reason is likely that the effect of physiological stress after fracture and surgery would be more pronounced in the patients without malnutrition, which is likely correlated with the poorly compensated function of the systemic organ. Also, malnutrition would induce glucocorticoid resistance and compromise the protective response to stress that is afforded by endogenous cortisol [45]. Furthermore, a significant fraction of cortisol activity receptors translocated to the nucleus, and the increased expression of inactive receptors was observed in malnutrition [45, 46], which might reduce the combination and activity of cortisol, but the mechanism that nutrition how influences the effect of corticosteroids on POD remains unknown. Certainly, this current study was done post hoc, and these results should be interpreted with caution as it is an exploratory analysis.
There were still several limitations in our study. First, the sample size was relatively small, and the power calculation was not precisely performed a priori, which is an inevitable drawback of this study. Although two different assessments (Nu-DESC and MDAS) and a relatively long observation duration for increasing the possibility of finding a POD were used to evaluate POD, these results should be interpreted as preliminary and hypothesis-driven for future studies. Second, the subjective bias of the investigator might be inevitable because of the single-blinded design. Third, patients with severe cognitive impairment who might have the highest risk of developing POD and suffer the greatest benefit from the intervention were not included in our study due to the protection of vulnerable groups. Fourth, anesthetic management without prespecified anesthetic protocols was left to the discretion of treating anesthesiologists, which might have a potential effect on the intervention. Fifth, prespecified stratified randomization was not performed at the recruitment, thereby further inferential conclusions about the impact of dexamethasone on subgroups could not be drawn. Finally, an increased probability of at least one false significant result might be inevitable due to the characteristic of secondary outcomes analysis. Therefore, the conclusion should necessarily be exploratory.
In conclusion, a single preoperative low-dose dexamethasone may reduce both the incidence and the severity of POD in geriatric ITF patients with internal fixation surgery.
Availability of data and materials
The dataset supporting the conclusions of this study is available upon request by contacting the corresponding author, but the primary data were not shared because other studies related these primary data were underway confidentially.
Code availability
Software applications used in this study are listed as follows: IBM SPSS Statistic for Windows, Version 25.0. Armonk, NY: IBM Corp; R.app GUI 1.79 (8160 High Sierra build), S. Urbanek & H.-J. Bibiko, © R Foundation for Statistical Computing, 2021 RStudio 2022.02.3 Build 386 © 2009–2023 Posit Software, PBC.
References
Cooper C, Campion G, Melton LJ. Hip fractures in the elderly: a world-wide projection. Osteoporos Int. 1992;2(6):285–9.
Dhanwal DK, Dennison EM, Harvey NC, Cooper C. Epidemiology of hip fracture: worldwide geographic variation. Indian J Orthop. 2011;45(1):15–22.
Berry SD, Rothbaum RR, Kiel DP, Lee Y, Mitchell SL. Association of clinical outcomes with surgical repair of hip fracture vs nonsurgical management in nursing home residents with advanced dementia. JAMA Intern Med. 2018;178(6):774–80.
Wu J, Yin Y, Jin M, Li B. The risk factors for postoperative delirium in adult patients after hip fracture surgery: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2021;36(1):3–14.
Yang Y, Zhao X, Dong T, Yang Z, Zhang Q, Zhang Y. Risk factors for postoperative delirium following hip fracture repair in elderly patients: a systematic review and meta-analysis. Aging Clin Exp Res. 2017;29(2):115–26.
Uzoigwe CE, O’Leary L, Nduka J, Sharma D, Melling D, Simmons D, et al. Factors associated with delirium and cognitive decline following hip fracture surgery. Bone Joint J. 2020;102-b(12):1675–81.
Bickel H, Gradinger R, Kochs E, Förstl H. High risk of cognitive and functional decline after postoperative delirium. A three-year prospective study. Dement Geriatr Cogn Disord. 2008;26(1):26–31.
van der Mast RC. Pathophysiology of delirium. J Geriatr Psychiatry Neurol. 1998;11(3):138–45; discussion 57–8.
Maldonado JR. Neuropathogenesis of delirium: review of current etiologic theories and common pathways. Am J Geriatr Psychiatry. 2013;21(12):1190–222.
Cerejeira J, Firmino H, Vaz-Serra A, Mukaetova-Ladinska EB. The neuroinflammatory hypothesis of delirium. Acta Neuropathol. 2010;119(6):737–54.
Cunningham C, Campion S, Lunnon K, Murray CL, Woods JF, Deacon RM, et al. Systemic inflammation induces acute behavioral and cognitive changes and accelerates neurodegenerative disease. Biol Psychiatry. 2009;65(4):304–12.
Clemmesen CG, Tavenier J, Andersen O, Palm H, Foss NB. Methylprednisolone and inflammatory stress response in older people undergoing surgery for hip fracture: a secondary analysis of a randomized controlled trial. Eur Geriatr Med. 2019;10(6):913–21.
Weis F, Beiras-Fernandez A, Schelling G, Briegel J, Lang P, Hauer D, et al. Stress doses of hydrocortisone in high-risk patients undergoing cardiac surgery: effects on interleukin-6 to interleukin-10 ratio and early outcome. Crit Care Med. 2009;37(5):1685–90.
Steinthorsdottir KJ, Kehlet H, Aasvang EK. Surgical stress response and the potential role of preoperative glucocorticoids on post-anesthesia care unit recovery. Minerva Anestesiol. 2017;83(12):1324–31.
Riegger H, Hollinger A, Seifert B, Toft K, Blum A, Zehnder T, et al. Baden Prevention and Reduction of Incidence of Postoperative Delirium Trial (PRIDe): a phase IV multicenter, randomized, placebo-controlled, double-blind clinical trial of ketamine versus haloperidol for prevention of postoperative delirium. Trials. 2018;19(1):142.
Clemmesen CG, Lunn TH, Kristensen MT, Palm H, Foss NB. Effect of a single pre-operative 125 mg dose of methylprednisolone on postoperative delirium in hip fracture patients; a randomised, double-blind, placebo-controlled trial. Anaesthesia. 2018;73(11):1353–60.
Kluger MT, Skarin M, Collier J, Rice DA, McNair PJ, Seow MY, et al. Steroids to reduce the impact on delirium (STRIDE): a double-blind, randomised, placebo-controlled feasibility trial of pre-operative dexamethasone in people with hip fracture. Anaesthesia. 2021;76(8):1031–41.
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–98.
Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–5.
Cohendy R, Gros T, Arnaud-Battandier F, Tran G, Plaze JM, Eledjam J. Preoperative nutritional evaluation of elderly patients: the Mini Nutritional Assessment as a practical tool. Clin Nutr. 1999;18(6):345–8.
Gaudreau JD, Gagnon P, Harel F, Tremblay A, Roy MA. Fast, systematic, and continuous delirium assessment in hospitalized patients: the nursing delirium screening scale. J Pain Symptom Manag. 2005;29(4):368–75.
Breitbart W, Rosenfeld B, Roth A, Smith MJ, Cohen K, Passik S. The memorial delirium assessment scale. J Pain Symptom Manag. 1997;13(3):128–37.
Zuckerman JD. Hip fracture. N Engl J Med. 1996;334(23):1519–25.
Li S, Sun T, Liu Z. Excess mortality of 1 year in elderly hip fracture patients compared with the general population in Beijing, China. Arch Osteoporos. 2016;11(1):35.
Delaney HD, Vargha A. Comparing several robust tests of stochastic equality with ordinally scaled variables and small to moderate sized samples. Psychol Methods. 2002;7(4):485–503.
Rizk P, Morris W, Oladeji P, Huo M. Review of postoperative delirium in geriatric patients undergoing hip surgery. Geriatr Orthop Surg Rehabil. 2016;7(2):100–5.
Aldecoa C, Bettelli G, Bilotta F, Sanders RD, Audisio R, Borozdina A, et al. European society of anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur J Anaesthesiol. 2017;34(4):192–214.
Jones RN, Cizginer S, Pavlech L, Albuquerque A, Daiello LA, Dharmarajan K, et al. Assessment of instruments for measurement of delirium severity: a systematic review. JAMA Intern Med. 2019;179(2):231–9.
De J, Wand AP. Delirium screening: a systematic review of delirium screening tools in hospitalized patients. Gerontologist. 2015;55(6):1079–99.
Shi Z, Wu Y, Li C, Fu S, Li G, Zhu Y, et al. Using the Chinese version of memorial delirium assessment scale to describe postoperative delirium after hip surgery. Front Aging Neurosci. 2014;6:297.
Sauerland S, Nagelschmidt M, Mallmann P, Neugebauer EA. Risks and benefits of preoperative high dose methylprednisolone in surgical patients: a systematic review. Drug Saf. 2000;23(5):449–61.
Mathiesen O, Jacobsen LS, Holm HE, Randall S, Adamiec-Malmstroem L, Graungaard BK, et al. Pregabalin and dexamethasone for postoperative pain control: a randomized controlled study in hip arthroplasty. Br J Anaesth. 2008;101(4):535–41.
Jules-Elysee KM, Lipnitsky JY, Patel N, Anastasian G, Wilfred SE, Urban MK, et al. Use of low-dose steroids in decreasing cytokine release during bilateral total knee replacement. Reg Anesth Pain Med. 2011;36(1):36–40.
Bergeron SG, Kardash KJ, Huk OL, Zukor DJ, Antoniou J. Perioperative dexamethasone does not affect functional outcome in total hip arthroplasty. Clin Orthop Relat Res. 2009;467(6):1463–7.
Waldron NH, Jones CA, Gan TJ, Allen TK, Habib AS. Impact of perioperative dexamethasone on postoperative analgesia and side-effects: systematic review and meta-analysis. Br J Anaesth. 2013;110(2):191–200.
Low Y, White WD, Habib AS. Postoperative hyperglycemia after 4- vs 8–10-mg dexamethasone for postoperative nausea and vomiting prophylaxis in patients with type II diabetes mellitus: a retrospective database analysis. J Clin Anesth. 2015;27(7):589–94.
O’Connell RS, Clinger BN, Donahue EE, Celi FS, Golladay GJ. Dexamethasone and postoperative hyperglycemia in diabetics undergoing elective hip or knee arthroplasty: a case control study in 238 patients. Patient Saf Surg. 2018;12:30.
Cape E, Hall RJ, van Munster BC, de Vries A, Howie SE, Pearson A, et al. Cerebrospinal fluid markers of neuroinflammation in delirium: a role for interleukin-1β in delirium after hip fracture. J Psychosom Res. 2014;77(3):219–25.
Palmi M, Frosini M, Becherucci C, Sgaragli GP, Parente L. Increase of extracellular brain calcium involved in interleukin-1 beta-induced pyresis in the rabbit: antagonism by dexamethasone. Br J Pharmacol. 1994;112(2):449–52.
van Munster BC, Bisschop PH, Zwinderman AH, Korevaar JC, Endert E, Wiersinga WJ, et al. Cortisol, interleukins and S100B in delirium in the elderly. Brain Cogn. 2010;74(1):18–23.
O’Keeffe ST, Devlin JG. Delirium and the dexamethasone suppression test in the elderly. Neuropsychobiology. 1994;30(4):153–6.
Parker CM, Cooper MN. Prednisolone versus dexamethasone for croup: a randomized controlled trial. Pediatrics. 2019;144(3):e20183772.
Qi YM, Li YJ, Zou JH, Qiu XD, Sun J, Rui YF. Risk factors for postoperative delirium in geriatric patients with hip fracture: A systematic review and meta-analysis. Front Aging Neurosci. 2022;14:960364.
Juliebø V, Bjøro K, Krogseth M, Skovlund E, Ranhoff AH, Wyller TB. Risk factors for preoperative and postoperative delirium in elderly patients with hip fracture. J Am Geriatr Soc. 2009;57(8):1354–61.
Manary MJ, Muglia LJ, Vogt SK, Yarasheski KE. Cortisol and its action on the glucocorticoid receptor in malnutrition and acute infection. Metabolism. 2006;55(4):550–4.
Bamberger CM, Bamberger AM, de Castro M, Chrousos GP. Glucocorticoid receptor beta, a potential endogenous inhibitor of glucocorticoid action in humans. J Clin Invest. 1995;95(6):2435–41.
Acknowledgements
We gratefully acknowledge L Li for his C-arm X-ray assistance during surgery.
Funding
Partially supported by the fund of Guangzhou municipal health commission (No. 2023C-TS32).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. The study was designed by YY. Material preparation and study were performed by all authors. The data collection and analysis were performed by JH, XG, ZX and YY. The first draft of the manuscript was written by JH and was revised by YY. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Guangzhou First People’s Hospital (K-2020-106-01). All patients in this study provided written informed consent after related complications and possible outcomes had been explained.
Consent for publication
All the authors have approved manuscript for publication.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. The ERAS procedure, Diagnostic criteria of safety-related outcomes, and Postoperative adverse events during hospitalization.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huang, Jw., Yang, Yf., Gao, Xs. et al. A single preoperative low-dose dexamethasone may reduce the incidence and severity of postoperative delirium in the geriatric intertrochanteric fracture patients with internal fixation surgery: an exploratory analysis of a randomized, placebo-controlled trial. J Orthop Surg Res 18, 441 (2023). https://doi.org/10.1186/s13018-023-03930-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-03930-2