
Abstract
Background
With the popularization of robot-assisted spinal surgeries, it is still uncertain whether robots with different designs could lead to different results in the accuracy of pedicle screw placement. This study aimed to compare the pedicle screw inserting accuracies among the spinal surgeries assisted by various types of robot and estimate the rank probability of each robot-assisted operative technique involved.
Methods
The electronic literature database of PubMed, Web of Science, EMBASE, CNKI, WANFANG and the Cochrane Library was searched in November 2021. The primary outcome was the Gertzbein–Robbins classification of pedicle screws inserted with various operative techniques. After the data extraction and direct meta-analysis process, a network model was established in the Bayesian framework and further analyses were carried out.
Results
Among all the 15 eligible RCTs, 4 types of robot device, namely Orthbot, Renaissance, SpineAssist and TiRobot, were included in this study. In the network meta-analysis, the Orthbot group (RR 0.27, 95% CI 0.13–0.58), the Renaissance group (RR 0.33, 95% CI 0.14–0.86), the SpineAssist group (RR 0.14, 95% CI 0.06–0.34) and the conventional surgery group (RR 0.21, 95% CI 0.13–0.31) were inferior to the TiRobot group in the proportion of grade A pedicle screws. Moreover, the results of rank probabilities revealed that in terms of accuracy, the highest-ranked robot was TiRobot, followed by Renaissance and Orthbot.
Conclusions
In general, current RCT evidence indicates that TiRobot has an advantage in the accuracy of the pedicle screw placement, while there is no significant difference among the Orthbot-assisted technique, the Renaissance-assisted technique, the conventional freehand technique, and the SpineAssist-assisted technique in accuracy.
Similar content being viewed by others

Introduction
The precise insertion of pedicle screws plays a central role in pedicle screw fixation, which provides three-column stabilization and is widely used in spine surgery. There were considerable variabilities in the anatomy of vertebral landmarks and the structure of pedicles due to specific physical or pathological variations. Even if pedicle screw insertion is the most foundational operation for spine surgeons, it is still hard to insert all pedicle screws precisely by the conventional freehand method [1]. Deviations in the placement without deviation are associated with a reduction of biomechanical strength and even a series of complications such as spinal instability, vascular injuries, and neurologic injuries [2].
With the advance of computer-assisted navigation technology and spinal robot technology, traditional pedicle screw placement has been partially replaced. Both navigation technology and robotic technology guide screw placement according to the three-dimensional mapping of the vertebrae; the major difference being surgeon-guided vs. robot-guided execution of the screw trajectory [3, 4]. There is no denying that the arrival of the spinal operative robot is a potential milestone in the development of spine surgery. With the maturity of robot technology, some revolutionary spinal robot products have been applied in clinical practice. Most spinal robot products are originally designed for navigation and positioning during operation. Therefore, these robots are especially suitable for the placement of pedicle screws. The application of spinal robots shows excellent promise in avoiding the drawbacks of the conventional freehand method, such as the instability of human hands. Consequently, robot-assisted spinal surgery is becoming increasingly prevalent.
In the comparison of robot-assisted surgery and conventional spinal surgery, the accuracy of pedicle screw insertion seems controversial. Even though most previous studies support the conclusion that the use of spinal robots can increase accuracy in pedicle screw insertion [5, 6], there are also some contradictory arguments [7, 8]. Moreover, there is no direct comparison report or intensive study on different types of spinal robot. It is still uncertain whether robots with different designs and structures can lead to different clinical results, such as the accuracy of pedicle screw placement.
The Bayesian network meta-analysis (NMA) approach allows for comparing methods that have never been compared directly through the common comparator. Therefore, the purpose of this NMA was to indirectly compare the pedicle screw inserting accuracies among the spinal surgeries assisted by various types of robot by evaluating data from published prospective randomized controlled trials. Furthermore, the rank probability of each particular spinal robot was estimated based on the Bayesian approach.
Materials and methods
This Bayesian network meta-analysis was reported according to the PRISMA for Network Meta-Analyses (PRISMA-NMA) statement [9]. Moreover, this research was registered in the PROSPERO database (CRD42021288938).
Searching and screening strategy
Up to November 2021, a comprehensive search was performed through PubMed, Web of Science, EMBASE, CNKI, WANFANG, and the Cochrane Library using a combination of the terms “robot-assisted,” “robotic,” “robot-aided,” “spine,” ”spinal” and “pedicle screw.” Two independent authors carried out the searching process without language limitation and screened records by title and abstracts. Then, probably eligible reports were examined with the same eligibility criteria. Discrepancies were discussed in the group meeting all members reached an agreement.
Eligibility criteria
Inclusion criteria were as follows: (a) prospective randomized controlled trials; (b) clinical trials performed on human beings; (c) adult patients (older than 18 years old); (d) patients with degenerative or traumatic spinal diseases; (e) patients undergoing lumbar, thoracolumbar or lumbosacral spine surgery with pedicle screw implantation; (f) comparison of the robot-assisted operative method and conventional operative method or two robot-assisted operative methods; (g) Accuracy of pedicle screw placement was evaluated by Gertzbein–Robbins Scale. Exclusion criteria were as follows: (a) cadaveric studies; (b) patients with spinal scoliosis; and (c) conference articles, editorials, or letters.
Quality assessment and data extraction
For each eligible report, two independent authors evaluated the quality according to the Cochrane risk of bias assessment scale, and the data were then extracted independently. The extracted items were as follows: (a) authors; (b) year of publication; (c) country; (d) study design; (e) disease; (f) the type of surgery; (g) robot devices; (h) the age of patients; (i) the gender of patients; (j) the number of patients; (k) instrumented vertebral body; (l) the number of pedicle screws; (m) pedicle screws classified by Gertzbein–Robbins Scale, etc. During the assessing and extracting process, the whole team checked and discussed all discrepancies.
Data analysis
The meta-analysis and Network meta-analysis were conducted using STATA statistical software and ADDIS software. P < 0.05 was set as the level of significance. The Risk ratio (RR) and corresponding 95% confidence interval (CI) were used to compare dichotomous variables. The random-effects model was used regardless of the heterogeneity. Moreover, the statistical heterogeneity was assessed with the forest plot and inconsistency statistic (I-squared). The funnel plot was used to evaluate reports for publication bias. As for the Bayesian network analysis, a network consistency model was built with Markov chain Monte Carlo methods [10]. The translated binary results of pedicle screw placement were networked and the relations among the risk ratios across the network were specified, as Cipriani et al. reported [11]. The RR of each operative procedure was calculated, and the proportion of iterations of the Markov chain of the RR ranking was counted so that the rank probability of each operative procedure could be estimated. The cumulative ranking curve and surface under the cumulative ranking curve (SUCRA) were also conducted. P < 0.05 and 95% CIs beyond the null value were adopted to assess the significance.
Results
Studies involved
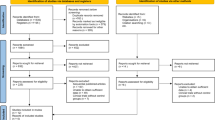
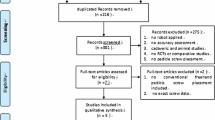
A total of 2372 candidate records were identified through database searching. After removing duplicates, 2138 records were screened by title and abstract. Of the 153 potential studies further assessed with the full text, 138 were excluded according to the inclusion and exclusion criteria details. The final number of eligible studies involved was fifteen (Fig. 1). The results of the quality assessment are shown in Fig. 2. The characteristics of the eligible studies are summarized in Table 1. Overall, 988 patients and 4594 pedicle screws were included in this study. There is no direct comparative study on different types of spinal robot device. All the studies were randomized controlled trials involving the comparison of the conventional spinal operation and the robot-assist operation with one particular type of spinal robot. Four types of robot device, namely Orthbot [12,13,14], Renaissance [8, 15, 16], SpineAssist [7, 17] and TiRobot [18,19,20,21,22,23,24], were included (Fig. 3). All 15 studies used the Gertzbein–Robbins Scale to describe early radiological outcomes of pedicle screws.

The flowchart of the searching and screening process

Risk of bias summary: green for low risk of bias, yellow for unclear bias and red for high risk of bias

The network plot of spinal operation with freehand and different robot types. The size of the node represents the number of patients. The line between nodes represents the existence of direct comparison, and the width of lines is proportional to the number of studies
Direct meta-analysis
Based on the Gertzbein–Robbins classification outcome reported by eligible studies, the direct meta-analysis revealed a significant difference between the overall robot-assisted operation group and the conventional group in the proportion of grade A pedicle screws (RR = 1.07, 95% CI 1.04–1.11). Further subgroup analysis by the type of robot device was carried out due to the existence of heterogeneity (I-squared = 68.9%, p < 0.001). In terms of the comparison to the conventional group in the proportion of grade A pedicle screws, the TiRobot subgroup (RR = 1.11, 95% CI 1.07–1.16, I-squared = 71.3%, p = 0.002) was detected with a significant difference, while the subgroups of Orthbot (RR = 1.07, 95% CI 0.97–1.19, I-squared = 0.0%, p = 0.552), Renaissance (RR = 1.03, 95% CI 0.99–1.06, I-squared = 0.0%, p = 0.925) and SpineAssist (RR = 0.93, 95% CI 0.77–1.13, I-squared = 76.5%, p = 0.039) were not significant (Fig. 4).

Forest plot showing the direct meta-analysis of the Gertzbein–Robbins classification of pedicle screws inserted with various operative techniques
Network meta-analysis
In light of the Bayesian approach, a consistency network model was established from the studies involved, and the median of variance parameters of which was 0.23 (95% CrI 0.01–0.77). According to the proportion of pedicle screws without breach of the cortical layer of the vertebral body or pedicle (Gertzbein–Robbins grade A), Fig. 5 summarizes the league tables with RR and 95% CIs of operative methods compared with each other. Taking the TiRobot group as reference, the Orthbot group (RR 0.27, 95% CI 0.13–0.58), the Renaissance group (RR 0.33, 95% CI 0.14–0.86), the SpineAssist group (RR 0.14, 95% CI 0.06–0.34) and the conventional surgery group (RR 0.21, 95% CI 0.13–0.31) showed significantly lower rates of grade A screws.

Multiple comparisons for pedicle screw inserting accuracy based on the network consistency model. Results are presented as relative risks with 95% confidence intervals
Rank probabilities
On the basis of the network model, the rank probability of each operative method was estimated (Fig. 6A). Each color represented one accuracy hierarchy, and the overall distribution was represented by histogram. Similarly, Fig. 6B shows the cumulative probabilities for each operative method at each possible rank. Larger SUCRA indicated better rank among all involved operative methods. Specifically, the SUCRA of the Orthbot group, the Renaissance group, the SpineAssist group, the TiRobot group and the conventional surgery group were, respectively, 64.0%, 77.8%, 18.0%, 99.8% and 40.0%.

A Histogram showing the distribution of ranking probabilities of each operative technique in accuracy. B Cumulative ranking plots comparing each of the operative techniques in pedicle screw inserting accuracy
Discussion
In the wake of developments in science and technology, the dream of robotic spinal surgery has come into reality. Even though most current spinal robot products were mainly designed for navigation and positioning during operation, these revolutionary robot devices can provide tremendous assistance in spinal surgery. Although designed by different companies and endowed with particular characteristics, these spinal robots have some similarities in both structure and function. And the vast majority of these robots, including SpineAssist (2004, Mazor Robotics Ltd., Caesarea, Israel), Renaissance (2011, Mazor Robotics Ltd., Caesarea, Israel), Excelsius GPS (2017, Globus Medical, Inc., Audubon, Pennsylvania, USA), TiRobot (2016, TINAVI Medical Technologies, Beijing, China), Orthbot (2019, Xin Junte, Shenzhen, China), and Mazor X Stealth Edition (2019, Medtronic, Memphis, TN, USA), are shared-control robots which allow both the robot and operator to control motions simultaneously [25, 26].
SpineAssist, the first shared-control robot approved by the FDA for use in spine surgery, mounts onto vertebral landmarks directly and aligns its arm along the designed trajectory. The location of the entry point and the direction for the guide wire are thus determined [27]. SpineAssist can merge preoperative CT with intraoperative fluoroscopy, and the planning of the target trajectory relies on CT imaging. Renaissance, the successor of SpineAssist, also requires a patient-mounted track. Renaissance contains some improvements in hardware and software on the basis of the first-generation Mazor robot, such as improved artifact rejection, faster image processing speed, and the ability to flatten bone at the entry points in order to avoid skiving [28, 29]. Neither SpineAssist nor Renaissance is equipped with integrated navigation [28]. Computer-assisted navigation allows for clearer visualizations of structural anatomy during spinal surgery [30]. After years of development, navigation technology has evolved from early two-dimensional navigation based on fluoroscopy to intraoperative computed tomography-based navigation [31]. The development of both computer-assisted navigation and spinal robot technology complements each other; in fact, many spinal robots are even considered special applications of three-dimensional navigation [32]. Most of recent spinal robot productions have been integrated with navigation systems. Excelsius GPS addresses several shortages of many previous spine robots, such as inaccurate registration and inaccurate navigation. The tubular robotic arm is able to withstand significant lateral force without displacement. Therefore, Excelsius GPS allows for screw placement without the usage of Kirschner wires [33]. TiRobot, a multi-indication orthopedic robot, is consisted of an optical tracking device, a robotic arm and a robotic workstation. The movement of the robotic arm is under the supervision of the stereo-tracking device. The intraoperative 3D navigation image, acquired from the C‐arm scanner and reconstructed by the workstation, can help to carry out the planning of the screw trajectories by checking trajectories and anatomical landmarks in real time. Before inserting the screw, a Kirschner wire has to be drilled along the robotic guided cannula as the guiding pin [26]. Though most spine robots are incapable of automatic drilling, Orthbot is an exception. A bone drill is combined into the mechanical arm, which is composed of a motor and a force sensor that can monitor the drilling pressure. Therefore, Orthbot has the capability to drill and insert the Kirschner wire autonomously [14]. As the latest generation of Mazor spine robot, Mazor X Stealth Edition includes an intraoperative O-arm scan, which makes it possible to provide real-time visualization of the drilling and screw placement process. In addition, Mazor X Stealth Edition obviates the need for a percutaneous pin and the need for a preoperative CT scan [34]. Being considered as representatives, these robots signify the inheritance and developmental direction for spinal robots in some ways; nonetheless, previous clinical studies have not yet provided enough high-quality evidence for each type of robot. According to the current result of the literature search, SpineAssist, Renaissance, TiRobot, and Orthbot have been investigated by randomized controlled trials. Therefore, these four types of spinal robot were the research objects of this study.
In accordance with previous reports [5, 6, 35], the result of the direct meta-analysis ((RR = 1.07, 95% CI 1.04–1.11)) confirms that the robot-assisted method is superior to the conventional technique in accuracy. Moreover, further subgroup analysis by the type of robot device shows the main positive effect is original from the subgroup of TiRobot (RR = 1.11, 95% CI 1.07–1.16). Moreover, no obvious publication bias is found in the funnel plot (Fig. 7). However, almost all previous research and traditional meta-analyses focused on the difference between the freehand technique and robot-assisted technique in spine surgery. In terms of various types of spinal robot, there was not sufficient research or even direct literature evidence.

A The funnel plot of the Orthbot group. B The funnel plot of the Renaissance group. C The funnel plot of the SpineAssist group. D The funnel plot of the TiRobot group
Through the common comparator, the NMA approach could compare various operative techniques indirectly without direct evidence. In order to compare the accuracies of different types of spinal robot, the Bayesian framework network was established so that the indirect connection of robot-assisted techniques could be linked through the common comparator technique, and indirect evidence could be further incorporated. The NMA has been recognized as a credible approach to comparing various treatments or techniques for its high consistency with reality [36]. The TiRobot-assisted technique shows higher accuracy than other techniques, while no significant difference was detected among other techniques. In addition, the Bayesian chain can be used to quantify the uncertainty and rank these techniques by measuring the corresponding probability [37]. In terms of the accuracy of pedicle screw placement, the TiRobot-assisted technique has a great probability of ranking first, followed by the Renaissance-assisted technique, the Orthbot-assisted technique, the conventional freehand technique and the SpineAssist-assisted technique.
The four types of spinal robot involved in this study, namely SpineAssist (entering the market in 2004), Renaissance (entering the market in 2011), TiRobot (entering the market in 2016) and Orthbot (entering the market in 2019), represent the inheritance and development history of robot-assisted spinal surgery to some extent. Compared with SpineAssist, the second-generation counterpart Renaissance has some improvements in both software and hardware. But it is reported that these two robots face a similar problem of screw misplacement secondary to skiving [27, 38], which may partially explain the rank probabilities (Fig. 6). With the progress of technology, the automation and intelligence levels of spinal robots have increased gradually. Orthbot is even capable of drilling and inserting the Kirschner wire autonomously. However, the introduction of the automatic drilling function might be associated with some losses in accuracy. The accuracy of the screw placement assisted by Orthbot is not significantly different from the conventional freehand group or the Renaissance group but inferior to the TiRobot group. Generally, the automation and accuracy of spinal robots gradually increase in the process of inheritance and development. According to the surface under the cumulative ranking curve, TiRobot ranks first on the accuracy of pedicle screw placement, followed by Renaissance, Orthbot, conventional technique, and SpineAssist. Launched in 2016, TiRobot reaches a peak in terms of accuracy. Along with the introduction of the automatic drilling function, the more recent Orthbot operates with a potential accuracy loss, while there is no significant difference among the Orthbot-assisted technique, the Renaissance-assisted technique, the SpineAssist technique, and the conventional technique in pedicle screw inserting accuracy based on the Bayesian network.
In this study, there were quite large differences in the number of studies and sample sizes between groups. The design of the Bayesian method represents dependencies between multiple variables as conditional probability distributions [39]. Accordingly, we could explicitly eliminate these differences by quantifying the joint probability of each group, obtaining objective comparison results. For the TiRobot group with the largest sample size, there was significant heterogeneity within the group (I-Squared = 71.3%). As a consequence, we conducted further influence analysis on the TiRobot group (Additional file 1: Fig. S1). Combining the results of the influence analysis and forest plot (Fig. 4), the study by Xu et al. [18] was the largest outlier effect source, which may have overestimated the positive effects of TiRobot. After excluding this study, the heterogeneity of the TiRobot group was significantly reduced (I-Squared = 59.4%), and the result of the direct meta-analysis remained significant (Additional file 1: Fig. S2). Compared to the original analysis, the resulting consistency network model of Bayesian network meta-analysis achieved a similar median variance parameter of 0.21 (95% CrI 0.01–0.75). Although the results changed slightly in numerical terms, the final conclusion remained unchanged (Additional file 1: Figs. S3 and S4). In addition, due to the limitation of the number of studies, other groups could not be further analyzed this way.
There are several limitations of this Bayesian network meta-analysis. Firstly, even if we have tried to select studies with relative homogeneity and high quality of evidence by setting strict criteria, some heterogeneities exist among the studies involved. Though clinical heterogeneity is inevitable, it makes little impact on the final conclusion. Secondly, accuracy is undoubtedly the most concerning outcome for robot-assisted spinal surgery, while other indexes such as radiation exposure, operative time, bleeding amount, and complication rate are also important. But currently available evidence cannot support comprehensive network meta-analyses for outcomes except for the accuracy of screw placement.
Conclusions
Current RCT evidence indicates that TiRobot has an advantage in the accuracy of the pedicle screw placement, while there is no significant difference among the Orthbot-assisted technique, the Renaissance-assisted technique, the conventional freehand technique, and the SpineAssist-assisted technique in accuracy. With the popularization of robot-assisted spinal surgeries and the emergence of new spinal robots, more well-designed randomized controlled trials and further studies are required in future.
Availability of data and materials
The data are available from the corresponding author on reasonable request.
Abbreviations
- RR:
-
Relative risk
- CI:
-
Confidence interval
- RCT:
-
Randomized controlled trials
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- NMA:
-
Network meta-analysis
- CrI:
-
Credible interval
- FDA:
-
Food and Drug Administration
- SUCRA:
-
The surface under the cumulative ranking curve
References
Hicks JM, Singla A, Shen FH, et al. Complications of pedicle screw fixation in scoliosis surgery: a systematic review. Spine. 2010. https://doi.org/10.1097/BRS.0b013e3181d1021a.
McCormick J, Aebi M, Toby D, et al. Pedicle screw instrumentation and spinal deformities: have we gone too far? Eur Spine J. 2013. https://doi.org/10.1007/s00586-012-2300-5.
Sielatycki JA, Mitchell K, Leung E, et al. State of the art review of new technologies in spine deformity surgery-robotics and navigation. Spine Deform. 2022. https://doi.org/10.1007/s43390-021-00403-6.
Nathoo N, Cavusoglu MC, Vogelbaum MA, et al. In touch with robotics: neurosurgery for the future. Neurosurgery. 2005. https://doi.org/10.1227/01.neu.0000153929.68024.cf.
Tarawneh AM, Salem KM. A systematic review and meta-analysis of randomized controlled trials comparing the accuracy and clinical outcome of pedicle screw placement using robot-assisted technology and conventional freehand technique. Global Spine J. 2021. https://doi.org/10.1177/2192568220927713.
Li HM, Zhang RJ, Shen CL. Accuracy of pedicle screw placement and clinical outcomes of robot-assisted technique versus conventional freehand technique in spine surgery from nine randomized controlled trials: a meta-analysis. Spine. 2020. https://doi.org/10.1097/BRS.0000000000003193.
Ringel F, Stuer C, Reinke A, et al. Accuracy of robot-assisted placement of lumbar and sacral pedicle screws: a prospective randomized comparison to conventional freehand screw implantation. Spine. 2012. https://doi.org/10.1097/BRS.0b013e31824b7767.
Hyun SJ, Kim KJ, Jahng TA, et al. Minimally invasive robotic versus open fluoroscopic-guided spinal instrumented fusions: a randomized controlled trial. Spine. 2017. https://doi.org/10.1097/BRS.0000000000001778.
Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015. https://doi.org/10.7326/M14-2385.
Valkenhoef G, Tervonen T, Zwinkels T, et al. ADDIS: a decision support system for evidence-based medicine. Decis Support Syst. 2013. https://doi.org/10.1016/j.dss.2012.10.005.
Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet. 2009. https://doi.org/10.1016/S0140-6736(09)60046-5.
Li Z, Chen J, Zhu QA, et al. A preliminary study of a novel robotic system for pedicle screw fixation: a randomised controlled trial. J Orthop Translat. 2020. https://doi.org/10.1016/j.jot.2019.09.002.
Li J, Huang L, Zhou W, et al. Evaluation of a new spinal surgical robotic system of Kirschner wire placement for lumbar fusion: a multi-centre, randomised controlled clinical study. Int J Med Robot. 2021. https://doi.org/10.1002/rcs.2207.
Li J, Wang Z, Zeng L, et al. Application and evaluation of an independent robotic arm system in K-wire placement for lumbar fusion. Clin Spine Surg. 2021. https://doi.org/10.1097/BSD.0000000000001191.
Kim HJ, Jung WI, Chang BS, et al. A prospective, randomized, controlled trial of robot-assisted vs freehand pedicle screw fixation in spine surgery. Int J Med Robot. 2017. https://doi.org/10.1002/rcs.1779.
Kim HJ, Lee SH, Chang BS, et al. Monitoring the quality of robot-assisted pedicle screw fixation in the lumbar spine by using a cumulative summation test. Spine. 2015. https://doi.org/10.1097/BRS.0000000000000680.
Roser F, Tatagiba M, Maier G. Spinal robotics: current applications and future perspectives. Neurosurgery. 2013. https://doi.org/10.1227/NEU.0b013e318270d02c.
Xu P, Ge P, Zhang RJ, et al. Effect of robot assisted pedicle screw fixation in the treatment of thoracolumbar fracture. J Cervicodynia Lumbodynia. 2018. https://doi.org/10.3969/j.issn.1005-7234.2018.06.004.
Tian W, Fan MX, Han XG, et al. Pedicle screw insertion in spine: a randomized comparison study of robot-assisted surgery and fluoroscopy-guided techniques. J Clin Orthop Res. 2016. https://doi.org/10.19548/j.2096-269x.2016.01.003.
Huang J, Han B, Liu JX et al. Clinical effect for orthopaedic robot assisted minimally invasive lumbar internal fixation surgery. Beijing Biomed Eng. 2020;
Feng S, Tian W, Sun Y, et al. Effect of robot-assisted surgery on lumbar pedicle screw internal fixation in patients with osteoporosis. World Neurosurg. 2019. https://doi.org/10.1016/j.wneu.2019.01.243.
Han X, Tian W, Liu Y, et al. Safety and accuracy of robot-assisted versus fluoroscopy-assisted pedicle screw insertion in thoracolumbar spinal surgery: a prospective randomized controlled trial. J Neurosurg Spine. 2019. https://doi.org/10.3171/2018.10.SPINE18487.
Yang R, Li Y, Zhang K, et al. Clinical application and experience of pedicle screw insertion assisted by tianjiorthopaedic robot. J Pract Orthop. 2019. https://doi.org/10.13795/j.cnki.sgkz.2019.10.008.
Feng S, Tian W, Wei Y. clinical effects of oblique lateral interbody fusion by conventional open versus percutaneous robot-assisted minimally invasive pedicle screw placement in elderly patients. Orthop Surg. 2020. https://doi.org/10.1111/os.12587.
Overley SC, Cho SK, Mehta AI, et al. Navigation and robotics in spinal surgery: where are we now? Neurosurgery. 2017. https://doi.org/10.1093/neuros/nyw077.
Huang M, Tetreault TA, Vaishnav A, et al. The current state of navigation in robotic spine surgery. Ann Transl Med. 2021. https://doi.org/10.21037/atm-2020-ioi-07.
D’Souza M, Gendreau J, Feng A, et al. Robotic-assisted spine surgery: history, efficacy, cost and future trends. Robot Surg. 2019. https://doi.org/10.2147/RSRR.S190720.
Alluri RK, Avrumova F, Sivaganesan A, et al. Overview of robotic technology in spine surgery. HSS J. 2021. https://doi.org/10.1177/15563316211026647.
Devito DP, Woo R. History and evolution of spinal robotics in pediatric spinal deformity. Int J Spine Surg. 2021. https://doi.org/10.14444/8141.
Virk S, Qureshi S. Navigation in minimally invasive spine surgery. J Spine Surg. 2019. https://doi.org/10.21037/jss.2019.04.23.
Kirnaz S, Gebhard H, Wong T, et al. Intraoperative image guidance for cervical spine surgery. Ann Transl Med. 2021. https://doi.org/10.21037/atm-20-1101.
Hussain I, Cosar M, Kirnaz S, et al. Evolving navigation, robotics, and augmented reality in minimally invasive spine surgery. Global Spine J. 2020. https://doi.org/10.1177/2192568220907896.
Jiang B, Karim Ahmed A, Zygourakis CC, et al. Pedicle screw accuracy assessment in ExcelsiusGPS(R) robotic spine surgery: evaluation of deviation from pre-planned trajectory. Chin Neurosurg J. 2018. https://doi.org/10.1186/s41016-018-0131-x.
O’Connor TE, O’Hehir MM, Khan A, et al. Mazor X stealth robotic technology: a technical note. World Neurosurg. 2021. https://doi.org/10.1016/j.wneu.2020.10.010.
Li C, Li W, Gao S, et al. Comparison of accuracy and safety between robot-assisted and conventional fluoroscope assisted placement of pedicle screws in thoracolumbar spine: a meta-analysis. Medicine. 2021. https://doi.org/10.1097/MD.0000000000027282.
Beliveau A, Boyne DJ, Slater J, et al. BUGSnet: an R package to facilitate the conduct and reporting of Bayesian network meta-analyses. BMC Med Res Methodol. 2019. https://doi.org/10.1186/s12874-019-0829-2.
Efthimiou O, Debray TP, van Valkenhoef G, et al. GetReal in network meta-analysis: a review of the methodology. Res Synth Methods. 2016. https://doi.org/10.1002/jrsm.1195.
Hu X, Ohnmeiss DD, Lieberman IH. Robotic-assisted pedicle screw placement: lessons learned from the first 102 patients. Eur Spine J. 2013. https://doi.org/10.1007/s00586-012-2499-1.
Kaikkonen L, Parviainen T, Rahikainen M, et al. Bayesian networks in environmental risk assessment: a review. Integr Environ Assess Manag. 2021. https://doi.org/10.1002/ieam.4332.
Acknowledgements
We appreciate the efforts of all the researchers whose trials were included in this study.
Funding
This study was funded by CAMS Innovation Fund for Medical Sciences (CIFMS) (2021-I2M-5-007).
Author information
Authors and Affiliations
Contributions
WT and DH contributed to the design of the work. Q-LW and QZ were involved in the searching and screening process. QZ and L-ZX contributed to the quality assessment and data extraction process. L-ZX and Q-LW were involved in the analysis process. L-ZX contributed to the writing of the original draft. DH and WT were involved in the review and editing of the draft. Supervision: DH. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Further analyses related to the heterogeneity of the TiRobot group.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xie, LZ., Wang, QL., Zhang, Q. et al. Accuracies of various types of spinal robot in robot-assisted pedicle screw insertion: a Bayesian network meta-analysis. J Orthop Surg Res 18, 243 (2023). https://doi.org/10.1186/s13018-023-03714-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-03714-8