
Abstract
Background
Reduction or elimination of inappropriate, ineffective, or potentially harmful healthcare services and public health programs can help to ensure limited resources are used effectively. Frameworks and models (FM) are valuable tools in conceptualizing and guiding the study of de-implementation. This scoping review sought to identify and characterize FM that can be used to study de-implementation as a phenomenon and identify gaps in the literature to inform future model development and application for research.
Methods
We searched nine databases and eleven journals from a broad array of disciplines (e.g., healthcare, public health, public policy) for de-implementation studies published between 1990 and June 2020. Two raters independently screened titles and abstracts, and then a pair of raters screened all full text records. We extracted information related to setting, discipline, study design, methodology, and FM characteristics from included studies.
Results
The final search yielded 1860 records, from which we screened 126 full text records. We extracted data from 27 articles containing 27 unique FM. Most FM (n = 21) were applicable to two or more levels of the Socio-Ecological Framework, and most commonly assessed constructs were at the organization level (n = 18). Most FM (n = 18) depicted a linear relationship between constructs, few depicted a more complex structure, such as a nested or cyclical relationship. Thirteen studies applied FM in empirical investigations of de-implementation, while 14 articles were commentary or review papers that included FM.
Conclusion
De-implementation is a process studied in a broad array of disciplines, yet implementation science has thus far been limited in the integration of learnings from other fields. This review offers an overview of visual representations of FM that implementation researchers and practitioners can use to inform their work. Additional work is needed to test and refine existing FM and to determine the extent to which FM developed in one setting or for a particular topic can be applied to other contexts. Given the extensive availability of FM in implementation science, we suggest researchers build from existing FM rather than recreating novel FM.
Registration
Not registered
Similar content being viewed by others


Background
Low-value and inappropriate medical care is recognized as a costly “wicked problem” in need of remedy [1]. In 2012, the Institute of Medicine (now the National Academy of Medicine) estimated that wasteful spending contributed to one-third of healthcare costs in the USA, and over $200 billion was attributed to unnecessary care [2, 3]. A 2018 report from the Organization for Economic Co-operation and Development (OECD) indicated that 20% of healthcare spending in the European Union was wasteful [4]. Another report stated that correcting for inappropriate or harmful practices accounts for over 10% of hospital spending in OECD member nations globally [5], indicating valuable resources are not being allocated efficiently.
Overuse or inappropriate use of screening, diagnostic services, and treatments contribute to patient harms including overdiagnosis and contraindicated treatments, unnecessary treatment and financial burden on patients, increased risk of adverse outcomes, and worsened care quality [6, 7]. A 2019 meta-analysis of studies published in three prominent medical journals found 396 reversals of medical practices [8], suggesting healthcare is rife with opportunities to eliminate ineffective or harmful practices. In public health, a classic example of an ineffective intervention is the D.A.R.E. program, which, despite evidence suggesting the program is ineffective and possibly counterproductive [9,10,11], is still offered in all US states and in more than 50 countries globally [12]. Another example is abstinence-only education models for sexual health, which despite evidence for the ineffectiveness and potential harms of these approaches, are still prevalent [13]. In Uganda, for example, evidence suggests abstinence only education was not effective in reducing the risk of sexually transmitted diseases, and numerous studies suggest detrimental impacts of such programs on sexual health [14,15,16]. Given there is far less funding in public health than in medicine [17], particularly in resource-limited settings, waste resulting from the continuation of ineffective programs is even more costly.
Low-value care also has implications for health equity. Helfrich and colleagues highlight several examples of racial and ethnic disparities in both overuse and underuse [18]. For instance, Black and Hispanic patients receive a higher rate of low value care than white patients for several services, such as inappropriate feeding tube use among dementia patients [19]. Furthermore, patients of color with low socioeconomic status subsidize low-value care among more affluent white patients [20]. When overprescribing or overuse occurs, this leaves fewer resources that can go to patients in need [21]. McKay and colleagues suggest it is unethical to leave harmful, ineffective, or unnecessary interventions in place when removal and/or replacement is warranted, and at the same time caution researchers to carefully consider the contextual factors surrounding these interventions and potential remedies as to not further disempower marginalized stakeholders [22].
These findings and others have helped bolster the importance of de-implementation research to develop approaches to promote the reduction of unnecessary interventions. De-implementation is defined as discontinuing or abandoning practices that are not proven to be effective, are less effective or less cost-effective than an alternative practice, or are potentially harmful [22, 23]. In public policy, “termination” is analogous to de-implementation, and refers to the “deliberate conclusion or cessation of specific government functions, programs, policies, or organizations,” [24] and unlike in implementation science, is agnostic about the weight and direction of evidence of effectiveness. This, along with other concepts from public policy, such as “disinvestment”, are particularly relevant to the study of de-implementation because they characterize in depth the context surrounding termination or disinvestment (e.g., landscape of risk to policymakers, constituent and political pressures, choices of strategy), policy characteristics that facilitate or hinder termination, and organizational termination processes [25,26,27]. Decades of research scattered across healthcare, public health, public policy, and business have been devoted to investigating efficient, effective means for removing unnecessary programs and phasing out policies that are no longer useful or relevant. However, the formal study of best practices in systematic cessation (i.e., de-implementation) remains a relatively new area of inquiry within the field of implementation science and has room for significant development [28].
Despite greater attention to the importance of reduction of overuse, there is a lack of guiding frameworks for this work to inform research, data collection, and analysis, and to generate scientific consensus [6]. Harris and colleagues conducted a literature review of disinvestment in health services; they did not find models for systematic organizational approaches to evidence-based decision making regarding disinvestment [29]. Although implementation science has an abundance of frameworks and models to guide the study of implementation, it is unclear if these are suitable guides for de-implementation research [30] given differences in processes involved and necessary behavior change strategies [28, 31]. A recent review of de-implementation studies published in 2013-2018 found ten theories, models, and frameworks to guide or explain de-implementation of low-value care [32]. Although this review provides helpful information for the field, it was limited in scope to five years of publications and was aimed mainly towards medical care. Decades of research on policy termination illustrate the potential to learn about de-implementation or discontinuance of practices from an array of disciplines, presenting an important opportunity to expand upon this work.
Given the importance of effective de-implementation to health outcomes and paucity of information about frameworks and models that can be applied to de-implementation, we conducted a scoping review to achieve the following aims: (1) To identify published frameworks and models that can be used to study de-implementation as a phenomenon; (2) To map each framework and model’s stated scope according to discipline, purpose, comprehensiveness, and measurement; and (3) To identify gaps in the literature to inform future model development and application for research. Our current review expands on previous efforts by including thirty years of publications from a broad array of relevant fields (e.g., healthcare, public policy, business), databases, and peer-reviewed journals. In the current review, frameworks are defined as “a set of variables and the relationships among them that are presumed to account for a set of phenomena.” [33] Models are conceptualized as more specific than frameworks and are “used to make specific assumptions about a limited set of parameters and variables” [33]. This review is explicitly focused on visual representations of frameworks and models (FM from here on) that may be used as a guide for researchers and practitioners in designing, executing, and evaluating de-implementation efforts.
Methods
Search strategy
We conducted a systematic search and scoping review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-ScR) guidelines for scoping reviews [34]. The authors reviewed canonical articles and consulted with a research librarian to develop search terms. A research librarian specializing in literature review assisted in searching published literature for the concepts of “de-implementation,” “models” and “frameworks,” and “use patterns.” Due to the broad nature of search terms used to capture these concepts, the search was optimized over multiple iterations. With each iteration, increased precision was achieved by utilizing controlled vocabulary terms, proximity searching, and keywords. In order to capture the maximum number of potentially relevant FM, nine databases were included in the search: Ovid Medline, Embase, Scopus, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Econlit, Global Health, APA PsycInfo, SocINDEX, and Cochrane. The search was limited to studies published in English from 1990 to June 2020 and did not include animal studies. The primary search resulted in 6,253 records. From this, incremental searches with journal limiters on the primary search and hand searching of eleven relevant journals for study protocols resulted in an additional 141 records (Supplemental File 1). Records were entered into EndNote reference management software for deduplication.
Inclusion and exclusion criteria
At the title and abstract screening phase, we applied broad inclusion criteria such that any article that used a de-implementation related term from our search strategy and mentioned a framework or model was included for full text review. Studies were excluded if they were not published in English, published prior to 1990, or did not include relevant terms in the title or abstract. We applied additional exclusion criteria at the full text screening phase, such that records were excluded if the full text record was irretrievable, the article did not include a visual representation of FM, the FM depicted were not relevant to de-implementation (e.g., indicated discontinuance of therapy upon patient recovery), or the search terms were used in a different context (e.g., “model” referred to a statistical model). We did not explicitly limit to strategies to support de-implementation (analogous to implementation strategies); we also included de-implementation processes, efforts, and projects broadly.
Screening procedures
Two raters (CWB and SG) conducted a pilot title and abstract screening with approximately five percent of records. A selected subset of records were brought to the full team for discussion and review to inform screening decisions. Once consensus was achieved, the two raters conducted independent title and abstract screenings. For cases where a clear decision could not be made, the raters deliberated with the full team to reach a decision.
Once the final set of records was identified for full text screening, the first author developed screening procedures based on team input. Two raters (CWB and ET) piloted the screening procedures with a randomly selected subset of 15 full text records. The study team refined the procedures and the two raters piloted a second set of randomly selected 15 full text records. Upon finalizing the screening procedures and reaching consensus, the two raters conducted dual independent screening of the remaining full text records. The raters met weekly for consensus. When consensus could not be reached, the raters consulted the full team for a final decision. By using a consensus coding approach, raters reached 100% agreement, thus an interrater reliability statistic was not calculated. The raters used a hierarchical exclusion approach such that the first applicable exclusion reason was applied (see Supplemental File 1 for exclusion codes). The team then conducted a subsequent hand-search of relevant references from articles included at the full text screening phase. This hand-searching approach primarily served to attempt to locate articles providing a visual representation of FM referenced in full text articles included in our review. We did not identify any additional articles that met the criteria to consider for full text review.
Data extraction
The first author developed a data extraction procedures manual incorporating team input. The constructs selected for extraction and coding were informed by previous reviews and conceptual articles in FM and de-implementation published by team members [22, 30, 35]. Two raters (CWB and ET) extracted descriptive information such as country and setting of study, topic area, and the subject of de-implementation (e.g., medical intervention, organizational practice, public policy). To capture how this topic is described in the literature, the raters extracted terms relevant to de-implementation. The raters then classified the de-implementation action targets of the FM based on the four categories presented by Norton and Chambers [35]: reduce, replace, restrict, remove. Reduce refers to the decrease in use (frequency, intensity) of an intervention. Replace indicates eliminating an inappropriate intervention and putting a new evidence-based program targeting the same or similar outcomes in its place. Restrict narrows by whom, where, and/or for whom an intervention is used. Remove occurs when an inappropriate intervention is eliminated from practice or a policy is terminated (without replacement).
We classified the evidence for de-implementation presented by included studies according to Norton and Chambers [35]. We coded a study as presenting supporting evidence that an intervention was ineffective if the authors cited studies demonstrating that the intervention does not improve patient outcomes or causes harm to patients. Contradicted evidence indicated that more recent or higher quality studies suggest that an intervention previously suggested to be beneficial may in fact be ineffective or harmful. Mixed evidence indicated that the quality and quantity of evidence available to support the effectiveness, or lack thereof, and/or harmfulness of an intervention is roughly equal. Untested suggested that the intervention has not yet been tested for effectiveness. If a study did not cite specific evidence for the de-implementation of a practice or policy, we coded this as not reported (NR).
To determine how de-implementation efforts are currently studied, we extracted information on study design, methodology, measurement, and outcomes of interest. FM characterization was informed by previous reviews on implementation models and frameworks [30, 32] and included model name, type of framework or model (i.e., determinants model, evaluation framework, process model, theoretical framework; see Supplemental File 2 for definitions), and the nature of relationships between constructs (i.e., linear; cyclical/feedback; nested). As in the previous review by Tabak and colleagues [30], we classified FM according to the socio-ecological framework (SEF) [36]. Recognizing that personal-level processes related to de-implementation can be within an individual (e.g., cognitive processes such as unlearning [37]) or involve interactions between individuals (e.g., shared decision-making between a patient and provider), we expanded our classification system to distinguish the individual level into “interpersonal” and “intrapersonal.” The coders’ approach to classifying the FM per the levels of the SEF relied on the authors’ descriptions of how the FM was applied in their study (for empirical articles) or the descriptions of FM development and application (for conceptual articles). Coders did not make inferences beyond what was available in the text or draw upon other background knowledge or text to assign levels of the SEF.
Two raters (CWB and ET) piloted the extraction procedures on two articles and met with the study team to revise. The final extraction procedures and extraction variables were entered into a Google Sheets extraction database. Two raters (CWB and ET) conducted dual non-independent data extraction such that a primary rater would highlight relevant text in the article and enter data into the database and the second rater would review for accuracy and completeness. The raters met weekly to generate consensus. As before, when consensus could not be achieved, the full team was consulted. Upon completing data extraction, the first author generated descriptive statistics (e.g., frequencies) and qualitative descriptions of the data, reviewed by the co-authors for accuracy. The protocol for this review is not registered with a review tracking database; however, a detailed protocol is available from the authors upon request.
Quality assessment
To assess the quality of the included empirical articles (n = 13), the first author applied the Mixed Methods Appraisal Tool (MMAT) [38], which allows for the assessment of a wide array of study designs. The MMAT includes two initial screening questions applicable to all study types to assess minimum quality for inclusion. Included studies are rated “yes”, “no”, or “can’t tell” on five questions specific to the type of study design (i.e., qualitative studies are rated on different criteria than quantitative designs). The MMAT authors do not recommend excluding studies based on poorer quality ratings or creating quality thresholds based quantitative ratings [38], thus we have not taken such an approach in our quality assessment. Due to the nature of the quality rating criteria, it was not possible to assess the quality of review studies and conceptual articles not involving data collection and analysis.
Results
Yield
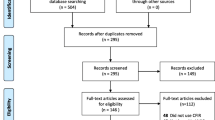
The final search yielded a total of 1860 unique records after deduplication. During the title and abstract screening phase, 1734 records were excluded, leaving 126 records for full text screening. During full text screening, 99 records were excluded, most frequently due to no visual depiction of a model or framework referenced in the text (n = 52). A total of 27 full text records were included for final data extraction (see PRIMSA-ScR Figure 1).

PRISMA flow diagram
Study characteristics
The 27 published articles extracted in the final search and included in this review were nearly-even split between empirical (n = 13; see Table 1) and non-empirical studies (n = 14; see Table 2). Mixed methods study designs (n = 11) were most common among empirical studies. Only two quantitative studies were included: one of which utilized a cross-sectional longitudinal design [49], the other of which was a randomized controlled trial [50]. No qualitative empirical studies were included in this review. Of the non-empirical studies, 11 were commentaries or conceptual pieces; two were review studies. Twenty of the 27 included studies reported where the study took place. All were based in OECD countries, including: the USA (n = 9), Australia (n = 4), and multiple countries within the OECD (n = 3). The majority of studies that met the final criteria for inclusion were from the healthcare or public health sector (n = 22). Three were from organizations across multiple sectors and two were from public policy broadly. The median number of MMAT criteria met by included empirical studies was 4 (out of 5). More detailed reporting of study quality is available in Supplemental File 3.
We identified primary action targets as the focal de-implementation outcome of the FM identified in the included studies. “Remove” was the most common stand-alone action target, occurring in 13 studies (e.g., “deprescribing” of inappropriate medications in older adults [59]). Seven studies sought to “reduce” a practice as a standalone primary action target (e.g., “reducing” unnecessary preoperative testing for low-risk surgical procedures [41]). Six studies had multiple primary action targets, indicating that FM have the power to inform several paths to a de-implementation outcome depending upon the context (e.g., “reduce” dosage or fully “remove” growth hormone therapy in pediatric patients [39]). Eight FM depicted supporting or intermediary steps to reach the primary action target; these were classified as secondary action targets. For example, in a study examining androgen deprivation therapy, restriction (i.e., pre-authorization order templates) was a secondary action to support reduction of this intervention [48].
Fifteen studies provided explicit evidence for the need for de-implementation. Evidence of ineffectiveness was most common (n = 12). Five of these 12 studies also cited evidence that previous support for an intervention was contradicted (e.g., Scott and colleagues’ study of de-implementation of polypharmacy interventions for older adults [59]). Because many of the FM included in our review were about de-implementation practices broadly, rather than targeting a specific intervention or policy, we also examined the extent to which authors cited costs or stakeholder input as justification for de-implementation. All but four studies cited specifically cost as a justification for de-implementation. Twenty studies included stakeholder input as part of their rationale for de-implementation; stakeholder input was collected from primary data collection (i.e., surveys, interviews) or cited from other studies (see Tables 1 and 2).
Model characteristics
In our final analysis, 27 unique FM were found across the 27 included articles. With one exception, the collection of articles from the Harris et al., “SHARE” study [29, 43,44,45], there was no repetition of models across studies. Process models were the most frequently occurring (n = 11), while determinants models were second most common (n = 8). Theoretical frameworks (n = 5) and evaluation frameworks (n = 3) were presented less frequently. Most FM depicted linear relationships between constructs (n = 18), suggesting that many authors conceptualized de-implementation activities or processes as a series of steps more often than relationships characterized by feedback or circular processes. Five FM did not depict a relationship between constructs, which may limit their utility in informing de-implementation intervention design or measurement.
Across the 27 studies, 13 unique terms were used to describe the phenomenon of interest. “Discontinuation” and “De-implementation” (and variants of these terms) were used most frequently, appearing across 15 and 13 studies, respectively. Terms that appeared less frequently, such as “deregulate” and “retrenchment” were found exclusively in the public policy literature and did not cross over into other disciplines, whereas other terms from the policy literature, such as “termination” and “disinvestment” were found across disciplines, including within healthcare and public health.
Twenty-one FM encompassed multiple levels of the SEF, indicating de-implementation was conceptualized as a complex and multi-faceted process, while only six operated at a single level. FM most frequently operated at the organization level (n = 18). Sixteen included the system level. The intrapersonal and interpersonal levels were represented in 15 and 14 models, respectively. Two of the models that operated at a single level did so at the organization level, while two operated solely at the system level (Table 3).
Discussion
The study of de-implementation is a relatively new area of inquiry within the established and growing field of implementation science [61]. Although a great deal of work in implementation science has been done to gather and classify FM, relatively little is known about the kind of FM that can be applied to study of de-implementation across various settings and topics. This review identified 27 unique FM with visual representations available from a wide range of disciplines, including public health, healthcare, and public policy.
Every study included in this review reported using a unique FM to inform their conceptualization or empirical investigation of de-implementation, suggesting there is considerable variability in topics subject to de-implementation efforts, and potentially in approaches to studying de-implementation. Although we did not see repetition of FM in the records included in this review (with the exception of FM across four articles published from a single study) there were several commonalities across many FM. In particular, we saw that most FM (n = 21) operated at two or more levels of the SEF reflecting that de-implementation is often a complex, multilevel process. Four of the six FM that operated at only one level did so at the organization or system level. This could potentially obscure the intrapersonal and interpersonal dynamics that feed into higher-level processes. In addition, we found two-thirds of the FM depicted linear relationships between constructs, while more complex relationships (e.g., feedback loops) were depicted less frequently. This simplified illustration of relationships between constructs or processes involved in de-implementation may dampen the extent to which real-world complexity is conceptualized and considered. Indeed, a review of low-value health services found that multicomponent interventions involving patients and providers were most effective in reducing low-value care [62], suggesting that the study of de-implementation warrants multilevel FM that depict these various components of a de-implementation effort.
As previously stated, apart from a collection of articles stemming from a single study [29, 43,44,45], we did not see FM repeat across studies included in our review, which may be due in part to the variety of settings and interventions included. The lack of congruence in conceptualization of de-implementation determinants and processes may make it difficult to compare findings across studies. The use of existing FM would allow for comparisons across studies, testing and confirmation of proposed relationships between variables related to de-implementation efforts, and offers opportunities for refinement and improved conceptual clarity within the study of de-implementation processes [63, 64]. As research focusing on de-implementation advances, we suggest that researchers begin with models reviewed here, with necessary adaptations, to help promote congruence and convergence within the field.
Only three of the FM included in our review were also included in a recently published review of de-implementation for low-value care [32]. Ultimately, we included 27 unique articles, compared to 10 included by Nilsen and colleagues. Despite differences in our review approach highlighted earlier, we note several similar findings. In both reviews, authors often did not specify the setting of interest; just over half of studies specified to what kind of clinical (or non-clinical) setting their FM applied. On the surface, broad descriptions of the settings may seem to suggest that the included FM can be applied to a wide array of contexts. However, we are limited in determining the extent to which FM developed in one setting or for a particular topic can be successfully applied to another substantive area (for example, would FM developed in the context of reducing medication overprescribing be suitable for discontinuation of a psychosocial intervention, or would FM developed for use in hospitals also be applicable in community settings). Across both reviews, samples were roughly evenly split between conceptual and empirical studies. This could suggest that, despite dating back as much as two decades, many proposed FM have yet to be empirically applied. This illustrates the need for additional testing and refinement of existing de-implementation FM.
Reducing low-value care can help improve health equity [18]. Cost savings from improved health care delivery can be used for addressing needs related to social determinants of health, expanding healthcare benefits to uninsured patients, and bolstering safety net care [21]. There is opportunity to more intentionally build an equity lens into de-implementation FM. Indeed, the revision and expansion of well-established implementation FM (e.g., RE-AIM, iPARIHS) to include health equity is already underway [65, 66]. Similar approaches can be emulated with de-implementation FM. There is also opportunity to harness de-implementation to improve health equity; however, caution is needed in ensuring that de-implementation efforts do not unintentionally perpetuate or exacerbate existing inequities [22]. For example, in the context of de-implementing outdated cancer screening guidelines, Shelton and colleagues note several important findings related to de-implementation and impacted stakeholders, including mistrust of healthcare systems among patients and misalignment of changing guidelines with the preferences and needs of African American women [67]. Finally, all studies for which the location of the work was reported (20 of 27 studies) were conducted in OECD counties. It is unclear the extent to which models developed in OECD contexts are applicable to low- and middle- income countries, or what lessons from de-implementation in these countries can be applied to resource-limited settings in high-income countries. More work is needed in conceptualizing and examining de-implementation in resource-limited locations.
Implementation science is an interdisciplinary field [68, 69], yet its use of FM has not taken advantage of the theoretical depth that exists in its associated disciplines. Implementation researchers have argued both for better integration of knowledge from other disciplines, including public administration and economics [70, 71], and improving implementation science’s use and development of theory [68]. Many analyses highlight the ability of public policy to better address the complexity of implementation, clarify the role of the outer context, conceptualize a broader range of policy outcomes, contribute to development of strategies at the systems level, and measure policy implementation determinants and outcomes [72,73,74]. Similar integration could serve as a way to advance the study of de-implementation by taking advantage of the comparatively large policy termination literature. Classic theories of policy feedback and incrementalism [75, 76] have proven particularly useful to de-implementation research in that they detail how the political landscapes change after a policy is adopted and sustained for some time, leading to distinct risks and barriers of termination of these policies than at adoption.
Although interest in de-implementation is growing, opportunities to advance this area of inquiry remain few [77]. Through 2016, only 20 federally-funded grants from the National Institutes of Health and the Agency for Healthcare Research and Quality focused explicitly on de-implementation [78]. Moullin and colleagues suggest several purposes and benefits of using FM to inform research and practice, including: defining the issue of interest and developing research or evaluation questions, selecting appropriate research or evaluation methods, discerning relevant determinants to de-implementation, selecting and tailoring strategies to support de-implementation, and to specify key outcomes to target [63]. Implementation science is a field that draws upon diverse disciplines, and there are numerous examples of FM that have been developed by scholars from a variety of fields (e.g., Theoretical Domains Framework developed by implementation scientists and behavioral researchers [79]). However, future work is still needed to determine the extent to which FM from other fields (e.g., cognitive psychology, organizational behavior) can be applied to de-implementation of healthcare interventions and public health policies and programs, as well as the transferability of FM from one content area to another (e.g., diabetes to cancer or prevention to treatment). Furthermore, additional investigation is needed to determine the extent to which FM for implementation are applicable to de-implementation. There may be opportunities to learn from previous implementation FM development work and to adapt implementation models for de-implementation. The field would benefit from a publicly available repository of de-implementation FM and associated literature, such as the resource available here: https://dissemination-implementation.org/.
We offer potential approaches for researchers and practitioners to use the information provided in this review. Readers seeking to use an existing FM to guide de-implementation work may wish to define their action target based on the categories used in this review (reduce, replace, restrict, remove) and select models that were applied to the same type of action. Readers may also wish to identify the level(s) of the SEF at which their intervention or approach to de-implementation operates and select from frameworks that operate at these level(s). Finally, as this review identifies over a dozen FM proposed in conceptual papers but (to our knowledge) have not been applied to empirical studies of de-implementation, readers may wish to test and refine FM identified in this review. The purpose of this review is to offer a broad understanding of existing FM to guide the study and practice of de-implementation; scholars can build upon this work to further specify and analyze de-implementation FM.
Limitations
While effective in some ways, the approach used in this review carries some limitations. Because visual representation of a FM (e.g., figure, table) was a requirement for inclusion, empirical studies that cited use of a FM but did not depict it, or for which we could not find a visual depiction in any of the literature referenced, were excluded. This approach was taken to minimize ambiguity of relationships between constructs and to include potentially helpful resources that can be used in future de-implementation studies. It is worth noting that many of the FM that did not have a visual depiction were prominent implementation frameworks that were not developed explicitly for the study or practice of de-implementation, thus would have been excluded from this review even with a visual representation. Further investigation is needed to determine the characteristics of other FM in existence that have been developed for the purpose of de-implementation yet do not yet have a visual representation available in the literature. These may offer additional opportunities to build upon existing work to develop, test, and refine de-implementation FM.
Although we conducted an extensive search incorporating seven databases and 11 peer-reviewed journals, our search did not yield a high number of records related to public policy de-implementation. It is possible that our search strategy was not inclusive of databases that include more policy-focused articles, or that relevant policy frameworks appear in books and other texts rather than peer-reviewed journals. Additionally, our single rater approach at the title and abstract screening phase may have resulted in relevant records being excluded. However, we limited our exclusion criteria at this phase and erred on the side of including records for full text screening if additional information was needed to determine article relevance. Finally, it was beyond the scope of this current review to conduct systematic coding and content analysis of the individual constructs in each of the FM. A future systematic review would be valuable in serving this purpose, and would allow for additional analyses, such as synthesis of the common issues identified across FM. It will also be useful to add de-implementation FM to webtools for finding, adapting, and using FM in implementation science [80].
Conclusions
This current review highlights the growing interest in the study of de-implementation and provides a broad overview of FM that can be applied to this area of inquiry. As we continue to build the de-implementation knowledge base, the field of implementation science, as well as implementation practitioners, would benefit from the greater specification of how FM are applied to de-implementation challenges. The use of identified de-implementation FM would enable researchers to make comparisons across studies and contribute to a knowledge base regarding key constructs related to de-implementation and the relationships between these.
Availability of data and materials
PDFs of articles included for data extraction and raw extraction data tables can be provided by the authors upon reasonable request.
Abbreviations
- FM:
-
Frameworks and models
- SEF:
-
Socioecological framework
- NR:
-
Not reported
References
Lyu H, Xu T, Brotman D, Mayer-Blackwell B, Cooper M, Daniel M, et al. Overtreatment in the United States. PLoS One. 2017;12(9):e0181970. https://doi.org/10.1371/journal.pone.0181970.
Smith M, Saunders R, Stuckhardt L, McGinnis J. Committee on the Learning Health Care System in America; Institute of Medicine. Best care at lower cost: the path to continuously learning health care in America. Washington, DC: National Academies Press; 2013.
Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA. 2012;307(14):1513–6. https://doi.org/10.1001/jama.2012.362.
OECD, European Union. Health at a glance: Europe 2018. 2018. https://doi.org/10.1787/health_glance_eur-2018-en.
OECD. Tackling wasteful spending on health. 2017. https://doi.org/10.1787/9789264266414-en.
Morgan DJ, Brownlee S, Leppin AL, Kressin N, Dhruva SS, Levin L, et al. Setting a research agenda for medical overuse. BMJ. 2015;351:h4534. https://doi.org/10.1136/bmj.h4534.
Hicks LK. Reframing overuse in health care: time to focus on the harms. J Oncol Pract. 2015;11(3):168–70. https://doi.org/10.1200/jop.2015.004283.
Herrera-Perez D, Haslam A, Crain T, Gill J, Livingston C, Kaestner V, et al. A comprehensive review of randomized clinical trials in three medical journals reveals 396 medical reversals. eLife. 2019;8:e45183. https://doi.org/10.7554/eLife.45183.
Vincus AA, Ringwalt C, Harris MS, Shamblen SR. A short-term, quasi-experimental evaluation of D.A.R.E.'s revised elementary school curriculum. J Drug Educ. 2010;40(1):37–49. https://doi.org/10.2190/DE.40.1.c.
Caputi TL, Thomas MLA. Truth and D.A.R.E.: Is D.A.R.E.’s new Keepin’ it REAL curriculum suitable for American nationwide implementation? Drugs. 2017;24(1):49–57. https://doi.org/10.1080/09687637.2016.1208731.
Hanson DJ. Drug Abuse Resistance Education (D.A.R.E.). The Encyclopedia of Clinical Psychology. Hoboken: Wiley; 2014. p. 1–3.
D.A.R.E. D.A.R.E. Hometowns – U.S.A. & International. https://dare.org/where-is-d-a-r-e/. 2021. Accessed 18 June 2021.
Ott MA, Santelli JS. Abstinence and abstinence-only education. Curr Opin Obstet Gynecol. 2007;19(5):446–52. https://doi.org/10.1097/GCO.0b013e3282efdc0b.
Lo NC, Lowe A. E. B. Abstinence Funding was not associated with reductions in HIV risk behavior in Sub-Saharan Africa. Health Aff. 2016;35(5):856–63. https://doi.org/10.1377/hlthaff.2015.0828.
Ankunda R, Atuyambe LM, Kiwanuka N. Sexual risk related behaviour among youth living with HIV in central Uganda: implications for HIV prevention. Pan Afr Med J. 2016;24(1):49. https://doi.org/10.11604/pamj.2016.24.49.6633.
Cohen J, Tate T. The less they know, the better: abstinence-only HIV/AIDS programs in Uganda. Reprod Health Matters. 2006;14(28):174–8. https://doi.org/10.1016/S0968-8080(06)28249-1.
Himmelstein DU, Woolhandler S. Public healthʼs falling share of US health spending. Am J Public Health. 2016;106(1):56–7. https://doi.org/10.2105/AJPH.2015.302908.
Helfrich CD, Hartmann CW, Parikh TJ, Au DH. Promoting health equity through de-implementation research. Ethn Dis. 2019;29(Suppl 1):93–6. https://doi.org/10.18865/ed.29.S1.93.
Schpero WL, Morden NE, Sequist TD, Rosenthal MB, Gottlieb DJ, Colla CH. For selected services, Blacks and Hispanics more likely to receive low-value care than whites. Health Aff. 2017;36(6):1065–9. https://doi.org/10.1377/hlthaff.2016.1416.
Xu WY, Jung JK. Socioeconomic differences in use of low-value cancer screenings and distributional effects in Medicare. Health Serv Res. 2017;52(5):1772–93. https://doi.org/10.1111/1475-6773.12559.
Beaudin-Seiler B, Ciarametaro M, Dubois RW, Lee J, FA M. Reducing low-value care. Health Equity: Health Affairs Blog; 2016.
McKay VR, Morshed AB, Brownson RC, Proctor EK, Prusaczyk B. Letting go: Conceptualizing intervention de-implementation in public health and social service settings. Am J Community Psychol. 2018;62(1-2):189–202. https://doi.org/10.1002/ajcp.12258.
Prasad V, Ioannidis JPA. Evidence-based de-implementation for contradicted, unproven, and aspiring healthcare practices. Implement Sci. 2014;9(1). https://doi.org/10.1186/1748-5908-9-1.
deLeon P. Public policy termination: an end and a beginning. Foreign Policy Anal. 1978;4(3):369–92.
Pierson P. The new politics of the welfare state. World Polit. 1996;48(2):143–79. https://doi.org/10.1353/wp.1996.0004.
Kirkpatrick SE, Lester JP, Peterson MR. The policy termination process: a conceptual framework and application to revenue sharing. Rev Policy Res. 1999;16(1):209–38. https://doi.org/10.1111/j.1541-1338.1999.tb00847.x.
Adam C, Bauer MW, Knill C, Studinger P. The termination of public organizations: theoretical perspectives to revitalize a promising research area. Public Organ Rev. 2007;7(3):221–36. https://doi.org/10.1007/s11115-007-0033-4.
Patey AM, Grimshaw JM, Francis JJ. Changing behaviour, ‘more or less’: do implementation and de-implementation interventions include different behaviour change techniques? Implement Sci. 2021;16(1):20. https://doi.org/10.1186/s13012-021-01089-0.
Harris C, Allen K, King R, Ramsey W, Kelly C, Thiagarajan M. Sustainability in Health care by Allocating Resources Effectively (SHARE) 2: identifying opportunities for disinvestment in a local healthcare setting. BMC Health Serv Res. 2017;17(1). https://doi.org/10.1186/s12913-017-2211-6.
Tabak RG, Khoong EC, Chambers DA, Brownson RC. Bridging research and practice: models for dissemination and implementation research. Am J Prev Med. 2012;43(3):337–50. https://doi.org/10.1016/j.amepre.2012.05.024.
van Bodegom-Vos L, Davidoff F. Marang-van de Mheen PJ. Implementation and de-implementation: two sides of the same coin? BMJ Qual Saf. 2017;26(6):495–501. https://doi.org/10.1136/bmjqs-2016-005473.
Nilsen P, Ingvarsson S, Hasson H, von Thiele SU, Augustsson H. Theories, models, and frameworks for de-implementation of low-value care: a scoping review of the literature. Implement Res Pract. 2020;1:2633489520953762. https://doi.org/10.1177/2633489520953762.
Carpiano RM, Daley DM. A guide and glossary on postpositivist theory building for population health. J Epidemiol Community Health. 2006;60(7):564–70. https://doi.org/10.1136/jech.2004.031534.
Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73. https://doi.org/10.7326/m18-0850.
Norton WE, Chambers DA. Unpacking the complexities of de-implementing inappropriate health interventions. Implement Sci. 2020;15(1). https://doi.org/10.1186/s13012-019-0960-9.
McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351–77. https://doi.org/10.1177/109019818801500401.
Helfrich CD, Rose AJ, Hartmann CW, van Bodegom-Vos L, Graham ID, Wood SJ, et al. How the dual process model of human cognition can inform efforts to de-implement ineffective and harmful clinical practices: a preliminary model of unlearning and substitution. J Eval Clin Pract. 2018;24(1):198–205. https://doi.org/10.1111/jep.12855.
Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inform. 2018;34:285–91. https://doi.org/10.3233/EFI-180221.
Cuttler L, Silvers JB, Singh J, Tsai AC, Radcliffe D. Physician decisions to discontinue long-term medications using a two-stage framework: the case of growth hormone therapy. Med Care. 2005;43(12):1185–93. https://doi.org/10.1097/01.mlr.0000185731.71972.d4.
Goodwin E, Frew EJ. Using programme budgeting and marginal analysis (PBMA) to set priorities: Reflections from a qualitative assessment in an English primary care trust. Soc Sci Med. 2013;98:162–8. https://doi.org/10.1016/j.socscimed.2013.09.020.
Grimshaw JM, Patey AM, Kirkham KR, Hall A, Dowling SK, Rodondi N, et al. De-implementing wisely: developing the evidence base to reduce low-value care. BMJ Qual Saf. 2020;29(5):409–17. https://doi.org/10.1136/bmjqs-2019-010060.
Gupta A, Brown TJ, Singh S, Sen A, Agrawal D, Li HC, et al. Applying the ‘COST’ (Culture, Oversight, Systems Change, and Training) framework to de-adopt the neutropenic diet. Am J Med. 2019;132(1):42–7. https://doi.org/10.1016/j.amjmed.2018.08.009.
Harris C, Allen K, Brooke V, Dyer T, Waller C, King R, et al. Sustainability in Health care by Allocating Resources Effectively (SHARE) 6: investigating methods to identify, prioritise, implement and evaluate disinvestment projects in a local healthcare setting. BMC Health Serv Res. 2017;17(1). https://doi.org/10.1186/s12913-017-2269-1.
Harris C, Green S, Elshaug AG. Sustainability in Health care by Allocating Resources Effectively (SHARE) 10: operationalising disinvestment in a conceptual framework for resource allocation. BMC Health Serv Res. 2017;17(1). https://doi.org/10.1186/s12913-017-2506-7.
Harris C, Allen K, Ramsey W, King R, Green S. Sustainability in Health care by Allocating Resources Effectively (SHARE) 11: reporting outcomes of an evidence-driven approach to disinvestment in a local healthcare setting Milena Pavlova. BMC Health Serv Res. 2018;18(1). https://doi.org/10.1186/s12913-018-3172-0.
McKay VR, Margaret Dolcini M, Hoffer LD. The dynamics of de-adoption: a case study of policy change, de-adoption, and replacement of an evidence-based HIV intervention. Transl Behav Med. 2017;7(4):821–31. https://doi.org/10.1007/s13142-017-0493-1.
Padek M, Allen P, Erwin PC, Franco M, Hammond RA, Heuberger B, et al. Toward optimal implementation of cancer prevention and control programs in public health: a study protocol on mis-implementation. Implement Sci. 2018;13(1). https://doi.org/10.1186/s13012-018-0742-9.
Skolarus TA, Hawley ST, Wittmann DA, Forman J, Metreger T, Sparks JB, et al. De-implementation of low value castration for men with prostate cancer: protocol for a theory-based, mixed methods approach to minimizing low value androgen deprivation therapy (DeADT). Implement Sci. 2018;13(1). https://doi.org/10.1186/s13012-018-0833-7.
Tangpong C, Abebe M, Li Z. A temporal approach to retrenchment and successful turnaround in declining firms. J Manag Stud. 2015;52(5):647–77. https://doi.org/10.1111/joms.12131.
Voorn VMA, van Bodegom-Vos L, So-Osman C. Towards a systematic approach for (de)implementation of patient blood management strategies. Transfus Med. 2018;28(2):158–67. https://doi.org/10.1111/tme.12520.
Amankwah-Amoah J. Integrated vs. add-on: a multidimensional conceptualisation of technology obsolescence. Technol Forecast Soc Change. 2017;116:299–307. https://doi.org/10.1016/j.techfore.2016.10.006.
Bain KT, Holmes HM, Beers MH, Maio V, Handler SM, Pauker SG. Discontinuing medications: a novel approach for revising the prescribing stage of the medication-use process. J Am Geriatr Soc. 2008;56(10):1946–52. https://doi.org/10.1111/j.1532-5415.2008.01916.x.
Bauer MW, Knill C. A conceptual framework for the comparative analysis of policy change: measurement, explanation and strategies of policy dismantling. J Comp Policy Anal Res Pract. 2014;16(1):28–44. https://doi.org/10.1080/13876988.2014.885186.
Davidson KW, Ye S, Mensah GA. Commentary: De-implementation science: a virtuous cycle of ceasing and desisting low-value care before implementing new high value care. Ethn Dis. 2017;27(4):463–8. https://doi.org/10.18865/ed.27.4.463.
Herald T, Verma D, Lubert C, Cloutier R. An obsolescence management framework for system baseline evolution-perspectives through the system life cycle. Syst Eng. 2009;12(1):1–20. https://doi.org/10.1002/sys.20106.
Hyun-Ju S, Ji Jeong P, Seon HL. A systematic review on current status of health technology reassessment: insights for South Korea. Health Res Policy Syst. 2016;14. https://doi.org/10.1186/s12961-016-0152-x.
Niven DJ, Mrklas KJ, Holodinsky JK, Straus SE, Hemmelgarn BR, Jeffs LP, et al. Towards understanding the de-adoption of low-value clinical practices: a scoping review. BMC Med. 2015;13(1). https://doi.org/10.1186/s12916-015-0488-z.
Norton WE, Chambers DA, Kramer BS. Conceptualizing de-implementation in cancer care delivery. J Clin Oncol. 2019;37(2):93–6. https://doi.org/10.1200/JCO.18.00589.
Scott IA, Gray LC, Martin JH, Pillans PI, Mitchell CA. Deciding when to stop: towards evidence-based deprescribing of drugs in older populations. Evid-Based Med. 2013;18(4):121–4. https://doi.org/10.1136/eb-2012-100930.
Soril LJ, MacKean G, Noseworthy TW, Leggett LE, Clement FM. Achieving optimal technology use: a proposed model for health technology reassessment. SAGE Open Med. 2017;5:2050312117704861.
Brownson RC, Colditz GA, Proctor EK. Dissemination and implementation research in health: translating science to practice. New York: Oxford University Press; 2017.
Colla CH, Mainor AJ, Hargreaves C, Sequist T, Morden N. Interventions aimed at reducing use of low-value health services: a systematic review. Med Care Res Rev. 2017;74(5):507–50. https://doi.org/10.1177/1077558716656970.
Moullin JC, Dickson KS, Stadnick NA, Albers B, Nilsen P, Broder-Fingert S, et al. Ten recommendations for using implementation frameworks in research and practice. Implement Sci Commun. 2020;1:42. https://doi.org/10.1186/s43058-020-00023-7.
Damschroder LJ. Clarity out of chaos: Use of theory in implementation research. Psychiatry Res. 2020;283:112461. https://doi.org/10.1016/j.psychres.2019.06.036.
Shelton RC, Chambers DA, Glasgow RE. An extension of RE-AIM to enhance sustainability: addressing dynamic context and promoting health equity over time. Front Public Health. 2020;8:134.
Woodward EN, Matthieu MM, Uchendu US, Rogal S, Kirchner JE. The health equity implementation framework: proposal and preliminary study of hepatitis C virus treatment. Implement Sci. 2019;14(1):26. https://doi.org/10.1186/s13012-019-0861-y.
Shelton RC, Brotzman LE, Johnson D, Erwin D. Trust and mistrust in shaping adaptation and de-implementation in the context of changing screening guidelines. Ethn Dis. 2021;31(1):119–32. https://doi.org/10.18865/ed.31.1.119.
Kislov R, Pope C, Martin GP, Wilson PM. Harnessing the power of theorising in implementation science. Implement Sci. 2019;14(1):103. https://doi.org/10.1186/s13012-019-0957-4.
Proctor EK, Landsverk J, Aarons G, Chambers D, Glisson C, Mittman B. Implementation research in mental health services: an emerging science with conceptual, methodological, and training challenges. Admin Pol Ment Health. 2009;36(1):24–34. https://doi.org/10.1007/s10488-008-0197-4.
Eisman AB, Kilbourne AM, Dopp AR, Saldana L, Eisenberg D. Economic evaluation in implementation science: making the business case for implementation strategies. Psychiatry Res. 2020;283:112433. https://doi.org/10.1016/j.psychres.2019.06.008.
Johansson S. Implementing evidence-based practices and programmes in the human services: lessons from research in public administration. Eur J Soc Work. 2010;13(1):109–25. https://doi.org/10.1080/13691450903135691.
Nilsen P, Ståhl C, Roback K, Cairney P. Never the twain shall meet? - a comparison of implementation science and policy implementation research. Implement Sci. 2013;8(1):63. https://doi.org/10.1186/1748-5908-8-63.
Bullock HL, Lavis JN, Wilson MG, Mulvale G, Miatello A. Understanding the implementation of evidence-informed policies and practices from a policy perspective: a critical interpretive synthesis. Implement Sci. 2021;16(1):18. https://doi.org/10.1186/s13012-021-01082-7.
Allen P, Pilar M, Walsh-Bailey C, Hooley C, Mazzucca S, Lewis CC, et al. Quantitative measures of health policy implementation determinants and outcomes: a systematic review. Implement Sci. 2020;15(1):47. https://doi.org/10.1186/s13012-020-01007-w.
Hayes M. Incrementalism. In: Araral E, Fritzen S, Howlett M, Ramesh M, Wu X, editors. Routledge Handbook of public policy. New York: Routledge; 2013.
Marier P. Policy feedback and learning. In: Araral E, Fritzen S, Howlett M, Ramesh M, Wu X, editors. Routledge handbook of public policy. New York: Routledge; 2013.
Korenstein D, Falk R, Howell EA, Bishop T, Keyhani S. Overuse of health care services in the United States: an understudied problem. Arch Intern Med. 2012;172(2):171–8. https://doi.org/10.1001/archinternmed.2011.772.
Norton WE, Kennedy AE, Chambers DA. Studying de-implementation in health: an analysis of funded research grants. Implement Sci. 2017;12(1):144. https://doi.org/10.1186/s13012-017-0655-z.
Atkins L, Francis J, Islam R, O’Connor D, Patey A, Ivers N, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. https://doi.org/10.1186/s13012-017-0605-9.
Rabin B, Glasgow RE, Ford B, Huebschmann A, Marsh R, Tabak RG et al. Dissemination & Implementation Models in Health Research & Practice. n.d.. https://dissemination-implementation.org/. Accessed 5 Oct 2021.
Acknowledgements
Our team thanks Brittany Sandler for her invaluable help in developing the search strategy and assistance organizing the records for screening.
Funding
This work was supported in part by the National Cancer Institute (number P50CA244431 and T32CA190194), the National Institute of Diabetes and Digestive and Kidney Diseases (numbers P30DK092950 and R25DK123008), the Centers for Disease Control and Prevention (number U48DP006395), and the Foundation for Barnes-Jewish Hospital.
Author information
Authors and Affiliations
Contributions
Study conceptualization: RCB, CWB, SG. Search strings and terms: SG with review from RCB, RT, AM, VM, WN. Eligibility criteria: all authors. Abstract screening: CWB, SG. Full text screening: CWB, ET. Data extraction: CWB, ET. Data aggregation: CWB; Writing: all authors. Editing: all authors. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
WN is on the Editorial Board of the journal Implementation Science. The remaining authors declare they have no conflicting interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Study identification and screening.
Additional file 2.
De-Implementation Review Data Extraction.
Additional file 3:
Quality assessment of empirical studies (N=13).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Walsh-Bailey, C., Tsai, E., Tabak, R.G. et al. A scoping review of de-implementation frameworks and models. Implementation Sci 16, 100 (2021). https://doi.org/10.1186/s13012-021-01173-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13012-021-01173-5