
Abstract
Background
This paper presents a comparative inventory of medicinal plant taxa and their uses by smallholder farming communities of four cultures in the Aswa River catchment of northern Uganda, situated in the eastern Sudanian savanna parkland ecotype of sub-Saharan Africa. The purpose of the study was to document the ethnobotanical use of medicinal plants by the Lango, Acholi, Teso (Atesot) and Ethur (jo Abwor), in an historical moment before civil conflict and mass displacement of the respondent communities disrupted the inter-generational transmission of traditional technical knowledge within the study area.
Methods
Following community consultations in four districts of northern Uganda during 1999–2000, interviews were conducted with holders of specialist knowledge on plants used as medicine on basis of a plant specimen allocated a voucher number and identified by the national herbarium. Use reports reflecting specific medicinal applications were compiled in aggregate to obtain a Relative Importance Index ranking. The commonality of medicinal taxa cited between each cultural interface was assessed by the Jaccard Index of Similarity, and the similarity of specific medicinal usage by taxon using Rahman’s Similarity Index.
Results
The data collected from 112 respondents comprise 280 medicinal use reports describing 263 applications for 62 medical conditions, citing 108 taxa from 44 botanical families of which Fabaceae comprised 20% of all use reports. No earlier mention could be found to corroborate 72 use reports (27% of the total), representing medicinal indications as yet undocumented, and potentially worthy of investigation. The RI values ranged between 15 and 94%, with 13 taxa having RI values above 50%. The JI ratios indicate the highest degree of similarity in the plant taxa used as medicine (21%) between the Lango and Teso cultures who share a common origin; however, Rahman’s Similarity Index indicates the highest similarity of specific medicinal usage by taxon between the Lango and Acholi, who share a common language group through cultural assimilation over time.
Conclusions
As a comparative study, the results imply that cultural exchange and assimilation may be a greater driver of inter-cultural similarity of ethnopharmacological use of a given taxon, as compared to shared historical origins.
Similar content being viewed by others


Background
Sustained by plant foods from our earliest origins, human use of plant medicines predates our earliest ancestry—and indeed our species—as a deep evolutionary behavior [1]. The plant kingdom has long provided panacea for human discomforts and diseases, as evidenced by archeological traces extending back as far as 1.2 million years ago [1]—and, much later, in the earliest of written records [2]. Of an estimated 390,900 plant species of record, over 28,000 have a recorded medicinal use [3]. Plant-derived molecules provide the basis for development of modern synthetic pharmaceuticals, and medicines derived directly from plants still constitute a quarter of the modern pharmacopeia [4].
Plant-based medicines are highly valued globally—more particularly for rural communities in sub-Saharan Africa, where conventional medical services are largely inaccessible and unaffordable—including rural northern Uganda. The World Health Organization (WHO) estimates that up to 80% of the global population relies on plant compounds in primary healthcare, while traditional medicines are becoming ever more popular as complementary therapies [5]. Based on a national-level survey, it has been estimated that 60% of Ugandans used traditional medicine, of which an estimated 90% was plant-based, noting that plant-based medicines are both more affordable than conventional therapies, and also more readily accessible—with a 1:700 ratio of traditional healers to population, versus a 1:25,000 ratio of medical doctors [6].
However, even as burgeoning global demand for medicinal plants in complementary treatments has come to threaten the survival of certain species [7], traditional knowledge of medicinal plant use is steadily receding from living memory, with inter-generational knowledge transfer declining further each year [8], in an accelerating process which has been termed cultural erosion [9].
In northern Uganda, this ongoing process was drastically accelerated by civil conflict in the early years of the current century, resulting in mass displacement of the civilian population into military camps just two years following data collection, resulting in severe disruption to traditional agriculture and transmission of indigenous knowledge on the use of plant biodiversity by rural communities [10]. The return of peace to the region (and the displaced to their homesteads) in 2007 brought other, demographic changes and socioeconomic challenges. Although Uganda is categorically an agricultural country, with 39% of households situated within the subsistence economy, its young and growing population—54% below 18 years—is online, aspirational and increasingly disinclined see their future in traditional agriculture [11]. In this socio-cultural context, the transmission of traditional knowledge can be considered as highly threatened.
Conceived as an inventory of taxa and their pharmacological use by culture, the operational hypothesis behind the study was that, given their similar geographies along a gradient of reduced rainfall from southwest to northeast, patterns of plant use within and between the four cultures surveyed would be similar, but also characteristically different—and that the relative degrees of relatedness of medicinal plant use between the four communities might be expected to reflect ethnic as well as cultural dimensions of their shared historical proximity.
The aim of the broader study, conducted under the auspices of an integrated conservation and development project aimed at documenting and reinforcing sustainable use of the tree and other woodland plant species, was to compile a full inventory of plant species traditionally utilized by rural communities, drawing upon the expertise and interest of key informants, and leveraging tacit knowledge from those motivated to share it in order to codify plant utilization and its management. This was achieved through a series of multi-dimensional (cultural, ethnographic, socioeconomic, ecological and botanical) studies of plant diversity, its use and management by smallholder farming households across the project area, of which this paper presents the results relevant to the use of medicinal plants.
Methods
The study area, landscapes and communities
The study area lies between 1° and 3° North and from 33° to 34° degrees East, comprising the southern catchment of the AswaFootnote 1 River, a major tributary of the Nile which rises from the Labwor Hills and other inselbergs punctuating wooded parkland on sandy loams over a lateritic ironstone layer [12]. At elevations ranging between 1025 and 1300 m, with unimodal rainfall between 750 and 1500 mm from April to October, and temperatures mostly ranging between 16° and 32°C [13], the study area corresponds to the Sudanian ecotype, which extends from eastern Senegal to the Gambella region of Ethiopia, and to Lake Kyoga at the geographic center of Uganda.
The plant biodiversity of Uganda as a whole, and of the study area in particular, has been documented historically—classified and mapped according to vegetation type at a scale of 1:500,000 [14], the central northern Uganda region characterized by a wooded savanna dominated by Vitellaria paradoxa C.F.Gaertn. subsp. nilotica (Kotschy) A.N.Henry, Chithra & N.C.Nair (formerly Butyrospermum paradoxum (C.F.Gaertn.) Hepper subsp. niloticum (Kotschy) Hepper) in association with other woody and herbaceous species (notably the savanna grass Hyparrhenia rufa Stapf.) The author participated in ground truthing of the 1:50,000 satellite data for revalidation of this floristic baseline in 1992–93 [15], which facilitated targeting of the study area for applied research on basis of its relative ecological integrity as reflected in the density of indigenous woodland.
The woodland species documented in the study area (and reflected in the use reports presented here) are found in similar association across this narrow band of Sudanian savanna [16], of which the shea butter tree Vitellaria paradoxa subsp. nilotica can be considered a cultural keystone species as defined by Garibaldi and Turner [17]. V. paradoxa is an indicator species of the parkland agroforestry system [18], characterized by the diversity of tree species conserved on farm when fallow woodland is cleared for cultivation [19], resulting a mosaic of cultivation embedded within a wooded landscape. According to the comprehensive review of earlier studies, the ethnopharmacology of the Sudanian ecotype and its resident cultures has been found to be distinctly under-represented in the ethnomedicinal literature as compared to the more humid forest biomes.
The respondent communities of the study area are distributed between the trading centers among rural hamlets, where households and communities remain profoundly connected to the plant biodiversity and its environmental services on which their livelihoods depend. As of 2014, the proportion of households engaged in subsistence farming as a main source of livelihood comprised 90.6% of the population of Otuke District [20], 91.1% of Agago [21], 85% of Amuria [22], and 86.7% of Abim [23]. Poverty is notably and pervasively higher in northern Uganda, literacy and access to sanitation notably lower than in other regions of the country [24].
The people of the study area—the Lango, Acholi, Teso (Atesot) and Ethur (jo Abwor)—are situated across four historical regions, comprising four distinct ethnicities, cultures and dialects across two major language groups. Each community recalls an early history of migration from a northern homeland to reside around an historic cultural boundary, or interface, represented by the massif of Mount Otuke—the remnant of an ancient granitic inselberg ridge, oriented northwest-southeast along the boundary between the present-day districts of Otuke and Abim (formerly Labwor, a name more reflective of its eponymous hills).
In its location and shared history, Mount Otuke represents a cultural frontier between the Lwo-origin Acholi and Ethur to the north, and the ‘Paranilotic’ Ateker-origin Teso and Lango to the south and east. Each of the four cultures recalls Mount Otuke as an ancestral hub or heartland around which they migrated in early times (a period known as aconya in the Lwo languages, asonya in Teso), particularly during the latter half of the 1700s [25]. At an elevation of 1400 m, the saddle-shaped ridgeline forms a natural boundary nearly 14 km long by two or three wide, extending to the southwest from the headwaters of the Aswa at the foot of the Labwor Hills [14]. The topography of the area effectively forces human movement around the southern slope, as an ecological gateway between the more ecologically fragile hills and rangelands of the northeast and the clement watered plains of the Lango region.
The prehistory of the study area, and the origin stories of the four cultures of relevance, originate in a complex and cyclical flow of human migrations undertaken in response to sustained periods of climatic stress; the names of famines from early times were passed down through centuries of oral tradition to be recorded during the mid-twentieth century, and validated into a chronology in the 1970s by early postcolonial scholarship drawing upon a record of Nile level measurements taken on the Nilometer on Rodah Island at Cairo, beginning in the Medieval era [26]. The historian’s task of dating the early history of present-day cultures is easier where there are king-lists, which are frequent among the more structured Bantu societies, including Buganda—but are also a feature of the Lwo cultural family, which arose in a ‘cradleland’ along the Bahr el Ghazal region of the Nile basin in present-day South Sudan [13, 26, 27].
While Lango culture is situated alongside the Acholi neighbors from whom they appropriated most of their language, they share a common historical origin with the Teso, as indicated by a remnant of distinctly Ateker-origin words—important nouns—remaining in Lango, including plant names and bodily organs (e.g., emany for liver). Lango history traces its descent primarily back to the Jie clan of the Karimojong, from which likewise descended the Teso—but at some remote point, the Lango gave up or drastically adapted their ancestral Ateker-based language in to adopt a Lwo dialect. Uzoigwe [28] considers the Lwo language “a very simple one” and speculates that although Lango origins may have been predominantly Ateker-speaking, the relatively simplicity of the Lwo tongue was likely a factor in the Lango adoption of a language common to their Acholi neighbors. In linguistic terms, as compared to the Ateker, the Lwo language has relative lack of syllabic complexity, and is of shallow orthographic depth [29, 30], apparently contributing to its wide adoption as a simple and effective lingua franca within the study area.
Cultural conceptions of health and illness
Extant within study area are culturally-specific explanatory models of health and disease, inclusive of 'folk etiologies' by which a given ailment may be related to internal states as well as external influences, in which the traditional healer serves as an intermediary between the patient and unseen causative agents both biotic and intangible [31, 32]. While the traditional healer relies on the bioactivity of plant-based medicines, her therapeutic portfolio may also involve purely ritual interventions to which are consigned illnesses or conditions ascribed to executive influences originating in the spirit world.
Central to the traditional religions of the Lango, Acholi and Ethur is the Lwo concept of Jok (Juok in leb Thur) as supreme being, the lexical root from which is derived jogi (plural of the small-j jok) as a generic name for individual spirits—including those particular to a clan or line of descent, those of known ancestors, and those of "unknown persons and dangerous beasts"—all of whom might possess a victim as a causative agent of affliction [33,34,35,36,37,38]. Likewise derived from the Jok root is the ajoka (Lango), ajwaka (Acholi) or ajuoga (Ethur)—a seer or diviner and healer who is initiated into knowledge of medicinal plants, and of the unseen influences which may cause physical or mental illness and may be propitiated by ritual (etogo) involving the individual, and at times the community (the latter category including chronic children's illnesses, impotence and eye disease) [39, 40]. In the words of the Acholi poet Okot p'Bitek, the healer is "a consultant psychiatrist, chemist and priest combined. He administered medicines which effected a cure and gave psychological treatment to patients who needed it" [38], including psychic ailments associated with social anxiety [41].
Writing a century ago, Driberg [33] describes an advanced Lango anatomical terminology (in which, for example, the hypogastrium or lower belly is named differently in men and women)—but laments the insufficiency of Lango medical nomenclature, in which etoku signifies yaws, eczema and sarcoma; angwal both paralysis and synovitis (synovial inflammation), and aola all manner of complaints of the throat, chest or lung involving cough. Indigestion was identified as "a much-dreaded complaint" then widely believed to be transmissible, and Driberg found the Lango "baffled" by all forms of veterinary illnesses. Atypically for a man of his era, Driberg credited the ajoka as being "endowed with wide knowledge and a scientific mind [as well as] primarily the physician of the soul… [with] an intimate knowledge of the use of herbs and plants for medicinal purposes above and beyond the popular remedies known to the vulgar, and certain operations are only performed by him, as for instance sucking the pus from boils" [33].
In opposition to the healer stands the wizard or ajok (ajwak) who delves in sorcery; as 'night-dancers' these wizards (who may be operating consciously or unconsciously) serve as agents of jealousy—attributed by the Ethur with causing complications in childbirth, elephantiasis and other disorders [42]. As causative agents of strife and illness, Lango culture recognizes a shade (tipu) originating in a person, and of non-human 'winds' (yamo)—elemental entities similar to the tiny beings of other cultures, which carry out the malign intentions of a tipu gone bad. In diagnosing occult ailments, chronic conditions with severe symptoms which can be traced to a known social conflict are the domain of shades, while passing ailments of less severe symptomology which cannot be traced to a social conflict are the domain of the winds [40]. Of the jok manifestations as diseases with a known ritual cure, the known and established endemic diseases were ascribed to the local Jok Lango, but others to the foreign Jok Nam (god of the lake), ruler of diseases thought to originate from the Bantu peoples to the southwest [34].
Following Driberg by a generation, the anthropologist Hayley usefully classified Lango medical conditions into three broad categories, comprising inevitable diseases of childhood which also afflict adults; unexplained illnesses of a purely biotic origin (two), and those ascribed to a manifestation of Jok power, of which the latter included "psychic disturbances and virulent diseases such as plague"—Jok (or a jok) being identified as the cause as well as the potential cure of such afflictions [37]. Hayley was struck by the fact that epilepsy (ekwinkwin) was explicitly recognized as being of a purely natural origin (at the time, untreatable) and thus relegated to the second, two category and not the third—underlining the fact that not all types of unexplained medical phenomena were automatically ascribed to occult influence in traditional society [37].
By comparison, Teso culture has many names for the supreme being, including Akuj ('the one above,' associated with the sun), prime mover of all things good and evil; the healing god Ejokit (as 'the good'), and Edeke—the 'god of calamity' (or vengeance) and a bringer of sickness, plague, and veneral disease [43, 44]. The latter name was also known among the Jie from which the Iteso descended [45]. It has been suggested that all events, including illnesses, have "a primary cause, Akuj, and a secondary cause, created agencies;" as a result, according to one traditional healer interviewed in 1979, it is unwise to rely on only one type of treatment for sickness [44].
Like the Lwo ajoka, the Teso emurwon ('diviner-prophet') works with ethnomedicinal cures and with ajokin (pure spirits) to counter the activity of acudan (the witch or sorcerer) and malign intentions of the elemental spirits iboro (plural of ibore), corresponding to the Lwo yamo, which can be distinguished by an otherworldly smell, and are said to be active when the finger-millet is ripening [44]. Like the Lwo ajoka, the Iteso emurwon receives their healing vocation from the spirit world (often after surviving a serious illness) but their phytomedicinal knowledge is transmitted from elder practitioners, and the institution is thought to predate the migration of the Iteso from their original homeland among the Jie [44, 45]. Like the ajoka, the emurwon is both a healer of diseases both physical and spiritual, and an intermediary between the departed and the living—treating afflictions caused by spirit possession both in the individual and within the broader community.
Given its cosmopolitan ethnic and historical origins, it may be reasonable to suggest that these disparate lines of cultural descent and influence may have provided the Lango with a relative diversity of ethnomedical traditions as compared to the other three cultures. At the outset of the study, it was supposed that some evidence of shared origins might be discerned in the commonality of medicinal plant use along the Lango cultural interfaces with the Acholi and Teso in particular.
Data collection
At the time of data collection, the continuity of traditional ways within the project area were reflected in the persistence of decentralized social and cultural institutions based around local (jago) chiefs and clan elders, particularly in the work-groups organized locally, in which agricultural labor was shared by neighbors on a rotating basis. These groups, known in leb Lango as wang tic (‘burn the work’) are often named after a vernacular proverb (e.g., the group name orib cing for ‘joined hands’—resonant of the proverb ‘many hands make light work’). These widely dispersed groups are constitute a social infrastructure which supported relief distribution during a series of droughts and crop failures in the 1980s, and provided access to revolving microcredit loans in support of rural livelihoods during the 1990s. Largely representative of the communities in which they are situated, with broad representation by women and the elderly in particular, these groups provide a forum for the exchange of ideas, making accessible the holders of traditional knowledge.
In order to establish prior informed consent among participating communities and individuals, introductory open meetings were convened at the community level over a period of several years, leading to a more focused set of community-based focus group discussions on plant use (Fig. 1), followed by a series of individual interviews on specific taxa, from which respondents holding specialized knowledge of plant use were engaged on basis of self-selection through purposive sampling, resulting in a de facto sample of 112 respondents, each of whom contributed one or more botanical specimens and use reports.

The study area
During 1999 and 2000, interviews on medicinal plant use were conducted with 112 subject matter specialists, each providing an herbarium specimen of a medicinal plant corresponding to one or more use reports, and describing the methods of harvest, processing and administration (Table 1). Herbarium samples were prepared by project staff and were subsequently presented to the Makerere University Herbarium (MHU) for identification and storage. Herbarium voucher codes for each specimen are provided by plant family and individual taxon in Table 2.
Concurrently with the data collection, an inventory of woody species and its size-class distribution was undertaken on a set of fixed and variable plots in the current districts of Otuke and Amuria [46], with an indication of overall frequency of woody species by size-class within these plots. Unfortunately, this work could not be extended to the current districts of Agago and Abim due to increasing insecurity including insurgent attacks on civilian targets within the study area at the time of data collection [47].
Data analysis
In August of 2022, and again in June 2023, the taxa list was updated according to the current botanical nomenclature. Based on the updated and current list of taxa, use reports were triangulated by three rounds of secondary research, beginning with a review of relevant ethnobotanical use reports, 13 of which were proximate to but outside of the current study area.
Standard reference books were also consulted, including J.O. Kowaro’s Medicinal plants of East Africa [48] and the five volumes of The Useful Plants of West Tropical Africa, H.M. Burkhill’s 1980–1990s revision of the original 1937 compendium by Dalziel [49,50,51,52,53]. A third reference resource of note is the online Prelude Medicinal Plants Database maintained by the Belgian AfricaMuseum (formerly Royal Museum for Central Africa), which yielded 30 corroborating use reports from 21 sources which could not be obtained directly [54]. A second database, PROSEA (Plant Resources of South-East Asia), was accessible during the first round of secondary research [55] and then went offline, but has been restored as of the time of publication.
In a second round of secondary research, the therapeutic profile of each taxon was assembled from the results of published pharmacological studies (mostly using in vitro and animal models), and from phytochemical analyses with a focus on bioactive compounds (either explicitly implicated, or potentially relevant). A third round of research surveyed the documented bioactivity and pathways of the specific molecules identified as being present in a particular taxon.
Comparative indices
The purpose of the study being to assemble an inventory of medicinal use applications among the four cultures, the interviewers did not request comprehensive or ranked lists of medicinal plants from each respondent, but use reports were based on the botanical specimens which were accessible to each respondent at the time the interview was conducted. Use of plant specimens as a focal point for structured interviews has been referred to as the ‘plant interview’ method of ethnobotanical research [56].
Data from the interviews were correlated in the aggregate to determine the relative importance of each taxon using the Relative Importance Index (RI), developed for ranking of medicinal plants by their pharmacological properties, and by the body systems affected [57]. The RI is a simple measure of the diversity of uses of a given taxon, without factoring in the number of informants [58], and without regard to any ranking of relative importance of each taxon by respondents.
where PHs(max) is obtained by dividing the normalized number of pharmacological properties attributed the species (PHs) by the maximum value in all medicinal species surveyed [PHs(max) = PHs/max (PH)], and BSs(max) is the normalized number of body systems affected by the species (BS) divided by the maximum number of body systems affected by all medicinal species cited [57].
Although some subsequent authors notably including De Albuquerque et al. have limited their calculations to published clinical data [59], the RI is used here to assess the relative importance of the cited taxa according to the totality of use reports for each taxon, not disregarding out of hand those use reports for which no prior published reports can be found.
In order to test the operational hypothesis, the Jaccard Index of similarity (JI) was first calculated as an indicator of relative degree of confluence (similarity) in the inventory of plants used as medicine among and between the four cultures of the study area [60], considering the ratio of species used by multiple cultures as compared to those cited by only one culture, without regard to commonality of specific use application.
where a is the number of taxa cited by both populations, b is the number of taxa cited only by the first of the two populations, and c the number of taxa cited by the second of the two populations [61].
Finally, the similarity of specific medicinal usage between the four cultures was assessed using Rahman’s Similarity Index (RSI), which provides a percentage of common use applications for each taxon between two populations.
where a is the number of taxa uniquely cited within the first population, b is the number of species unique to the second population, c is the number of taxa common to both populations for all uses, and d is the number of common species used to treat similar ailments by both populations [62, 63].
Results
Table 1 presents a summary of interview data and herbarium specimens collected from 112 respondents in 67 locations within the four districts, languages and cultures of the study area. The 112 key informant interviews yielded 289 medicinal use reports for 194 herbarium specimens used as medicine, subsequently identified as 108 taxa from 44 botanical families, of which just 12 families account for more than two thirds of all use reports. Fabaceae was by far the most cited plant family, at 20% of cited taxa and 21% of all total use reports.
Table 2 presents 280 medicinal use reports describing 263 different use applications for the treatment of 62 maladies or conditions (use categories), including the plant part used, preparation and administration and method of use, and the Relative Importance ranking of each taxon. Of the Relative Importance figures presented in Table 2, 13 taxa were ranked at 50% or higher, while 5 taxa were ranked above 70% (Table 3).
Plant parts used as medicine (Fig. 2) indicated a strong preference for the root, comprising about 60% of all use reports, followed by leaf (over 23%) in most cases involving dilution or decoction of the macerated root paste taken orally. Notable exceptions to this method of administration include those plant compounds which are applied topically to the skin (Cussonia arborea to treat pain and swelling, Cissus cornifolia for boils) or to cuts made in the skin (Rotheca myricoides and Sarcocephalus latifolius for pain, Erythrina abyssinica for paralysis, Steganotaenia araliacea to treat snakebite, Sclerocarya birrea for scorpion sting).

Plant parts used as medicine by proportion of Use Reports
The number of cited taxa and use reports by malady (Fig. 3) indicates an overall ranking frequency of three conditions—measles, diarrhea, and cough, all at above 20 taxa cited per condition, followed by stomach problems and wounds (all above 10 taxa cited), eye problems, sexually-transmitted diseases, and worms (above 5 taxa cited), and a long tail of eight maladies ranging between 5 and 3 taxa cited. With 41 use reports involving 27 taxa, treatment of measles was by far the most cited medicinal application, closely followed by measles and cough, and a second level of prevalence for stomach problems, wounds, and eye infections.

Ranking of maladies by number of Use Reports
Figure 4 and Table 4 show how the cited taxa are distributed by culture, including commonality of plant use along the six cultural interfaces, while Table 5 indicates the commonality of specific medicinal use application between the four cultures, indicating the strongest commonality between the Lango and Acholi cultures (united by markedly similar languages), by a factor of two over the Lango and Teso cultural interface, which represents shared historical origins, but no longer a common language.

Medicinal taxa cited by culture and interface (n = 108)
Of the 108 taxa cited across the study, 49 use reports cited 15 species in 18 identical use applications for 10 maladies shared between two or more cultures, of which only one species use application was shared between three cultures—Psorospermum febrifugum root for treatment of scabies (Table 6).
Not included in this analysis of cultural similarity of use were those use reports involving different plant parts of the same species used to treat the same malady, e.g., Bridelia scleroneura bark used in Lango to treat diarrhea, while the root is used in Teso for that purpose. One species, Solanum incanum, was cited by respondents of Teso and Ethur for unrelated ailments (root for diarrhea, fruit for eye infection).
Discussion
Context of historical studies
As provided in the supplemental file, review of the secondary research yielded 403 citations from 139 ethnobotanical publications, including full or partial matches to species/genus, plant part and administration by indication (malady or condition), providing full or partial corroboration of 193 (73%) of the 263 reported use applications. Of the 70 use applications which were not found in any earlier ethnobotanical reports, 16 (22%) were found to be possibly supported by secondary data from in vitro and in vivo studies, including those involving compounds reported to be present in the respective taxon or genus.
Of the 263 use applications by taxon listed in Table 2, 191 are at least partially corroborated by one or more earlier ethnobotanical studies drawn from across the entire Africa region. Indeed, several of the cited taxa have been identified among the earliest medicinal plant remains recovered by archeological studies in northern Nigeria, including Vitex spp. dating back to c. 2800–2450 BP, and Bridelia scleroneura, Pavetta sp. and Sarcocephalus latifolius dated earlier than 800 CE [64].
No earlier mention can be found within the earlier ethnobotanical literature of 72 of the 263 medicinal applications in the current study (about 27% all use reports obtained. One notable example is Lepistemon owariense (Convolvulaceae), with an RI value of 79% based on four reported pharmacological properties affecting seven body systems, for which no earlier mention has been found. Other use applications undocumented in the earlier literature include seven taxa used to treat measles (Albizia coriaria, Gardenia ternifolia., Leonotis nepetifolia, Pavetta crassipes, Strychnos innocua, Vitex madiensis and Zanthoxylum chalybeum); three as anti-emetic (Celosia leptostachya, Indigofera arrecta, Phoenix reclinata); Dicoma sessiliflora for urinary problems, and Vernonia perrottetii for eye problems.
Of the apparently novel use applications, eight have some association with bioactivity in pharmacological (in vitro or animal model) or phytochemical studies, including antiviral compounds in Commiphora Africana, Chrysanthellum americanum and Vernonia perrottetii; antibacterial compounds in Albizia amara and Synedrella nodiflora; anti-inflammatory compounds in Vachellia hockii and Senegalia polyacantha, diuretic compounds in Sarcocephalus latifolius, and antimicrobial, anti-inflammatory, analgesic and antipyretic compounds in Physalis minima, the leaf-paste of which is applied to the umbilical cord of the new-born infant.
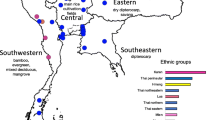
Figure 5 provides a geographic and historical context of the ethnopharmacological studies undertaken within Uganda, indicating that no earlier data were collected within the study area.

Geographic context of the Uganda studies
Of the earlier Ugandan studies mapped in Fig. 5, most accounts were limited to a specific ailment or condition [53, 65, 66] or a specific locality and culture [51, 52, 67,68,69,70].
Floristic and ecological context
From an ecological perspective, the number of cited taxa and use reports was compiled by plant family with intention to compare the findings with earlier studies, and with what is known of the floristic composition of the study area. Unfortunately, the earlier data (notably including the species lists compiled by Langdale-Brown et al. [14]) do not indicate relative abundance or frequency of occurrence, and the inventory and size-class distribution data collected on fixed and variable plots within the study area concurrently with data collection, some results of which were presented in an earlier paper [71], include only woody and not herbaceous species. Nonetheless, the degree to which Fabaceae have been selected for medicinal use stands in contrast to their natural occurrence—comprising over 24% of all medicinal use reports, as compared to the woody species inventory data, which places the family at just 4.2% of woody species by basal area in Otuke, and 18.6% by species composition in Amuria.
Folk taxonomy and medicinal use categories
Table 2 is organized by family, and some commonality of use is visually evident within particular genera and families—examples including the remedies for cough and diarrhea within the Combretaceae, wound care among the Compositae, treatment for diarrhea in Moraceae, hernia among the Rubiaceae, and measles and cough among the Rutaceae.
Table 2 provides the common vernacular phytonyms for each taxon cited according to each of the cultures citing it for a medicinal use. Classification systems within the vernacular nomenclature reflect emic dimensions of cultural meaning [32] by which plants are classified according to folk systematics [72]. In general, the vernacular phytonyms presented here differ between cultures in the interpretive accessibility of information held within them, partly a function of the linguistic structures of the vernacular languages in which they are recorded.
Among the Lwo phytonyms, such linguistic qualifiers include adjectives referring to morphological characters, with the adjectives white, black and red (atar, achol and rema) commonly used to distinguish plant species within a genus or family. Taxonomically, the generic name for a group of species formerly classified together under the genus Acacia is okutu, of which Vachellia sieberiana is known as okutu atar, or white acacia; the genus Terminalia is called opok (of which T. mollis is opok acol, black terminalia), and in the genus Albizia (ibata), A. schimperiana (ibata atar) is distinguished from another, non-medicinal species known as ibata achol.
Other Lwo adjectives and descriptive nouns are likewise used as qualifiers in the vernacular nomenclature to distinguish related species within a genus, such as Amaranthus caudatus L. (ocobo), from which A. graecizans L. is distinguished as local by the qualifier ‘Lango’ (as ocobo Lango), in the same manner that ash filtrate is called ‘local salt’ (kado Lango). Similarly, the cultivated Cleome gynandra L. (akeo) is distinguished from C. monophylla L. as akeo Jok, in which the qualifier may signify its wild occurrence, or other properties.
While some Lwo plant names have a clear meaning for which a basis is not evident (for example, kongo ogwal-ogwal or ‘frog’s beer’ for Physalis minima), the basis for others is more directly related to the pharmacological activities attributed to the plants. Notable examples here include ocoko lac for Dicoma sessiliflora, a treatment for urinary infections, in which ocoko stands for the name of the plant, while the suffix ‘lac’ signifies urine, thus indicating its application.
Perhaps the most pharmacologically significant example is the qualifier ‘yat’. Defined by Kokwaro and Johns as “a general term for shrub, tree or medicine” [73], these three meanings are listed separately by other sources [74, 75], the latter separating its meanings as referring to a tree (or wood), to medicine or to an herb. In each such case, yat is followed by a second noun, often indicating a malady or condition to which the plant can be applied as a remedy, and thus indicative of its primary pharmacological property according to the current or past therapeutic application.
Examples of such nomenclature provided in Table 2 include Aerva lanata, yat dobo (or ‘leprosy medicine’ in leb Acholi); Pleurolobus gangeticus, yat aola (cough medicine); Oxalis corniculata, yat leny (heartburn medicine). Another example is Gloriosa superba.—yat ania, referring to its use in treatment of pneumonia (despite the notoriously extreme colchicine toxicity of the plant), and the tuber of an unidentified creeper called yat cak (milk medicine), credited with increasing milk production in humans and in livestock. Although no identification could be made on basis of the specimen provided, the taxonomic description and reported morphology of the plant are consistent with Dioscorea L. species, of which several are known to contain estrogenic compounds [76], and nine are present within the study area [77]. Estrogen is known to stimulate development of the mammary ducts, and, in association with progesterone, to stimulate proliferation of secretory tissues [78].
Examples of Ateso plant names which seem to imply their given therapeutic use may include Vachellia hockii (ekisim), the flowers of which are rubbed on the breasts (ekisin) of a mother who has lost her child to stop milk flow; Pseudocedrela kotschyi (eputon), the root of which is used to treat measles (epuru), and Zanthoxylum chalybeum (eusuk), various parts of which are used as a cough treatment—the word for lung given being euko [79]. By contrast, the name for Rhynchosia sp. (ookot) is strongly suggestive of blood (aokot [80]), but is only cited here as a diarrhea treatment in Teso. This again may imply a former medicinal use no longer in practice within the respondent communities of the study area.
Data interpretation in the epidemiological context
From the etic perspective, results are consistent with the documented epidemiology of the study area. Together accounting for over 36% of use reports, the findings around the three major maladies—measles, diarrhea and cough—largely reflect the historical prevalence of these conditions among the respondent communities [81]. The national measles vaccination coverage rate in 2002 was just 74% [82], leaving over a quarter of all Ugandan children unprotected against measles; this number is likely to be considerably higher within the study area, given regional disparities in health-related outcomes and access and availability of treatment [83]. Bbaale [84] notes that rates of both diarrhea and acute respiratory infection are highest in the northern region, which he conjecturally linked to the history of civil conflict and displacement ending in 2008.
While measles was the malady most cited by number of taxa and number of combined use reports, this ranking is based specifically on the 27 use reports from Teso (Amuria District), the highest value (by a factor of two) of any malady by district. The highly contagious disease measles (rubeola) is caused by a single-stranded, negative sense RNA virus in the genus Morbillivirus of the family Paramyxoviridae, which also includes other parainfluenza viruses, e.g., mumps, rubella, and respiratory syncytial virus (RSV); measles results in a wide variety of health complications including pneumonia, blindness and chronic neurological conditions—and, although largely preventable by vaccine, measles remains responsible for an estimated 100,000 deaths each year [85,86,87,88,89]). Given the limited coverage of measles vaccination, these figures underline the relevance of locally available ameliorative treatments to manage the symptoms of the disease [90].
While a wide variety of phytochemical compounds have been found to inhibit viral replication via various pathways [91, 92], very few compounds are specifically linked to inhibition of the measles virus itself. Recently identified as antiviral agents with therapeutic value [93, 94], non-flavonoid phenolic coumarins and their derivatives (including pyranocoumarins) have been found to inhibit measles virus replication [95]. Although the mechanism of action is not understood, coumarin-like compounds have been found to interfere with or inhibit the viral enzymes of other, single-stranded positive sense Ribonucleic acid (RNA) viruses including Human Immunodeficiency Virus (HIV) [85]. According to the compositional studies consulted, coumarins and coumarin derivatives have been reported as present in 9 of the 27 taxa cited by respondents as being used in treatment of measles (Table 2).
Diarrhea was the highest-ranked malady by taxon and use report in three of the four cultures (Lango, Acholi and Ethur), by a factor of two over the second-ranked malady in those cultures. Diarrhea is the second leading cause of death globally in children under five years old, and a leading cause of malnutrition in that age group; nearly 1.7 billion cases of childhood diarrheal disease result in an estimated 525,000 child deaths each year [96]. Ugandans suffer the highest mortality rate of children under 5 years old in the East Africa region [97], with diarrhea accounting for over 20% of child deaths, against a global average of 8.6% [98, 99]. At the time of the data collection, prevalence of diarrhea within the northern region was the highest in Uganda, at any moment affecting 29.3% of the population [100], while a 2018 study specific to Agago District found the proportion children under 5 suffering from diarrhea to be over 40% [98].
Causative organisms of acute diarrhea include viruses (notably Rotavirus), Gram-positive and Gram-negative strains of bacteria (notably Shigella and Campylobacter spp., Escherichia coli and Staphylococcus aureus), and protozoa (notably Giardia lamblia) [101]. Phytochemical compounds effective in treating diarrhea include polyphenol catechins and tannins [102, 103] and the flavonol quercetin [104], specifically through increased colonic water and electrolyte reabsorption [103].
Cough was ranked at second in terms of use reports in all for regions, including Teso with 16 use reports. Persistent cough in Uganda has been linked to household air pollution including exposure to indoor smoke from cooking and lighting [105], and to infection by human pathogens including the influenza virus, particularly during the rainy season [106] and the Gram-negative, aerobic, pathogenic, encapsulated coccobacillus Bordetella pertussis, responsible for an estimated 400,000 annual deaths, mostly of infants in developing countries [99]. Several other bacteria—most notably the Gram-positive Streptococcus pneumoniae but also the Gram-negative Mycoplasma pneumoniae and Chlamydophila pneumoniae—are implicated in infectious pneumonia, the leading cause of mortality among children under 5 in sub-Saharan Africa, accounting for 12.8% of all such deaths [98]. In Uganda, Acute Respiratory Infections (ARIs) remain the leading cause of childhood morbidity and mortality among under-five children [107].
Phytochemical compounds with documented therapeutic activity in the treatment of cough include polysaccharides, anthraquinones and their derivatives. An in vivo study of cats [108] found cough suppressive activity in polysaccharide compounds isolated from nine plant species. [109]. Another study found that anthraquinone derivatives ameliorate lung inflammatory response, an effect recently reviewed with particular reference to Aloe (Asphodelaceae), Senna (Fabaceae) and Rheum L. (Polygonaceae) species [110].
Of the taxa cited for treatment of cough, Aloe volkensii is conspicuously abundant in polysaccharides [111], with a phytochemical profile including anthraquinones and pre-anthraquinones [112], as well as alkaloids, saponins, glycosides, flavonoids, and tannins [113] [114], noting that antioxidant compounds have been associated with a protective effect in cough suppression [115, 116].
Other maladies and conditions for which fewer use reports were obtained and species cited are nonetheless highly significant in terms of their mortality or morbidity, notably including snakebite—responsible for an estimated 32,000 annual deaths across sub-Saharan Africa (a quarter of the global total), leaving as many as 100,000 survivors with permanent physical disabilities [117]. The health burden on survivors of snakebite may involve hemorrhage, tetanus, contractures (debilitating stiffening of muscle or connective tissue), myonecrosis (life-threatening muscle infection), scarring, and tissue inflammation that result from the bites [118], resulting in 5000–15,000 amputations annually [119].
Horse-derived antivenin sera comprise the sole medical treatment for snakebite—but these are highly perishable, are unable to prevent local tissue damage, can induce adverse reactions including anaphylactic shock, and are scarce and unaffordable in the rural areas where nearly all envenomation occurs [118]. A 2018 study decried a compound global "crisis" of poor antivenom quality, availability and reliability of supply [120], and other authors have questioned the clinical effectiveness of available products within the Africa region in particular, as many such antivenin products were developed specifically to treat envenomation by Asian snake species [117]. In northern Uganda, where more than a third of snakebite victims are younger than 18 years, antivenom supplies are insufficient even at hospitals for optimum treatment of envenomation according to WHO guidelines [121]. These interrelated factors underline the importance of locally available envenomation treatments.
Of the four taxa cited for use in treatment of snakebite, Annona senegalensis Pers. root for treatment of snakebite was corroborated nine times in the ethnobotanical reports, and has been assessed clinically against venom of puff adder Bitis arietans [122], black-necked spitting cobra Naja nigricollis [123, 124], and West African Carpet viper Echis ocellatus [125].
No clinical antivenom studies were found on Gardenia ternifolia, although a 2015 study observed anti-inflammatory cyclooxygenase-1 (COX-1) inhibitory activity in an unspecified ethanolic extract, noted as a pathway of relevance to mouse hind paw oedema induced by Bothrops insularis (Golden Lancehead pit viper) snake venom [126]. Two studies [127, 128] have evaluated the in vitro antioxidant activity of G. ternifolia leaf extract containing flavonoid aglycones.
Although Steganotaenia araliacea root is cited as a snakebite remedy in seven ethnobotanical sources (with another report for its leaves), no clinical studies nor phytochemical data could be found for the species. No clinical evidence of antivenom activity was found on Trichilia emetica, but compositional studies indicate the presence of compounds with activity along potential antivenom pathways, including limonoid triterpenoids in root bark with notable anti-inflammatory properties [129, 130], noting further that a 2007 study reported a neurotoxin blocking activity of the limonoid triterpenoid toosendanin [131]. The flavonoid glycosides found to be present in a T. emetica seed extract [132] have been found to inhibit the phospholipase A2 (PLA2)-II toxins associated with some snake venoms [133, 134].
Although malaria is evidently a malady of great significance in northern Uganda, and the leading cause of morbidity and mortality in Uganda [135], it was ranked very low in the data (with just two use reports in Teso, and one in Lango), possibly reflecting the availability of pharmaceutical treatments, which are widely sold across the region by local traders and at weekly rural markets. The vernacular name for Schkuhria pinnata, reported as being used to treat malaria, was recorded as ‘kilorokwin’ in Ateso—certainly not a word characteristic of that language, but phonetically identical in the local pronunciation to the antimalarial compound chloroquine (chloroquine phosphate)—long the first line of pharmaceutical defense against non-resistant Plasmodium infection.
The sole taxon cited by respondents (in both Lango and Acholi) as a treatment for epilepsy, Hoslundia opposita, is abundantly evidenced in both the ethnobotanical record and in clinical studies. Noting its use in treatment of convulsion and epilepsy, as well as vertigo and mental disturbance, the anticonvulsant (central nervous system depressant) activity of a chloroform root extract of H. opposita was assessed in an animal model at 60% protection against leptazol-induced convulsions, and the extract was credited with potentiating the phenobarbitone sleeping time with an anticonvulsant activity comparable to benzodiazepines [136]. A later study [137] confirmed these results with respect to in vitro γ-Aminobutyric acid (GABA)A-benzodiazepine receptor binding activity of an ethanolic H. opposita leaf extract.
Cited in 7 use applications across three body systems for an RI of 71%, the root paste of Sarcocephalus latifolius is applied to incisions, or taken orally, as analgesic 'for any pains’. This use application is corroborated by multiple ethnobotanical sources cited by Burkhill [49]. More recently, a highly controversial 2013 paper [138] claimed to have isolated from the root ( ±)cis-2-[(dimethylamino) methyl]-1-(3 methoxyphenyl) cyclohexanol—a morphine analog commonly known by its international non-proprietary name, tramadol. A 2016 study [139] followed up on this controversial finding with a comprehensive study of S. latifolius which identified multiple antinociceptive compounds, most notably indoloquinolizidine alkaloids to which they attributed antiplasmodial and antibacterial, as well as analgesic activities.
Beyond the purely medical conditions which can be cross-referenced to the clinical data, respondents cited indications for more clinically ambiguous conditions which cannot be identified with confidence, which presented interpretive challenges in terms of data triangulation, which are discussed in the limitations section below. Four taxa were cited with reference to use applications loosely corresponding to ‘debility’—interpreted by the author to reflect use of the specified extract as an immunostimulatory tonic. Among them, the ‘bulb’ (corm) of Gladiolus dalenii was said to be chewed ‘to treat any sickness,' while the root paste of Kigelia africana was indicated as treatment for ‘general body weakness’. Respondents likewise ascribed immunostimulatory activities in the leaves of Cyphostemma adenocaule and the fruit of Strychnos innocua (‘you cannot get sick after eating’).
Perhaps related to these applications are the two taxa more specifically cited for treatment of anemia—the bulb extract of Gloriosa superba (notoriously toxic due to its high levels of the cytotoxic alkaloid colchicine), and the root extract of Grewia villosa. The antihemolytic activity of G. superba extracts has been evaluated in in vitro studies [140, 141], while a 2010 study [142] reported in vitro antioxidant and in vivo hepatoprotective activity γ-lactones isolated from a stem extract of a species identified as 'Grewia tiliaefolia' (presumably G. tiliifolia A.Rich., syn. G. amicorum Steud.).
In another ambiguous indication, the root paste of Rhynchosia hirta was reported to be burnt, the smoke inhaled by patient ‘to chase devils’—interpreted by the author as an antipsychotic treatment. While the ethnobotanical literature holds no corroboration of this usage, the presence of alkaloids and saponins in Rhyncosia species as been noted [143] noted, to which antipsychotic activities have been [144].
Other notable results which beg a degree of cultural interpretation include the reported use of Synedrella nodiflora in treatment of a condition called ‘false tooth’ or ebino. Although classified here as a dental condition, in fact there is no clinical basis to support a cultural belief, widespread within the region, that the eruption of primary canine teeth causes fever and diarrhea, often leading to removal of the emerging tooth buds using unsterilized instruments and without anesthesia or antiseptic [145]. Several years prior to the study, the author witnessed one such extraction within the Lango sub-region, effected with a sharpened bicycle spoke.
The belief in ‘false tooth’ has been explained by emergence of the primary canine teeth corresponding to the time of first exposure to a range of ailments including diarrhea, which may lead to dehydration which may make the tooth bud more pronounced in appearance [145]. Because complications following the extraction are linked to increased morbidity and mortality, the use of an herbal treatment in lieu of traditional extraction (rightly termed ‘infant oral mutilation’ [146] may be considered a positive development.
Limitations
According to other contemporaneous data sets obtained in the study area in parallel to this study, the results presented here seem to have under-reported the actual use of some taxa—most notably including Vitellaria paradoxa subspecies nilotica, around which the broader study of on-farm biodiversity was oriented. In addition to a biodiversity inventory and size class distribution of woodland species within the project area, results of which were published in an earlier paper [71], the project facilitated applied research on the cultural values of the tree which yielded 105 use reports specific to the medicinal uses of the tree in Lango and Teso in particular, compiled in a graduate thesis by a project intern [147].
In corroboration of the sole use report obtained for that species in this study, treatment of diarrhea in the Bratcher data was mentioned in 12 use reports focused on the roots of the tree, and 10 use reports on the bark, and a single use report on the leaves, with treatment of stomach ache similarly reported for roots (7 use reports), bark (5), shea butter (2) leaves (1) and seed. Of the 105 use reports in that report, 32 focused on topical use of shea butter for ‘smearing’ of new-born infants to protect the skin, also reflecting a cultural belief that the practice facilitates growth and strength (in the words of one respondent, ‘so they'll sleep nicely and grow fast with smooth skin’), with 7 use reports on the same application for children after bathing, 7 on use of shea butter to treat wounds, 4 for cough, 2 for stomachache, 2 to treat the cut umbilical cord, 2 to treat dry or sun-burnt skin, 2 for massage for sickness or dislocations, and one each for use of the liquid shea butter as a decongestant, to treat swelling (or infection), rashes, scabies, for skin care in pregnancy, for removing splinters or things from ear, as an emetic, and to treat measles and tuberculosis. Single use reports were collected for V. paradoxa roots cited for treatment of sexually-transmitted infections and worms, and flowers for measles, the leaf latex to treat fresh wounds, and the dross (seed matter remaining after shea butter extraction) in veterinary medicine to treat a chick's eyes and ears. These findings indicate that a methodology not strictly based on the availability of botanical specimens may have yielded a higher number of use reports by respondents.
The results presented here are bounded by limitations imposed by the study design, as well as the circumstances of its implementation and analysis. Although the literature around best ethnobotanical methods and their theoretical basis has been prolific in the intervening years since the data were collected [148], at the time of the data collection these methods were largely nascent [56]. A fundamental limitation of the study is that it was not originally intended for publication, but as a baseline and diagnostic study of on-farm biodiversity within the four communities (and cultures) served by an integrated conservation and development project. According to the parallel data set described above, this focus seems to have led to compensatory under-reporting on that species in particular—further suggesting that the data presented here are less than exhaustive in scope.
Presenting additional challenges to its analysis, data presented here were collected using two different data collection instruments over the course of the study, requiring careful reading of all original entries by the author. The original form used as a guide in the first key informant interviews initially allocated limited space for data collection, inconveniently listing five specimens over two paper pages—a layout requiring much back-and forth by the interviewer, and limited opportunity for elaboration on the part of the respondent. A second instrument was subsequently developed to provide a dedicated full page to each taxon, which allowed for supplementary notes to be added by the researcher to accommodate additional details of cultural context and practice.
Because participation was voluntary and sampling based on self-selection, some holders of relevant knowledge may have opted out, or not shared all available information on the maladies and conditions for which data were collected; we cannot know what was withheld or lost.
Another notable limitation is the rigidity of the study protocol, limiting data collection to taxa for which botanical voucher specimens could be collected and successfully identified by the national herbarium at Makerere University, in line with standard ethnobotanical practice [149, 150]. Thus, the timing of each interview would have limited the availability of the required botanical material, as would the seasonal morphology of the taxon, and its form; in the earlier publication on food plants [71] cited above, this requirement seems to have led to notable under-reporting on the important fruit tree Borassus aethiopum Mart—the tall savanna palm posing a daunting prospect for the most determined botanical collector.
In preparing this study for publication twenty years after the data collection, the author worked from the original entries and notes made by the interviewers, ranging from sparse initial entries to more expansive and anecdotal accounts. In many cases this involved interpretation, particularly as regards the body systems involved in a particular ailment, such as ‘stomach problems’ or ‘eye problems’ which have been left as such in Table 2, although according to the Relative Importance Index metric described above, the author was obliged to provide interpretations as to the number of pharmacological properties attributed to each taxon, and the number of body systems within which these properties were active. Because these interpretations could no longer be checked with the respondents, this may represent a source of error in the rankings.
An example of (apparently) purely ritual function, bumping the head of a mumps sufferer on a bough of Kigelia africana, was included in Table 2 as a medical treatment prima facie—whereas another example, exorcism of spirits from a patient by in taking by inhalation of leaf volatiles in steam, was subject to author interpretation as a treatment for psychosis. Otherwise, maladies and conditions of indication are left as recorded, representative as they are of the emic (respondent cultural) perspective.
Conclusions
The study provides an inventory of medicinal plant use applications and an account of the indigenous ethnopharmacological knowledge held within four cultures of northern Uganda, at an historical moment before conflict and dislocation disrupted the transmission of traditional knowledge to the current generation. During the two-decade interval since the data were collected, Uganda has produced its share or better of ethnobotanical studies, reflecting a relatively high level of awareness and an enabling policy environment, which provide a degree of ethnobotanical, pharmacological and phytochemical corroboration of the majority of reported use applications, including some around the periphery of the study area. Of the 309 sources consulted here, 224 (72%) were published during the last 20 years.
The ethnopharmacological use of plants in the Acholi, Teso and Ethur cultures of Uganda have previously not been documented in earlier ethnopharmacological studies—to date, a lacuna comprising the Nilotic cultural family, within northern Uganda and contiguous areas of South Sudan—so their inclusion here contributes new data to the field in that respect. By comparison to the earlier Uganda studies, this paper presents a more comprehensive review of several types of corroborating literature, distinguishing ethnobotanical uses from pharmacological and compositional data, drawing deeply from an extensive body of literature including ethnobotanical, pharmacological and phytochemical studies. As such, this paper will assist in extending interpretation of the historical Ugandan corpus.
While the results of the study are largely consistent with earlier ethnobotanical studies of the Africa region as a whole, and a majority of reported use applications reflected in the literature, a significant proportion of the use reports (on the order of 27%) cannot be corroborated by those earlier studies, though pharmacological and phytochemical data for some taxa show promise. These taxa, in particular, should be investigated further by future researchers. Future studies should likewise seek to determine whether the body of knowledge presented here is still held within the study area, and whether use patterns and frequency of use described by the respondents have changed over time.
It has been suggested that the environmental knowledge of rural communities can provide a foundation upon which to establish collaborative conservation and management of plant biodiversity [8], and that cultural comparisons of ethnobiological knowledge provide a basis for conservation of species through locally-driven resource management [151]. As such, it is hoped that the results of this study may contribute to these long-term outcomes.
Availability of data and materials
The dataset supporting the conclusions of this article is included within the article and its additional file.
Notes
Also spelled as Aswaa, Acwa, Acwaa.
Abbreviations
- ARIs:
-
Acute Respiratory Infections
- COX-1:
-
Cyclooxygenase-1
- GABA:
-
γ-Aminobutyric acid
- HIV:
-
Human Immunodeficiency Virus
- JI:
-
Jaccard Index of Similarity
- MHU:
-
Makerere University Herbarium
- PL:
-
Phospholipase
- PROSEA:
-
Plant Resources of South-East Asia
- RSI:
-
Rahman’s Similarity Index
- RNA:
-
Ribonucleic acid
- RI:
-
Relative Importance Index
- RSV:
-
Respiratory Syncytial Virus
- STD:
-
Sexually-Transmitted Disease
- UR:
-
Use Report
- WHO:
-
World Health Organization
References
Hardy K. Paleomedicine and the use of plant secondary compounds in the Paleolithic and Early Neolithic. Evol Anthropol. 2019;28(2):60–71.
Scurlock J. Ancient mesopotamian medicine. In: A Companion to the Ancient Near East. 2005:302-15.
Willis K. State of the world's plants 2017. Royal Botanical Gardens Kew. 2017. https://stateoftheworldsplants.com/2017/report/SOTWP_2017.pdf
Fowler MW. Plants, medicines and man. J Sci Food Agric. 2006;86(12):1797–804.
World Health Organization. WHO traditional medicine strategy: 2014–2023. World Health Organization; 2013.
Chatora R. An overview of the traditional medicine situation in the African region. African Health Monitor. 2003;4(1):4–7.
Howes MJ, Quave CL, Collemare J, Tatsis EC, Twilley D, Lulekal E, Farlow A, Li L, Cazar ME, Leaman DJ, Prescott TA. Molecules from nature: reconciling biodiversity conservation and global healthcare imperatives for sustainable use of medicinal plants and fungi. Plants People Planet. 2020;2(5):463–81.
Alves RR, Rosa IM. Biodiversity, traditional medicine and public health: Where do they meet? J Ethnobiol. 2007;3:1–9.
Voeks RA, Leony A. Forgetting the forest: assessing medicinal plant erosion in eastern Brazil. Econ Bot. 2004;58(1):S294-306.
Gauvin LR. In and out of culture: Okot p'Bitek's work and social repair in post-conflict Acoliland. Oral Tradition. 2013;28(1).
UBOS. Uganda demographic and health survey 2016. Kampala. Uganda Bureau of Statistics (UBOS) and ICF. Kampala and Rockville, Maryland, USA (2018).
Farbrother HG, Muro JM. Water. In: Jameson JD, editor. Agriculture in Uganda. 2nd ed. Oxford: Oxford University Press; 1970.
Jameson JD, editor. Agriculture in Uganda. 2nd ed. Oxford: Oxford University Press; 1970.
Langdale-Brown I, Osmaston HA, Wilson JG. The vegetation of Uganda and its bearing on land use. Government of Uganda: Entebbe (1964).
Petrie G, Liwa EJ. Comparative tests of small-scale aerial photographs and Spot satellite images for topographic mapping and map revision in eastern, central and southern Africa. ITC J. 1995;1(1):43–55.
Hall JB, Aebischer DP, Tomlinson HF, Osei-Amaning E, Hindle JR. Vitellara paradoxa: a monograph. Bangor: University of Wales; 1996.
Garibaldi A, Turner N. Cultural keystone species: implications for ecological conservation and restoration. Ecol Soc. 2004;9(3):18.
Boffa JM. Agroforestry parklands in sub-Saharan Africa. Rome: FAO; 1999.
Pullan RA. Farmed parkland in West Africa. Savanna. 1974;3(2):119–51.
UBOS. Otuke. The National Population and Housing Census 2014—Area Specific Profile Series, Uganda Bureau of Statistics: Kampala, Uganda (2017)
UBOS. Agago. The National Population and Housing Census 2014—Area Specific Profile Series, Uganda Bureau of Statistics: Kampala, Uganda (2017).
UBOS. Amuria. The National Population and Housing Census 2014—Area Specific Profile Series, Uganda Bureau of Statistics: Kampala, Uganda (2017).
UBOS. Abim. The National Population and Housing Census 2014—Area Specific Profile Series, Uganda Bureau of Statistics: Kampala, Uganda. 2017.
Westerhaus M. Linking anthropological analysis and epidemiological evidence: formulating a narrative of HIV transmission in Acholiland of northern Uganda. SAHARA-J. 2007;4(2):590–605.
Herring RS. The view from Mount Otuke: migrations of the Lango Omiro. In: Webster, JB. (ed.) Chronology, Migration and Drought in Interlacustrine Africa, pp. 283–316. Longman (1979)
Webster JB. Noi! Noi!: Famines as an aid to interlacustrine chronology. In: Webster, JB. (ed.) Chronology, migration and drought in interlacustrine Africa, pp. 1–37. Longman (1979).
Ogot BA. History of the southern Luo: Migration and Settlement.
Uzoigwe GN. The beginnings of Lango society: A review of evidence. J Hist Soc Nigeria. 1973;1:397–411.
Frost R, Katz L, Bentin S. Strategies for visual word recognition and orthographical depth: a multilingual comparison. J Exp Psychol Hum Percept. 1987;13(1):104.
Seymour PH, Aro M, Erskine JM. Foundation literacy acquisition in European orthographies. Br J Psychol. 2003;94(2):143–74.
Foster GM. Disease etiologies in non-western medical systems. Am Anthropol Dec. 1976;78(4):773–82.
Gaoue OG, Coe MA, Bond M, Hart G, Seyler BC, McMillen H. Theories and major hypotheses in ethnobotany. Econ Bot. 2017;71:269–87.
Driberg JH. The Lango. TF Unwin Limited (1923).
Hayley TS. The power concept in Lango religion. Uganda J. 1940;7:98–122.
Wright AC. The supreme being among the acholi of Uganda: another viewpoint. Uganda J. 1940;7(3):130–7.
Akena N. Lango religion. Uganda J. 1959;23(2):188–90.
Ogot BA. The concept of Jok. Afr Stud. 1961;20(2):123–30.
p’Bitek O. The concept of jok among the Acholi and Lango. Uganda J. 1963;27(1):15–29.
Abrahams RG. Spirit, twins, and ashes in Labwor, Northern Uganda. In: The Interpretation of Ritual, pp. 115–34. London: Tavistock Publications (1972).
Curley RT. Elders, shades, and women: ceremonial change in Lango. Uganda: Univ of California Press; 1973.
p’Bitek O. Religion of the central Luo. Nairobi: East Africa Literature Bureau; 1971.
Abrahams R. A modern witch-hunt among the Lango of Uganda. Camb Anthropol. 1985;1:32–44.
Lawrance JCD. A history of Teso to 1937. Uganda J. 1955;19(1):7–40.
Ekeya BJ. The Emurwon-diviner/prophet-in the religion of the Iteso (Doctoral dissertation, University of Nairobi).
Lamphear JE. The traditional history of the Jie of Uganda. University of London, School of Oriental and African Studies (United Kingdom); 1972
Nkuutu D, Lovett PN, Masters ET, Ojok P, Obua J. Tree management and plant utilisation in the agroforestry parklands of Northern Uganda. In: Proceedings, the shea butter tree Vitellaria paradoxa: first regional conference for Eastern & Central Africa. COVOL Uganda: Lira, Uganda. 2000;26–30.
Nannyonjo J. Conflicts, poverty and human development in Northern Uganda. The Round Table. 2005;94(381):473–88
Kokwaro JO. Medicinal Plants of East Africa. East African Literature Bureau; 1976.
Burkhill, HM. The useful plants of West Tropical Africa, vol. 1, 2nd edn. Royal Botanic Gardens: Kew; 1985.
Burkill, HM. The useful plants of West Tropical Africa, volume 2, 2nd edn. Families E-I., Royal Botanic Gardens: Kew; 1994.
Burkhill HM. The Useful Plants of West Tropical Africa, vol. 3, 2nd edn. Families J–L., Royal Botanic Gardens: Kew; 1995.
Burkhill HM.The useful plants of West Tropical Africa, vol. 4, 2nd edn. Families M-R., Royal Botanic Gardens: Kew; 1997.
Burkhill HM. The useful plants of West Tropical Africa, vol. 5, 2nd edn. Families S–Z., Royal Botanic Gardens: Kew, 2000.
PRELUDE. Medicinal Plants Database. 2023. Online at: https://www.africamuseum.be/en/research/collections_libraries/biology/prelude
Hidayat S. Synedrella nodiflora (L.) Gaertner [Internet] Record from Proseabase. van Valkenburg, JLCH, Bunyapraphatsara N. (eds.). PROSEA (Plant Resources of South-East Asia) Foundation, Bogor, Indonesia. http://www.proseanet.org, 2001 [currently at https://prosea.prota4u.org/]. Accessed 12 Aug 2021.
Alexiades MN, Sheldon JW. Selected guidelines for ethnobotanical research: a field manual. Bronx: New York Botanical Garden; 1996.
Bennett BC, Prance GT. Introduced plants in the indigenous pharmacopoeia of Northern South America. Econ Bot. 2000;1:90–102.
Leonti M. The relevance of quantitative ethnobotanical indices for ethnopharmacology and ethnobotany. J Ethnopharmacol. 2022;24(288): 115008.
De Albuquerque UP, De Medeiros PM, De Almeida ALS, Monteiro JM, Neto EMDFL, de Melo JG, Dos Santos JP. Medicinal plants of the caatinga (semi-arid) vegetation of NE Brazil: a quantitative approach. J Ethnopharmacol. 2007;114(3):325–54.
Jaccard P. Nouvelles recherches sur la distribution florale. Bull de la Soc Vaud des Sci Nat. 1908;44:223–70.
Höft M, Barik SK, Lykke AM. Quantitative ethnobotany. Applications of multivariate and statistical analyses in ethnobotany. People and Plants working paper. 1999;6:1–49.
Rahman IU, Hart R, Afzal A, Iqbal Z, Ijaz F, Abd Allah EF, Ali N, Khan SM, Alqarawi AA, Alsubeie MS, Bussmann RW. A new ethnobiological similarity index for the evaluation of novel use reports. Appl Ecol Environ Res. 2019;17(2):2765–77.
Asiimwe S, Namukobe J, Byamukama R, Imalingat B. Ethnobotanical survey of medicinal plant species used by communities around Mabira and Mpanga Central Forest Reserves, Uganda. Trop Med Health. 2021;49(1):52.
Orijemie EA. The Archaeobotany of the later stone age (LSA) in Nigeria: a review. In: Mercuri, A.M. et al. (eds.) Plants and people in the African past. 2018;362–379.
Anywar G, van’t Klooster CI, Byamukama R, Wilcox M, Nalumansi PA, de Jong J, Rwaburindori P, Kiremire BT. Medicinal plants used in the treatment and prevention of malaria in Cegere Sub-County, Northern Uganda. Ethnobot Res Appl. 2016;14:505–16.
Tabuti JR, Kukunda CB, Waako PJ. Medicinal plants used by traditional medicine practitioners in the treatment of tuberculosis and related ailments in Uganda. J Ethnopharmacol. 2010;127(1):130–6.
Kamatenesi MM, Acipa A, Oryem-Origa H. Medicinal plants of Otwal and Ngai sub counties in Oyam district, Northern Uganda. J Ethnobiol. 2011;7(1):1–4.
Tabuti JR, Lye KA, Dhillion SS. Traditional herbal drugs of Bulamogi, Uganda: plants, use and administration. J Ethnopharmacol. 2003;88(1):19–44.
Tabuti JR, Dhillion SS, Lye KA. Ethnoveterinary medicines for cattle (Bos indicus) in Bulamogi county, Uganda: plant species and mode of use. J Ethnopharmacol. 2003;88(2–3):279–86.
Tugume P, Kakudidi EK, Buyinza M, Namaalwa J, Kamatenesi M, Mucunguzi P, Kalema J. Ethnobotanical survey of medicinal plant species used by communities around Mabira Central Forest Reserve, Uganda. J Ethnobiol. 2016;12(1):1–28.
Masters ET. Traditional food plants of the upper Aswa River catchment of northern Uganda—a cultural crossroads. J Ethnobiol Ethnomed. 2021;17(1):1–21.
Phanuel AS. Plant species in the folk medicine of Kit Mikayi Region, Western Kenya. Ethnobot Leafl. 2010;2010(7):13.
Kokwaro JO, Johns T. Luo biological dictionary. Nairobi: East African Publishers; 1998.
Carollo B. Practical Lango Grammar. EUT Edizioni Università di Trieste. 1991.
Okonye G. A simplified Lango—English English—Lango dictionary. Kampala: Fountain Publishers; 2012.
Cheng WY, Kuo YH, Huang CJ. Isolation and identification of novel estrogenic compounds in yam tuber (Dioscorea alata Cv. Tainung No. 2). J Agric Food Chem. 2007;55(18):7350–8.
Lind EM, Tallantire AC. Some common flowering plants of Uganda. London: Oxford University Press; 1962.
Erb RE, Monk EL, Mollett TA, Malven PV, Callahan CJ. Estrogen, progesterone, prolactin and other changes associated with bovine lactation induced with estradiol-17β and progesterone. J Anim Sci. 1976;42(3):644–54.
Ongodia SP, Ejiet A. Ateso English dictionary. Kampala: Fountain Publishers; 2008.
Apuda IL. Medicinal plants in Teso (Indigenous Medicine). Annotated list. In: Ateso-English dictionary for intermediate learners. Ebook and Mobile app. Katakwi, Uganda: Strategic Outcomes Inc. 2007.
Ayiga N, Ntozi JP, Ahimbisibwe FE, Odwee JO, Okurut FN. Causes, patterns, differentials and consequences of AIDS mortality in Northern Uganda. In: The Continuing African HIV/AIDS epidemic: responses and coping strategies. Canberra: Australian National University, National Centre for Epidemiology and Population Health, Health Transition Centre. 1999;139–54.
Muwonge A, Nanyunja M, Rota PA, Bwogi J, Lowe L, Liffick SL, Bellini WJ, Sylvester S. New measles genotype, Uganda. Emerg Infect Dis. 2005;11(10):1522.
Armstrong-Hough M, Kishore SP, Byakika S, Mutungi G, Nunez-Smith M, Schwartz JI. Disparities in availability of essential medicines to treat non-communicable diseases in Uganda. PLoS ONE. 2018;13(2): e0192332.
Bbaale E. Determinants of diarrhea and acute respiratory infection among under-fives in Uganda. Australas Medical J. 2011;4(7):400–9.
Barnard DL. Inhibitors of measles virus. Antivir Chem Chemother. 2004;15(3):111–9.
Danova I. A review of measles virus. Probl Infect Parasit Dis. 2021;49(2):5–13.
Leung AK, Hon KL, Leong KF, Sergi CM. Measles: a disease often forgotten but not gone. Hong Kong Med J. 2018;24(5):512–20.
Moss WJ. Measles. Lancet. 2017;390:2490–502.
Perry RT, Halsey NA. The clinical significance of measles: a review. J Infect Dis. 2004;189(Supplement_1):S4-16.
Plemper RK, Snyder JP. Measles control–Can measles virus inhibitors make a difference? Curr Opin Investig Drugs. 2009;10(8):811.
Ben-Shabat S, Yarmolinsky L, Porat D, Dahan A. Antiviral effect of phytochemicals from medicinal plants: applications and drug delivery strategies. Drug Deliv Transl Res. 2020;10:354–67.
Musarra-Pizzo M, Pennisi R, Ben-Amor I, Mandalari G, Sciortino MT. Antiviral activity exerted by natural products against human viruses. Viruses. 2021;13(5):828.
Hassan MZ, Osman H, Ali MA, Ahsan MJ. Therapeutic potential of coumarins as antiviral agents. Eur J Med Chem. 2016;10(123):236–55.
Mishra S, Pandey A, Manvati S. Coumarin: an emerging antiviral agent. Heliyon. 2020;6(1):e03217.
Barnard DL, Xu ZQ, Stowell VD, Yuan H, Smee DF, Samy R, Sidwell RW, Nielsen MK, Sun L, Cao H, Li A. Coumarins and pyranocoumarins, potential novel pharmacophores for inhibition of measles virus replication. Antivir Chem Chemother. 2002;13(1):39–59.
WHO. WHO Fact Sheet: Diarrheal disease. 2017. At: https://www.who.int/news-room/fact-sheets/detail/diarrheal-disease
Omona S, Malinga GM, Opoke R, Openy G, Opiro R. Prevalence of diarrhea and associated risk factors among children under five years old in Pader District, northern Uganda. BMC Infect Dis. 2020;20:1–9.
Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, Lawn JE, Cousens S, Mathers C, Black RE. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388(10063):3027–35.
Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747–57.
Ssenyonga R, Muwonge R, Twebaze FBN, Mutyabule R. Determinants of acute diarrhea in children aged 0–5 years in Uganda. East Afr Med J. 2009;86(11):513–9.
Aranda-Michel J, Giannella RA. Acute diarrhea: a practical review. Am J Med. 1999;106(6):670–6.
Dryden GW, Song M, McClain C. Polyphenols and gastrointestinal diseases. Curr Opin Gastroenterol. 2006;22(2):165.
Galvez J, Zarzuelo A, Crespo ME, Utrilla MP, Jimenez J, Spiessens C, de Witte P. Antidiarrhoeic activity of Sclerocarya birrea bark extract and its active tannin constituent in rats. Phytother Res. 1991;5(6):276–8.
Galvez J, Crespo ME, Jimenez J, Suarez A, Zarzuelo A. Antidiarrhoeic activity of quercitrin in mice and rats. J Pharm Pharmacol. 1993;45(2):157–9.
Coker E, Katamba A, Kizito S, Eskenazi B, Davis JL. Household air pollution profiles associated with persistent childhood cough in urban Uganda. Environ Int. 2020;1(136): 105471.
Cummings MJ, Bakamutumaho B, Kayiwa J, Byaruhanga T, Owor N, Namagambo B, Wolf A, Wamala JF, Morse SS, Lutwama JJ, O’Donnell MR. Epidemiologic and spatiotemporal characterization of influenza and severe acute respiratory infection in Uganda, 2010–2015. Ann Am Thorac Soc. 2016;13(12):2159–68.
Nshimiyimana Y, Zhou Y. Analysis of risk factors associated with acute respiratory infections among under-five children in Uganda. BMC Public Health. 2022;22(1):1.
Nosalova G, Jurecek L, Hromadkova Z, Kostalova Z, Sadlonova V. Antioxidant activity of herbal polysaccharides and cough reflex. In: Pokorski M, editor. Neurobiology of respiration. Dordrecht: Springer; 2013. p. 51–7.
Kwon KS, Lee JH, So KS, Park BK, Lim H, Choi JS, Kim HP. Aurantio-obtusin, an anthraquinone from Cassiae semen, ameliorates lung inflammatory responses. Phytother Res. 2018;32(8):1537–45.
Xin D, Li H, Zhou S, Zhong H, Pu W. Effects of anthraquinones on immune responses and inflammatory diseases. Molecules. 2022;27(12):3831.
Grace OM, Light ME, Lindsey KL, Mulholland DA, Van Staden J, Jager AK. Antibacterial activity and isolation of active compounds from fruit of the traditional African medicinal tree Kigelia africana. S Afr J Bot. 2002;68(2):220–2.
Van Wyk BE, Yenesew A, Dagne E. Chemotaxonomic survey of anthraquinones and pre-anthraquinones in roots of Aloe species. Biochem Syst Ecol. 1995;23(3):267–75.
Mukundi MJ. Antidiabetic activity and safety of Aloe volkensii, Acacia nilotica, Euclea divinorum, Rhoicissus tridentata, Cynanchum viminale and Urtica dioica in mice. Doctoral dissertation, Kenyatta University. (2015).
Waithaka PN, Gathuru EM, Githaiga BM, Kazungu RZ. Antimicrobial properties of Aloe vera, Aloe volkensii and Aloe secundiflora from Egerton University. Acta Sci Microbiol. 2018;1(5):06–10.
Brozmanova M, Plevkova J, Bartos V, Plank L, Javorka M, Tatar M. The interaction of dietary antioxidant vitamins and oxidative stress on cough reflex in guinea-pigs after long term oxygen therapy. J Physiol Pharmacol. 2006;57:45–54.
Grievink L, Smit HA, Ocké MC, van’t Veer P, Kromhout D. Dietary intake of antioxidant (pro)-vitamins, respiratory symptoms and pulmonary function: the MORGEN study. Thorax. 1998;53(3):166–71.
Harrison RA, Oluoch GO, Ainsworth S, Alsolaiss J, Bolton F, Arias AS, Gutiérrez JM, Rowley P, Kalya S, Ozwara H, Casewell NR. Preclinical antivenom-efficacy testing reveals potentially disturbing deficiencies of snakebite treatment capability in East Africa. PLOS Negl Trop Dis. 2017;11(10):e0005969.
Omara T, Kiwanuka Nakiguli C, Naiyl RA, Atieno Opondo F, Otieno SB, Ndiege ML, Mbabazi I, Nassazi W, Nteziyaremye P, Kagoya S, Okwir A. Medicinal plants used as snake venom antidotes in East African Community: review and assessment of scientific evidences. J Med Chem Sci. 2021;2021(4):107–44.
Chippaux JP. Estimate of the burden of snakebites in sub-Saharan Africa: a meta-analytic approach. Toxicon. 2011;57(4):586–99.
Habib AG, Brown NI. The snakebite problem and antivenom crisis from a health-economic perspective. Toxicon. 2018;1(150):115–23.
Lang HJ, Amito J, Dünser MW, Giera R, Towey R. Intensive-care management of snakebite victims in rural sub-Saharan Africa: an experience from Uganda. South Afr J Crit Care. 2020;36(1):39–45.
Chinyere NH, Milala MA, Zannah H. Effects of aqueous root extract of Annona senegalensis on Bitis arietans venom protease and phospholipase A2 activities. J Pharm Biomed Anal. 2016;6(8):469–73.
Adzu B, Abubakar MS, Izebe KS, Akumka DD, Gamaniel KS. Effect of Annona senegalensis rootbark extracts on Naja nigricotlis nigricotlis venom in rats. J Ethnopharmacol. 2005;96(3):507–13.
Bando DC, Ogu EO, Nuhu I, Suleiman AD, Tubasen HN, Funu K, Jesse PS, Segun RA. Anti-hemorrhagic activity of wild custard apple (Annona senegalensis) ethanolic leaf extract on spitting cobra (Naja negricollis) metalloprotease. ASRJETS. 2020;70(1):77–89.
Amlabu E, Ebinbin A, Amlabu W. Detoxification of Echis ocellatus venom-induced toxicity by Annona senegalensis Pers. J Complement Integr Med. 2014;11(2):93–7.
Larsen BHV, Soelberg J, Jäger AK. COX-1 inhibitory effect of medicinal plants of Ghana. S Afr J Bot. 2015;1(99):129–31.
Barbosa AM, Amaral RO, Teixeira CDFP, Hyslop S, Cogo JC. Pharmacological characterization of mouse hind paw oedema induced by Bothrops insularis (Jararaca ilhoa) snake venom. Toxicon. 2003;42(5):515–23.
Awas E, Omosa LK, Midiwo JO, Ndakala A, Mwanik J. Antioxidant activities of flavonoid aglycones from Kenyan Gardenia ternifolia Schum and Thonn. J Pharm Biol Sci. 2016;11:136–41.
Tan QG, Luo XD. Meliaceous limonoids: chemistry and biological activities. Chem Rev. 2011;111(11):7437–522.
Passos MS, Nogueira TSR, de Aquino AO, Vieira MGC, da Silva TW, Braz-Filho R, Vieira IJC. Limonoids from the genus Trichilia and biological activities. Phytochem Rev. 2021;1:1–32.
Shi YL, Li MF. Biological effects of toosendanin, a triterpenoid extracted from Chinese traditional medicine. Prog Neurobiol. 2007;82(1):1.
Usman A, Thoss V, Nur-e-Alam M. A new flavonoid glycoside from Trichilia emetica. J Med Chem Sci. 2019;2:144–50.
Alam MI, Alam MA, Alam O, Nargotra A, Taneja SC, Koul S. Molecular modeling and snake venom phospholipase A2 inhibition by phenolic compounds: structure–activity relationship. Eur J Med Chem. 2016;23(114):209–19.
Soares AM, Ticli FK, Marcussi S, Lourenco MV, Januario AH, Sampaio SV, Giglio JR, Lomonte B, Pereira PS. Medicinal plants with inhibitory properties against snake venoms. Curr Med Chem. 2005;12(22):2625–41.
Nuwa A, Oola J, Obonyo SO, Feldman M, Karungi S, Kertho E, Odong DS, Kimera I, Magumba G, Beinomugisha G, Chitty A. District-led malaria surveillance and response as an effective way to manage malaria upsurges following the withdrawal of indoor residual spraying: a case study from Nwoya District, northern Uganda. Malar J. 2022;21(1):55.
Olajide OA, Awe SO, Makinde JM. Central nervous system depressant effect of Hoslundia opposita Vahl. Phytother Res. 1999;13(5):425–6.
Risa J, Risa A, Adsersen A, Gauguin B, Stafford GI, van Staden J, Jäger AK. Screening of plants used in southern Africa for epilepsy and convulsions in the GABAA-benzodiazepine receptor assay. J Ethnopharmacol. 2004;93(2–3):177–82.
Boumendjel A, Sotoing Taïwe G, Ngo Bum E, Chabrol T, Beney C, Sinniger V, Haudecoeur R, Marcourt L, Challal S, Ferreira Queiroz E, Souard F. Occurrence of the synthetic analgesic tramadol in an African medicinal plant. Angew Chem Int Ed. 2013;52(45):11780–4.
Boucherle B, Haudecoeur R, Queiroz EF, De Waard M, Wolfender JL, Robins RJ, Boumendjel A. Nauclea latifolia: biological activity and alkaloid phytochemistry of a West African tree. Nat Prod Rep. 2016;33(9):1034–43.
Ashokkumar K. Gloriosa superba (L.): a brief review of its phytochemical properties and pharmacology. Int J Pharmacogn Phytochem Res. 2015;7(6):1190–3.
Kumarapppan C, Jaswanth A, Kumarasunderi K. Antihaemolytic and snake venom neutralizing effect of some Indian medicinal plants. Asian Pac J Trop Med. 2011;4(9):743–7.
Ahamed MBK, Krishna V, Dandin CJ. In vitro antioxidant and in vivo prophylactic effects of two γ-lactones isolated from Grewia tiliaefolia against hepatotoxicity in carbon tetrachloride intoxicated rats. Eur J Pharmacol. 2010;631(1–3):42–52.
Mothogoane MS. Studies on the medicinally important Rhynchosia (Phaseoleae, Fabaceae) species: taxonomy, ethnobotany, phytochemistry and antimicrobial activity. Master's Dissertation. University of Johannesburg. 2019.
Ajao AAN, Alimi AA, Olatunji OA, Balogun FO, Saheed SA. A synopsis of anti-psychotic medicinal plants in Nigeria. Trans R Soc South Africa. 2018;73(1):33–41.
Accorsi S, Fabiani M, Ferrarese N, Iriso R, Lukwiya M, Declich S. The burden of traditional practices, ebino and tea-tea, on child health in Northern Uganda. Soc Sci Med. 2003;57(11):2183–91.
Wandera MN, Kasumba B. “Ebinyo”—the practice of infant oral mutilation in Uganda. Front Public Health. 2017;17(5):167.
Bratcher V. Cultural values of the Lango and Iteso concerning the Shea tree. Master’s Dissertation. School for International Training: Brattleboro, Vermont USA; 2000.
Heinrich M, Edwards S, Moerman DE, Leonti M. Ethnopharmacological field studies: a critical assessment of their conceptual basis and methods. J Ethnopharmacol. 2009;124(1):1–7.
Cunningham AB. Professional ethics and ethnobotanical research. In: Alexiades MN, Sheldon JW, editors. Selected guidelines for ethnobotanical research: a field manual. Bronx: New York Botanical Garden; 1996.
dos Santos AE, Kuster R, Yamamoto KA, Salles TS, Campos R, de Meneses MD, Soares MR, Ferreira D. Quercetin and quercetin 3-O-glycosides from Bauhinia longifolia (Bong.) Steud. show anti-Mayaro virus activity. Parasites Vectors. 2014;7:1–7.
Vandebroek I. Cultural comparisons in ethnobiological research. In: Albuquerque UP, Alves RR, editors. Introduction to ethnobiology. 2016;265–71.
World Flora Online database. Online at: http://worldfloraonline.org/
NEMA. The National Environmental Act, Cap 153. Kampala: Uganda National Environment Management Authority. 1995.
NEMA. National Biodiversity Strategy and Action Plan II (2015–2025). Kampala: Uganda National Environment Management Authority. 2016.
Parliament of Uganda. Traditional and Complementary Medicines Act, 2019. Kampala: Parliament of Uganda. 2020.
International Society of Ethnobiology (ISE) Code of Ethics (2006, with 2008 additions). Online: http://ethnobiology.net/code-of-ethics/
Acknowledgements
The author is profoundly grateful to the study participants, in particular the informants who gave so generously of their time and knowledge—and often of their hospitality—and to the staff of the Makerere University Herbarium for their diligence in specimen identification. The author acknowledges with gratitude the tireless efforts of the project staff of the Cooperative Office for Voluntary Organizations of Uganda (COVOL Uganda), including a team of five interviewers who covered countless kilometers under conditions of uncertainty and outright insecurity, further acknowledging the supportive role played by the student interns from the Makerere University College of Agricultural and Environmental Sciences. The current botanical nomenclature used in this paper was derived by consultation of the World Flora Online database [152]. Special thanks to David Nkuutu, who compiled all herbarium specimens, undertook specimen collection and interviews in Otuke District, and established a collaborative relationship between the project and the Makerere University Herbarium by which the specimens were botanically identified; to Patrick Abwango, Anna Awio, Leonora Okello and Patrick Lomumba, who made initial contact with the study informants, informed of the aims and purposes of the study, and arranged for focus group discussions, and to the interviewers Charles Erongot, Simon Atyang, Lilliane Akot and Paul Ojok. Special thanks as well to Perpetua Apili, who entered all data at the time of its collection, subsequently and arranged follow-up visits by the author within the study area during September and October of 2019.
National biodiversity policy frameworks
The study was conducted with support from a bilateral project implemented by agreement of the Government of Uganda under the 1995 Uganda National Environmental Act, Cap 153, the purpose of which was, among other objectives, to ‘conserve the cultural heritage and use the environment and natural resources of Uganda for the benefit of both present and future generations’ [153]. As such, this study contributes to national policy priorities defined in the more recent Strategic Plan for Biodiversity (2011–2020), and the current national biodiversity strategy and action plan (2015–2025), which among other objectives undertake to facilitate and build capacity for research, monitoring and information management on biodiversity [154]. This study closely aligns include the Traditional and Complementary Medicines Act (2019), which seeks to promote the rational use of traditional and complementary medicine through the provision of scientific evidence [155].
Funding
Funding from 1995 to 2003 was provided by the US Agency for International Development (USAID) under cooperative agreements 623-0124-A-00-5113-00, 617-G-00-98-00001-00 and 617-A-00-98-00007-00; by the European Commission under International Cooperation (INCO) Contract No. IC18-CT98-0261, and by the McKnight Foundation under Grant No.98-798. Additional observations were made, and interviews conducted in a series of follow-up visits in 2019 with funding from the Nelson Marlborough Institute of Technology (NMIT).
Author information
Authors and Affiliations
Contributions
The author conceived and designed the study, assembled an applied research team under the auspices of the Shea Project, for which he negotiated funding, and subsequently undertook data cleaning and analysis, and provided interpretation and the writing up of all results for publication. While the data collection (investigation), project administration and supervision tasks were undertaken by project staff as indicated in the Acknowledgments, the author thus takes full responsibility for conceptualization of the study, for data curation and formal analysis, funding acquisition, methodology, resources, software, validation; visualization, writing of the original draft, and all subsequent review and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The author declares that the present study was performed according to international, national and institutional rules considering animal experiments, clinical studies and biodiversity rights. The author further attests that the data collection and analysis were undertaken in accordance with the International Society of Ethnobiology Code of Ethics [156]. Prior informed consent was obtained from each informant. Participants were informed of the scope and purposes of the study, and were assured that all contributions, made on a voluntary basis, would be kept confidential, and that no commercial use would be made of any of the results of the study.
Consent for publication
Not applicable.
Competing Interests
The author declares that the research was conducted in the absence of any competing interests, financial or non-financial.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Cross-referencing of the data provided in Table 2 with the findings of earlier ethnobotanical studies on medicinal applications, and with pharmacological and compositional studies on bioactivity and compounds of interest.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Masters, E.T. Medicinal plants of the upper Aswa River catchment of northern Uganda - a cultural crossroads. J Ethnobiology Ethnomedicine 19, 48 (2023). https://doi.org/10.1186/s13002-023-00620-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13002-023-00620-5