
Abstract
Preservation of museum objects with inorganic arsenic compounds and contamination of the surroundings has previously been documented. The present study addresses the exposure of museum staff by measuring arsenicals in urine.
After 1 week without exposure, urinary samples were taken before and after handling of preserved skins and analysed by HPLC-ICP-MS for inorganic arsenic, arsenic metabolites and arsenobetaine. The sum of inorganic arsenic and metabolites was an index of exposure. Information about work and seafood intake was obtained by questionnaire.
One out of five subjects had a work-related rise in the exposure index of 18.1 μg As/L to a post-exposure level of 37.1 μg As/L. Four subjects had no certain exposure-related increase in the index.
The study indicates that museum staff may be exposed to arsenic from handling arsenic-preserved objects and supports the use of specified arsenic analysis to avoid interference from organic arsenic.
Similar content being viewed by others


Introduction
Employees may be occupationally exposed to hazardous substances by the contact with materials contaminated in previous, eventually not documented processes. Organic objects in ethnological and natural history museums have been treated with toxic preservatives for centuries. Besides other substances, inorganic arsenic compounds have been applied for this purpose and several studies have revealed an arsenic pollution at these workplaces [1,2,3,4,5].
Arsenicals, particularly inorganic arsenic compounds, have chronic health effects including cancer, skin lesions, neurotoxicity and cardiovascular disorders [6, 7]. The most important routes of exposure to arsenic are inhalation and oral uptake. Additionally, some arsenic compounds including inorganic arsenite (As(III)) compounds have shown a limited dermal penetration ability [8, 9]. Therefore measurements of the arsenic air concentration alone may not sufficiently cover the exposure of the employees. In this case, human biomonitoring could be a better way of obtaining a comprehensive and accurate exposure assessment.
There are three different approaches, all of them based on urinary analyses, for human biomonitoring of exposure to arsenic compounds: (a) determination of total arsenic (inorganic plus organic arsenicals); (b) determination of inorganic arsenicals and the main metabolites monomethylarsonic acid (MMA) and dimethylarsinic acid (DMA) by transference to arsine; (c) separation and quantification of different arsenic species, which almost all consist of arsenite (As(III)), arsenate (As(V)), MMA, DMA and arsenobetaine (AsB) [10]. As(III) and As(V) are specific parameters for the uptake of inorganic arsenic, whereas AsB is the most prominent organic arsenic species mostly derived from marine sources. Inorganic arsenicals are, to a great extent, transformed during human metabolism into the methylated species MMA and DMA [11].
The compound-specific analysis (c) thus differentiates between occupational exposure to inorganic arsenicals and dietary exposure to organic arsenicals [12, 13]. The Commission for the Investigation of Health Hazards of Chemical Compounds in the Work Area of the Deutsche Forschungsgemeinschaft has recently published biological reference values based on 95th percentiles of the parameter in a non-occupationally exposed population of working age (Biologischer Arbeitsstoff-Referenzwert, BAR) for arsenite, arsenate, MMA and DMA in urine, thus supporting the evaluation of arsenic species for the assessment of occupational arsenic exposure [14, 15].
Following measurements of very high arsenic concentrations in a historically preserved bird skin of a kind regularly handled by the staff at the Zoological Museum of the University of Copenhagen, the Department of Occupational and Environmental Medicine, Bispebjerg Hospital was engaged in the risk evaluation. The exposure to arsenic was examined using urinary excretion of inorganic arsenic compounds, their methylated metabolites and AsB, before and after handling animal skins presumed to be preserved by arsenicals. To the best of our knowledge, this is the first study which applies a biomonitoring approach to assess the exposure of the employees to this type of exposure.
Methods and materials
Five employees at the Zoological Museum, involved in handling preserved animal skins were, due to the characteristics of the skins, taken for being potentially exposed to arsenic by the Museums Safety Organization and were included in the study.
After at least 1 week without working with preserved skins, urine specimens were taken before and after a working day’s regular preparation of the exhibit materials without any external intervention. The pre-exposure specimens served as the unexposed control. Both samplings were collected outside the museums premises, after changing clothes and washing hands in order to avoid an external contamination. Information about timing, duration of exposure, personal protection and recent seafood intake were retrieved by a questionnaire.
The urine was analysed for arsenic species at the Institute and Outpatient Clinic of Occupational, Social and Environmental Medicine, University of Erlangen-Nuremberg, Germany by HPLC-ICP-MS according to a procedure proved and published by the Deutsche Forschungsgemeinschaft [16]. Briefly, 100 μL of the urine sample was diluted with the same amount of an aqueous solution containing 1.5% 1 M NH4H2PO4, 0.24% 1 M NaNO3, 0.8% 1 M Na-Acetate and 1% ethanol. 50 μL of the mixture was injected into an Agilent 1200 LC system. Separation was performed on a Hamilton PRP-X100 column (250 mm × 4.1 mm, 10 μm) using a gradient from an aqueous 0.5 mM to a 15 mM NH4H2PO4 solution with a flow rate of 1.2 mL/min. Arsenic was quantified in an ICP-MS system (Agilent 7500) with a MicroMist nebulizer and a collision/reaction cell by detecting the mass element 75. The quantitative estimation was performed by external calibration in the range of 0.1–25 μg/L. Samples with results exceeding the upper calibration range were reanalysed after appropriate dilution. For all species (As(III), As(V), MMA, DMA and AsB) the limit of detection (LOD) was 0.07 μg/L and the limit of quantification (LOQ) was 0.2 μg/L. The arsenic concentration was reported as μg arsenic/L urine. The sum of inorganic arsenic and metabolites (As(III), As(V), MMA and DMA) was used as an index of exposure. The creatinine concentration in the spot urine samples was determined by the Jaffé procedure [17]. Only samples, whose creatinine content ranged between 0.3 and 3.0 g/L, were included in the study. The quality of all analyses was proved/ verified by internal quality control measurements as well as by the successful participation in the proficiency tests of the German External Quality Assessment Scheme [18].
The presence of arsenic in the skins was qualitatively analysed in specimens taken from two skins handled by each of the employees on the day of investigation. These analyses were performed by X-ray fluorescence (XRF) and inductively coupled plasma mass spectrometry (ICP-MS) at the Chemical Division, Danish Emergency Management Agency.
Results and discussion
The five employees handled skins for 2½-3 h without using protective equipment. The presence of arsenic was confirmed by the results of the XRF analyses in all analysed skins, but cannot be quantified.
Post-exposure urinary specimens were taken almost all during the next 2 h after cessation of exposure with the exception of subject 4, who did sampling 5 h after exposure. One of the employees (Subject 1 in Table 1) had eaten seafood the evening before sampling. Another employee (Subject 4) had a daily intake of seafood, including two meals with seafood items between the first and second sample, while none of the remaining three subjects had eaten seafood within 4 days of the sampling.
The results of the urinary analyses are displayed in Table 1, which also includes data from two population-based studies and the German reference value for comparison [19, 20].
The concentration of inorganic arsenic (As(III) and As(V)) was below LOQ in 16 out of 20 analyses and showed no clear increase in the post-exposure concentration in any of the five subjects.
The metabolite MMA was detected in four out of ten samples including both samples of Subject 5 with a post-exposure increase of 6.5 μg/L. Additionally, MMA was found in low concentration in the pre-exposure sample of Subject 2 and the post-exposure sample of Subject 3.
DMA, the major metabolite of inorganic arsenic, was detected in both pre- and post-exposure samples of all five individuals. For Subjects 1 and 5 the DMA concentration increased from pre- to post-exposure samples by 10.6 and 11.3 μg/L urine respectively. The remaining three subjects had DMA concentrations at a lower level and without post-exposure increase.
Arsenobetaine was found in high concentrations in urine from subject 1 and 4, in accordance with seafood intake within 24 h of the two samplings. For three subjects without recent seafood intake, urinary AsB concentration was at a low or moderate level.
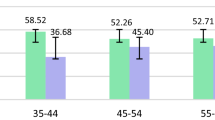
The sum of inorganic arsenic and metabolites (index of exposure) showed an increase in Subject 1 and 5 at 10.6 and 18.1 μg/L, reaching a post-exposure level of 37.1 μg/L for Subject 5, Fig. 1. This subject also showed an increase in the single compounds included in the index, except for As(V), Table 1.

Urinary concentrations of the sum of As(III), As(V), MMA and DMA in urine of five subjects before and after handling of arsenic preserved skins
The result strongly suggests a certain exposure to arsenic for subject 5 by handling preserved skins. After about 3 h of work, the post-exposure value exceeded the US Biological Exposure Index (BEI) for occupational exposure to inorganic arsenic at 35 μg arsenic/L but not the German guidance value at 50 μg arsenic/L [14, 21].
The exposure-related increase in the exposure index of subject 1 at 10.6 μg/L was solely due to an increase in the metabolite DMA. This person had eaten seafood the evening before sampling, which was reflected in a high level of arsenobetaine especially in the first sample. It cannot be excluded that the rise in DMA was caused by seafood intake since some organic arsenicals in seafood may be metabolised to DMA [22,23,24]. For the three remaining subjects no exposure-related increase in the urinary concentrations of arsenicals was found.
Inorganic arsenic and MMA levels were low for all subjects, except for Subject 5, and for most analyses below the LOQ of 0.2 μg/L. These results were at a level comparable to values in European general population studies indicating no or a not detectable additional exposure to inorganic arsenic in these subjects, see Table 1 [19, 20].
DMA is the major metabolite of inorganic arsenic, but has, as mentioned before, also been associated with metabolism of organic arsenic compounds in seafood. This component exceeded the German reference value (BAR) in both samples of Subject 5. The two subjects with recent seafood intake also presented values above the BAR concomitant with inorganic arsenic and a MMA urinary concentration below LOQ. These results are both in concert with the established metabolism of inorganic arsenic into DMA and with experimental findings that certain organic arsenic in seafood may provide or be metabolized to DMA [22,23,24,25].
The results support a moderate uptake of arsenic in one subject who dealt with museum objects definitely containing arsenicals and who wasn’t using protective equipment. No indication of exposure to arsenic from the preserved skins was found for four subjects. An explanation might be that the actually handled skins or some of them contained less arsenic than had been previously found; an explanation which cannot be verified since the arsenic content of the skins was not quantified. The handling of the skins may also have been safer than assumed, but this explanation isn’t in concert with the rapid increase in the exposure index of Subject 5 exceeding the US Biological Exposure Index after few hours of handling skins. Therefore, we recommend a systematic review of the prevention measures considering the reasonable use of respiratory and dermal protection as well as the consequent separation of operation and break areas.
The main limitations of the study are the limited number of individuals involved and the lack of quantitative measurements of arsenic in the handled skins. These two limitations are due to the study being conducted “per occasionem”, i.e. as part of the routine prevention surveillance.
Organic objects in museum collections are a potential source of arsenic exposure, which has received limited attention. The present study indicates that the risk of high exposure to inorganic arsenic from preserved skin is limited. However, the study has limited potential to evaluate the exposure in detail. The clear increase in urinary inorganic arsenic and metabolites detected in the post-exposure urine samples of one of the investigated subjects makes it an issue that ought to be evaluated in depth in further studies. In any case, the study supports specified analyses of arsenicals in order to avoid incorrect exposure measurements from interfering organic arsenicals in seafood.
References
Gribovich A, Lacey S, Franke J, Hinkamp D. Assessment of arsenic surface contamination in a museum anthropology department. J Occup Environ Med. 2013;55:164–7. https://doi.org/10.1097/JOM.0b013e3182717e51
Marte F, Péquignot A, von Endt DW. Arsenic in taxidermy collections: history, detection, and management. Collection Forum. 2006;21:143–50.
Miller PL. Arsenic, old lace, and stuffed owls may be dangerous to your health: environmental concerns for museum personnel. Caduceus. 1991;7:63–70.
Seifert SA, Boyer LV, Odegaard N, Smith DR, Dongoske KE. Arsenic contamination of museum artifacts repatriated to a Native American tribe. JAMA. 2000;283:2658–9. https://doi.org/10.1001/jama.283.20.2653
Smith B, Coulhan B. Potential exposure to arsenic and other highly toxic chemicals when handling museum artifacts. Appl Occup Environ Hyg. 2002;17:741–3. https://doi.org/10.1080/10473220290096078
Albernathy CO, Thomas DJ, Calderon RL. Health effects and risk assessment of arsenic. J Nutr. 2003;133:1536S–8S.
Vahidnia A, Van der Voet GB, De Wolff FA. Arsenic neurotoxicity – a review. Human Environ Toxicol. 2007;26:823–32. https://doi.org/10.1177/0960327107084539
Lowney YW, Ruby MV, Wester RC, Schoof RA, Holm SE, Huy XY, Barbadillo S, Maibach HI. Percutaneous absorption of arsenic from environmental media. Toxicol Ind Health. 2005;21:1–14. https://doi.org/10.1191/0748233705th205oa
Ouypornkochagorn S, Feldmann J. Dermal uptake of arsenic through human depends strongly on its speciation. Environ Sci Technol. 2010;44:3972–8. https://doi.org/10.1021/es903667y
Orloff K, Mistry K, Metcalf S. Biomonitoring for environmental exposures to arsenic. J Toxicol Environ Health B. 2009;12:509–24. https://doi.org/10.1080/10937400903358934
Carter DE, Aposhian HV, Gandolfi AJ. The metabolism of inorganic arsenic oxides, gallium arsenide, and arsine: a toxicochemical review. Toxicol Appl Pharmacol. 2003;93:309–34. https://doi.org/10.1016/j.taap.2003.07.009
Apostoli P, Bartoli D, Alessio L, Buchet JP. Biological monitoring of occupational exposure to inorganic arsenic. Occup Environ Med. 1999;56:825–32. https://doi.org/10.1136/oem.56.12.825
Morton J, Mason H. Speciation of arsenic compounds in urine from occupantional unexposed and exposed persons in the U.K: Using a routine LC-ICP-MS method. J Anal Toxicol. 2006;30:293–301. https://doi.org/10.1093/jat/30.5.293
DFG - Deutsche Forschungsgemeinschaft. List of MAK and BAT Values 2015. Commission for the Investigation of Health Hazards of Chemical Compounds in the Work Area. Report No. 51. Weinheim: Wiley-VCH; 2015. https://doi.org/10.1002/9783527695539.
Weistenhöfer W, Ochsmann E, Göen T, Drexler H, Klotz K. Tracing for arsenic exposure--a differentiation of arsenic compounds is essential for the health assessment. Dtsch Med Wochenschr. 2016;141:59–60. https://doi.org/10.1055/s-0041-104370
Schramel P, Michalke B, Emons H, Göen T, Hartwig A, MAK Commission. Determination of arsenic species in urine by HPLC-ICP-MS. MAK Collect Occup Health Saf. 2018;3 in press
Larsen K. Creatinine assay by a reaction-kinetic principle. Clin Chim Acta. 1972;41:209–17.
Göen T, Schaller KH, Drexler H. External quality assessment of human biomonitoring in the range of environmental exposure levels. Int J Hyg Environ Health. 2012;215:229–32. https://doi.org/10.1016/j.ijheh.2011.08.012
Heitland P, Köster HD. Fast determination of arsenic species and total arsenic in urine by HPLC-ICP-MS: concentration ranges for unexposed German inhabitants and clinical case studies. J Anal Toxicol. 2008;32:308–14. https://doi.org/10.1093/jat/32.4.308
Leese E, Morton J, Tan E, Gardiner PHE, Carolan VA. μLC-ICP-MS determinations of unexposed UK urinary arsenic speciation reference values. J Anal Toxicol. 2014;38:24–30. https://doi.org/10.1093/jat/bkt090
ACGIH - American Conference of Governmental Hygienists. Threshold Limit Values & Biological Exposure Indices. Cincinnati: ACGIH; 2016.
Heinrich-Ramm R, Mindt-Prüfert S, Szadkowski D. Arsenic species excretion after controlled seafood consumption. J Chromatogr B. 2002;778:263–73. https://doi.org/10.1016/S0378-4347(01)00443-1
Molin M, Ulven SM, Dahl L, Telle-Hansen VH, Holck M, Skjegstad G, et al. Humans seem to produce arsenobetaine and dimethylarsinate after a bolus dose of seafood. Environ Res. 2012;112:28–39. https://doi.org/10.1016/j.envres.2011.11.007
Molin M, Ydersbond TA, Ulven SM, Holck M, Dahl L, Sloth JJ, et al. Major and minor arsenic compounds accounting for the total urinary excretion of arsenic following intake of blue mussels (Mytilus Edulis): a controlled human study. Food Chem Toxicol. 2012;50:2462–72. https://doi.org/10.1016/j.fct.2012.04.026
Yang F, Zhang N, Wei C, Liu J, Xie S. Arsenic speciation in organisms from two large shallow freshwater lakes in China. Bull Environ Contam Toxicol. 2017;98:226–233. http://dx.doi.org/. https://doi.org/10.1007/s00128-016-2018-x.
Acknowledgements
The authors acknowledge Michaela Förster and Karin Haji Abbas Zarrabi for proof-reading.
Funding
The exposure evaluation was part of the routine prevention surveillance of the Museum and not funded by any third party.
Availability of data and materials
The datasets analyzed during the current study are available in Table 1.
Author information
Authors and Affiliations
Contributions
AM and PJ analyzed and interpreted the patient data. TG performed the determination of the arsenic species in urine. GF performed the XRF analyses of the exhibits. AM, TG and PJ made major contributions to the writing of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The exposure evaluation was part of the routine prevention surveillance of the Museum. Thus, consent of the Research Ethics Committee was not required. Nevertheless, all participants were informed about the purpose and procedure of the analyses, and participation was voluntary.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Mithander, A., Göen, T., Felding, G. et al. Assessment of museum staff exposure to arsenic while handling contaminated exhibits by urinalysis of arsenic species. J Occup Med Toxicol 12, 26 (2017). https://doi.org/10.1186/s12995-017-0173-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12995-017-0173-6