
Abstract
Background
An Ebola outbreak started in December 2013 in Guinea and spread to Liberia and Sierra Leone in 2014. The health systems in place in the three countries lacked the infrastructure and the preparation to respond to the outbreak quickly and the World Health Organisation (WHO) declared a public health emergency of international concern on August 8 2014.
Objective
The aim of this study was to determine the effects of health systems’ organisation and performance on the West African Ebola outbreak in Guinea, Liberia and Sierra Leone and lessons learned. The WHO health system building blocks were used to evaluate the performance of the health systems in these countries.
Methods
A systematic review of articles published from inception until July 2015 was conducted following the PRISMA guidelines. Electronic databases including Medline, Embase, Global Health, and the Cochrane library were searched for relevant literature. Grey literature was also searched through Google Scholar and Scopus. Articles were exported and selected based on a set of inclusion and exclusion criteria. Data was then extracted into a spreadsheet and a descriptive analysis was performed. Each study was critically appraised using the Crowe Critical Appraisal Tool. The review was supplemented with expert interviews where participants were identified from reference lists and using the snowball method.
Findings
Thirteen articles were included in the study and six experts from different organisations were interviewed. Findings were analysed based on the WHO health system building blocks. Shortage of health workforce had an important effect on the control of Ebola but also suffered the most from the outbreak. This was followed by information and research, medical products and technologies, health financing and leadership and governance. Poor surveillance and lack of proper communication also contributed to the outbreak. Lack of available funds jeopardised payments and purchase of essential resources and medicines. Leadership and governance had least findings but an overarching consensus that they would have helped prompt response, adequate coordination and management of resources.
Conclusion
Ensuring an adequate and efficient health workforce is of the utmost importance to ensure a strong health system and a quick response to new outbreaks. Adequate service delivery results from a collective success of the other blocks. Health financing and its management is crucial to ensure availability of medical products, fund payments to staff and purchase necessary equipment. However, leadership and governance needs to be rigorously explored on their main defects to control the outbreak.
Similar content being viewed by others


Background
Ebola Virus Disease (EVD) was first discovered in 1976, near the Ebola river in the Democratic Republic of Congo (formerly known as Zaire) [1]. More than 25 Ebola outbreaks have been recorded since then, but the West African outbreak which started in 2013 recorded the highest number of deaths compared to all previous outbreaks combined [2]. According to Dr. Margaret Chan, World Health Organisation (WHO) Director General at the time of the outbreak, the 2014–2015 Ebola outbreak was the largest and worst of its kind, jeopardising the fragile health systems and economic stabilities of West Africa [3]. Although it started in December 2013 in a small village in Guinea [4], it was not until August 8 2014 that WHO officially announced Ebola as a Public Health Emergency of International Concern (PHEIC) [5]. As of March 27 2016, total cases were highest in Guinea (3811), Liberia (10,675) and Sierra Leone (14,124), making them the three most affected countries of the region [6].
The failure to contain Ebola has been argued to be a violation of the 2005 International Health Regulations (IHR) which urges member states to detect, assess, report and respond promptly to outbreaks and health emergencies [5]. The magnitude of this outbreak and the speed of Ebola transmission presented a significant threat to international security. The United Nations Security Council therefore unanimously passed a resolution to establish the first ever UN Emergency Health Agency, the United Nations Mission for Emergency Ebola Response (UNMEER) [7]. UNMEER’s responsibilities were transferred to the WHO after it reached its main objective of strengthening surveillance, supporting health workforce and efficiently mobilising resources [8].
The unprecedented spread of Ebola in the region has been explained in many ways and has been linked to factors such as human mobility between the affected countries, behavioural and cultural practices like traditional burials or bush meat consumption, as well as inefficient health systems [9]. Guinea, Liberia, and Sierra Leone have suffered from devastating civil wars, which have had a profound impact on the countries’ health system infrastructure [7]. According to the WHO Health report, they have the lowest human development indexes and among the weakest health system infrastructures in the world [10, 11].
In Guinea, health workforce density (physicians, nurses, midwives, dentists, pharmacists, and psychiatrists) is less than 1.5 per 10,000 population [12], with a total of three hospital beds per 10,000 population [13]. The per capita government expenditure on health is 9 US$ per year [14]. Sierra Leone has a health workforce density of 2.2 per 10,000 population [14] and approximately four hospital beds per 10,000 population [15]. Their per capita government expenditure on health is 12 US$ [14]. In Liberia, the density of the health workforce is less than 3.7 per 10,000 population [14], with around eight hospital beds per 10,000 population [13] and a per capita government expenditure on health of 13 US$ [14]. The public health system infrastructure of the three countries lacked the primary essential elements required to control an outbreak [16], including a strong healthcare workforce [17, 18]. However, the Ebola outbreak also had a significant impact on the already weak health systems and contributed to the decline in the availability of human and physical resources for health.
The aim of this study was to assess existing evidence on the links between the West African Ebola outbreak in Guinea, Liberia and Sierra Leone and the organisation and performance of the countries’ health systems by undertaking a systematic literature review completed by structured expert interviews. Two objectives were developed to achieve this aim: 1) identify effects of the health systems in Guinea, Liberia and Sierra Leone on the management of the Ebola outbreak, and 2) explore the impacts of the Ebola outbreak on the existing health systems in the three countries.
WHO health system building blocks
The WHO states that “a well-functioning health system working in harmony is built on having trained and motivated health workers, a well maintained infrastructure, and a reliable supply of medicines and technologies, backed by adequate funding, strong health plans and evidence-based policies” [19]. These elements have been referred to as the WHO Health System Building Blocks, a framework which will be used in this study to explore the health systems of Guinea, Liberia and Sierra Leone [19–21]. They were selected as a set of internationally agreed health priorities set to create a common understanding of what a health system is and how can it be strengthened [22]. A health system involves all organisations, people and actions whose ultimate priority is to promote, restore or maintain health [22, 23]. The six building blocks are 1) health workforce, 2) health financing, 3) information and research, 4) medical products and technologies, 5) leadership and governance, and 6) service delivery [19–21].
Health workforce include service providers such as physicians, nurses, pharmacists and dentists, health management and support workers [21]. At least 23 physicians, nurses and midwives per 10,000 population are needed for well-functioning primary health care interventions [21]. Their availability should be adequately distributed to offer the best outcomes to the entire population [19–21]. Health workforce should be well qualified, capable, responsive and efficient [19–21].
Strong health systems are adequately financed to provide people with the services they need while ensuring they do not suffer from the financial hardships of the inability to pay for their care [19–21]. Health financing is indispensable to maintain and improve human welfare by ensuring workforce employment, availability of medicines and offering promotion and prevention public health programs [21].
A well-functioning information and research system ensures the effective and timely collection, analysis, distribution, and communication of information [19–21]. Reliable information is needed for policy development, implementation, governance and regulation, training and health education and for the support of the other five building blocks [21]. Information and research is also important for monitoring and evaluation of diseases and programmes and for early warning of health emergencies [21].
Medical products (including essential medicines), vaccines and technologies should be available and accessible to the population [19–21]. They should also be of high quality and efficacy, and scientifically proven to be safe and cost effective [19–21]. Essential medicines are those that satisfy the population’s priority needs [21].
A well led and governed health system is one that has vital policy frameworks in place, together with proper stewardship, established partnerships, a respect of regulations, and provision of incentives [19–21]. Leadership and governance are closely linked to accountability [21].
Good service delivery is achieved when services are delivered in a timely manner, are cost effective, and safe [21]. They should be of high quality and easily accessible to the entire population, independently from their social status or geographical locations [19–21]. Service delivery also includes person-centred services organised around the patient [21].
Methods
A very limited number of studies about the West African Ebola outbreak were expected to be found due to the recent occurrence of the outbreak. The systematic literature review was therefore supplemented by expert interviews [24]. The steps undertaken to conduct this study follow the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidance [25]. The study also used the PRISMA flowchart for study selection [26]. PRISMA was adopted and modified as this study did not assess interventions and included qualitative and observational studies.
Search strategy
Since this study included qualitative and observational data, the SPIDER tool (Sample – Phenomenon of Interest – Design – Evaluation – Research type) was adopted and modified to formulate the research questions and to establish the inclusion and exclusion criteria [27] (Table 1). Search terms (Medical subject headings (MeSH) and Keywords) were developed to identify articles from the following databases: MEDLINE (1946 to July 15th 2015), Embase Classic + Embase (1947 to July 15th 2015) and Global Health (1973 to 2015 Week 27) (Table 2). No publication date criteria was set for the search in order to have a better understanding of the context of the topic. A grey literature search was also performed in the Cochrane library, Scopus, Google Scholar, and various institutional websites (WHO, Médecins Sans Frontières (MSF) and Centers for Disease Prevention and Control (CDC)). Finally, additional studies or grey literature were searched for in the reference lists of all included articles. Selected articles were exported to Endnote X7 to organise, screen and group them. After all articles were exported, duplicates were removed electronically and manually.
Study selection (inclusion and exclusion criteria)
The review only included articles from Guinea, Liberia and Sierra Leone, as they recorded the highest numbers of cases and deaths ever resulting from an Ebola outbreak [28]. Studies on Ebola outbreaks before 2014/2015, Ebola outside these three countries, or any other outbreaks, such as haemorrhagic fevers, were excluded. Articles on randomised control trials, vaccines, treatments, clinical picture, disease manifestations, modelling and epidemiological studies, military interventions and commentaries were excluded. Reports from international organisations such as WHO, CDC, and MSF were included. Only papers published in English were considered as translation services were unavailable during this study.
Studies identified with the search strategy, were screened for eligibility through their titles and abstracts according to the predetermined inclusion and exclusion criteria. Studies that met eligibility criteria were then referred for further full text assessment (Table 3).
Data extraction and analysis
Data was extracted into a spreadsheet created in Microsoft Excel (Tables 4 and 5) based on the research questions formulated using the SPIDER tool. Extracted data included the study setting, author, title, aims of the study, study design and methods, study area and year, health system building block being discussed, key findings, future recommendations, issues raised during the study, and forms of bias. Studies were analysed and assessed using the Crowe Critical Appraisal Tool (CCAT) [29]. The CCAT has 8 main sections with scores ranging from 0 to 5 giving it a total score of 40 per study [29]. The CCAT was used as it was proven to be valid and reliable to all research designs [30].
Expert interviews
Expert interviews are a relatively new field of study, and differ from qualitative semi-structured or in-depth interviews in that they only aim to gather information (as opposed to data). Smith et al. mentioned how interviews with experts in a topic of interest can help complement a study [31], while Otto-Banaszak et al. mentioned that experts are people who are responsible for the development, implementation or control of solutions, strategies or policies and have authorised access to certain populations or information on certain decision processes [32]. They also have access to insights on topics that are very important and where insufficient information is available [32].
Experts were identified from published literature and using the snowball method. They were selected to include senior academics, professionals from international organisations and advisors to the Ministries of Health (MoH) who have worked on health system strengthening during the Ebola outbreak in either of the three countries.
Questions, based on the study objectives, were developed and reviewed by two health systems experts. Interviews lasted 30 min and were recorded on a digital recorder with prior participant approval. After being informed that the recorded interviews would be deleted once the study was over, experts approved the disclosure of their answers. Results were transcribed manually, and then extracted into an extraction table in Microsoft Excel. The table included names and affiliation of the experts, date and duration of the interviews, method and location of the interview, building blocks discussed, and their personal opinions about the outbreak. The expert interviews and answers gathered are considered as information to supplement this study and not as additional data.
Results
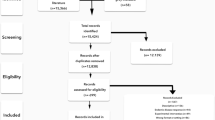
The search strategy yielded a total of 969 articles, out of which 13 articles (four studies and nine reports) were selected for data extraction (Fig. 1) (Table 6). One study scored 55% [33], two scored 40% [34, 35] and one scored 25% on the CCAT quality assessment (Table 7) [36]. Since there was lack of homogeneity of the study designs and no quantitative metrics were found, a meta-analysis was not conducted. Most articles identified, focused on the “medical products and technologies” and “health workforce” WHO building blocks, followed by “information and research”, “health financing”, and “leadership and governance”. No article explored “health system delivery”. Seven experts agreed to take part in the study, out of which one did not send the transcribed version on time for the results to be analysed (Table 8).

PRISMA Database flow diagram: for the systematic review following the Preferred Reporting Items on Systematic Reviews and Meta-Analysis (PRISMA) flow diagram. A total of 969 articles were found from databases search and external sources. 537 duplicates were removed and 432 were left for screening. 390 were excluded based on titles and abstracts leaving 42 articles for full text assessment for eligibility. Thirteen studies were eventually included after 29 were excluded since they did not meet the eligibility criteria. Of the thirteen articles, four were reviews and 9 were reports
Health workforce
Five articles argued that a lack of skilled health workforce was a major obstacle in containing the outbreak [33, 35, 37–39]. Two studies mentioned that the lack of workforce was compounded by the civil wars the three countries were emerging from [33, 35]. Furthermore, some of the available healthcare workers lacked the basic infection prevention and control measures (IPC) knowledge [38, 39]. Two experts also supported these findings [40, 41].
Five articles discussed the impact of the Ebola outbreak on existing health workforce [33, 34, 37, 42, 43]. Ebola created an atmosphere of fear among those involved in the outbreak [33, 34, 37, 42, 43], and Alexander et al. indicated that health staff were stigmatised and rejected by communities [34] while an expert expressed that Ebola had a negative psychological impact on healthcare workers [44].
An expert argued that Ebola claimed more lives among healthcare workers than any other viral haemorrhagic fevers [41]. Another expert said “healthcare workers put their heart and soul in defending the lives of others. We have lost a huge resource there that would take years and years to build back.” [45]. This weakened an already understaffed healthcare system, and added additional burden on existing healthcare workers, that led to increased exhaustion and fatal mistakes [34]. Buseh et al. ratified this finding recognising that nurses became the frontline of the outbreak which threatened their productivity and decreased their efficiency [33]. A WHO report noted that Ebola also threatened the management of human resources for health in these countries which led to a high turnover rate, and staff not knowing who to report to, and not having the appropriate skills to respond to the outbreak [42].
Health financing
Buseh et al. mentioned that a lack of adequate funds invested in health system infrastructure and purchase of supplies contributed to the poor management of the Ebola outbreak [33]. According to an expert, the lack of investment in training healthcare workers, infrastructure, supply chain management, and community engagement was the biggest problem [41].
A WHO report found that as a consequence to the outbreak, the international community and the three countries’ governments allocated additional financial support to medical supplies, human resources, beds, laboratory capacity, contact tracing, safe burials and increased transportation services [46]. One expert explained that this outbreak led to an influx of funding for health systems strengthening, which led governments to establish some IPC projects [45].
Information and research
Four articles stated that shortage of information and research was a considerable problem during the outbreak [33, 37, 42, 43]. Buseh et al. explained that people with Ebola symptoms approached traditional healers, who lacked knowledge on Ebola treatment, resulting in a clash between traditional and modern medicine [33]. Two WHO reports stated there was a severe shortage of surveillance, epidemiological data collection and statistical analysis [37, 42]. Similar views were reflected by experts, explaining that Ebola was not detected early due to a lack of appropriate surveillance methods [41]. All articles stated that health surveys, health system resource tracking, capacity for analysis, synthesis and data validation were lacking [33, 37, 42, 43].
Three CDC reports highlighted the impact of Ebola on the information and research systems of the affected countries. Ebola led to the development of a Community Event Based Surveillance system to help widen and bolster Liberia’s Ebola surveillance and response systems [47]. In Sierra Leone, the Emergency Operations Centre established a toll-free national call centre for Ebola which offers health education messages, flags alerts, and refers people to the appropriate health officials [48]. IPC training protocols, evaluation programs and quality assurance metrics were also developed by Sierra Leone’s MoH [38].
Medical products and technologies
Studies found that lack of medical supplies, resources, personal protective equipment, electricity and IPC led to an increased rate of infections and poor control of Ebola during the outbreak [33, 36–39, 43]. Delays in testing and diagnosis were also reported due to the paucity in specimen transfer, transportation, ambulances and proper coherent communication methods between health officials, villages and urban areas [38, 39, 43]. One expert argued that Sierra Leone started strengthening information collection and surveillance, with the establishment of a new IPC unit and a disaster preparedness unit [45].
Leadership and governance
Four articles emphasised the role of leadership in the outbreak without providing specific information [34, 35, 42, 46]. Two experts mentioned that lack of leadership at the national governmental level was the main reason that led to the poor coordination and absence of a prompt response [45, 49]. One expert explained that Ebola was not publicly discussed by the Liberian President until July 2014 [45].
Only two reports noted the impact of Ebola on leadership and governance in Liberia [46, 50]. A presidential advisory committee on Ebola was established and an Incident Management System (IMS) was introduced to ensure capacities and resources were available [46]. After these two initiatives were developed, health officials saw the benefits and the need for community engagement [46].
Service delivery
No article studied service delivery. However, five experts explained how Ebola impacted the delivery of health services during and after the outbreak [40, 41, 44, 45, 51]. Two experts emphasised that none of the general health services were offered adequately [40, 51]. One expert said: “Ebola’s burden has jeopardised the services being delivered and led to high numbers of comorbidities and fatalities from malaria. People who died from malaria were twice as much as Ebola. Babies died from diarrhoea and pneumonia” [51]. Another expert observed that the shutdown of schools led to an increase in teenage pregnancy and said: “the number of women giving birth in hospitals decreased causing a rise in maternal mortality. Immunization rates fell and other epidemics (as measles) emerged” [41]. Two experts stated that patients were afraid of seeking treatment due to loss of faith in the medical system; people believed that if healthcare workers were not able to cure themselves, they would not be able to help their patients either [44, 45].
Discussion
This systematic review, complemented by expert interviews, explored the nature of the link between the West African Ebola outbreak and health systems in Guinea, Liberia and Sierra Leone.
Health workforce
The results from this study suggest that health workforce had a major effect on the control of the outbreak. In fact, other countries previously affected by Ebola effectively controlled their outbreaks by quickly deploying skilled health staff [9, 16, 52, 53]. Guinea, Liberia and Sierra Leone had not faced outbreaks of such magnitude before and therefore lacked the experience and resources to respond promptly and appropriately [9]. For instance, although Nigeria does not have a highly developed health system, they immediately mobilised their health workforce to prevent Ebola from spreading, for instance including epidemiologists trained in the control of polio [16, 40, 41, 52, 54].
Shortage of healthcare workers is also likely to be due to recent civil wars [16, 55]. Poor working conditions and salaries made healthcare workers flee to other countries when the Ebola outbreak started, which has been seen in other countries during past outbreaks [56, 57]. Surveillance, diagnostic facilities and investigation of cases are important to control an outbreak, but these would be useless without trained health workforce [53]. For this reason, the international community sent foreign staff to support the construction of treatment units, treatment of patients and setting up surveillance systems [5, 7, 53].
Healthcare workers face a particularly high risk of infection and death, as they are in direct contact with symptomatic patients [58–60]. This also creates an indirect impact on other health staff, who are afraid and anxious to face rejection from their families and communities [16, 55, 61, 62]. This led to additional burden, exhaustion, a rapid rate of turnover and poor management of healthcare workers [16, 34, 45, 55, 61–63]. Since nurses were the most involved and connected to the community, it would be useful to train them to disseminate effective messages [33]. Ebola survivors can also be recruited to share their experiences and help control future outbreaks [64].
The WHO Emergency Committee on the 2014 Ebola outbreak in West Africa met throughout the outbreak to share updates and discuss actionable points to control the outbreak in affected countries in accordance with the IHR [65]. Some of the recommendations included that health workforce deployed during an outbreak should be very well trained and qualified. Engagement of community leaders is also very important to reach communities with cultural, religious, or ideological oppositions [65]. Adequate medical care should also be made available for airline personnel and communication should be harmonised in case of symptomatic passengers [65]. Funerals and burials should be conducted by well-trained medical staff to avoid transmission of Ebola [65].
Information and research & medical products and technologies
Healthcare workers in the three affected countries lacked health education and knowledge to control and respond to the outbreak [41, 66]. Nigeria had an Integrated Disease Surveillance and Response programme and the Nigerian Centre for Diseases Prevention and Control, which conducted epidemiological work, data gathering, surveillance and analysis [52]. It also used innovative technologies to help mapping, identification, investigation, management and follow up of cases [67]. Senegal also had an established “Institut Pasteur laboratory” in Dakar to identify cases and respond promptly [68]. Tambo et al. concluded that having an adequate efficient surveillance response system with early warnings and the capability of determining transmission projections is crucial to monitor and control epidemics [69].
Traditional medicine is highly prevalent in West Africa, which has been known to sometimes conflict with modern medicine [33]. Cultural traditions and a lack of healthcare workers meant that patients sought help from traditional healers, who did not always have the appropriate knowledge to provide adequate advice but also protect themselves from infection [9, 52].
All three countries noted an extreme deficiency in medical supplies, efficient transport systems, communication methods and diagnostic tools [33, 63, 64, 70]. Their collective availability is essential to successfully control Ebola according to Raabea et al. [71]. It is vital to have stronger communication and surveillance, isolation, IPC training, testing protocols, Geographical Information Systems (GIS) and modelling to estimate disease projections [38, 39, 42, 72]. Since Ebola has always affected developing countries, there was little incentive in investing in vaccines and drugs development [55, 58, 73]. However, once the outbreak was declared a PHEIC, pharmaceutical companies started working on the development of various new vaccines [64].
In line with the IHR, the Heads of States should activate their emergency management mechanisms and establish an emergency operation centre as soon as an outbreak starts [65]. Information regarding new cases should be efficiently shared, IPC measures should be deployed and surveillance and diagnostic facilities should be set up [65]. An effective contract tracing and case management system is also required together with an adequate supply of PPE and medical commodities to staff in operation [65].
Leadership and governance & health financing
Guinea, Liberia and Sierra Leone did not have the adequate policies or IPC strategies in place before the start of the Ebola outbreak [49]. There was a lack of investment made in the infrastructure, training, and in the purchase of needed supplies and drugs [54, 74, 75]. This made it difficult for health officials to respond promptly.
After the outbreak deprived these countries from staff, governments started working with international organisations and research institutions to strengthen capacity and educate the public [76, 77]. Leadership and governance and health financing have an overarching effect on the rest of the health system building blocks. Despite the international support, investment is needed in the countries’ health systems infrastructure for sustainable development. Funding should include adequate payments, support surveillance, purchase of needed supplies and research development [41, 51].
The Emergency Committee advised heads of states of the affected countries to declare a national emergency and inform the public by sharing information on the situation and the importance of community engagement to control the spread of Ebola [65]. The importance of adequate communication between countries should also be emphasised in order to facilitate the mobilisation of necessary services and workforce to control the outbreak [65]. Leadership and resource allocation in this outbreak is of ultimate importance to meet the IHR. It is also important for leaders to ensure that the healthcare workers receive adequate and timely payment for their services as well as appropriate training and education [65].
Service delivery
Due to a lack of resources, programmes like vaccination campaigns were interrupted, which led to outbreaks of other infectious diseases [16, 40, 54]. Healthcare services for other conditions than Ebola were almost inexistent during the outbreak, which for instance meant pregnant women suffering from high fever were turned down by healthcare workers if they tested negative for Ebola [51, 63]. The stigma attached to healthcare workers also caused patients to avoid seeking treatment for other conditions out of fear [16, 41, 45, 51, 54]. Location of treatment and holding centres was also a problem, with some patients having to travel great distances to reach access any form of care. Improvement in road networks and transport services is important to ensure transportation of patients or specimen on time and improve access to healthcare service delivery. A Short Messaging System has been recommended to map patients with Ebola symptoms to their closest health facilities [36]. In order to comply with IHR, the Emergency Committee advised that treatment centres and diagnostic laboratories should be placed close to places of Ebola transmission and that medical services should also be supplied in a timely manner [65].
Limitations
There was a very limited number of articles available and the included studies had a low CCAT score and did not evenly assess the health systems comprehensively, as per the WHO health system building blocks. No study offered quantitative metrics to assess the health systems and hence quantitative conclusions could not be drawn. Factors which led to the three countries’ weak health systems prior to the outbreak and those that were not linked to health systems were not explored and could have had an impact on managing the outbreak. This study did not conduct a thorough analysis of the political and economic problems in the three West African countries prior to the outbreak or that contributed to the outbreak, and thus a conclusion cannot be drawn on their links to health systems. The study only looked at articles published in English and therefore might have excluded other relevant articles, particularly French articles from Guinea.
Since this study included expert interviews, some limitations were also associated with the ways experts were identified and invited. A problem with the snowball method used is the exclusion of experts who are not within the same network of the experts being interviewed. This leads to selection bias. The number of experts interviewed was small due to their active involvement in the outbreak. Most experts commented on the situation in Sierra Leone which might have led to an under-representation of issues in Guinea and Liberia. Expert interviews are viewed as and should be treated as information and not data and thus, the results cannot be considered generalizable or representative. Experts based in one of three countries might have also had a biased opinion of the situation in their country which they could have generalised to other countries. Despite searching several databases, there still remains the risk of not capturing articles or reports that were not published and were kept for internal communications between organisations.
Lessons learned and recommendations
This study offers several implications for practice and research. An already weak health workforce suffered a lot from this outbreak. Since nurses were the most involved and connected to the community, it would be useful to train them so that they can easily disseminate effective messages, for instance for case reporting [33]. The workforce needs to be fully trained, qualified, on standby and familiar with their roles [9, 33, 49]. Employment of Ebola survivors as staff within community and at hospital levels would be helpful in sharing experiences [64]. Despite the international support, investment is needed in the health systems infrastructure to provide sustainable development of the affected countries. Funding should include adequate payments, more surveillance, purchase of needed supplies and research development [41, 51].
Governments should acknowledge the need to respond quickly to outbreaks, learn from successful examples such as those from Nigeria and Uganda, and ensure community engagement is maintained. The IHR needs to be properly adopted and country leaders should ensure in country coordination, collaboration with others and flexible Trade-Related Aspects of Intellectual Property Rights (TRIPS) agreement are in place in case of outbreaks or public health crisis [42, 46]. It is essential to have stronger communication and surveillance, protocols for isolation and testing, modelling to estimate disease projections, GIS and IPC training as they proved to be very efficient in controlling other outbreaks [38, 39, 42, 72]. Improvement in the road networks and transport services is clearly important to ensure transportation of patient or specimen. Medical supplies such as gloves, disinfectants and PPE are needed on a continuous basis [39, 72].
This study does not offer a comprehensive analysis of the health systems of Guinea, Liberia, and Sierra Leone. Further research needs to be undertaken to conduct an extensive health system analysis of the countries before and after Ebola and to assess each building block using quantitative metrics to determine the exact magnitude of problems and the extent of support needed. More research should also focus on community barriers to care, in order to achieve a more patient centred health system.
Conclusion
Shortage of health workforce was a major challenge in controlling Ebola during the West African outbreak, but was also severely affected by the outbreak. Further research needs to be undertaken to provide a comprehensive analysis of the health systems, including all building blocks, before and after the Ebola outbreak. The importance of community barriers to outbreak control measures also need to be emphasised, to place the patient at the centre of care and ensure a high uptake of interventions by the population.
Ebola is now viewed as an opportunity to rebuild resilient health systems and invest more in capacity building to revive weakened health systems [78]. International attention has also been drawn towards the establishment of an international health systems fund [79] which would help in infrastructure investment. Finally, a strong health system is a result of collective well-functioning building blocks and outbreak control activities should address all of them in order to be successful.
Abbreviations
- CCAT:
-
Crowe Critical Appraisal Tool
- CDC:
-
Centres of Disease Control and Prevention
- EVD:
-
Ebola Virus Disease
- GIS:
-
Geographical Information Systems
- IHR:
-
International Health Regulations
- IMS:
-
Incident Management System
- IPC:
-
Infection Prevention and Control
- MeSH:
-
Medical Subject Headings
- MoH:
-
Ministry of Health
- MSF:
-
Medecins San Frontieres
- PHEIC:
-
Public Health Emergency of International Concern
- PPE:
-
Personal Protective Equipment
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- SPIDER:
-
Sample, Phenomenon of Interest, Design, Evaluation, Research
- UNMEER:
-
United Nations Mission for Emergency Ebola Response
- WHO:
-
World Health Organisation
References
Piot P. No time to lose: a life in pursuit of deadly viruses: WW Norton & Company; 2012
Prevention CfDCa. Outbreaks chronology: Ebola virus disease. https://www.cdc.gov/vhf/ebola/outbreaks/history/chronology.html.
Chan M. Report by the Director-General to the Special Session of the Executive Board on Ebola. World Health Organisation (WHO). 2015
Baize S, Pannetier D, Oestereich L, Rieger T, Koivogui L, Magassouba N, et al. Emergence of Zaire Ebola virus disease in Guinea. N Engl J Med. 2014;371(15):1418–25.
Safari SB, Baratloo A, Rouhipour A, Ghelichkhani P, Yousefifard M. Ebola hemorrhagic fever as a public health emergency of international concern: a review article. Emergency. 2015;3(1):3–7.
WHO. Ebola situation report. World Health Organization: 2016.
Boozary ASF, Farmer PE, Jha AK. The Ebola outbreak, fragile health systems, and quality as a cure. JAMA, J Am Med Assoc. 2014;312(18):1859–60.
Ki-moon B. Statement by Secretary-General Ban Ki-moon on the transition of UN Ebola emergency respons. United Nations, https://www.un.org/sg/en/content/sg/statement/2015-07-31/statement-secretary-general-ban-ki-moon-transition-un-ebola.
Mbonye AKW, Wamala JF, Nanyunja M, Opio A, Makumbi I, Aceng JR. Ebola viral hemorrhagic disease outbreak in West Africa- lessons from Uganda. Afr Health Sci. 2014;14(3):495–501.
Human Development Index. Report on human development 2014. United Nations Development Programme (UNDP) at: http://hdr.undp.org/en/content/table-1-human-development-index-and-its-components.
WHO. The world health report 2000 - Health systems: improving performance. World Health Organization: 2000.
WHO. Health Workforce - African Health Observatory: World Health Organization - Regional Office for Africa; [25 November 2016]. Available from: http://www.aho.afro.who.int/profiles_information/index.php/Guinea:Health_workforce_-_The_Health_System#Inventaire_et_r.C3.A9partition_des_ressources_humaines_en_sant.C3.A9.
WHO. World health statistics 2014 Report. Global Health Observatory (GHO) data: 2014.
WHO. World health statistics 2015 Report. Global Health Observatory (GHO) data: 2015.
The World Factbook - Hospital bed density [Internet]. Available from: https://www.cia.gov/library/publications/the-world-factbook/fields/2227.html.
Bellizzi S. The current Ebola outbreak: old and new contexts. J Infect Dev Ctries. 2014;8(11):1378–80.
Global Health Observatory Data Repository, absolute numbers, data by country. [Internet]. World Health Organization. Available from: http://apps.who.int/gho/data/node.main.A1443?lang=e
Center for Strategic and International Studies. The road to recovery: Rebuilding Liberia’s health system. http://csis.org/files/publication/120822_Downie_RoadtoRecovery_web.pdf
WHO. Health systems: World Health Organization. Available from: http://www.who.int/healthsystems/about/en/
WHO. The WHO Health Systems Framework: World Health Organization. Available from: http://www.wpro.who.int/health_services/health_systems_framework/en/.
WHO. Monitoring the building blocks of health systems: a handbook of indicators and their measurement strategies. World Health Organization Library Cataloguing-in-Publication Data. 2010
WHO. Everybody’s business - strengthening health systems to improve health outcomes : WHO’s framework for action. Geneva: World Health Organization; 2007. p. 44.
WHO. Health Systems Strengthening Glossary. Available from:http://www.who.int/healthsystems/hss_glossary/en/index5.html.
Meuser M, Nagel U. Expertinneninterviews; vielfach erprobt, wenig bedacht. Ein Beitrag zur qualitativen Methodendiskussion. In: Garz D, Kraimer K, editors. Qualitativ-empirische, Sozialforschung, Konzepte, Methoden, Analysen. Opladen: Westdeutscher Verlag; 1991.
Moher D, Liberati A, Tetzlaff J, Altman D, Group tP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9.
Liberati A, Altman D, Tetzlaff J, Mulrow C, Getzsche P, Ioannidis J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151(4):W-65–94.
Cooke A, Smith D, Booth A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis. SAGE Journals. 2012;22(10):1435–43.
Centers for Disease Control and Prevention C. 2014 Ebola Outbreak in West Africa - Case Counts. CDC - Ebola (Ebola Virus Disease) - 2014 West Africa Outbreak. 2015; https://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-counts.html
Crowe M, Sheppard L. A review of critical appraisal toold show they lack rigor: alternative tool structure is proposed. J Clin Epidemiol. 2011;64(1):79–89.
Crowe M, Sheppard L. A general critical appraisal tool: an evaluation of construct validity. Int J Nurs Stud. 2011;48(12):1505–16.
Smith V, Devane D, Begley C, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol. 2011;11:15.
Otto-Banaszak I, Matczak P, Wesseler J, Wechsung F. Different perceptions of adaptation to climate change: a mental model approach applied to the evidence from expert interviews. Springerlink. 2011;11:217–28.
Buseh AGS, Stevens PE, Bromberg M, Kelber ST. The Ebola epidemic in West Africa: challenges, opportunities, and policy priority areas. Nurs Outlook. 2015;63(1):30–40.
Alexander KA, Sanderson CE, Marathe M, Lewis BL, Rivers CM, Shaman J, Drake JM, Lofgren E, Dato VM, Eisenberg MC, Eubank S. What factors might have led to the emergence of Ebola in West Africa?. PLoS Negl Trop Dis. 2015;9(6):e0003652.
Gostin LOF, Friedman EA. A retrospective and prospective analysis of the west African Ebola virus disease epidemic: robust national health systems at the foundation and an empowered WHO at the apex. Lancet. 2015;385(9980):1902–9.
Trad MA, Jurdak R, Rana R. Guiding Ebola patients to suitable health facilities: an SMS-based approach. F1000Research. 2015;4:43.
WHO. Ebola virus disease (EVD) in West Africa: an extraordinary epidemic. Wkly Epidemiol Rec. 2015;90(10):89–96.
Pathmanathan IOC, O’Connor KA, Adams ML, Rao CY, Kilmarx PH, Park BJ, Mermin J, Kargbo B, Wurie AH, Clarke KR, Centers for Disease Control Prevention. Rapid assessment of Ebola infection prevention and control needs–six districts, Sierra Leone, October 2014. MMWR Morb Mortal Wkly Rep. 2014;63(49):1172–4.
Summers AN, Nyenswah TG, Montgomery JM, Neatherlin J, Tappero JW, T N, M F, M M, Centers for Disease Control Prevention. Challenges in responding to the ebola epidemic - four rural counties, Liberia, August-November 2014. MMWR Morb Mortal Wkly Rep. 2014;63(50):1202–4
Heymann D. The link between the 2015/2015 Ebola outbreak and health systems in Guinea., Liberia and Sierra Leone. In: Shoman H, editor. August 12th 2015.
McKay G. The link between the 2015/2015 Ebola outbreak and health systems in Guinea., Liberia and Sierra Leone. In: Shoman H, editor. August 12th 2015.
WHO. Report of the Ebola interim assessment panel. World Health Organization: 2015.
Forrester JD, Pillai SK, Beer KD, Neatherlin J, Massaquoi M, Nyenswah TG, Montgomery JM, De Cock K, Centers for Disease Control and Prevention. Assessment of ebola virus disease, health care infrastructure, and preparedness - four counties, Southeastern Liberia, August 2014. MMWR Morb Mortal Wkly Rep. 2014;63(40):891–3.
Lewis C. The link between the 2014/2015 Ebola outbreak and health systems in Guinea, Liberia and Sierra Leone. Shoman H, editor. 28th August 2015.
Polich E. The link between the 2015/2015 Ebola outbreak and health systems in Guinea, Liberia and Sierra Leone. Shoman H, editor. August 12th 2015.
WHO. How Liberia reached zero cases of Ebola virus disease. Wkly Epidemiol Rec. 2015;90(21):259–60.
Crowe SH, Hertz D, Maenner M, Ratnayake R, Baker P, Lash RR, Klena J, Lee-Kwan SH, Williams C, Jonnie GT, Gorina Y, Anderson A, Saffa G, Carr D, Tuma J, Miller L, Turay A, Belay E, Centers for Disease Control Prevention. A plan for community event-based surveillance to reduce Ebola transmission - Sierra Leone, 2014–2015. MMWR Morb Mortal Wkly Rep. 2015;64(3):70–3.
Miller LAS, Stanger E, Senesi RG, DeLuca N, Dietz P, Hausman L, Kilmarx PH, Mermin J, Centers for Disease Control Prevention. Use of a nationwide call center for Ebola response and monitoring during a 3-day house-to-house campaign - Sierra Leone, September 2014. MMWR Morb Mortal Wkly Rep. 2015;64(1):28–9.
Atchison C. The link between the 2014/2015 Ebola outbreak and health systems in Guinea, Liberia and Sierra Leone. Shoman H, editor. 7th August 2015
Pillai SKN, Nyenswah T, Rouse E, Arwady MA, Forrester JD, Hunter JC, Matanock A, Ayscue P, Monroe B, Schafer IJ, Poblano L, Neatherlin J, Montgomery JM, de Cock KM. Developing an incident management system to support Ebola response - Liberia, July-August 2014. Morb Mortal Wkly Rep. 2014;63(41):930–3.
Whitworth J. The link between the 2014/2015 Ebola outbreak and health systems in Guinea, Liberia and Sierra Leone. Shoman H, editor. London School of Hygiene and Tropical Medicine 30th July 2015.
Oleribe OOS, Salako BL, Ka MM, Akpalu A, McConnochie M, Foster M, Taylor-Robinson SD. Ebola virus disease epidemic in West Africa: lessons learned and issues arising from West African countries. Clin Med. 2015;15(1):54–7.
Gao GFF, Feng Y. On the ground in Sierra Leone. Science. 2014;346(6209):666.
Etuk EE. Ebola: a West African perspective. J R Coll Physicians Edinb. 2015;45(1):19–22.
Bausch D. Glimmers of hope on the Ebola front. Bull World Health Organ. 2014;92(10):704–5.
Gulland A. More health staff are needed to contain Ebola outbreak, warns WHO. BMJ. 2014;349:g5485.
De Frey A. Letters in the time of Ebola. Travel Med Infect Dis. 2014;12(5):541–2.
Chiappelli FB, Bakhordarian A, Thames AD, Du AM, Jan AL, Nahcivan M, Nguyen MT, Sama N, Manfrini E, Piva F, Rocha RM, Maida CA. Ebola: translational science considerations. J Transl Med. 2015;13:11.
Aylward BBP, Bawo L, Bertherat E, Bilivogui P, Blake I, Brennan R, Briand S, Chakauya JM, Chitala K, Conteh RM, Cori A, Croisier A, Dangou JM, Diallo B, Donnelly CA, Dye C, Eckmanns T, Ferguson NM, Formenty P, Fuhrer C, Fukuda K, Garske T, Gasasira A, Gbanyan S, Graaff P, Heleze E, Jambai A, Jombart T, Kasolo F, Kadiobo AM, Keita S, Kertesz D, Kone M, Lane C, Markoff J, Massaquoi M, Mills H, Mulba JM, Musa E, Myhre J, Nasidi A, Nilles E, Nouvellet P, Nshimirimana D, Nuttall I, Nyenswah T, Olu O, Pendergast S, Perea W, Polonsky J, Riley S, Ronveaux O, Sakoba K, Krishnan RSG, Senga M, Shuaib F, Van Kerkhove MD, Vaz R, Kannangarage NW, Yoti Z. Ebola virus disease in West Africa - the first 9 months of the epidemic and forward projections. N Engl J Med. 2014;371(16):1481–95.
Barnes SH, Hussain N, Hogan J, Logan V, Wardrope J. The view from the Ebola Treatment Centre, Makeni, central Sierra Leone. Emerg Med J. 2015;32(7):571–3.
Wiwanitkit V. Unprecedented scale Ebola epidemic in Guinea: what we should know. Asian Pacific Journal of Tropical Biomedicine. 2014;4(9):675.
Weyer JG, Grobbelaar A, Blumberg L. Ebola virus disease: history, epidemiology and outbreaks. Curr Infect Dis Rep. 2015;17(5):1–8.
Butler YS. Ebola virus: exposing the inadequacies of public health in Liberia. Mayo Clin Proc. 2014;89(12):1596–8.
Brown CA, Arkell P, Rokadiya S. Ebola virus disease: the ‘Black Swan’ in West Africa. Trop Doct. 2015;45(1):2–5.
WHO. Statement on the 1st meeting of the IHR Emergency Committee on the 2014 Ebola outbreak in West Africa World Health Organization: Media centre; 2014. Available from: http://www.who.int/mediacentre/news/statements/2014/ebola-20140808/en/.
Wiwanitkit VT, Tambo E, Ugwu EC, Ngogang JY, Zhou XN. Are surveillance response systems enough to effectively combat and contain the Ebola outbreak? Infect. 2015;4(1):7.
Tom-Aba DO, Olaleye A, Olayinka AT, Nguku P, Waziri N, Adewuyi P, Adeoye O, Oladele S, Adeseye A, Oguntimehin O, Shuaib F. Innovative technological approach to Ebola virus disease outbreak response in Nigeria using the open data Kit and form Hub technology. PLoS One. 2015;10(6):e0131000.
WHO. Ebola situation in Senegal remains stable. World Health Organization - Media Centre situation assessment 2014.
Tambo E, Ugwu EC, Ngogang JY. Need of surveillance response systems to combat Ebola outbreaks and other emerging infectious diseases in African countries. Infectious Diseases of Poverty. 2014;3:29.
Bosl EDW, Fehling SK, Strecker T, Eickmann M, Diederich U, Otto A, Streubel K, Becker S. Ebola virus disease - handling of personal protective equipment (ppe). [German]. Intensiv- und Notfallbehandlung. 2014;39(4):146–66.
Vanessa NR, Matthias B. Infection control during filoviral hemorrhagic fever outbreaks. Journal of global infectious diseases. 2014;4(1):69–74.
Klenk HD. Lessons to be learned from the ebolavirus outbreak in West Africa. Emerging microbes & infections. 2014;3(8):e61.
Roca AA, Afolabi MO, Saidu Y, Kampmann B. Ebola: a holistic approach is required to achieve effective management and control. J Allergy Clin Immunol. 2015;135(4):856–67.
Das DG, Guerin PJ, Leroy S, Sayeed AA, Abul Faiz M. The largest Ebola outbreak - what have we learned so far. J Med. 2015;16(1):1–4.
Dhama KM, Malik YS, Malik SV, Singh RK. Ebola from emergence to epidemic: the virus and the disease, global preparedness and perspectives. J Infect Dev Ctries. 2015;9(5):441–55.
Gostin LOW, Waxman HA, Foege W. The president’s national security agenda curtailing Ebola, safeguarding the future. JAMA, J Am Med Assoc. 2015;313(1):27–8.
Griffiths P. Ebola in west Africa: the end of the first year. Rev Med Virol. 2015;25(2):69–70.
Kieny MPE, Evans DB, Schmets G, Kadandale S. Health-system resilience: reflections on the Ebola crisis in western Africa. Bull World Health Organ. 2014;92(12):850.
Gostin LO. Ebola: towards an international health systems fund. Lancet. 2014;384(9951):49–51.
Acknowledgements
I would like to thank Dr. Henock Taddese and staff from Imperial College London, School of Public Health for their input. I am also grateful for the support I got from the department of Primary Care and Public Health and Dr. Sondus Hassounah. Following my visit to the WHO Headquarters in Geneva, Switzerland, I would like to extend my appreciation to the Ebola response team and heads of departments (Dr. Edward Kelly and Dr. Najeeb Al Shorbaji) as they offered insights on the situation and they connected me with the people I needed for the interviews I conducted.
Technical advice given from the Imperial College Library staff at St. Mary’s Campus and Charing Cross Campus, has been of great help in using Endnote and the OVID platform. I would also like to thank Professor David Heymann from Chatham House and Public Health England, Professor Jimmy Whitworth from London School of Hygiene & Tropical Medicine, Dr. Christina Atchison from NHS England, Sir Chris Lewis from Department for International Development and Gillian McKay and Erin Polich from GOAL International for their advices and assistance in collecting my data and for being interviewed.
Funding
No financial support was sought in this study.
Availability of data and material
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
Authors’ contributions
HS has designed, gathered, analysed and wrote the manuscript. EK co-supervised the project, helped in the peer review process, the editing of the manuscript and data extraction. SR was the main supervisor who advised on the design of the study and the identification of the expert interview participants. This manuscript started as HS thesis. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
All authors have consented the publication of this manuscript.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Shoman, H., Karafillakis, E. & Rawaf, S. The link between the West African Ebola outbreak and health systems in Guinea, Liberia and Sierra Leone: a systematic review. Global Health 13, 1 (2017). https://doi.org/10.1186/s12992-016-0224-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12992-016-0224-2