
Abstract
Background
The presence of mental distress among students affects their cognitive, emotional, physical, and interpersonal functioning. Besides, it predisposes to substance use problems and finally affects academic performance negatively. Therefore, this study was designed to estimate the magnitude and identify associated factors for the mental distress of students at Wollo University, Dessie, Ethiopia.
Methods
This institution-based cross-sectional survey assessed mental distress among 585 undergraduate students at Wollo University from April 10 to May 10/2019 using a multi-stage stratified sampling technique. Kessler-10 item scale was used to collect data about mental distress. Variables with p-value < 0.25 in bivariate logistic regression were pooled into a multi-variable logistic regression model and p-value < 0.05 in the multi-variable model was considered significant statistically. The strength of the relationship was interpreted using the odds ratio with 95% CI. The model adequacy in multi-variable regression was approved with Hosmer and Lemeshow goodness of fit test.
Results
Among 585 questionnaires distributed, 548 clear and completed questionnaires were included in the analysis with a response rate of 93.7%. The mental distress prevalence in the current study was 106 (19.3%). From this 65 (11.9%), 28 (5.1%), and 13 (2.4%) were found to be mild, moderate and severe mental distress respectively. Never attending a place of worship (AOR = 4.2, 95% CI 1.73, 10.39), family history of mental illness (AOR = 2.1, 95% CI 1.12, 3.95), current cigarette smoking (AOR = 3.2, 95% CI 1.69, 6.20), current alcohol use (AOR = 2.5, 95% CI 1.49, 4.25), and current cannabis use (AOR = 3.4, 95% CI 1.18, 9.57) were the associated factors for mental distress.
Conclusion
One in five students was affected by mental distress. Never attending a place of worship, family history of mental illness, current cigarette smoking, current alcohol use, and current cannabis use were the factors associated with it. Therefore, all stakeholders should be involved in overcoming this public health problem. Besides, clubs should be established in the university and have to play an active role in bringing behavioral change to substance use.
Similar content being viewed by others

Background
Mental distress can be defined as a state of mind with vague manifestations of anxiety, depression as well as ranges of somatic symptoms like headache, backache, and disturbance of vegetative functions such as disturbed sleep [1, 2]. The contribution of mental disorders like mental distress to the burden of diseases and disability is alarmingly increasing globally. The latest reports from World Health Organization (WHO) showed that nearly 33.3% of the disability-adjusted life years in the world is due to psychiatric disorders of different type and of all population in the world, one in four individual is affected by a mental disorder [3]. Though little attention is given, African countries also take the highest share of mental distress and the contribution of mental distress to the burden of disease and disability in Africa has been documented to be 5% and 19%, respectively [4].
University students are at a higher risk of mental distress when compared to the general population [5] or their community counterparts [6,7,8] and the prevalence of mental distress in students varies widely in different countries and study periods. The Worldwide prevalence of mental distress among medical students was documented to be in a range of 25–90% [9, 10]. A study at Fayoum University showed that 62.4%, 64.3%, and 60.8% of students were found to have mental distress, anxiety, and depression, respectively [11]. Many other studies also revealed that mental distress was 39.7% (20.7% mild, 7.8% moderate, and 11.2% severe distress) in Canada [12], 50% in Singapore [13], 70% in Pakistan [14], 19.2% and 16.5% in Australia [8, 15], 41% in Malaysia [16], 52% in India [17] and 26.9% in Nigeria [18], 19.8% in Somaliland, 40.9%, 30% and 39.6% in Ethiopia [19,20,21].
Many factors were identified so far that contribute to a higher prevalence of mental distress in university students [22,23,24,25,26]. A study in France justified that female gender, alcohol abuse, smoking cigarette, and cyber addiction were contributing risks for mental distress [27]. Other studies also showed that a family history of mental illness was an associated factor for mental distress in students in Iraq [10], Pakistan [14], and Ethiopia [19, 28]. Besides, substance-related variables in France [27], Nepal [29] and Somaliland [30], Female gender in United States [26], Iran [10], Sweden [31], Australia [8] and Somaliland [30], poor worship practice in Ethiopia [19, 28] were some of the factors identified to account for mental distress in university students.
Mental distress affects many aspects of a student's life such as problems of interpersonal relationship, cognitive, physical, and emotional dysfunction, and inability to attain and sustain pleasure in life in many ways as well as increased test anxiety and poor-self-efficacy. This, in turn, will have a detrimental impact on the ability of students to study and finally will end in poor academic achievement; lowers student grades [8, 31, 32]. Above all, mental distress in students if not addressed timely will progress to more severe psychiatric disorders. Despite this, there is a poor help-seeking intention for mental distress among university students [33,34,35].
However, little has been done in this area among university students in Ethiopia; even those studies done focused particularly on medical students [20, 36] and it might not be representative of other university students. Moreover, some of the studies are done in the long past and might not be consistent with the changing situation of university students at present. The aim of this study was therefore to assess the prevalence and factors associated with mental distress among students in Wollo University.
Methods and materials
Study design and setting
This institution-based cross-sectional survey was aimed to assess the magnitude of mental distress and identify the factors associated with it among undergraduate students in a regular study at Wollo University from April 10 to May 10/2019. This study was conducted at Wollo University, Dessie, Amhara Regional State, 400 km from the capital city of Ethiopia; Addis Ababa, in the Northeast of Ethiopia. Dessie is a low temperate area and its latitude and longitude location are 11°8′N and 39°38′E, respectively with an elevation between 2470 and 2550 m above sea level [37]. Wollo University, Dessie campus has 5 colleges, 2 schools and a total of 62 departments.
Participants
The number of undergraduate regular students enrolled in 2018/2019 in Dessie campus colleges, schools, and departments of Wollo University is 7248 and it was considered as the source population whereas the study population consisted of all undergraduate regular students from eighteen selected departments at final stage of multi-stage sampling and enrolled in 2018/ 2019 in the selected colleges. All students from selected departments present at the time of data collection were included while those who were absent and with impairment in the visual field were excluded.
The required sample size for this study was calculated using proportion formula for a single population and was found to be 585. The following assumptions were considered in the calculation procedure; Prevalence of mental distress among university students 41% from a previous study in Gondar University [19], the level of significance to be within 5% margin of error and 95% confidence level, correction formula has been used since the number of regular undergraduate students in 2019 at Wollo university (N) was 7248 which is < 10,000, 10% contingency for probable non-response and a design effect of 1.5 has been taken as multiple stages were involved in calculating sample size.
Multi-stage stratified sampling was adopted for this study according to the colleges and year level of the students. In the first stage, we selected randomly three colleges (college of medicine and health sciences, college of law and College of Natural science) using a lottery method. In the second stage, again lottery method was employed to select 18 departments from three colleges selected at first stage and finally, the proportional allocation was used to determine the number of students to be included from each department and study years.
Assessment of mental distress and its independent variables
Data were collected using structured pre-tested and self -administered questionnaires in the English language. The first section is the questionnaire for the assessment of socio-demographic (age, sex, residence, frequency of worship practice, and family history of mental illness) and academic-related variables (department choice, interest to one’s department, year of study, cumulative grade point average, and having a close friend at school) which were developed by investigators by reviewing previously published works.
The next section was the Kessler-10 psychological distress scale which is a measurement scale for mental distress [38]. This scale asses the following 10 elements in the past 4 weeks (About how often did you feel tired out for no good reason? about how often did you feel nervous? about how often did you feel so nervous that nothing could calm you down?, about how often did you feel hopeless?, about how often did you feel restless or fidgety?, about how often did you feel so restless you could not sit still?, about how often did you feel depressed?, about how often did you feel that everything was an effort?, about how often did you feel so sad that nothing could cheer you up? and about how often did you feel worthless?) each element with a five-level response scale ranging from score1 (none of the time) to score 5 (all of the time). Scores of the 10 elements are then summed, providing a minimum total score of 10 and a maximum score of 50.
A score of 10–19 was considered normal, 20–24 likely to have mild distress, 25–29 a moderate distress, and 30–50 was considered as severe distress with an overall score of 20 suggesting mental distress [38]. The internal consistency of the Kessler-10 psychological distress scale in the present study was checked with a reliability assessment and was found to be 0.86. This scale has been utilized in many previous studies in Ethiopia [39,40,41]. The last section consisted of questions for the assessment of substance-related variables (khat, alcohol, cigarette, and cannabis) [42]. Data collectors were trained BSc nurses and two MSc in mental health professionals and the principal investigator were closely monitoring the data collection process. A pre-test has been implemented on 28 regular undergraduate students a week before the main data collection period and the result was not part of the final survey.
Data management methods
After the distributed questionnaires were collected back, the task done was exploring and checking for its completeness as well as data cleaning. Consequently, complete data were entered to epi-info version-7 and analyzed using SPSS version 20 software package. Descriptive statistics were done to illustrate the distribution of socio-demographic, academic and substance use characteristics of the study participants. The association of mental distress with its independent variables was assessed using binary logistic regression. All independent variables with p-value < 0.25 in bivariate logistic regression were pooled into a multi-variate logistic regression model and p-value < 0.05 in the final model was considered statistically significant.
The strength of the relationship between mental distress and its correlates was interpreted using AORs with 95% CI. The model adequacy in final multi-variable regression was approved with Hosmer and Lemeshow goodness of fit test.
Ethical considerations
This research was conducted after obtaining an official ethical clearance from the Ethical institutional review committee of Wollo University. An official letter from Wollo University Psychiatry department was written to the university academic vice president office to get permission for data collection. Finally, a permission letter from the university academic vice president office was received. Purpose and importance of the study were explained to the study participants and written informed consent was obtained from participants before starting the data collection. Confidentiality of the data was assured by keeping anonymous procedures throughout the research work.
Results
Socio-demographic and academic-related characteristics of Wollo university regular undergraduate students
Out of the total 585 questionnaires distributed to students for data collection, 548 were collected back and responded with complete data making the response rate to be 90.9%. The mean (± SD) age of the participant students was 21.4 (± 1.82) years and more than half (62.6%) of the students were above mean age. Nearly half, 291 (53.1%), were males. About 343 (62.6%) of participants have satisfactory results based on the CGPA score. The proportion of students in the first, second, third and fourth year were 33.8%, 26.5%, 31.9, and 8%, respectively. The majority of students, 441 (80.5%), have close friends and 70 (12.8) have a history of mental illness. One hundred twenty-five (22.8%) of participated students joined their department without their choice and 82 (15%) are not interested in their department currently (Table 1).
Substance-related characteristics of Wollo university regular undergraduate students
From all university students participated in current study, 139 (25.4%) have been using alcohol in the past one month, 104 (19%) have been using khat, and 22 (4%) had been entertained in using cannabis (hashish) during the last one month of study period (Table 2).
Prevalence of mental distress among Wollo university regular undergraduate students
Mental distress among students in this study was assessed with Kessler-10 mental distress scale with a score of 20–24, 25–29, and 30–50 indicating mild, moderate, and severe mental distress respectively which means that a score of 20 and above on Kessler-10 mental distress scale indicates mental distress and a score of less than 19 on Kessler-10 was considered as not having mental distress. The prevalence of mental distress among Wollo university undergraduate students in this study was 106 (19.3%) with 95% CI (16.10, 22.80). From this, 65 (11.9%), 28 (5.1%), and 13 (2.4%) of participants were found to have mild, moderate, and severe mental distress, respectively (Fig. 1). The mean value of prevalence of mental distress in this study was 12.94 with a standard deviation (SD) and variance of 8.18 and 66.99, respectively.

Prevalence of mental distress among Wollo university regular undergraduate students
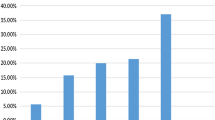
The prevalence of mental distress among males is 19.6% and females 19% but this difference is not statistically supported (AOR = 1.46 95% CI (0.86, 2.47). The highest prevalence of psychological distress was noticed among freshman students (Fig. 2). Considering specific mental distress symptoms about 112 (20.4%), 77 (14.1%), and 72 (13.1%) of students feel that everything was an effort, feel restless/fidgety, and feel depressed, respectively most of the time in the past 4 weeks of data collection (Table 3).

Prevalence of mental distress as the seniority level of students increases
Socio-demographic, academic as well as substance-related factors associated with mental distress among Wollo university students.
Age, department choice, interest to one’s department, living area, cumulative GPA, frequency of attending worship, having close friend, family history of mental illness, using chat, smoking cigarette, alcohol use, and cannabis use within the past one month of data collection were found to have a p-value of < 0.25 in bivariate logistic regression analysis and thus fitted to multi-variable regression.
However, only never attending a place of worship (AOR = 4.2, 95% CI 1.73, 10.39), family history of mental illness (AOR = 2.1,95% CI 1.12, 3.95) current cigarette smoking (AOR = 3.2, 95% CI 1.69, 6.20), current alcohol use (AOR = 2.5,95% CI 1.49, 4.25), and current cannabis use (AOR = 3.4, 95% CI 1.18, 9.57) were found to be associated factors for mental distress with p-value < 0.05 in multi-variable analysis.
Even though, lack of interest to field of study (COR = 1.5, 95% CI 0.89, 2.67), having no close friend (COR = 1.5, 95% CI 0.94, 2.55), and current chat use (COR = 3.4, 95% CI 2.10, 5.43) revealed a higher odds of mental distress on bivariate analysis, this was not significant in multi-variable analysis. The multicollinearity diagnosis was done and Collinearity is not a problem of the current study as Variance inflation factor (VIF) is < 10 for all independent variables included in the multi-variable model (Table 4).
Discussion
To investigators' knowledge, this study is the first to assess the magnitude and associated factors of mental distress among university students in Ethiopia using the Kessler-10 item mental distress assessment scale. This might make it an important overview of magnitude as well as factors associated with mental distress in students in Ethiopia.
Out of 585 university students, 106 (19.3%); 95% CI (16.10, 22.80) had mental distress in this survey. At most 22.8% (upper bound of the 95% CI) of the university students included in this survey had suffered from mental distress within the 4 weeks before data collection. Considering severity, 65 (11.9%), 28 (5.1%), and 13 (2.4%) of study subjects were with mild, moderate, and severe mental distress, respectively.
A lower magnitude of mental distress was obtained in the current study as compared to a study conducted at Canadian university among medical students and residents, in which the prevalence of mental distress was found to be 39.7% (20.7% mild, 7.8% moderate, and 11.2% severe distress [12]. It is also lower than results of earlier studies which found that mental distress among university students was 50% in Singapore [13], 70% in Pakistan [14], 61.3% in Iraq [10] and 41% in Malaysia [16], 52% in India [17] and 26.9% in Nigeria [18] and 40.9%, 30%, and 39.6% in Ethiopia [19,20,21].
On the contrary, this study was higher than a study finding from Michigan; the USA in which only 15.6% of students have emotional distress [43] and 10.8% in Kenya [44]. The difference in prevalence between the current study and the above-mentioned studies might be due to differences in socio-economic, environmental, and behavioral risk factors. Besides, cultural factors in which mental illness is stigmatized by society in low-income countries like Ethiopia may hinder the help-seeking intention and practice of students, thus increasing the prevalence of mental distress. Also, most of the previous studies were conducted among medical students and it might be the stress full nature of medical study due to the high workload which increased the prevalence. Moreover, most of the previous studies used SRQ-20 and the current study used the Kessler-10 distress scale to screen mental distress and sample size variation might account for the difference in prevalence.
However, a result of this survey is consistent with studies in Australian universities (19.2%) [8] and 16.5% [15], 19.8% in Somaliland [30] and 21.6% in Ethiopia [28]. In the current study feeling that “everything was an effort”, feel restless/ fidgety and feel depressed was the mental distress symptoms complained most of the time by students within the past 4 weeks of study. This was more or less consistent with an Australian study at which the symptoms contributing most to mental distress were found to be feeling tired, ‘everything being an effort and being nervous [15].
In the current study, never attending a place of worship was a risk factor for mental distress. No matter how University students follow any type of religion, those students who never attend worship programs were 4.2 times more risky to developmental distress than students who attend worship programs daily. Supportive evidence for this was also found in studies from Adama [28] and Gondar [19]. The possible reason for this would be religion practice builds the highest strength in life and those with good religious practice will have good coping mechanisms from stressful events and factors [45, 46].
A family history of mental illness was also a determinant variable showing a positive association with mental distress in this study. Students who have a family member with mental illness were almost 2 times more likely to have mental distress as compared to those who have no family history of mental illness. These premises are supported by similar findings from studies conducted in Iraq [10], Pakistan [14], Adama [28], and Gondar [19]. Genetic predisposition, and the socio-economic as well as psychological burden caused by the mental illness of family members and care for it, might contribute to such a higher magnitude of mental distress [19].
In this study, current cigarette smoking, current alcohol use as well as current cannabis use were found to have a significant association with mental distress. University students included in current study and who were smoking cigarette, drinking alcohol and using cannabis within the past 4 weeks of study was 3.2, 2.5, and 3.4 times more likely to have a problem of mental distress as compared to those students who did not smoke cigarette, did not drink alcohol and did not use cannabis in the specified time period above respectively. Supportive findings for these were from a study in France [27], Nepal [29], Somaliland [30], and Gondar [19]. This might be due to multi-dimensional effects of substance use like a disturbance in the sleep–wake cycle, dependent producing effects of substances thus causing withdrawal, disturbing interpersonal relationships, increased class absence, and finally leading to poor academic achievement and development of mental distress [47].
Even though, female sex was not found to have a significant association with mental distress in current study, previous studies in the United States [26], Iran [10], Sweden [31], Australia [8], Somaliland [30], and Gondar [19] showed an association between sex (being female) and mental distress in university students. The reason for this could be because, biologically females are predisposed to affective disorders, hormonal factors, and violence from environmental factors [48].
Limitations
We should keep in mind the limitations of this study in analyzing, and utilizing its results. The primary limitation rose from the cross-sectional nature of study making causal inference difficult. So, further follow up studies that can solve this problem should be considered. Next, a lack of a dedicated instrument for the assessment of substance-related variables which are found to be associated factors for mental distress should be emphasized.
Conclusion
One in five undergraduate regular students in Wollo University has been affected by mental distress as per the result of this study and never attending a place of worship, family history of mental illness, current cigarette smoking, current alcohol use as well as current cannabis use were its risk factors. Therefore, all stakeholders should emphasize this problem and strive to overcome it, since otherwise mental distress affects cognitive, emotional as well as interpersonal functioning and academic performance. Besides clubs regarding behavioral and substance-related issues should be established in the university and have to play an active role in bringing behavioral change to substance use.
Availability of data and materials
The datasets used throughout this research process are available from the corresponding author on a reasonable request.
Abbreviations
- AOR:
-
adjusted odds ratio
- CGPA:
-
cumulative grade point average
- OR:
-
odds ratio
- PHQ-9:
-
Patient Health Questionnaire-9
- SD:
-
standard deviation
- SPSS:
-
Statistical Package for Social Science
- SRQ-20:
-
Self-reporting Questionnaire
- USA:
-
United States of America
- WHO:
-
World Health Organization
References
Bao Giang K, Viet Dzung T, Kullgren G, Allebeck P. Prevalence of mental distress and use of health services in a rural district in Vietnam. Global Health Action. 2010;3(1):2025.
Rocha SV, Almeida MMG, Araújo TM, Virtuoso JS. Prevalence of common mental disorders among the residents of urban areas in Feira de Santana Bahia. Rev Brasil Epidemiol. 2010;13(4):630–40.
Demyttenaere K, Bruffaerts R, Posada-Villa J, Gasquet I, Kovess V, Lepine J, et al. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization World Mental Health Surveys. JAMA. 2004;291(21):2581–90.
Amuyunzu-Nyamongo M. The social and cultural aspects of mental health in African societies. Commonwealth Health Partnerships. 2013;2013:59–63.
Svanum S, Zody ZB. Psychopathology and college grades. J Counsel Psychol. 2001;48(1):72.
Cvetkovski S, Reavley NJ, Jorm AF. The prevalence and correlates of psychological distress in Australian tertiary students compared to their community peers. Aust N Z J Psychiatry. 2012;46(5):457–67.
Leahy CM, Peterson RF, Wilson IG, Newbury JW, Tonkin AL, Turnbull D. Distress levels and self-reported treatment rates for medicine, law, psychology and mechanical engineering tertiary students: cross-sectional study. Aust N Z J Psychiatry. 2010;44(7):608–15.
Stallman HM. Psychological distress in university students: a comparison with general population data. Aust Psychol. 2010;45(4):249–57.
Sherina M, Rampal L, Kaneson N. Psychological stress among undergraduate medical students. Med J Malaysia. 2004;59(2):207–11.
Koochaki G, Charkazi A, Hasanzadeh A, Saedani M, Qorbani M, Marjani A. Prevalence of stress among Iranian medical students: a questionnaire survey. East Mediter Health J. 2011;17(7):593–8.
Yusoff MSB, Rahim AFA, Baba AA, Ismail SB, Pa MN. Prevalence and associated factors of stress, anxiety and depression among prospective medical students. Asian J Psychiatry. 2013;6(2):128–33.
Matheson KM, Barrett T, Landine J, McLuckie A, Soh NL, Walter G. Experiences of psychological distress and sources of stress and support during medical training: a survey of medical students. Acad Psychiatry. 2016;40(1):63–8.
Ko S, Kua E, Fones C. Stress and the undergraduates. Singapore Med J. 1999;40(10):627–30.
Khan MS, Mahmood S, Badshah A, Ali SU, Jamal Y. Prevalence of depression, anxiety and their associated factors among medical students in Karachi, Pakistan. J Pak Med Assoc. 2006;56(12):583.
Mulder AM, Cashin A. Health and wellbeing in students with very high psychological distress from a regional Australian university. Adv Mental Health. 2015;13(1):72–83.
MohdSidik S, Rampal L, Kaneson N. Prevalence of emotional disorders among medical students in a Malaysian university. Asia Pacific Fam Med. 2003;2(4):213–7.
Kawa MH, Shafi H. Evaluation of internet addiction and psychological distress among university students. Int J Mod Soc Sci. 2015;4(1):29–41.
Uwadiae E, Osasona S. Psychological distress amongst undergraduate students of a Nigerian University. Cent Afr J Med. 2016;62(5–8):42–8.
Dachew BA, Bisetegn TA, Gebremariam RB. Prevalence of mental distress and associated factors among undergraduate students of University of Gondar, Northwest Ethiopia: a cross-sectional institutional based study. PLoS ONE. 2015;10(3):e0119464.
Melese B, Bayu B, Wondwossen F, Tilahun K, Lema S, Ayehu M, et al. Prevalence of mental distress and associated factors among Hawassa University medical students, Southern Ethiopia: a cross-sectional study. BMC Res Notes. 2016;9(1):485.
Tesfahunegn TB, Gebremariam EH. Mental distress and associated factors among Aksum University students, Ethiopia: a cross-sectional study. BMC Psychiatry. 2019;19(1):71.
Wynaden D, Wichmann H, Murray S. A synopsis of the mental health concerns of university students: results of a text-based online survey from one Australian university. Higher Educ Res Dev. 2013;32(5):846–60.
Bore M, Pittolo C, Kirby D, Dluzewska T, Marlin S. Predictors of psychological distress and well-being in a sample of Australian undergraduate students. Higher Educ Res Dev. 2016;35(5):869–80.
Bayati A, Beigi M, Salehi M. Depression prevalence and related factors in Iranian students. Pak J Biol Sci. 2009;12(20):1371–5.
Niemz K, Griffiths M, Banyard P. Prevalence of pathological Internet use among university students and correlations with self-esteem, the General Health Questionnaire (GHQ), and disinhibition. Cyberpsychol Behav. 2005;8(6):562–70.
Storrie K, Ahern K, Tuckett A. A systematic review: students with mental health problems—a growing problem. Int J Nurs Pract. 2010;16(1):1–6.
Tavolacci MP, Ladner J, Grigioni S, Richard L, Villet H, Dechelotte P. Prevalence and association of perceived stress, substance use and behavioral addictions: a cross-sectional study among university students in France, 2009–2011. BMC public health. 2013;13(1):724.
Dessie Y, Ebrahim J, Awoke T. Mental distress among university students in Ethiopia: a cross sectional survey. Pan Afr Med J. 2013;15(1):95.
Gyawali B, Choulagai BP, Paneru DP, Ahmad M, Leppin A, Kallestrup P. Prevalence and correlates of psychological distress symptoms among patients with substance use disorders in drug rehabilitation centers in urban Nepal: a cross-sectional study. BMC Psychiatry. 2016;16(1):314.
Hersi L, Tesfay K, Gesesew H, Krahl W, Ereg D, Tesfaye M. Mental distress and associated factors among undergraduate students at the University of Hargeisa, Somaliland: a cross-sectional study. Int J Ment Health Syst. 2017;11(1):39.
Dahlin M, Joneborg N, Runeson B. Stress and depression among medical students: a cross-sectional study. Med Educ. 2005;39(6):594–604.
Verger P, Guagliardo V, Gilbert F, Rouillon F, Kovess-Masfety V. Psychiatric disorders in students in six French universities: 12-month prevalence, comorbidity, impairment and help-seeking. Soc Psychiatry Psychiatr Epidemiol. 2010;45(2):189–99.
Alzahem A, VanderMolen H, Alaujan A, Schmidt H, Zamakhshary M. Stress amongst dental students: a systematic review. Eur J Dent Educ. 2011;15(1):8–18.
Galbraith ND, Brown KE. Assessing intervention effectiveness for reducing stress in student nurses: quantitative systematic review. J Adv Nurs. 2011;67(4):709–21.
Tyssen R, Vaglum P, Grønvold NT, Ekeberg O. Factors in medical school that predict postgraduate mental health problems in need of treatment A nationwide and longitudinal study. Med Educ. 2001;35(2):110–20.
Alem A, Araya M, Melaku Z, Wendimagegn D, Abdulahi A. Mental distress in medical students of Addis Ababa University. Ethiop Med J. 2005;43(3):159–66.
Chelkeba L. Antihypertension medication adherence and associated factors at Dessie hospital, north East Ethiopia. Ethiopia. Int J Res Med Sci. 2013;1(3):191–7.
Andrews G, Slade T. Interpreting scores on the Kessler psychological distress scale (K10). Aust N Z J Public Health. 2001;25(6):494–7.
Tadegge AD. The mental health consequences of intimate partner violence against women in Agaro Town, southwest Ethiopia. Trop Doct. 2008;38(4):228–9.
Hanlon C, Medhin G, Selamu M, Breuer E, Worku B, Hailemariam M, et al. Validity of brief screening questionnaires to detect depression in primary care in Ethiopia. J Affect Disord. 2015;186:32–9.
Fekadu A, Medhin G, Selamu M, Hailemariam M, Alem A, Giorgis TW, et al. Population level mental distress in rural Ethiopia. BMC Psychiatry. 2014;14(1):194.
Humeniuk R, Ali R, Babor TF, Farrell M, Formigoni ML, Jittiwutikarn J, et al. Validation of the alcohol, smoking and substance involvement screening test (ASSIST). Addiction. 2008;103(6):1039–47.
Eisenberg D, Gollust SE, Golberstein E, Hefner JL. Prevalence and correlates of depression, anxiety, and suicidality among university students. Am J Orthopsychiatry. 2007;77(4):534–42.
Jenkins R, Njenga F, Okonji M, Kigamwa P, Baraza M, Ayuyo J, et al. Prevalence of common mental disorders in a rural district of Kenya, and socio-demographic risk factors. Int J Environ Res Public Health. 2012;9(5):1810–9.
Nabi N, Yousuf A, Iqbal A. Prevalence of anxiety and depression among doctors working in a Private Hospital in Pakistan. In: Advisory Board, Associate Editors and Psychiatric Computer Interviews: Editorial Board Members ii-iv How Precise, Reliable And Accepted Are They? 69–80 Information for Authors v. 2012:13.
Goebert D, Thompson D, Takeshita J, Beach C, Bryson P, Ephgrave K, et al. Depressive symptoms in medical students and residents: a multischool study. Acad Med. 2009;84(2):236–41.
Ningombam S, Hutin Y, Murhekar MV. Prevalence and pattern of substance use among the higher secondary school students of Imphal, Manipur, India. Natl Med J India. 2011;24(1):11–5.
Pagel MD, Erdly WW, Becker J. Social networks: we get by with (and in spite of) a little help from our friends. J Pers Soc Psychol. 1987;53(4):793.
Acknowledgements
First, we would like to express our gratitude to Wollo University for the technical support provided when needed, and then students who supplied the data for this work genuinely and data collectors are provided with our special gratitude.
Funding
The researchers have no financial support for this research work or write up of the manuscript.
Author information
Authors and Affiliations
Contributions
YZ and MN contributed to the design, conduct, and doing analyses of the research and in the manuscript preparation, and contributed to the review of the manuscript. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research was conducted after obtaining an official ethical clearance from the Ethical institutional review committee of Wollo University. Also, an official letter from Wollo University Psychiatry department was written to the university academic vice president office to get permission for collecting data. Finally, a permission letter from the university academic vice president office was received. The purpose and importance of the study were explained to the study participants and written informed consent was obtained from them. Confidentiality of the data was assured by keeping anonymous procedures throughout the research work.
Consent for publication
Not applicable.
Competing interests
The authors declared that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zenebe, Y., Necho, M. Socio-demographic and substance-related factors associated with mental distress among Wollo university students: institution-based cross-sectional study. Ann Gen Psychiatry 18, 28 (2019). https://doi.org/10.1186/s12991-019-0252-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12991-019-0252-4