
Abstract
Background
Exposure to air pollution is associated with elevated cardiovascular risk. Evidence shows that omega-3 polyunsaturated fatty acids (omega-3 PUFA) may attenuate the adverse cardiovascular effects of exposure to fine particulate matter (PM2.5). However, it is unclear whether habitual dietary intake of omega-3 PUFA protects against the cardiovascular effects of short-term exposure to low-level ambient air pollution in healthy participants. In the present study, sixty-two adults with low or high dietary omega-3 PUFA intake were enrolled. Blood lipids, markers of vascular inflammation, coagulation and fibrinolysis, and heart rate variability (HRV) and repolarization were repeatedly assessed in 5 sessions separated by at least 7 days. This study was carried out in the Research Triangle area of North Carolina, USA between October 2016 and September 2019. Daily PM2.5 and maximum 8-h ozone (O3) concentrations were obtained from nearby air quality monitoring stations. Linear mixed-effects models were used to assess the associations between air pollutant concentrations and cardiovascular responses stratified by the omega-3 intake levels.
Results
The average concentrations of ambient PM2.5 and O3 were well below the U.S. National Ambient Air Quality Standards during the study period. Significant associations between exposure to PM2.5 and changes in total cholesterol, von Willebrand factor (vWF), tissue plasminogen activator, D-dimer, and very-low frequency HRV were observed in the low omega-3 group, but not in the high group. Similarly, O3-associated adverse changes in cardiovascular biomarkers (total cholesterol, high-density lipoprotein, serum amyloid A, soluable intracellular adhesion molecule 1, and vWF) were mainly observed in the low omega-3 group. Lag-time-dependent biphasic changes were observed for some biomarkers.
Conclusions
This study demonstrates associations between short-term exposure to PM2.5 and O3, at concentrations below regulatory standard, and subclinical cardiovascular responses, and that dietary omega-3 PUFA consumption may provide protection against such cardiovascular effects in healthy adults.
Similar content being viewed by others


Background
Ambient air pollution is a major global environmental health problem. Exposure to ambient air pollution [particulate matter (PM) and ozone (O3)] was estimated to be responsible for 4.51 million deaths worldwide in 2019 [1]. Among the health impacts of air pollution, cardiovascular diseases (CVD) garner great concern as ischemic heart disease and stroke are the top two leading causes of death worldwide [2]. Short-term and long-term exposure to fine PM (PM2.5) is linked to an elevated risk for myocardial infarction, stroke, heart failure, and arrhythmia, and potentiates development of chronic cardiometabolic conditions such as diabetes [3].
As oxidative stress and inflammation are important mechanistic pathways mediating air pollution-associated cardiovascular effects, research has been undertaken to investigate potential interventional strategies at an individual level, focusing on these pathways to confer cardiovascular protection. Some omega-3 polyunsaturated fatty acids (PUFA) are dietary fats from marine sources [4]. Mechanistically, marine omega-3 PUFA, eicosapentaenoic acid (EPA, 20:5) and docosahexaenoic acid (DHA, 22:6), can serve as antioxidants and are also substrates for the synthesis of specialized pro-resolving mediators (SPMs) that orchestrate key signaling processes in mediating the resolution of inflammation and a return to homeostasis [5, 6]. Evidence shows that dietary omega-3 PUFA intake in the dose range of 2–4 g/day as fish or fish-oil products is associated with 25–40% lower blood triglyceride and possibly reduced cardiovascular risk among CVD patients [7].
A few studies have reported health benefits of omega-3 PUFA against air pollution exposure. We previously showed that fish oil supplementation (3 g/day for 4 weeks) attenuated adverse cardiac and lipid effects associated with a 2-h exposure to concentrated ambient particulate matter (avg. 278 µg/m3) in healthy middle-aged participants in a controlled exposure study setting [8]. Lin and colleagues reported that fish oil supplementation (2.5 g/day for 2 months) blunted ambient PM2.5 (avg. 38 µg/m3)—induced changes in biomarkers of inflammation, coagulation, and endothelial function among young adults in China [9]. Fish oil supplementation also alleviated systemic oxidative stress caused by ambient O3 and nitrogen dioxide in the same participants [10]. It should be noted that the air pollutant levels in these studies were higher than the U.S. National Ambient Air Quality Standards (NAAQS). However, evidence has shown increased cardiovascular risk in populations exposed to air pollution at concentrations below the established air quality standards, especially in susceptible groups [11, 12]. Thus, knowledge gaps remain on whether increased dietary omega-3 PUFA consumption can attenuate cardiovascular effects caused by ambient air pollution at low levels.
In this panel study, participants were enrolled based on their habitual omega-3 PUFA dietary intake and stratified according to their erythrocyte omega-3 index. We focused on subclinical endpoints of blood lipids, vascular inflammation, coagulation and fibrinolysis, and heart rate variability (HRV) and repolarization. We hypothesized that habitual omega-3 PUFA consumption can alleviate adverse cardiovascular effects induced by short-term exposure to low levels of ambient PM2.5 and O3.
Results
Descriptive statistics
Of the 62 enrolled participants, the majority (56) completed 5 sessions, while 3 completed 4 sessions and another 3 completed 3 sessions. As shown in Table 1, 28 participants were in the low omega-3 group and 34 in the high group. No statistical differences were observed in age, sex, race, smoking history, BMI, or systolic and diastolic blood pressure between the two groups. As expected, the difference in omega-3 index between the low and high groups was statistically significant (4.0% vs. 6.8%, p < 0.001). The description of all cardiovascular biomarkers across all sessions in both low and high omega-3 groups are presented in Additional file 1: Table S1.
During the study period, daily PM2.5 concentrations ranged from 1.8 to 68.0 µg/m3, with a mean of 10.2 µg/m3 and an IQR of 4.7 µg/m3. Average maximum 8-h O3 concentration was 40.8 ppb (range 10–71 ppb, IQR: 17 ppb). Temperature and relative humidity ranged from -8.6 to 31.1 °C and 30 to 100%, respectively. We observed weak or moderate correlations between air pollutants and meteorological measurements (Table 2).
Overview of the regression results
As summarized in Table 3, differential effects of ambient air pollution on cardiovascular biomarkers were observed in the low and high omega-3 groups. Specifically, in the low omega-3 group, significant associations were observed between increased air pollutant concentrations and changes in cardiovascular biomarkers. However, in the high omega-3 group, the associations were either null or in a direction of mitigation of the adverse effects. The detailed results are described below. We only report effect estimates [95% confidence interval (CI)] for markers significantly associated with either PM2.5 or O3 and pinteraction if between-group difference was significant (pinteraction < 0.1).
Effects of blood omega-3 PUFA on the association between PM2.5 exposure and cardiovascular biomarkers
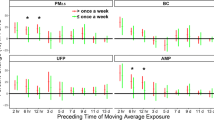
The significant effects of PM2.5 on total cholesterol, vWF, tPA, D-dimer, and VLF were observed in the low omega-3 group, but not in the high group (Table 3, Fig. 1). Specifically, in the low omega-3 group: an IQR increase in the concentration of PM2.5 was associated with decreased total cholesterol at lag1 [-2.4% (-4.3%, -0.4%)], lag2 [-2.2% (-4.0%, -0.4%)], and 5dMA [-3.7% (-6.5%, -0.8%)] (Fig. 1A); PM2.5 was positively associated with vWF at lag0 [6.3% (1.1%, 11.8%), pinteraction = 0.099] while the association shifted to negative at lag3 [-5.8% (-10.0%, -1.5%), pinteraction = 0.07] and lag4 [-4.9% (-9.2%, -0.4%)] (Fig. 1B); PM2.5 was associated with increased tPA at lag3 [6.1% (1.0%, 11.4%)] (Fig. 1C); PM2.5 was associated with increased D-dimer at lag1 [13.1%, (1.0%, 26.8%), pinteraction = 0.09] but the association was negative at lag4 [-11.1% (-20.6%, -0.6%)] (Fig. 1D); PM2.5 was also associated with decreased VLF at lag0 [-20.2% (-34.8%, -2.2%)] (Fig. 1E). These associations were not observed in the high omega-3 group. In the high omega-3 group, positive associations between PM2.5 and P complexity were observed at lag4 [7.7% (2.1%, 13.6%), pinteraction = 0.03] and 5dMA [12.0% (2.5%, 22.5%)] (Fig. 1F). No significant effects of PM2.5 on other biomarkers were observed in either group (Additional file 1: Tables S2-S6).

Influence of omega-3 PUFA on PM2.5 affected cardiovascular biomarkers. Effect estimates (95% CI) in total cholesterol (A), vWF (B), tPA (C), D-dimer (D), VLF (E), and P complexity (F) were corresponded to an IQR increase in PM2.5 concentrations in the low (blue) and high (red) omega-3 groups. * p < 0.05 for significant association within a group. # pinteraction < 0.1 and ## pinteraction < 0.05 for significant differences in the effect estimates between groups
Effects of blood omega-3 PUFA on the association between O3 exposure and cardiovascular biomarkers
Similar to the findings with PM2.5 exposure, significant associations between O3 exposure and the biomarkers were observed in the low omega-3 group with only a few found in the high group (Table 3, Fig. 2). In the low omega-3 group: an IQR increase in the concentration of O3 was significantly associated with increases in total cholesterol at lag0 [3.8% (0.9%, 6.9%), pinteraction = 0.02] but the association was negative at lag2 [-3.5% (-6.2%, -0.8%)], lag3 [-2.9% (-5.6%, -0.2%)], and lag4 [-2.9% (-5.2%, -0.4%)] (Fig. 2A); O3 exposure was significantly associated with decreases in HDL at lag2 [-5.0% (-8.8%, -1.0%), pinteraction = 0.03], lag3 [-4.5% (-8.3%, -0.6%), pinteraction = 0.01], lag4 [-3.6% (-7.1%, -0.1%), pinteraction = 0.05], and 5dMA [-9.2% (-15.4%, -2.4%), pinteraction = 0.01] (Fig. 2C); O3 exposure was significantly associated with increases in SAA at lag1 [27.2% (3.1%, 57.0%)] and 5dMA [47.5% (2.3%, 112.7%)] (Fig. 2D); O3 exposure was also associated with increases in sICAM-1 [4.4% (1.0%, 7.9%), pinteraction = 0.03] and vWF [14.0% (6.9%, 21.5%), pinteraction < 0.01)] at lag0 (Figs. 2E and 2F). In the high omega-3 group, a negative association was observed between O3 and total cholesterol [-2.7% (-5.1%, 0.1%), pinteraction = 0.07] and between O3 and LDL [-5.3% (-8.8%, -1.8%), pinteraction = 0.01] at lag1 (Figs. 2A and 2B). We did not observe significant associations between O3 exposure and other cardiovascular biomarkers in either group (Additional file 1: Table S2-S6).

Influence of omega-3 PUFA on O3 affected cardiovascular biomarkers. Effect estimates (95% CI) in total cholesterol (A), LDL (B), HDL (C), SAA (D), sICAM-1 (E), and vWF (F) were corresponded to an IQR increase in O3 concentrations in the low (blue) and high (red) omega-3 groups. *p < 0.05 for significant association within a group. #pinteraction < 0.1 and ##pinteraction < 0.05 for significant differences in the effect estimates between groups

Schematic showing cardiovascular benefits of dietary omega-3 PUFA against short-term exposure to ambient air pollution. Healthy participants were enrolled in the low and high omega-3 groups based on their dietary omega-3 PUFA intake. Associations between exposure to ambient PM2.5 and O3 and cardiovascular biomarkers in blood and heart rate variability were assessed. Differential impacts of dietary omega-3 PUFA were observed on the cardiovascular biomarkers in response to short-term exposure to low-level ambient air pollution. DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PM2.5, fine particulate matter; SAA, serum amyloid A; sICAM-1, soluble intercellular adhesion molecule 1; tPA, tissue plasminogen activator; VLF, very-low frequency; vWF, von Willebrand factor
All effect estimates remained stable in two pollutant models (Additional file 1: Table S7–S8) and after excluding outliers (Additional file 1: Table S9), indicating that the air pollutants act independently and that the effect estimates are not likely to be driven by outcome outliers.
Discussion
In the present study, we investigated the potential cardioprotective effects of dietary omega-3 PUFA consumption against short-term exposure to low levels of ambient air pollution in healthy adults. As summarized in Fig. 3, we examined a range of cardiovascular biomarkers in response to exposure to ambient PM2.5 and O3, and report protective effects of higher omega-3 PUFA levels in mitigating changes in blood lipids, vascular inflammation, coagulation and fibrinolysis, and HRV.
Although the average concentrations of ambient air pollution during this study period were well below the U.S. NAAQS (24-h PM2.5: 35 μg/m3; 8-h O3: 70 ppb), significant changes in cardiovascular biomarkers were observed in association with these short-term exposures. Similarly, several studies have reported short-term exposure to ambient PM2.5 below the NAAQS levels was associated with cardiovascular effects in susceptible individuals in the U.S. [13,14,15]. In addition, some studies showed that long-term exposure to PM2.5, PM10, or NO2 at concentrations below established air quality standards was significantly associated with increased cardiovascular and respiratory risk among susceptible populations [11, 12]. These findings highlight the need for research on the low-level air pollution-induced health effects and potential interventions that may be effective against such low-level exposures.
Previous efforts have been made to identify interventional approaches to reduce the adverse health effects of air pollution [16]. Mechanistically, air pollution induced-cardiovascular effects are partly driven by oxidative stress and inflammation, suggesting an approach using dietary supplementation with antioxidant and anti-inflammatory agents [17]. Marine omega-3 PUFA are rich in oxidizable carbon–carbon double bonds and are substrates for the synthesis of SPMs. These features of omega-3 PUFA confer antioxidant and anti-inflammatory properties and therefore may blunt the pathophysiology of arteriosclerosis and acute coronary syndrome [4]. A meta-analysis of 13 clinical trials reported a consensus that omega-3 PUFA supplementation lowers the risk for myocardial infarction, coronary heart disease and CVD [18]. Two controlled randomized trials have demonstrated that dietary fish oil supplementation provided cardioprotective effects against high levels of PM2.5 exposure [8, 9]. Our results are in line with these studies in that we show omega-3 PUFA can mitigate adverse cardiovascular effects caused by exposure to air pollution.
Elevated blood lipids, especially triglycerides, total cholesterol and LDL are risks factors for CVD, while increased HDL is considered protective [19]. In the present study, decreased total cholesterol levels were observed in association with PM2.5 in the low omega-3 group. This result is in line with another study conducted in North Carolina showing that short-term exposure to ambient PM2.5 was associated with decreased blood lipid levels in diabetic patients [13]. However, it should be noted that both LDL and HDL, two important lipoproteins for cardiovascular risks, were not affected by PM2.5 regardless of omega-3 PUFA levels. Our previous controlled exposure study also reported that fish oil supplementation did not change the blood HDL and LDL associated with PM2.5 exposure [8], suggesting that dietary supplementary omega-3 PUFA did not significantly alter these lipoproteins. Triglyceride levels in the high omega-3 group showed a decreasing trend (Additional file 1: Table S1) that was not seen in the low omega-3 group, consistent with the use of fish oil supplementation for the treatment of hypertriglyceridemia [20].
Coagulation and fibrinolysis are two highly regulated and inter-related processes in response to tissue injury, ensuring balanced homeostasis of thrombus formation and degradation. vWF plays a major role in blood coagulation by binding to factor VIII and promoting platelet adhesion to injured vasculature [21]. tPA is a serine protease that converts plasminogen to plasmin for fibrin degradation, while D-dimer is a product of the fibrin degradation process [21, 22]. In the present study, elevated vWF was associated with immediate PM2.5 exposure (lag0), but the association shifted to null or negative at delayed lag days in the low omega-3 group, suggesting an acute PM2.5 impact on the increased coagulation activity. Consistently, a meta-analysis showed that a positive association between short-term PM2.5 exposure and vWF was only observed within 3 days of the exposure [23]. An association between PM2.5 exposure and elevated tPA or D-dimer in the low omega-3 group suggests an active fibrinolytic process in response to PM2.5 exposure. Interestingly, none of the significant findings mentioned above were found in the high omega-3 group, suggesting participants with high blood omega-3 PUFA levels were less susceptible to PM2.5 induced coagulation and fibrinolytic activities. Lin and colleagues also reported amelioration of plasma vWF and plasminogen by fish oil supplements in response to PM2.5 exposure in young subjects [9].
HRV is an index of autonomic nervous system control on the heart. A meta-analysis of 29 epidemiological studies showing that exposure to PM2.5 could alter HRV, including LF and HF [24]. Changes in VLF power, strongly correlated with normal sinus beats, have been shown to be associated with the risk for arrhythmic death [25]. In this study, a negative association between PM2.5 and VLF was observed in the low omega-3 group at lag0, implying possible effects on normal sinus beats associated with acute PM2.5 exposure. PM2.5-induced increases in P-wave complexity were observed at lag4 and 5dMA only in the high omega-3 group. As increased P-wave indices are associated with abnormal atrial conduction [26], our results suggest that omega-3 PUFA may affect atrial conduction with short-term exposure to PM2.5, although this finding warrants further investigation. Most of these changes were prominent in the low but not in the high omega-3 group, suggesting that omega-3 PUFA may modulate PM2.5-induced cardiac changes. However, caution is advised when interpreting the HRV results given that these healthy participants were exposed to low levels of ambient air pollution and the transient HRV changes may not be captured by a relatively short period of monitoring in this study.
Similarly, most adverse associations between O3 and cardiovascular biomarkers were in the low omega-3 group while the associations were either null or protective in the high omega-3 group. Specifically, most significant associations between blood lipids or vascular inflammation biomarkers and O3 exposure were observed in the low omega-3 group. The significant changes in total cholesterol and HDL in the low omega-3 group and LDL in the high omega-3 group, suggesting that dietary omega-3 PUFA may maintain a blood lipid profile in favor of reduced cardiac risk in response to O3 exposure. As O3 is considered a strong oxidant that can promote blood lipid oxidation [27], the quenching or antioxidant properties of omega-3 PUFA may mitigate such effects.
SAA is a biomarker of acute inflammation and tissue injury while sICAM-1 and sVCAM-1 participate in leukocyte adhesion to the endothelium and play an important role in all stages of atherosclerosis [28]. Increased SAA, sICAM-1 and sVCAM-1 levels in association with O3 were found in the low omega-3 group, but not in the high group, indicating the protection of omega-3 PUFA against O3-induced vascular inflammation. Data on the modifying effects of omega-3 PUFA on ozone-induced health effects are sparse. A study showed amelioration of fish oil on systemic oxidative stress induced by ambient O3 and NO2 exposure in human subjects [10]. An animal study also found vasoprotective effects and alleviation of cardiac dysfunction of fish oil supplementation against O3 exposure (800 ppb) in rats [29, 30].
It is noteworthy that we observed a lag-time-dependent biphasic change in several biomarkers in the low omega-3 group. Specifically, the positive associations between PM2.5 or O3 and total cholesterol, LDL, sICAM-1, vWF, and D-dimer were mainly observed at lag0 or lag1, but the associations trended null and negative at lag2-4. These observations indicate that the air pollutant-induced adverse effects are acute and normally reversible, which are consistent with current literature [31, 32]. The null and negative associations at delayed lag days suggest that the low-level of air pollution in our study did not have an extended adverse impact on the assessed biomarkers. This could be partly explained by the active defensive responses to limit and resolve the adverse effects in the subclinical biomarkers caused by low-level of air pollution. Omega-3 PUFA is an antioxidant that can readily react with oxidant air pollutants potentially mitigating their interaction with tissue targets. On the other hand, prolonged exposure to air pollution may generate reactive oxidized lipid products that are biologically active. We recently reported that a high omega-3 index protected lung function decrements associated with ozone exposure in the immediate term but potentiated the effect on lagging days [33]. Nevertheless, these changes were mainly observed in the low omega-3 group, implying that an increased susceptibility to adverse impacts of air pollution are in participants who are deficient in omega-3 PUFA.
We stratified participants into low and high groups based on their blood omega-3 index with the cutoff values of < 4% and > 5.5% respectively. Omega-3 indices approximately 4% and 5.5% correlate with relatively high and low risk for coronary heart disease, respectively [34]. Although there is no consensus in clinical practice on optimal omega-3 index values for cardiovascular health, there have been studies supporting the notion that a higher omega-3 index is cardioprotective [34, 35]. The American Heart Association recommends that patients with coronary heart diseases consume 1 g per day of EPA and DHA to lower the CVD risk. The recently approved highly purified prescription form of EPA (Icosapent ethyl) has been shown to significantly reduce cardiovascular risk in patients with hypertriglyceridemia [20], further promoting the use of omega-3 PUFA in CVD. We also reported beneficial modification of dietary omega-3 PUFA on the association between short-term exposure to ambient NO2 and respiratory and cardiovascular outcomes [36]. Taken together, these findings suggest that dietary omega-3 PUFA may confer cardioprotective benefits against adverse health effects of exposure to ambient air pollution in healthy adults even at levels below current air quality standards.
The findings of this study are noteworthy in several respects. First, this observational study was carried out with participants conducting their daily activities, making the findings more generalizable to real-life scenarios. Second, the 24-h dietary recall methodology employed to monitor dietary intake of EPA + DHA for each participant throughout the study indicated that the EPA + DHA intake levels remained relatively stable for both low and high omega-3 groups [37]. Third, this is the first study to report cardiovascular benefits of omega-3 PUFA against exposure to lower-than-NAAQS levels of PM2.5 and O3, indicating its potential as an interventional strategy against health effects of low-level air pollution. Fourth, relatively high omega-3 PUFA levels were achieved by participants through habitual fish and/or fish oil consumption, suggesting long-term cardiovascular benefits of dietary omega-3 PUFA against exposure to air pollution.
There are also a few limitations of this study. This study did not recruit participants who are considered susceptible to air pollution, such as the elderly and those with pre-existing cardiovascular diseases. Nonetheless, we have observed moderating effects of omega-3 PUFA on changes of cardiovascular biomarker associated with ambient air pollutants, and it is likely that these effects would be more prominent if susceptible population were included. This study employed a relatively small sample size and short-term exposure scenario; thus, caution is warranted inferring causal association and long-term implication of the findings. Only the health effects of PM2.5 and O3 were considered in the study while there might be other components of air pollution in play such as secondary organic aerosols. Furthermore, air pollution data were based on central air quality monitoring stations rather than individual exposure metrics such as location, time spent indoor vs. outdoor, and activity level, which could possibly introduce non-differential exposure misclassification. Finally, even though we have restricted dietary and medication usage during the study period, other factors such as lifestyle (exercise, balanced diet, stress, etc.) could be potential confounders.
Conclusions
This observational study demonstrates that habitual dietary omega-3 PUFA may provide benefits in ameliorating the cardiovascular effects associated with short-term exposure to low levels of ambient air pollutants including PM2.5 and O3. These findings suggest that dietary omega-3 PUFA intake may offer a simple and effective interventional approach at an individual level to mitigate the adverse cardiovascular effects of exposure to ambient air pollution.
Methods
Study population and design
The study was carried out in Central North Carolina from October 2016 to September 2019. Healthy participants meeting the following criteria were recruited: 25–55 years old; body mass index (BMI) between 19 and 35; having no history of cardiovascular disease, chronic respiratory disease, cancer, uncontrolled hypertension (≥ 140 systolic, ≥ 90 diastolic), or diabetes; non-smokers for at least 1 year; not taking β-adrenergic receptor blockers, anti-inflammatory drugs, and statins. Participants were recruited from Research Triangle area in close proximity to the U.S. Environmental Protection Agency (U.S.EPA) Human Studies Facility (HSF) in North Carolina, USA.
Eligible participants were further screened and enrolled into low or high omega-3 PUFA groups meeting one of the following criteria: 1) As described previously [38], an inhouse open-ended dietary questionnaire was used to screen participants whose EPA + DHA intake was less than 0.5 g/week (low) or at least 3 g/week (high) for 6 months or longer; 2) Omega-3 index (OmegaQuant, Sioux Falls, SD), a measurement of EPA and DHA in erythrocyte membrane, was employed to screen participants whose omega-3 index was less than 4.0% (low) or at least 5.5% (high).
Each enrolled volunteer visited the Human Studies Facility (HSF) of the U.S.EPA for up to 5 sessions separated by at least 7 days between two sessions. Participants were instructed to keep their diet routine during the study and refrain from using any pain medications for two weeks before each session. Each session consists of two visits on consecutive days. On the first day, participants were outfitted with a Holter monitor and recorded continuously for 30 min. On the second day, venous blood was collected for biomarker measurements and Holter monitoring was recorded for 30 min. Written informed consent was given by all participants prior to enrollment. The study was approved by the Institutional Review Board of the University of North Carolina at Chapel Hill and the U.S.EPA and registered at ClinicalTrials.gov (NCT02921048).
Exposure assessment
Hourly concentrations of ambient PM2.5 and O3 were obtained from a central air quality monitoring station (Millbrook) approximately 44 km (27 miles) from the HSF. Twenty four-hour average concentrations of PM2.5 were calculated from hourly pollutant data averaged between 9 and 8 AM, with a valid day defined as having at least 18 hourly measurements over the 24-h period. Daily maximum 8-h O3 concentrations were defined as the highest 8-h moving average concentrations between 9 and 8 AM. For missing data, an alternative central monitoring station (Durham Armory) approximately 18 km (11 miles) from the HSF was employed. Concentrations were assigned to each visit session (the day of blood sample collection is defined as lag0), as well as to 4 days prior (lag1–lag4), and the 5-day moving average (5dMA). Twenty four-hour averages of NO2 concentration, air temperature and relative humidity were collected from the same monitoring station.
Venous blood samples
A portion of each blood sample was sent to a commercial lab (LabCorp, Burlington, NC) for quantification of blood lipids. The remainders of the blood samples were separated for plasma and stored at -80 ℃ prior to biomarker analysis. Commercially available multi-array plates were used to quantify levels of von Willebrand factor (vWF), tissue plasminogen activator (tPA), and D-dimer (MesoScale, Rockville, MD). In addition, vascular inflammation biomarkers including soluable intercellular adhesion molecule 1 (sICAM-1), soluable vascular cell adhesion molecule 1 (sVCAM-1), and serum amyloid A (SAA) were measured using a multiplex kit from MesoScale Diagnostics (Gaithersburg, MD). All experiments were performed per manufacturers’ instructions.
Holter monitoring
As described previously [39], a Holter monitor was placed on the participants on both days of each session. The participants reclined in a dark room for 30 min and Holter were recorded using a H12 + 12-Lead ECG Recorder (Mortara, Milwaukee, WI). HRV and repolarization parameters were measured during the last 5 min of Holter recording. Time-domain measurements [standard deviation of normal-to-normal (SDNN), root-mean square of successive differences (rMSSD)] and frequency-domain measurements [very-low frequency (VLF), normalized low frequency (LFn), normalized high frequency (HFn), and low-to-high frequency power (LF/HF)] were measured. Cardiac repolarization was assessed by measuring the QT interval and corrected by heart rate (QTc). T wave complexity was measured in each beat by principal component analysis based on all 12 leads and averaged. QRS complexity and P wave complexity was calculated with the Mortara software.
Statistical analysis
The data analysis was performed using R (version 3.6.2) with the “gamm4” package. To improve normality in the residuals, we log-transformed all dependent variables except for LFn and HFn. Generalized linear mixed models with random subject effects were employed to analyze the associations between exposure to air pollutants and cardiovascular biomarkers. Based on the repeated measurements in the same subjects, this approach assessed the within-subject variabilities in biomarkers under different exposure levels. The statistical model was adjusted for age, sex, race, BMI, long-term and seasonal trends, day of the week, temperature, and relative humidity. The long-term and seasonal trends were controlled for by a penalized spline of time with eight degrees of freedom (df) per year. Temperature (lag0-1 for high temperatures and lag 0–4 for low temperatures) and relative humidity (lag0-4) were incorporated as penalized splines with the df selected by the Generalized Cross Validation criterion. Linear terms of PM2.5 and O3 were included in the model separately to assess the immediate (lag0), delayed (lag1 to lag4), or cumulative (5-day moving average, 5dMA) effects. A product term of omega-3 groups and air pollutant concentrations was added to assess between-group differences. The results were interpreted as percent change from the mean of the measured outcome per interquartile range (IQR) increase of exposure. We also conducted two sensitivity analyses to test the robustness of the results. First, we restricted analyses to outcome data without outliers (defined as those lower than 1st quartile − 3 \(\times\) IQR and those higher than 3rd quartile + 3 \(\times\) IQR). Second, we adjusted the analyses using a 2-pollutant model; for example, we adjusted effect estimates of biomarkers per IQR increase in PM2.5 with either O3 or NO2 concentrations at the same lag. Statistical significance was set at a two-sided p < 0.05 for the air pollution effects and a two-sided p < 0.1 for the interaction with the two groups.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available in the EPA ScienceHub repository.
Abbreviations
- CI:
-
Confidence interval
- DHA:
-
Docosahexaenoic acid
- EPA:
-
Eicosapentaenoic acid
- HDL:
-
High-density lipoproteins
- HFn:
-
Normalized high frequency
- HRV:
-
Heart rate variability
- IQR:
-
Interquartile range
- LDL:
-
Low-density lipoproteins
- LFn:
-
Normalized low frequency
- LF/HF:
-
Low to high frequency power
- PM2.5 :
-
Fine particulate matter
- PUFA:
-
Polyunsaturated fatty acids
- QTc:
-
Q-T corrected
- RMSSD:
-
Root mean square of successive differences
- SAA:
-
Serum amyloid A
- SD:
-
Standard deviation
- SDNN:
-
Standard deviation standard deviation of normal-to-normal
- sICAM-1:
-
Soluble intercellular adhesion molecule 1
- SPM:
-
Specialized pro-resolving mediator
- sVCAM-1:
-
Soluble vascular cell adhesion molecule 1
- tPA:
-
Tissue plasminogen activator
- VLF:
-
Very-low frequency
- vWF:
-
Von Willebrand factor
References
Collaborators GBDRF. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1223–49. https://doi.org/10.1016/S0140-6736(20)30752-2.
WHO: The top 10 causes of death. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (2020). Accessed Janurary 25th 2021.
Brook RD, Newby DE, Rajagopalan S. The global threat of outdoor ambient air pollution to cardiovascular health: time for intervention. JAMA Cardiol. 2017;2(4):353–4. https://doi.org/10.1001/jamacardio.2017.0032.
Swanson D, Block R, Mousa SA. Omega-3 fatty acids EPA and DHA: health benefits throughout life. Adv Nutr. 2012;3(1):1–7. https://doi.org/10.3945/an.111.000893.
Serhan CN, Levy BD. Resolvins in inflammation: emergence of the pro-resolving superfamily of mediators. J Clin Invest. 2018;128(7):2657–69. https://doi.org/10.1172/JCI97943.
Souza PR, Marques RM, Gomez EA, Colas RA, Matteis RD, Zak A, et al. Enriched marine oil supplements increase peripheral blood specialized pro-resolving mediators concentrations and reprogram host immune responses. Circ Res. 2020;126(1):75–90. https://doi.org/10.1161/CIRCRESAHA.119.315506.
Weinberg RL, Brook RD, Rubenfire M, Eagle KA. Cardiovascular impact of nutritional supplementation with omega-3 fatty acids. J Am Coll Cardiol. 2021;77(5):593–608. https://doi.org/10.1016/j.jacc.2020.11.060.
Tong H, Rappold AG, Diaz-Sanchez D, Steck SE, Berntsen J, Cascio WE, et al. Omega-3 fatty acid supplementation appears to attenuate particulate air pollution-induced cardiac effects and lipid changes in healthy middle-aged adults. Environ Health Perspect. 2012;120(7):952–7. https://doi.org/10.1289/ehp.1104472.
Lin Z, Chen R, Jiang Y, Xia Y, Niu Y, Wang C, et al. Cardiovascular benefits of fish-oil supplementation against fine particulate air pollution in China. J Am Coll Cardiol. 2019;73(16):2076–85. https://doi.org/10.1016/j.jacc.2018.12.093.
Jiang Y, Wang C, Lin Z, Niu Y, Xia Y, Liu C, et al. Alleviated systemic oxidative stress effects of combined atmospheric oxidant capacity by fish oil supplementation: a randomized, double-blinded, placebo-controlled trial. Ecotoxicol Environ Saf. 2019;184: 109598. https://doi.org/10.1016/j.ecoenv.2019.109598.
McGuinn LA, Schneider A, McGarrah RW, Ward-Caviness C, Neas LM, Di Q, et al. Association of long-term PM2.5 exposure with traditional and novel lipid measures related to cardiovascular disease risk. Environ Int. 2019;122:193–200. https://doi.org/10.1016/j.envint.2018.11.001.
Zhao Q, Kress S, Markevych I, Berdel D, von Berg A, Gappa M, et al. Long-term air pollution exposure under EU limits and adolescents’ lung function: modifying effect of abnormal weight in GINIplus/LISA birth cohorts. Chest. 2021. https://doi.org/10.1016/j.chest.2021.02.007.
Schneider A, Neas LM, Graff DW, Herbst MC, Cascio WE, Schmitt MT, et al. Association of cardiac and vascular changes with ambient PM2.5 in diabetic individuals. Part Fibre Toxicol. 2010;7:14. https://doi.org/10.1186/1743-8977-7-14.
Schneider A, Alexis NE, Diaz-Sanchez D, Neas LM, Harder S, Herbst MC, et al. Ambient PM2.5 exposure up-regulates the expression of costimulatory receptors on circulating monocytes in diabetic individuals. Environ Health Perspect. 2011;119(6):778–83. https://doi.org/10.1289/ehp.1002543.
Breitner S, Schneider A, Devlin RB, Ward-Caviness CK, Diaz-Sanchez D, Neas LM, et al. Associations among plasma metabolite levels and short-term exposure to PM2.5 and ozone in a cardiac catheterization cohort. Environ Int. 2016;97:76–84. https://doi.org/10.1016/j.envint.2016.10.012.
Rajagopalan S, Brauer M, Bhatnagar A, Bhatt DL, Brook JR, Huang W, et al. Personal-level protective actions against particulate matter air pollution exposure: a scientific statement from the American Heart Association. Circulation. 2020;142(23):e411–31. https://doi.org/10.1161/CIR.0000000000000931.
Tong H. Dietary and pharmacological intervention to mitigate the cardiopulmonary effects of air pollution toxicity. Biochim Biophys Acta. 2016;1860(12):2891–8. https://doi.org/10.1016/j.bbagen.2016.05.014.
Hu Y, Hu FB, Manson JE. Marine omega-3 supplementation and cardiovascular disease: an updated meta-analysis of 13 randomized controlled trials involving 127 477 participants. J Am Heart Assoc. 2019;8(19): e013543. https://doi.org/10.1161/JAHA.119.013543.
Felix-Redondo FJ, Grau M, Fernandez-Berges D. Cholesterol and cardiovascular disease in the elderly. Facts and gaps. Aging Dis. 2013;4(3):154–69.
Bhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, Ketchum SB, et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380(1):11–22. https://doi.org/10.1056/NEJMoa1812792.
Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17–24. https://doi.org/10.1016/j.blre.2014.09.003.
de Bono D. Significance of raised plasma concentrations of tissue-type plasminogen activator and plasminogen activator inhibitor in patients at risk from ischaemic heart disease. Br Heart J. 1994;71(6):504–7. https://doi.org/10.1136/hrt.71.6.504.
Liang Q, Sun M, Wang F, Ma Y, Lin L, Li T, et al. Short-term PM2.5 exposure and circulating von Willebrand factor level: a meta-analysis. Sci Total Environ. 2020;737:140180. https://doi.org/10.1016/j.scitotenv.2020.140180.
Pieters N, Plusquin M, Cox B, Kicinski M, Vangronsveld J, Nawrot TS. An epidemiological appraisal of the association between heart rate variability and particulate air pollution: a meta-analysis. Heart. 2012;98(15):1127–35. https://doi.org/10.1136/heartjnl-2011-301505.
Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Health. 2017;5:258. https://doi.org/10.3389/fpubh.2017.00258.
O’Neill J, Bounford K, Anstey A, D’Silva J, Clark L, Plein S, et al. P wave indices, heart rate variability and anthropometry in a healthy South Asian population. PLoS ONE. 2019;14(8):e0220662. https://doi.org/10.1371/journal.pone.0220662.
Miller DB, Ghio AJ, Karoly ED, Bell LN, Snow SJ, Madden MC, et al. Ozone exposure increases circulating stress hormones and lipid metabolites in humans. Am J Respir Crit Care Med. 2016;193(12):1382–91. https://doi.org/10.1164/rccm.201508-1599OC.
Vasan RS. Biomarkers of cardiovascular disease: molecular basis and practical considerations. Circulation. 2006;113(19):2335–62. https://doi.org/10.1161/CIRCULATIONAHA.104.482570.
Snow SJ, Cheng WY, Henriquez A, Hodge M, Bass V, Nelson GM, et al. Ozone-induced vascular contractility and pulmonary injury are differentially impacted by diets enriched with coconut oil, fish oil, and olive oil. Toxicol Sci. 2018;163(1):57–69. https://doi.org/10.1093/toxsci/kfy003.
Tong H, Snow SJ, Chen H, Schladweiler MC, Carswell G, Chorley B, et al. Fish oil and olive oil-enriched diets alleviate acute ozone-induced cardiovascular effects in rats. Toxicol Appl Pharmacol. 2020;409: 115296. https://doi.org/10.1016/j.taap.2020.115296.
Bromberg PA. Mechanisms of the acute effects of inhaled ozone in humans. Biochim Biophys Acta. 2016;1860(12):2771–81. https://doi.org/10.1016/j.bbagen.2016.07.015.
Shi L, Zanobetti A, Kloog I, Coull BA, Koutrakis P, Melly SJ, et al. Low-concentration PM2.5 and mortality: estimating acute and chronic effects in a population-based study. Environ Health Perspect. 2016;124(1):46–52. https://doi.org/10.1289/ehp.1409111.
Tong H, Zhang S, Shen W, Chen H, Salazar C, Schneider A, et al. Lung function and short-term ambient air pollution exposure: differential impacts of omega-3 and omega-6 fatty acids. Ann Am Thorac Soc. 2021. https://doi.org/10.1513/AnnalsATS.202107-767OC.
Harris WS, Von Schacky C. The Omega-3 Index: a new risk factor for death from coronary heart disease? Prev Med. 2004;39(1):212–20. https://doi.org/10.1016/j.ypmed.2004.02.030.
Harris WS, Del Gobbo L, Tintle NL. The Omega-3 Index and relative risk for coronary heart disease mortality: estimation from 10 cohort studies. Atherosclerosis. 2017;262:51–4. https://doi.org/10.1016/j.atherosclerosis.2017.05.007.
Chen H, Zhang S, Shen W, Salazar C, Schneider A, Wyatt L, et al. The influence of dietary intake of omega-3 polyunsaturated fatty acids on the association between short-term exposure to ambient nitrogen dioxide and respiratory and cardiovascular outcomes among healthy adults. Environ Health. 2021;20(1):123. https://doi.org/10.1186/s12940-021-00809-9.
Lukens MK, Kerri L, Tong H, Chen H, Shen W. A comparison of Omega-3 fatty acids intakes from three dietary screening tools. Int J Health Nutr Exerc Sci 2021;1.
Shen W, Weaver AM, Salazar C, Samet JM, Diaz-Sanchez D, Tong H. Validation of a dietary questionnaire to screen omega-3 fatty acids levels in healthy adults. Nutrients. 2019;11(7):1. https://doi.org/10.3390/nu11071470.
Mirowsky JE, Carraway MS, Dhingra R, Tong H, Neas L, Diaz-Sanchez D, et al. Ozone exposure is associated with acute changes in inflammation, fibrinolysis, and endothelial cell function in coronary artery disease patients. Environ Health. 2017;16(1):126. https://doi.org/10.1186/s12940-017-0335-0.
Acknowledgements
The authors would like to acknowledge Dr. Kirby Zeman for his critical review and valuable suggestions. We thank Tracey Montilla, Julie Wood, Martin Case, Lisa Dailey, Joleen Soukup, and Shirley Harder for their excellent technical support. We thank the recruitment service from MPF Federal. This project was supported in part by an appointment to the Research Participation Program at the U.S. Environmental Protection Agency, administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the U.S. Department of Energy and EPA.
Disclaimer The research described in this article has been reviewed by the Center for Public Health and Environmental Assessment, EPA, and approved for publication. The contents of this article should not be construed to represent agency policy nor does mention of trade names or commercial products constitute endorsement or recommendation for use.
Funding
This work was supported by the U.S. Environmental Protection Agency Intramural Research Program.
Author information
Authors and Affiliations
Contributions
HC acquired, analyzed, interpreted data, conceived the figures, drafted the manuscript, and revised the manuscript. SZ acquired data, performed statistical analysis, interpreted data, drafted parts of the manuscript, and revised the manuscript. WS co-designed the project, acquired, analyzed, and interpreted data. CS acquired data. AS co-designed the project, analyzed, and interpreted data, and revised the manuscript. LHW acquired data. AGR analyzed and interpreted data. DDS co-designed the project and interpreted data. RBD co-designed the project and interpreted data. JMS co-designed the project, acquired, and interpreted data, and revised the manuscript. HT co-designed the project, managed project, acquired, and interpreted data, and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of the University of North Carolina at Chapel Hill and the U.S.EPA and registered at ClinicalTrials.gov (NCT02921048).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no actual or competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Omega-3 fatty acids attenuate cardiovascular effects of short-term exposure to ambient air pollution.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, H., Zhang, S., Shen, W. et al. Omega-3 fatty acids attenuate cardiovascular effects of short-term exposure to ambient air pollution. Part Fibre Toxicol 19, 12 (2022). https://doi.org/10.1186/s12989-022-00451-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12989-022-00451-4