
Abstract
Background
The health effects of short-term exposure to ambient ultrafine particles in micro-environments are still under investigation.
Methods
Sixty-four individuals with type 2 diabetes and impaired glucose tolerance recorded ambulatory electrocardiograms over five to six hours on 191 occasions in a panel study in Augsburg, Germany. Personal exposure to particle number concentrations (PNC) was monitored for each individual on 5-minute basis concurrently and particulate matter with an aerodynamic diameter < 2.5 μm (PM2.5) was acquired from a central monitoring site on an hourly basis.
Results
More than 11,000 5-minute intervals were available for heart rate and measures of heart rate variability including SDNN (standard deviation of NN intervals). A concurrent decrease in 5-minute SDNN of −0.56% (95% confidence limits (CI): −1.02%; −0.09%) and a 5-minute delayed increase in heart rate of 0.23 % (95% CI: 0.11%; 0.36%) was observed with an increase in personal PNC of 16,000 per cm3 in additive mixed models. Models evaluating the association of concurrent 5-minute personal PNC and of 1-hour PM2.5 showed independent effects on SDNN.
Conclusion
The data suggest that freshly emitted ultrafine particles and aged fine particulate matter are both associated with changes in cardiac function in individuals with type 2 diabetes and impaired glucose tolerance in urban areas.
Similar content being viewed by others

Background
Over the past decade, ambient particulate matter has been established as a likely causal risk factor for cardiovascular disease morbidity and mortality [1]. In particular, exacerbation of cardiovascular disease has been observed within individuals with diabetes during episodes of high ambient air pollution exposures [2-4]. It has been noted that ambient particles [5,6] as well as exposure to traffic [7,8] might trigger myocardial infarctions within one or two hours. It is hypothesized that these associations may be a consequence of a direct effect on the electric system of the heart [1]. The effects of air pollution on heart rate (HR) and heart rate variability (HRV) were extensively studied [1] since Pope et al. [9,10], Peters et al. [11], and Gold et al. [12] initially reported these associations. The most consistent evidence with respect to cardiovascular disease exists for fine particulate matter with an aerodynamic diameter smaller than 2.5 μm (PM2.5) [1]. Especially, particles from mobile sources are suggested to be linked strongly to cardiovascular disease exacerbation [13]. Particles from emitted mobile sources are much smaller, mostly in the ultrafine range below 100 nm and have the potential to act systemically in organisms [14,15].
Recent evidence from controlled exposures to ultrafine carbon particles suggested altered autonomic function during the exposure in subjects with type 2 diabetes [16]. The study presented here aimed to assess the immediate impact of personal exposure particle to number concentrations (PNC) on HR and HRV measured by ambulatory electrocardiograms (ECG) during five to six hour periods in individuals with diagnosed type 2 diabetes or impaired glucose tolerance (IGT). Specifically, we assess the impact of personally measured PNC during the morning hours on heart rate variability. We build on previous analyses that assessed the association between centrally monitored ambient air pollution and cardiac function within the same study [17]. We had previously reported associations between 1-hour PM2.5 and decreased heart rate variability upon concurrent exposure as well as exposures occurring up to 4 hours before the ECG recording.
Results and discussion
Patient characteristics
Sixty-four non-smoking panel members were recruited for repeated measurements of personal exposure to PNC and parallel ECG recording. Table 1 describes the baseline characteristics of the 32 individuals with confirmed diagnosis of type 2 diabetes and 32 individuals with IGT recruited based on the KORA F4 study [18,19]. No differences were observed between the type 2 diabetes patients and the individuals with IGT concerning their age, gender, body mass index or disease history. Glycosylated hemoglobin A1c (HbA1c) concentrations above 6.5% were more frequently observed in individuals with diabetes than those with IGT. Diabetes prescriptions were taken by more than half of the participants with diabetes and one participant with IGT. More than 14,000 repeated 5-minute ECG measures and more than 1,200 1-hour ECG measures were available (Table 1). Patients with diabetes had lower HR and HRV on a 5-minute basis. This different was no longer apparent for HRV based on 1-hour ECG recordings.
Personal exposures to particle number concentrations
Table 2 describes the distribution of the personal PNC measurements and the distribution of particle concentrations at the central monitoring site. Substantially higher variation in personal PNC was observed during personal monitoring compared to the background level (Table 2). Figure 1 describes an example indicating that elevated levels of PNC may occur during times spent in traffic, while indoor concentrations may be substantially lower in the absence of indoor sources. Elevated personal PNC were observed when individuals spent time in traffic (median = 17,884 cm−3, N = 3,523), when cooking (median = 43,612 cm−3, N = 285) or exposed to environmental tobacco smoke (ETS) (median = 21,929 cm−3, N = 148). In contrast, personal PNC concentrations were lower during times spent at home without cooking or ETS exposure (median = 8,833 cm−3, N = 6,930). By design of the study, participants were commuting within the urban area of Augsburg in the morning and midday hours. Thereby, personal exposures were impacted by the morning rush-hour as well as by lower traffic volumes during midday and were there deviating from concentrations measured at an urban background monitoring site within the city center. Subject-specific Spearman correlation coefficients between 1-hour personal PNC concentrations and 1-hour ambient ultrafine particles (UFP) had a median of 0.35 and ranged from −0.60 at the 10th percentile to 0.90 at the 90th percentile. Personally measured PNC characterise the exposure to mobile source emissions or other sources of freshly emitted particles and are determined by the personal activities as well as meteorological influences in the region of Augsburg, Germany [20,21].

Example of personal measurements of PNC. Data was collected starting and ending at the KORA Study Center on November 27th 2007.
Ambient UFP were only moderately correlated with PM10 and PM2.5 measured at the same central monitoring site (spearman correlation coefficients of 0.49 and 0.42, respectively). In contrast, accumulation mode particles (ACP) were highly correlated to 1-hour PM10, PM2.5 and UFP (Spearman correlation coefficients of 0.79, 0.75 and 0.70, respectively).
Changes in heart rate variability in response to particle exposure
Table 3 shows the associations between 5-minute personal exposures to PNC and HR and HRV assessing concurrent and exposures lagged up to 15 minutes. It shows a slightly delayed response of HR and an immediate decrease in SDNN. Different responses of HR and SDNN to PNC may be reasonable given the fact that correlation between HR and SDNN differed substantially between individuals with a median Spearman correlation of −0.10 and a range between −0.53 and 0.55.
Associations between PNC and SDNN appear to be more pronounced in individuals with diabetes than in individuals with IGT (Figure 2). Exploratory analyses extending the time-lag between 5-minute personal exposure to PNC and HR, SDNN or RMSSD up to one hour showed no consistent pattern beyond 15 minutes.

Effects of personally measured 5-minute PNC on SDNN based on 5-minute ECG recordings in patients with diabetes or impaired glucose tolerance. Effect estimates are shown for an increase of 16,000 particles cm−3.
We had previously shown associations between 1-hour ambient air pollution concentrations and cardiac function occurring up to a lag of 4 hours [17]. We had chosen one hour intervals of exposure and ECG recordings a priori as we considered this the minimal time scale for a central monitoring site in an urban background location to represent population average exposures. In Table 4 we compare the association between 1-hour averages of personal PNC and ambient UFP, ACP, PM10 and PM2.5 and concurrent measures of HR and HRV over 1-hour. No consistent associations between personal or ambient particles number concentrations (PNC, UFP, ACP) and HR were observed. In contrast, PM10 and PM2.5 were associated both with SDNN and RMSSD as reported previously [17]. The association between PM2.5 and HRV was stronger in individuals with IGT than those with type 2 diabetes, but the differences did not achieve statistical significance. In line with our results, Chan and colleagues observed significant decreases in SDNN and RMSSD in association with an increase of 10,000 particles/cm3 in personally measured particles in the size range between 20 nm and 1 μm in a prospective panel study [22]. Adverse changes in HR and HRV were also observed in association with ambient UFP in panel or cross-over studies [23-28] and with concentrated UFP in controlled chamber studies [29,30] albeit some associations were not significant. However, some studies reported no or even positive associations between HRV and UFP [31-33].
Effect estimates were larger for the 1-hour PM2.5 than for personal PNC and associations between 1-hour PM2.5 concentrations and 5-minute HRV strengthened when adjusting for personal PNC (Figure 3). PM2.5 measured at an urban background monitoring site quantifies the overall particulate matter level predominantly determined by the meteorological conditions. In the present study, we demonstrate therefore that particle exposures determined by personal proximity to sources and by urban background levels both are associated with changes in cardiac function on a very immediate time scale.

Two pollutant models for 5-minute personal PNC and 1-hour ambient PM 2.5 on 5-minute HR and HRV parameters. in patients with diabetes or impaired glucose tolerance. Effect estimates are shown for an increase of 16,000 particles cm−3 and 12 μg m−3 PM2.5.
Earlier studies have observed associations between hourly concentrations of PM2.5 and the onset of myocardial infarction in Boston, MA [5] and Rochester, NY [6]. Moreover, times spent in traffic were associated with the onset of myocardial infarction [7,8] and controlled exposure studies suggest that effects of diesel exposures might be enhanced by exercise [34]. Previous studies have in many instances indicated that personal exposures to PM2.5 or to gaseous pollutants are associated with changes in HRV [26,35-51]. The study participants ranged from healthy adults to patients with cardiovascular diseases or asthma and were studied in different settings around the world. We had chosen individuals with impaired glucose metabolism because individuals with type 2 diabetes had been shown to be susceptible to air pollution [2-4]. A study of controlled human exposures to concentrated ultrafine particles showed immediate effects on subjects with metabolic syndrome, however, did not observe changes in HRV one hour after the exposure [30]. In contrast, in a study in subjects with type 2 diabetes indicated a decrease in the high frequency component of heart rate variability and increased heart rates persisting up to 48 hours [16]. Furthermore, there is an emerging body of evidence linking ambient air quality as one of the risk factors to type 2 diabetes [52]. Data from controlled animal experiments [53] as well as analyses in prospective population-based cohort studies [54-58] support this association. Systemic inflammation, activation of innate immunity in the lung and an imbalance of the autonomic nervous system induced by air pollution exposures jointly potentially provide the link to insulin resistance and diabetes exacerbation [52]. Sudden changes in cardiac function may predispose susceptible individuals to sudden cardiac deaths during episodes with elevated particle concentrations [59]. Most likely, different underlying intrinsic mechanisms are activated by 5-minute PNC and 1-hour PM2.5. We hypothesize that shortly elevated PNC may activate irritant receptors and lead thereby to changes in the autonomic control [60]. In contrast, we hypothesize that the changes in HRV observed in association with PM2.5 are associated with an activation of host defense on an alveolar level, which may involve translocation of particle components, immediate systemic oxidative stress response and an activation of leukocytes [52].
Sensitivity analyses
Associations were robust in sensitivity analyses and a summary is given in Figure 4 for the association between personally measured personal PNC and SDNN. No statistically significant difference was observed in individuals without beta-blockers intake or statin use. By selecting individuals with impaired glucose tolerance, we intended to study the impact of particles in individuals who were not heavily treated by beta-blockers or statins as these medications may obliterate the effects of particle exposures [61,62].

Sensitivity analyses of the association between concurrent exposure to personally measured PNC and SDNN. *Regression coefficient as reported in Table 3.
Excluding time periods when the participants recorded ETS exposures or cooking rendered consistent results, but suggested that indoor sources contributed to the observed associations. We employed two different ways to adjust for physical activity. Neither adjusting for the diary entries of physical activity nor for heart rate did change the effect estimates. Models including personal noise exposure showed stronger associations with personal PNC (Figure 3) and increased 5-minute SDNN (3.35% [95% CI: 2.95% ; 4.11%] per 5 db[A]) as reported previously [63]. These analyses suggested that the associations of PNC and noise with ECG-parameters were potentially confounding each other. To further test the impact of the model choices, we conducted sensitivity analyses for the immediate effect of PNC on SDNN. Including a time trend within the measurements or including the previous segments of SDNN as a predictor did not change the effect estimates substantially (5-minute SDNN: −0.56% [−0.98%;-0.13%] or −0.42% [−0.77%;-0.06%] per 16,000 cm−3 PNC, respectively).
Limitations
The study assessed personal measurements of PNC which is a novel marker for personal exposure to fresh combustion particles. The study thereby overcomes one large limitation of previous panel studies. By employing direct measurements of PNC it also provides different and novel information compared to studies of personal PM2.5 or gaseous pollutants [26,35-49]. However, the measurement devices are usually operated by technical personnel to measure indoor and outdoor particle concentrations and were not designed for study participants. As a consequence we were only able to achieve 80% of the planned hourly measurements albeit stringent examiner training, review of the instruction sessions by audiotape, and written instructions for the participants. The missing measurements had no certain pattern and were related to diligence in following the instructions by the study participants. Diaries were kept by the participants, but no geographic positioning system data was acquired. ECG data and personal PNC data were processed independently. While the examiners and the participants were aware of the study hypotheses, information on their HR was not available and levels of PNC were not discussed with respect to limit or guideline values as these do not exist.
Timing of the measurements were based on recorded times from the instruments and the study protocols. Discrepant times were checked individually, discussed with the study nurses and corrected wherever possible.
Each day’s measurement provided control data for the individual and correlation within the day and the individual was considered. Analyses proved to be relatively robust against other assumptions of the covariance structure. Confounding by physical activity, a potentially important individual time-varying factor was considered but did not prove to be strong and resulted in changes of the effect estimates of less than 10%.
There were no statistically significant differences with respect to age, body mass index, HbA1c concentrations, history of cardiovascular disease and medication use when comparing the study participants to all individuals with either diabetes or IGT in the underlying sample of the KORA cohort study. Participants of the panel study were more likely to be unemployed, many of them already retired. In addition, the proportion of ex-smokers was higher in the present study than in the overall sample.
As this study is assessing short-term impacts of urban area ambient particulate matter, it does not address the question, whether long-term exposure to particulate matter is associated with an increased risk for incident diabetes as recently shown [54-58]. However, the data reported here provides evidence that short-term exposure to ambient particulate matter may contribute to cardiovascular disease exacerbation in individuals with impaired glucose metabolism or diabetes.
Conclusion
The data presented here shows changes in HRV associated with personally measured PNC and ambient PM2.5 suggesting that both freshly emitted ultrafine particles as well as aged aerosol in urban areas are associated with changes in cardiac function. The study suggests that personal activities and elevated particle concentrations in micro-environments may modify personal exposures and thereby impact on cardiac function. The study was conducted in individuals with type 2 diabetes and IGT suggesting that these subgroups of the population might be at risk for cardiovascular disease exacerbation when transiently exposed to fresh and aged urban particulate matter.
Methods
Study design
A prospective panel study was conducted in Augsburg, Germany, between March 19, 2007 and December 17, 2008. Individuals with diabetes mellitus type 2 or impaired glucose tolerance (IGT) were recruited from an ongoing examination of 3,080 individuals as part of the KORA F4 cohort study (Cooperative Health Research in the Region of Augsburg) as described in detail elsewhere [18,19]. Type 2 diabetes was defined on based on a validated physician diagnosis, or newly diagnosed diabetes (≥7.0 mmol⁄l fasting or ≥ 11.1 mmol⁄l 2-h glucose) determined by an oral glucose tolerance test. IGT was defined according to the 1999 World Health Organization diagnostic criteria [64]. Exclusion criteria for the present study were 1) current active smoking, 2) intake of platelet aggregation inhibitors except for acetylsalicylic acid, 3) a myocardial infarction and/or interventional procedure (PTCA, bypass surgery) less than 6 months before the beginning of the study, and 4) chronic inflammatory diseases such as Crohn’s disease, colitis ulcerosa, and rheumatoid arthritis. Furthermore, individuals were not included in case of 1) an implanted pacemaker, 2) atrial fibrillation, 3) allergy to latex, and 4) thrombosis or shunt in an arm to standardize HRV analyses. All individuals participated in repeated visits scheduled every 4–6 weeks on the same weekday and at the same time of the day.
Ethics and consent statement
The study was conducted in compliance with the Helsinki Declaration. Ethical approval for the study was granted by the Ethics Committee of the Bayerische Landesärztekammer, München, Germany. The study protocol including the participant information and the consent form were part of the ethics review. The study participants gave informed written consent before entering into the study.
ECG monitoring
In the personal monitoring program, participants were equipped for five to six hours with an electrocardiogram (ECG) device during their second up to the fifth visit as described previously [17]. ECGs were recorded with a 12-lead Mortara H12 digital Holter recorder (Mortara Instrument, Milwaukee, WI, USA). Analyses of heart rate variability were restricted to ECGs that had at least 200 beats available for 5-minute intervals. Heart rate (HR) and time domain parameters of HRV, the standard deviation of all normal-to-normal (NN) intervals (SDNN), and the root mean square of successive NN interval differences (RMSSD) were determined on a 5-minute and an hourly basis. Only individuals with at least one ECG recording with duration of at least two hours were used for analysis.
Personal particle number concentration monitoring
Personal exposure to PNC was measured using a portable condensation particle counter model 3007 (TSI Inc., USA) which covered a diameter range from 10 nm to 1 μm. Participants were instructed on how to restart the measurements if tilting might have resulted in an automated stop of the measurements. They carried the device in a specially designed carrier bag within an inlet at the top. Moreover, participants were asked to keep a diary on their activities during the 5–6 hours of personal measurements including information on times spent indoors or outdoors, times spent in traffic, indoor activities such as cooking and sources such as environmental tobacco smoke exposures (ETS). The participants were instructed to always keep the device close by, but at least within the same room at a central location. Diary information was checked for plausibility and used to process the measurement data. In four instances, participants did not carry the PNC device with them for short periods of time (8 minutes, 10 minutes, 30 minutes or 1 hour). These data were excluded from the analyses. Usually, measurements started around 7:30 a.m.; participants were free to go wherever they liked and returned at around 1 p.m. Three portable condensation particle counters were employed during the study. All of them were serviced before the start of the study and comparison measurements were conducted in March 2007. Additional service periods were conducted every six months. More detail is provided in [20].
Central site air pollution monitoring
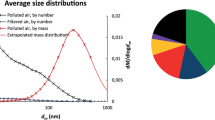
Ambient air pollution was measured at a central measurement site in Augsburg throughout the complete study period as described previously [65,66]. The measurement location was in urban background approximately 1 km to the south-east of the city center. Particle mass concentrations of PM2.5 and PM10 (particulate matter ≤ 2.5 or 10 μm in aerodynamic diameter, respectively) were measured by two separate Tapered Element Oscillating Microbalance (TEOM, model 1400ab, Thermo Fisher Scientific Inc., USA). To correct the PM measurements for aerosol volatility effects, each TEOM was equipped with a Filter Dynamics Measurement System (FDMS, model 8500b, Thermo Fisher Scientific Inc., USA). Particle size distributions in the range from 3–900 nm were measured by a custom-built Twin Differential Mobility Particle Sizer (TDMPS) system consisting of two cylindrical, Vienna-type Differential Mobility Analyzers (DMA) covering complementary size ranges (3 to 23 nm as well as 18 to 900 nm). For the analysis we used the size fraction of ultrafine particles from 10 to 100 nm (ambient UFP) and of accumulation mode particles from 100 to 800 (ambient ACP).
Statistical analyses
Repeated continuous outcome data was analyzed using mixed models with random patient effects to accommodate repeated measures and to account for unobserved heterogeneity of the data. To account for dependencies of the outcome measures, covariance structure considered autocorrelation of the first order for measurements of the same day and correlation between measurements of the same individual at days apart. This was done within the framework of additive mixed models to allow for semi-parametric and non-parametric exposure-response functions. Models were selected separately for HR, SDNN, and RMSSD as described previously [17]. Final models included for HR: time trend (linear), time of day (morning vs. afternoon), 1-hour air temperature (lag 2, polynomial of degree 2), 1-hour relative humidity (lag 1, linear); for SDNN: time trend (linear), time of day (morning vs. afternoon), 1-hour air temperature (concurrent, linear), 1-hour relative humidity (concurrent, linear) ; and for RMSSD: time trend (linear), time of day (morning vs. afternoon), 1-hour air temperature (lag 7, linear), 1-hour relative humidity (lag 4, linear).
Models were adjusted for ambient meteorology and temporal trends. Penalized splines were used to allow for non-linear confounder adjustment. Results are presented as %-change from the mean per 16,000 ultrafine particles cm−3 or the respective interquartile ranges together with 95% confidence intervals. A number of sensitivity analyses were conducted including models adjusting for personal 5-minute noise exposure measured as A-weighted equivalent continuous sound pressure levels (Leq) reported in units of A-weighted decibels [dB(A)] (Spark® model 703; Larson Davis Inc., Depew, NY, USA) as described elsewhere [63]. Data were analyzed using SAS statistical software (version 9.1; SAS Institute Inc., Cary, NC, USA).
References
Brook RD, Rajagopalan S, Pope III CA, Brook JR, Bhatnagar A, Diez-Roux AV, et al. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation. 2010;121:2331–78.
Zeka A, Zanobetti A, Schwartz J. Individual-level modifiers of the effects of particulate matter on daily mortality. Am J Epidemiol. 2006;163:849–59.
Zanobetti A, Schwartz J. Cardiovascular damage by airborne particles: are diabetics more susceptible? Epidemiology. 2002;13:588–92.
Zanobetti A, Schwartz J. Are diabetics more susceptible to the health effects of airborne particles? Am J RespirCrit Care Med. 2001;164:831–3.
Peters A, Dockery DW, Muller JE, Mittleman MA. Increased particulate air pollution and the triggering of myocardial infarction. Circulation. 2001;103:2810–5.
Gardner B, Ling F, Hopke PK, Frampton MW, Utell MJ, Zareba W, et al. Ambient fine particulate air pollution triggers ST-elevation myocardial infarction, but not non-ST elevation myocardial infarction: a case-crossover study. Part Fibre Toxicol. 2014;11:1.
Peters A, von Klot S, Heier M, Trentinaglia I, Hormann A, Wichmann HE, et al. Exposure to traffic and the onset of myocardial infarction. N Engl J Med. 2004;351:1721–30.
Peters A, von Klot S, Mittleman MA, Meisinger C, Hormann A, Kuch B, et al. Triggering of acute myocardial infarction by different means of transportation. Eur J Prev Cardiol. 2013;20:750–8.
Pope CA, Dockery DW, Kanner RE, Villegas GM, Schwartz J. Oxygen saturation, pulse rate, and particulate air pollution: a daily time-series panel study. Am J RespirCrit Care Med. 1999;159:365–72.
Pope 3rd CA, Verrier RL, Lovett EG, Larson AC, Raizenne ME, Kanner RE, et al. Heart rate variability associated with particulate air pollution. Am Heart J. 1999;138:890–9.
Peters A, Perz S, Doring A, Stieber J, Koenig W, Wichmann HE. Increases in heart rate during an air pollution episode. Am J Epidemiol. 1999;150:1094–8.
Gold DR, Litonjua A, Schwartz J, Lovett E, Larson A, Nearing B, et al. Ambient pollution and heart rate variability. Circulation. 2000;101:1267–73.
Zanobetti A, Stone PH, Speizer FE, Schwartz JD, Coull BA, Suh HH, et al. T-wave alternans, air pollution and traffic in high-risk subjects. Am J Cardiol. 2009;104:665–70.
Kreyling WG, Semmler-Behnke M, Takenaka S, Moller W. Differences in the Biokinetics of Inhaled Nano- versus Micrometer-Sized Particles. Acc Chem Res. 2013;46:714–22.
Cassee FR, Heroux ME, Gerlofs-Nijland ME, Kelly FJ. Particulate matter beyond mass: recent health evidence on the role of fractions, chemical constituents and sources of emission. Inhal Toxicol. 2013;25:802–12.
Vora R, Zareba W, Utell MJ, Pietropaoli AP, Chalupa D, Little EL, et al. Inhalation of ultrafine carbon particles alters heart rate and heart rate variability in people with type 2 diabetes. Part Fibre Toxicol. 2014;11:31.
Hampel R, Breitner S, Schneider A, Zareba W, Kraus U, Cyrys J, et al. Acute air pollution effects on heart rate variability are modified by SNPs involved in cardiac rhythm in individuals with diabetes or impaired glucose tolerance. Environ Res. 2012;112:177–85.
Rathmann W, Strassburger K, Heier M, Holle R, Thorand B, Giani G, et al. Incidence of Type 2 diabetes in the elderly German population and the effect of clinical and lifestyle risk factors: KORA S4/F4 cohort study. Diabet Med. 2009;26:1212–9.
Meisinger C, Strassburger K, Heier M, Thorand B, Baumeister SE, Giani G, et al. Prevalence of undiagnosed diabetes and impaired glucose regulation in 35-59-year-old individuals in Southern Germany: the KORA F4 Study. Diabet Med. 2010;27:360–2.
Gu J, Kraus U, Schneider A, Hampel R, Pitz M, Breitner S, et al. Personal day-time exposure to ultrafine particles in different microenvironments. Int J Hyg Environ Health. 2015;218:188–95.
Deffner V, Kuchenhoff H, Maier V, Pitz M, Cyrys J, Breitner S et al. Personal exposure to ultrafine particles: Two-level statistical modeling of background exposure and time-activity patterns during three seasons. J Expo Sci Environ Epidemiol 2014;1-9.
Chan CC, Chuang KJ, Shiao GM, Lin LY. Personal exposure to submicrometer particles and heart rate variability in human subjects. Environ Health Perspect. 2004;112:1063–7.
Park SK, O’Neill MS, Vokonas PS, Sparrow D, Schwartz J. Effects of air pollution on heart rate variability: the VA normative aging study. Environ Health Perspect. 2005;113:304–9.
Bartell SM, Longhurst J, Tjoa T, Sioutas C, Delfino RJ. Particulate air pollution, ambulatory heart rate variability, and cardiac arrhythmia in retirement community residents with coronary artery disease. Environ Health Perspect. 2013;121:1135–41.
Rich DQ, Zareba W, Beckett W, Hopke PK, Oakes D, Frampton MW, et al. Are ambient ultrafine, accumulation mode, and fine particles associated with adverse cardiac responses in patients undergoing cardiac rehabilitation? Environ Health Perspect. 2012;120:1162–9.
Weichenthal S, Kulka R, Belisle P, Joseph L, Dubeau A, Martin C, et al. Personal exposure to specific volatile organic compounds and acute changes in lung function and heart rate variability among urban cyclists. Environ Res. 2012;118:118–23.
Timonen KL, Vanninen E, de Hartog J, Ibald-Mulli A, Brunekreef B, Gold DR, et al. Effects of ultrafine and fine particulate and gaseous air pollution on cardiac autonomic control in subjects with coronary artery disease: the ULTRA study. J Expo Sci Environ Epidemiol. 2006;16:332–41.
Schneider A, Neas LM, Graff DW, Herbst MC, Cascio WE, Schmitt MT, et al. Association of cardiac and vascular changes with ambient PM2.5 in diabetic individuals. Part FibreToxicol. 2010;7:14.
Hagerman I, Isaxon C, Gudmundsson A, Wierzbicka A, Dierschke K, Berglund M, et al. Effects on heart rate variability by artificially generated indoor nano-sized particles in a chamber study. Atmos Environ. 2014;88:165–71.
Devlin RB, Smith CB, Schmitt MT, Rappold AG, Hinderliter A, Graff D, et al. Controlled exposure of humans with metabolic syndrome to concentrated ultrafine ambient particulate matter causes cardiovascular effects. Toxicol Sci. 2014;140:61–72.
Laumbach RJ, Kipen HM, Ko S, Kelly-McNeil K, Cepeda C, Pettit A, et al. A controlled trial of acute effects of human exposure to traffic particles on pulmonary oxidative stress and heart rate variability. Part Fibre Toxicol. 2014;11:45.
Samet JM, Rappold A, Graff D, Cascio WE, Berntsen JH, Huang YC, et al. Concentrated ambient ultrafine particle exposure induces cardiac changes in young healthy volunteers. Am J Respir Crit Care Med. 2009;179:1034–42.
Zareba W, Couderc JP, Oberdorster G, Chalupa D, Cox C, Huang LS, et al. ECG parameters and exposure to carbon ultrafine particles in young healthy subjects. Inhal Toxicol. 2009;21:223–33.
Mills NL, Tornqvist H, Gonzalez MC, Vink E, Robinson SD, Soderberg S, et al. Ischemic and thrombotic effects of dilute diesel-exhaust inhalation in men with coronary heart disease. N Engl J Med. 2007;357:1075–82.
Magari SR, Schwartz J, Williams PL, Hauser R, Smith TJ, Christiani DC. The association between personal measurements of environmental exposure to particulates and heart rate variability. Epidemiology. 2002;13:305–10.
Tarkiainen TH, Timonen KL, Vanninen EJ, Alm S, Hartikainen JE, Pekkanen J. Effect of acute carbon monoxide exposure on heart rate variability in patients with coronary artery disease. Clin Physiol Funct Imaging. 2003;23:98–102.
Chang CC, Hwang JS, Chan CC, Wang PY, Hu TH, Cheng TJ. Effects of concentrated ambient particles on heart rate, blood pressure, and cardiac contractility in spontaneously hypertensive rats. Inhal Toxicol. 2004;16:421–9.
Vallejo M, Ruiz S, Hermosillo AG, Borja-Aburto VH, Cardenas M. Ambient fine particles modify heart rate variability in young healthy adults. J Expo Sci Environ Epidemiol. 2006;16:125–30.
Riojas-Rodriguez H, Escamilla-Cejudo JA, Gonzalez-Hermosillo JA, Tellez-Rojo MM, Vallejo M, Santos-Burgoa C, et al. Personal PM2.5 and CO exposures and heart rate variability in subjects with known ischemic heart disease in Mexico City. J Expo Sci Environ Epidemiol. 2006;16:131–7.
Chang LT, Tang CS, Pan YZ, Chan CC. Association of heart rate variability of the elderly with personal exposure to PM 1, PM 1–2.5, and PM 2.5-10. Bull Environ Contam Toxicol. 2007;79:552–6.
Cardenas M, Vallejo M, Romano-Riquer P, Ruiz-Velasco S, Ferreira-Vidal AD, Hermosillo AG. Personal exposure to PM2.5 air pollution and heart rate variability in subjects with positive or negative head-up tilt test. Environ Res. 2008;108:1–6.
Fan ZT, Meng Q, Weisel C, Laumbach R, Ohman-Strickland P, Shalat S, et al. Acute exposure to elevated PM2.5 generated by traffic and cardiopulmonary health effects in healthy older adults. J Expo Sci Environ Epidemiol. 2009;19:525–33.
Folino AF, Scapellato ML, Canova C, Maestrelli P, Bertorelli G, Simonato L, et al. Individual exposure to particulate matter and the short-term arrhythmic and autonomic profiles in patients with myocardial infarction. Eur Heart J. 2009;30:1614–20.
De Hartog JJ, Lanki T, Timonen KL, Hoek G, Janssen NA, Ibald-Mulli A, et al. Associations between PM2.5 and heart rate variability are modified by particle composition and beta-blocker use in patients with coronary heart disease. Environ Health Perspect. 2009;117:105–11.
Wu CF, Kuo IC, Su TC, Li YR, Lin LY, Chan CC, et al. Effects of personal exposure to particulate matter and ozone on arterial stiffness and heart rate variability in healthy adults. Am J Epidemiol. 2010;171:1299–309.
He F, Shaffer ML, Li X, Rodriguez-Colon S, Wolbrette DL, Williams R, et al. Individual-level PM(2).(5) exposure and the time course of impaired heart rate variability: the APACR Study. J Expo Sci Environ Epidemiol. 2011;21:65–73.
Langrish JP, Li X, Wang S, Lee MM, Barnes GD, Miller MR, et al. Reducing personal exposure to particulate air pollution improves cardiovascular health in patients with coronary heart disease. Environ Health Perspect. 2012;120:367–72.
Shields KN, Cavallari JM, Hunt MJ, Lazo M, Molina M, Molina L, et al. Traffic-related air pollution exposures and changes in heart rate variability in Mexico City: A panel study. Environ Health. 2013;12:7.
Huang J, Deng F, Wu S, Lu H, Hao Y, Guo X. The impacts of short-term exposure to noise and traffic-related air pollution on heart rate variability in young healthy adults. J Expo Sci Environ Epidemiol. 2013;23:559–64.
Hampel R, Ruckerl R, Yli-Tuomi T, Breitner S, Lanki T, Kraus U, et al. Impact of personally measured pollutants on cardiac function. Int J Hyg Environ Health. 2014;217:460–4.
Sarnat JA, Golan R, Greenwald R, Raysoni AU, Kewada P, Winquist A, et al. Exposure to traffic pollution, acute inflammation and autonomic response in a panel of car commuters. Environ Res. 2014;133:66–76.
Rajagopalan S, Brook RD. Air pollution and type 2 diabetes: mechanistic insights. Diabetes. 2012;61:3037–45.
Sun Q, Yue P, Deiuliis JA, Lumeng CN, Kampfrath T, Mikolaj MB, et al. Ambient air pollution exaggerates adipose inflammation and insulin resistance in a mouse model of diet-induced obesity. Circulation. 2009;119:538–46.
Raaschou-Nielsen O, Sorensen M, Ketzel M, Hertel O, Loft S, Tjonneland A, et al. Long-term exposure to traffic-related air pollution and diabetes-associated mortality: a cohort study. Diabetologia. 2013;56:36–46.
Andersen ZJ, Raaschou-Nielsen O, Ketzel M, Jensen SS, Hvidberg M, Loft S, et al. Diabetes incidence and long-term exposure to air pollution: a cohort study. Diabetes Care. 2012;35:92–8.
Puett RC, Hart JE, Schwartz J, Hu FB, Liese AD, Laden F. Are particulate matter exposures associated with risk of type 2 diabetes? Environ Health Perspect. 2011;119:384–9.
Coogan PF, White LF, Jerrett M, Brook RD, Su JG, Seto E, et al. Air pollution and incidence of hypertension and diabetes mellitus in black women living in Los Angeles. Circulation. 2012;125:767–72.
Kramer U, Herder C, Sugiri D, Strassburger K, Schikowski T, Ranft U, et al. Traffic-related air pollution and incident type 2 diabetes: results from the SALIA cohort study. Environ Health Perspect. 2010;118:1273–9.
Zareba W, Nomura A, Couderc JP. Cardiovascular effects of air pollution: what to measure in ECG? Environ Health Perspect. 2001;109 Suppl 4:533–8.
Schulz H, Harder V, Ibald-Mulli A, Khandoga A, Koenig W, Krombach F, et al. Cardiovascular effects of fine and ultrafine particles. J Aerosol Med. 2005;18:1–22.
Timonen KL, Hoek G, Heinrich J, Bernard A, Brunekreef B, de Hartog J, et al. Daily variation in fine and ultrafine particulate air pollution and urinary concentrations of lung Clara cell protein CC16. Occup Environ Med. 2004;61:908–14.
Ruckerl R, Greven S, Ljungman P, Aalto P, Antoniades C, Bellander T, et al. Air pollution and inflammation (interleukin-6, C-reactive protein, fibrinogen) in myocardial infarction survivors. Environ Health Perspect. 2007;115:1072–80.
Kraus U, Schneider A, Breitner S, Hampel R, Ruckerl R, Pitz M, et al. Individual daytime noise exposure during routine activities and heart rate variability in adults: a repeated measures study. Environ Health Perspect. 2013;121:607–12.
Organisation WH. Definition, Diagnosis and Classification of Diabetes Mellitus and its Complications. Part 1: Diagnosis and Classification of Diabetes Mellitus. In: Report of a WHO consultation. Geneva: WHO; 1999.
Birmili W, Heinke K, Pitz M, Matschullat J, Wiedensohler A, Cyrys J, et al. Particle number size distributions in urban air before and after volatilisation. Atmos Chem Phys. 2010;10:4643–60.
Pitz M, Birmili W, Schmid O, Peters A, Wichmann HE, Cyrys J. Quality control and quality assurance for particle size distribution measurements at an urban monitoring station in Augsburg, Germany. J Environ Monit. 2008;10:1017–24.
Acknowledgement
This research has been funded in part by the United States Environmental Protection Agency through STAR (“Science to Achieve Results”) grant RD 832415 to the University of Rochester. It has not been subjected to the Agency’s required peer and policy review and therefore does not necessarily reflect the views of the Agency and no official endorsement should be inferred. This study was supported in part by a grant from the German Federal Ministry of Education and Research (BMBF) to the German Center for Diabetes Research (DZD e.V.). The KORA research platform (KORA, Cooperative Health Research in the Region of Augsburg) and the MONICA Augsburg studies were initiated and financed by the Helmholtz Zentrum München, German Research Center for Environmental Health (formerly GSF, National Research Center for Environment and Health), which is funded by the German Federal Ministry of Education and Research and by the State of Bavaria.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AP conceived the study design, obtained funding, supervised the study, directed the data analyses, drafted the manuscript and compiled its final version. RH and SB analyzed the data, JC and designed and supervised the air pollution monitoring, UG performed the data quality assurance, UK supervised the activity diary, WZ designed and performed the ECG analyses, AS contributed to the study design and supervised the field work, quality assurance and data analyses. All authors contributed to interpreting the results, commented on the manuscript and approved its final version.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Peters, A., Hampel, R., Cyrys, J. et al. Elevated particle number concentrations induce immediate changes in heart rate variability: a panel study in individuals with impaired glucose metabolism or diabetes. Part Fibre Toxicol 12, 7 (2015). https://doi.org/10.1186/s12989-015-0083-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12989-015-0083-7