
Abstract
Background
Serologic detection of Zika virus (ZIKV) infections is challenging because of antigenic similarities among flaviviruses.
Objective
To evaluate the sensitivity and specificity of commercial ZIKV IgM and IgG enzyme-linked immunoassay (ELISA) kits.
Methods
We used sera from febrile patients with RT-PCR-confirmed ZIKV infection to determine sensitivity and sera from RT-PCR-confirmed dengue cases and blood donors, both of which were collected before ZIKV epidemics in Brazil (2009–2011 and 2013, respectively) to determine specificity.
Results
The ZIKV IgM-ELISA positivity among RT-PCR ZIKV confirmed cases was 0.0% (0/14) and 12.5% (1/8) for acute- and convalescent-phase sera, respectively, while its specificity was 100.0% (58/58) and 98.3% (58/59) for acute- and convalescent-phase sera of dengue patients, and 100.0% (23/23) for blood donors. The ZIKV IgG-ELISA sensitivity was 100.0% (6/6) on convalescent-phase sera from RT-PCR confirmed ZIKV patients, while its specificity was 27.3% (15/55) on convalescent-phase sera from dengue patients and 45.0% (9/20) on blood donors’ sera. The ZIKV IgG-ELISA specificity among dengue confirmed cases was much greater among patients with primary dengue (92.3%; 12/13), compared to secondary dengue (7.1%; 3/42).
Conclusions
In a setting of endemic dengue transmission, the ZIKV IgM-ELISA had high specificity, but poor sensitivity. In contrast, the ZIKV IgG-ELISA showed low specificity, particularly for patients previously exposed to dengue infections. This suggests that this ZIKV IgM-ELISA is not useful in confirming a diagnosis of ZIKV infection in suspected patients, whereas the IgG-ELISA is more suitable for ZIKV diagnosis among travelers, who reside in areas free of flavivirus transmission, rather than for serosurveys in dengue-endemic areas.
Similar content being viewed by others

Background
Zika virus (ZIKV) is an emerging mosquito-borne flavivirus. Majority of human infections evolve asymptomatically or cause mild and self-limited clinical manifestations. Non-specific signs and symptoms may include exanthema, low-grade fever, conjunctivitis, and arthralgia [1,2,3]. However, following ZIKV outbreaks in French Polynesia and Brazil, increase in cases of Guillain-Barré syndrome in adults and of congenital abnormalities in newborns were identified, and subsequent studies confirmed ZIKV infection during pregnancy as a cause of congenital neurological abnormalities [4, 5].
Due to the similarity in the initial clinical presentation between ZIKV infections and other infectious diseases, especially with other arboviral diseases that usually co-occur in tropical and sub-tropical regions, such as dengue (DENV) and chikungunya (CHIKV), clinical diagnosis is challenging, and often depends on laboratory confirmation. However, ZIKV laboratory diagnosis is difficult because viremia tends to be low [6]. In addition, ZIKV presents structural similarities with other flaviviruses, especially DENV, resulting in cross-reactive antibodies [1, 7]. Consequently, serological tests for ZIKV may cross-react with DENV, particularly when pre-existing immunity to DENV is present [7,8,9,10].
A correct differential diagnosis between ZIKV and other arboviral infections is critical to alert patients and clinicians for potentially evolving complications, as well as to guide appropriate supportive care (i.e. fluid replacement for severe dengue patients). In addition, an accurate ZIKV laboratory diagnosis can inform surveillance activities, which include detection and monitoring of virus circulation, estimation of disease burden, guiding preventive and control actions to interrupt virus transmission, and informing pregnant women on the risk of a gestational infection.
Objectives
In this study, we evaluated the diagnostic sensitivity of commercial enzyme-linked immunoassays (ELISAs) (Euroimmun, Lübeck, Germany) for detection of ZIKV IgM and IgG antibodies in sera of febrile patients with ZIKV infections. We also assessed the specificity of these kits in sera of both dengue-confirmed patients and blood donors.
Study design
Study site and design
This study was conducted and reported according to the STARD (Standards for Reporting of Diagnostic Accuracy) guideline [11]. The performance of the IgM- and IgG-ELISAs was evaluated using serum collections from clinical-epidemiological studies conducted in Salvador, northeast Brazil. Since DENV introduction in Salvador in 1995, the city has experienced periodic DENV epidemics [12]. Between 2011 and 2016, approximately 7000 dengue cases per year were reported in Salvador [13], but the actual disease burden has been estimated to be at least 12 times greater [14]. In early 2015, Salvador faced a large outbreak of acute exanthematous illness later attributed to ZIKV, with over 17,000 reported cases [3, 4].
Most of the serum samples used for our diagnostic test evaluation were obtained from an acute febrile illness (AFI) enhanced surveillance study that we conducted in a public emergency health unit of Salvador, between January 2009 and August 2016. Details were previously described [15]. Briefly, the surveillance study enrolled patients ≥5 years of age with reported fever or measured axillary temperature ≥ 37.8 °C of up to 7 days of duration. Self-reported data on days of symptoms and clinical characteristics were obtained from participants at enrollment.
We collected blood samples from participants at study enrollment (acute-phase sample) and ≥ 15 days post-enrollment (convalescent-phase sample). Sera were stored in aliquots at − 20 °C and − 70 °C for serologic and molecular testing, respectively. Acute-phase samples were tested for DENV by NS1- and IgM-ELISA (Panbio Dengue Early ELISA and Panbio Dengue IgM Capture, Panbio Diagnostics, Brisbane, Australia) and convalescent-phase samples by IgM-ELISA (Panbio Dengue IgM Capture, Panbio Diagnostics, Brisbane, Australia). Between 2009 and 2014, acute-phase samples that yielded a positive result in either ELISA underwent RNA extraction (Maxwell® 16 Total RNA Purification kit by Promega, Wisconsin, USA, or QIAmp® Viral RNA mini kit by Qiagen, Hilden, Germany) and RT-PCR (AccessQuick RT-PCR System, Promega, Madison,WI) for dengue typing [16]. Beginning in 2014, however, all acute-phase samples underwent RT-PCRs for DENV [16], ZIKV [17] and CHIKV [18]. Dengue IgG-ELISA (Panbio Dengue IgG Indirect ELISA, Panbio Diagnostics, Brisbane, Australia) was performed for all acute-phase serum samples of dengue-confirmed cases; those with a negative result were considered a primary dengue infection, whereas those with a positive result were considered secondary dengue infections.
Additionally, we obtained sera from presumably health volunteer blood donors at the State Blood Donation Center located in Salvador during December 2013. Collection of blood was performed after the regular screening process (which, among others, excludes donors reporting fever in the previous 15 days). Blood donors’ sera were stored in − 20° and subsequently tested for DENV with the same NS1-, IgM- and IgG-ELISA kits.
Sample selection
To determine the sensitivity of the ZIKV IgM- and IgG-ELISA (Anti-Zika Virus IgM ELISA and Anti-Zika Virus IgG ELISA, EUROIMMUN, Lübeck, Germany), we tested the available sera (14 acute-phase and 8 convalescent-phase serum samples) for the 14 patients enrolled during the surveillance study who had a ZIKV infection confirmed by RT-PCR (all of them recruited between May and July, 2015). To determine the specificity of the ZIKV IgM- and IgG-ELISA in a group of confirmed dengue patients, we selected from RT-PCR-positive dengue cases detected during the AFI surveillance study the first 20 cases positive for each DENV serotype. We selected the first 20 confirmed cases of each DENV type to ensure that there was no recognized ZIKV transmission in Salvador at the time, such that there was limited chance of a prior ZIKV infection. The selected DENV1-confirmed patients were detected from April 2009 to May 2011; the DENV2 from February 2009 to February 2010; and DENV4 from October 2010 to April 2011. DENV-3 patients were not selected for testing because we confirmed only a very small number of such cases during the study period. To augment the confidence that these DENV patients did not have a concomitant ZIKV infection, we also performed ZIKV RT-PCR on their acute-phase serum samples. We also determined the specificity of the ZIKV IgM- and IgG-ELISA in randomly selected sera from 23 blood donors. The initially planned number of samples from DENV-confirmed patients and blood donors (143 samples: 60 DENV acute- and convalescent-phase samples each and 23 blood donor samples) was defined to provide 95% confidence for an estimated specificity of 95% and a precision of ~ 3.5%.
Zika IgM- and IgG-ELISA testing
The ZIKV IgM-ELISA (El 2668–9601 M) and ZIKV IgG-ELISA (El 2668–9601 G) by Euroimmun (Lübeck, Germany) were performed according to the manufacturer’s instructions for semiquantitative interpretations. Although assay performers were not blinded to group identification of tested samples (ZIKV, DENV, or blood donors), reading was performed by automated microplate reader (TECAN, Maennedorf, Switzerland). Positive and negative controls were provided by the test’s manufacturer.
Data analysis
The AFI patients with a RT-PCR-based diagnosis of ZIKV or DENV were characterized according to demographic characteristics (sex and age) and clinical manifestations. We calculated the accuracy of ZIKV IgM- and IgG-ELISA tests, with respective 95% confidence intervals, using the samples from RT-PCR-confirmed cases of ZIKV infection as the reference group of positives for sensitivity estimation, and the samples from RT-PCR-confirmed dengue cases, as well as blood donors as reference groups of negatives for specificity estimation. We also calculated the specificity among dengue-confirmed cases stratified by the infecting DENV type and by the type of infection (primary versus secondary). Samples with equivocal ELISA results were excluded from the accuracy analysis.
Results
Participants characteristics
The 14 RT-PCR-confirmed Zika cases had a median age of 22.5 years and 42.9% were male. The most frequent clinical manifestations were headache (92.9%), myalgia (85.7%), retro-orbital pain (71.4%), rash (71.4%), and pruritus (71.4%) (Table 1). Median time between symptoms onset and acute- and convalescent-phase blood collection was 2.5 and 27 days, respectively (Table 1). The 60 RT-PCR-confirmed dengue cases had a median age of 18 years and 51.6% were male. The most frequent clinical manifestations were headache (96.7%), myalgia (76.7%), retro-orbital pain (56.7%), and arthralgia (46.7%) (Table 1). Contrasting with the Zika cases, only 10.0% of the dengue cases presented with rash. The median time between onset of symptoms and acute- and convalescent-phase blood collection was 2 and 27 days, respectively (Table 1). The RT-PCR-positive dengue cases were also positive by NS1-ELISA (10 patients), by NS1- and IgM-ELISA in the acute-phase sera (6 patients), by IgM-ELISA seroconversion between acute- and convalescent-phase sera (23 patients), and by NS1-ELISA and IgM-ELISA seroconversion (21 patients). Of the 60 RT-PCR-positive dengue cases, 47 had available serum to test by ZIKV RT-PCR and all of them (100.0%) were ZIKV negative.
For the Zika and dengue cases, the blood sample availability for ZIKV IgM- and IgG-ELISAs testing are also summarized in Table 1. The median age for the 23 blood donors was 32 years and 69.6% were male. All blood donors tested negative by dengue NS1- and IgM-ELISA, and 20 (87.0%) tested positive by DENV IgG-ELISA.
ZIKV IgM-ELISA performance
As expected, none of the 14 acute-phase samples of RT-PCR-confirmed Zika cases yielded a positive result in the ZIKV IgM-ELISA, whereas one of 8 convalescent-phase samples was positive (12.5% sensitivity; Table 2). Zika IgM-ELISA yielded a positive result in only one of the 140 non-Zika sera tested (99.3% specificity overall; Table 2). None of the blood donors and acute-phase sera from dengue cases tested positive in the ZIKV IgM-ELISA (100% specificity in both groups). Among the convalescent-phase sera from dengue cases, only one (from a patient with a primary infection with DENV-2) tested positive in the ZIKV IgM-ELISA (98.3% specificity).
Zika IgG-ELISA performance
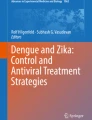
Of the 14 RT-PCR-confirmed Zika cases, 13 had had their acute-phase sera tested with the ZIKV IgG-ELISA and 6 (46.1%) were positive, 4 (30.8%) negative, and 3 (23.1%) equivocal (Table 3). All the 8 convalescent-phase samples from RT-PCR-confirmed Zika cases tested with the ZIKV IgG-ELISA were positive, yielding 100% sensitivity (Table 3). Among convalescent-phase sera from confirmed dengue cases, ZIKV IgG-ELISA yielded positive results in 40 (66.7%) samples, negative results in 15 (25.0%) samples, and equivocal results in 5 (8.3%) samples. Among the 23 sera from blood donors, 11 (47.8%) were positive in the ZIKV IgG-ELISA, 9 (39.1%) were negatives, and 3 (13.0%) generated equivocal results.
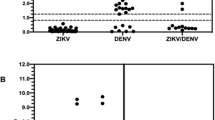
Overall, the specificity of the ZIKV IgG-ELISA for the 75 samples with valid results was 32.0%. The specificity for convalescent-phase samples of dengue patients was 27.3%, ranging for 5.9% in DENV-4 infections to 45.0% in DENV-1 infections (Table 3). The specificity was much lower for patients diagnosed secondary DENV infections (7.1%) compared to those with primary DENV infections (92.3%). Specificity of the Zika IgG-ELISA among blood donors was 45.0%. All 11 blood donors’ samples for which the ZIKV IgG-ELISA returned a positive result had anti-dengue IgG antibodies, as did 6 of the 9 blood donors samples that were negative on the ZIKV IgG-ELISA. The mean optical density value found on the DENV IgG-ELISA of blood donors with positive results on the ZIKV IgG-ELISA was 2.738 (standard deviation [SD]: 0.179, min. 2.307, max. 2.965), a value statistically greater than the mean found on blood donors with negative results on the ZIKV-IgG-ELISA (1.549, SD: 1.283, min. 0.036, max. 2.873; Wilcoxon rank-sum test P = 0.04).
Discussion
In this study, we evaluated the diagnostic performance of commercial IgM- and IgG-ELISAs for serodiagnosis of Zika virus infection. We used a set of sera collected from AFI patients prospectively enrolled in an enhanced surveillance study designed to detect arboviral infections, rather from a reference laboratory serum sample collection. Thus, we were able to characterize the clinical manifestations of the patients providing the sera tested, and to evaluate the accuracy of the tests in a group of patients’ samples that represent a realistic epidemiologic situation. Of note, clinical manifestations of RT-PCR-confirmed Zika and dengue AFI patients were similar, with the exception of rash, which was most commonly reported among Zika patients, reinforcing the difficulties in clinically differentiating these arboviral infections.
We found a high specificity for the Euroimmun ZIKV IgM-ELISA among both dengue-infected and blood donor control groups. Specificity among dengue controls was not affected by infecting serotype or prior dengue infection status. However, the sensitivity of the ZIKV IgM-ELISA was low for either acute- or convalescent-phase serum samples of Zika febrile patients (0.0 and 12.5%, respectively). As the time elapsed between Zika symptoms onset and acute-phase serum collection was short (median 2.5 days), a low IgM detection in the acute-phase sample was expected. However, even for the convalescent-phase serum samples, collected on average 3–6 weeks after disease onset, the ZIKV IgM-ELISA yielded a low sensitivity. This low performance was also reported for RT-PCR-confirmed Zika samples from residents from other ZIKV- and DENV-endemic areas (Suriname, Dominican Republic and Colombia), where Euroimmun Zika IgM-ELISA detected 6 of the 19 evaluated samples collected ≥1 days post onset of symptoms (dpos) and 5 of 12 samples collected ≥6 dpos, yielding sensitivities of 31.6 and 41.7%, respectively [19]. Interestingly, the same study reported sensitivities of 87.5 and 100.0% among RT-PCR-confirmed Zika samples from returning travelers with ≥1 dpos and ≥ 6 dpos, respectively, suggesting that previous flavivirus infections may alter ZIKV antibody responses.
Although recent studies suggest a high specificity of this Zika IgG-ELISA against dengue infections in returning travelers [19,20,21,22], we have demonstrated an overall low performance in a dengue-endemic region. This may be due to a greater frequency of secondary DENV infections in the population we studied (78.3%), in which specificity was 7.1% contrasting with 92.3% in primary infections. The low specificity of the Zika IgG-ELISA among our blood donor control group may be also explained by the high frequency (87.0%) of DENV IgG antibodies observed in this group. We also found a large difference in the ZIKV IgG-ELISA specificity among DENV-confirmed samples according to DENV serotype, varying from 5.9% in DENV4-infected patients to 45.0% in DENV1-infected patients. This difference is likely explained by the prior dengue-immune status of these patients, since 100% of DENV4-infected patients had secondary infections, contrasting with 65% of DENV1-infected patients. Although ZIKV IgG antibodies were detected in all 8 convalescent-phase samples of Zika cases, the same samples were also positive for dengue IgG antibodies, making it impossible to exclude cross-reactions.
The main limitation of our study was the small number of ZIKV-confirmed cases. Technical difficulties in ZIKV diagnosis, especially due to the low viremia during infection and the cross-reactions with other circulating arboviruses in tropical and subtropical regions, has hampered composing large subsets of Zika cases’ samples to be used in diagnostic test accuracy studies. As another limitation, we did not perform ZIKV RT-PCR on the acute-phase samples of all dengue cases to ensure the absence of co-infection. Even though, sufficient serum was available to perform RT-PCR in 47 of the 60 dengue cases, and none of them yielded a positive result. Considering that our dengue case selection specifically included patients with infections that occurred prior to 2012, it is unlikely that they had a dengue and Zika co-infection or a prior ZIKV infection, because ZIKV introduction into Brazil was estimated to have occurred between late 2012 and early 2013 [23,24,25]. In addition, prior ZIKV infections in the study group of blood donors cannot be completely ruled out because their serum samples were obtained in December 2013; but, as the ZIKV spread in Salvador was clearly recognized during a large outbreak in 2015, it is improbable that these individuals had ZIKV infections before study enrollment.
Strengths of our study included the use of RT-PCR as a confirmation criterion for both Zika and dengue cases because as ZIKV and DENV transmission are endemic in our setting, a molecular diagnosis ensures a more accurate distinction between these flaviviruses compared to serologic diagnosis. In addition, the availability of paired sera provided a unique opportunity to evaluate the performance of commercial ZIKV IgM- and IgG-ELISAs in detection of antibodies in acute- and convalescent-phase samples.
Conclusion
In conclusion, our study revealed a high specificity but low sensitivity of the Euroimmun ZIKV IgM-ELISA in an endemic region for both dengue and Zika, as well as a high specificity of the Euroimmun ZIKV IgG-ELISA in DENV primary infections contrasting with low specificity in DENV secondary infections. This suggests that this IgG-ELISA may be more suitable for Zika diagnosis in travelers returning from non-endemic areas than for serosurveys in endemic areas. Further studies with larger well-characterized samples are needed to assess the diagnostic accuracy not only of this test, but also of several others serological ZIKV assays.
References
Duffy MR, Chen T-H, Hancock WT, Powers AM, Kool JL, Lanciotti RS, et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. N Engl J Med. 2009;360:2536–43.
Musso D, Gubler DJ. Zika Virus. Clin Microbiol Rev [Internet]. 2016;29:487–524. Available from: http://cmr.asm.org/content/29/3/487.
Cardoso CW, Paploski IAD, Kikuti M, Rodrigues MS, Silva MMO, Campos GS, et al. Outbreak of Exanthematous Illness Associated with Zika, Chikungunya, and Dengue Viruses, Salvador, Brazil. Emerg Infect Dis J [Internet]. 2015;21:2274–6. Available from: http://wwwnc.cdc.gov/eid/article/21/12/15-1167
Paploski IAD, Prates APPB, Cardoso CW, Kikuti M, Silva MMO, Waller LA, et al. Time Lags between Exanthematous Illness Attributed to Zika Virus, Guillain-Barré Syndrome, and Microcephaly, Salvador, Brazil. Emerg Infect Dis J [Internet]. 2016;22 Available from: http://wwwnc.cdc.gov/eid/article/22/8/16-0496
Cao-Lormeau V-M, Blake A, Mons S, Lastère S, Roche C, Vanhomwegen J, et al. Guillain-Barré syndrome outbreak associated with Zika virus infection in French Polynesia: a case-control study. Lancet Elsevier. 2016;387:1531–9.
Musso D, Rouault E, Teissier A, Lanteri MC, Zisou K, Broult J, et al. Molecular detection of Zika virus in blood and RNA load determination during the French Polynesian outbreak. J Med Virol [Internet]. 2016;9999:1–6. Available from: http://dx.doi.org/10.1002/jmv.24735
Lanciotti RS, Kosoy OL, Laven JJ, Velez JO, Lambert AJ, Johnson AJ, et al. Genetic and serologic properties of Zika virus associated with an epidemic, yap state, Micronesia, 2007. Emerg Infect Dis. 2008;14:1232–9.
Dejnirattisai W, Supasa P, Wongwiwat W, Rouvinski A, Barba-Spaeth G, Duangchinda T, et al. Dengue virus sero-cross-reactivity drives antibody-dependent enhancement of infection with zika virus. Nat Immunol [Internet]. Nature Publishing Group, a division of Macmillan Publishers Limited. All Rights Reserved.; 2016;17:1102–8. Available from: https://doi.org/10.1038/ni.3515
Felix AC, Souza NCS, Figueiredo WM, Costa AA, Inenami M, da Silva RMG, et al. Cross reactivity of commercial anti-dengue immunoassays in patients with acute Zika virus infection. J Med Virol [Internet]. 2017;89:1477–1479. Available from: https://doi.org/10.1002/jmv.24789
Priyamvada L, Quicke KM, Hudson WH, Onlamoon N, Sewatanon J, Edupuganti S, et al. Human antibody responses after dengue virus infection are highly cross-reactive to Zika virus. Proc Natl Acad Sci [Internet]. 2016;113:7852–7. Available from: http://www.pnas.org/content/113/28/7852.
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig L, et al. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ [Internet]. 2015;351:h5527. Available from: https://www.bmj.com/content/351/bmj.h5527.long.
Teixeira M da G, Costa M da CN, Barreto ML, Barreto FR. Epidemiologia do dengue em Salvador-Bahia,1995–1999. Rev Soc Bras Med Trop [Internet]. 2001;34:269–274. Available from: https://doi.org/10.1590/S0037-86822001000300007.
BRASIL. Dengue: Notificações registradas no Sistema de Informação de Agravos de Notificação – SINAN, Brazil. [Internet]. 2017 [cited 2017 Oct 24]. Available from: http://www.tabnet.saude.salvador.ba.gov.br/tabcgi.exe?sinan_online/dengueneton.def
Silva MMO, Rodrigues MS, Paploski IAD, Kikuti M, Kasper AM, Cruz JS, et al. Accuracy of Dengue Reporting by National Surveillance System, Brazil. Emerg Infect Dis J [Internet]. 2016;22:336. Available from: http://wwwnc.cdc.gov/eid/article/22/2/15-0495
Kikuti M, Cunha GM, Paploski I a. D, Kasper AM, Silva MMO, Tavares AS, et al. Spatial distribution of dengue in a Brazilian urban slum setting: role of socioeconomic gradient in disease risk. PLoS Negl Trop Dis [Internet]. 2015;9:e0003937. Available from: http://dx.plos.org/10.1371/journal.pntd.0003937
Lanciotti RS, Calisher CH, Gubler DJ, Chang GJ, Vorndam AV. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. J Clin Microbiol [Internet]. 1992/03/01 ed. 1992;30:545–51. Available from: http://jcm.asm.org/content/30/3/545.long.
Balm MND, Lee CK, Lee HK, Chiu L, Koay ESC, Tang JW. A diagnostic polymerase chain reaction assay for Zika virus J Med Virol [Internet]. 2012;84:1501–1505. Available from: http://doi.wiley.com/10.1002/jmv.23241
Edwards CJ, Welch SR, Chamberlain J, Hewson R, Tolley H, Cane PA, et al. Molecular diagnosis and analysis of Chikungunya virus. J Clin Virol [Internet]. 2007;39:271–275. Available from: http://linkinghub.elsevier.com/retrieve/pii/S1386653207001850
Steinhagen K, Probst C, Radzimski C, Emmerich P, Van EM, Schinkel J, et al. Serodiagnosis of Zika virus ( ZIKV ) infections by a novel NS1-based ELISA devoid of cross-reactivity with dengue virus antibodies : a multicohort study of assay performance, 2015 to 2016. Euro Surveill. 2016;21:30426.
Van EM, Meersman K, Michiels J, Ariën KK, Van Den BD. Letter to the editor : specificity of Zika virus ELISA : interference with malaria. Euro Surveill. 2016;21:3–4.
Huzly D, Hanselmann I, Panning M. High specificity of a novel Zika virus ELISA in European patients after exposure to different flaviviruses. Euro Surveill. 2016;21:1–4.
Lustig Y, Zelena H, Venturi G, Van Esbroeck M, Rothe C, Perret C, et al. Sensitivity and Kinetics of an NS1-Based Zika Virus Enzyme-Linked Immunosorbent Assay in Zika Virus-Infected Travelers from Israel, the Czech Republic, Italy, Belgium, Germany, and Chile. J Clin Microbiol [Internet]. 2017;55 :1894–901. Available from: http://jcm.asm.org/content/55/6/1894.
Faria NR, Azevedo R d. S d. S, Kraemer MUG, Souza R, Cunha MS, Hill SC, et al. Zika virus in Americas: Early epidemiological and genetic findings. Science (80- ) [Internet]. 2016;352:345–9. Available from: http://www.sciencemag.org/cgi/doi/10.1126/science.aaf5036
Ayllón T, Campos R de M, Brasil P, Morone FC, Câmara DCP, Meira GLS, et al. Early Evidence for Zika Virus Circulation among <em>Aedes aegypti</em> Mosquitoes, Rio de Janeiro, Brazil. Emerg Infect Dis J [Internet]. 2017;23:1411. Available from: http://wwwnc.cdc.gov/eid/article/23/8/16-2007
Passos SRL, Santos MAB dos, Cerbino-Neto J, Buonora SN, Souza TML, Oliveira RVC de, et al. Detection of Zika Virus in April 2013 Patient Samples, Rio de Janeiro, Brazil. Emerg Infect Dis J [Internet]. 2017;23:2120. Available from: http://wwwnc.cdc.gov/eid/article/23/12/17-1375
Acknowledgements
We thank Moyra M. Portilho, Caroline X. Carvalho, Paula S. Barbosa, Rejane H. Carvalho, and Gabriela S. Menezes for their laboratory assistance, Renan Rosa for his data management support, the health professionals from Centro de Emergência São Marcos, Pau da Lima, Salvador, Brazil, and all subjects of this study.
Funding
This study was supported by the Brazilian National Council for Scientific and Technological Development (grant 550160/2010–8 to MGR, grants 400830/2013–2 and 440891/2016–7 to GSR; and scholarships to IADP, UK, MGR, and GSR); the Bahia Foundation for Research Support (grant PNX0010/2011 to MGR, grants PPP0055/2011, JCB0020/2013, PET0026/2013, APP0044/2016, and PET0022/2016 to GSR); and the Coordination for the Improvement of Higher Education Personnel, Brazilian Ministry of Education (grant 440891/2016–7 to GSR and scholarship to MK). The funding sources had no role in study design; in the collection, analysis and interpretation of data; in the writing of the paper; and in the decision to submit the article for publication.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
MK, IADP, and GSR conceived the study and oversaw its preparation and writing; MK, and GSR wrote first draft of the manuscript; MK, LBT, PSSM, and GCS performed laboratory tests; MK and IADP analyzed the data; MK, LBT, PSSM, GCS, IADP, SCW, MGR, UK, and GSR participated in the discussion of the study and critical reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This project was approved by the Research Ethics Committee at the Gonçalo Moniz Institute, Oswaldo Cruz Foundation. All adult subjects provided written informed consent. Participants < 18 years old who could read provided written assent following written consent from their parent or guardian. All study data were anonymized before analysis.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kikuti, M., Tauro, L.B., Moreira, P.S.S. et al. Diagnostic performance of commercial IgM and IgG enzyme-linked immunoassays (ELISAs) for diagnosis of Zika virus infection. Virol J 15, 108 (2018). https://doi.org/10.1186/s12985-018-1015-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12985-018-1015-6