
Abstract
Background
In Ethiopia, there is lack of data on the prevalence of hepatitis B virus (HBV), hepatitis C virus (HCV) and human immune deficiency virus (HIV) infections in adult population at community level. This study aimed at determining the HBV, HCV and HIV seroprevalence in adult population at community level in East and West Gojjam zones in Amhara region, Ethiopia.
Methods
A cross-sectional study was conducted between October 01 and November 30, 2015. The Hepatitis B surface antigen (HBsAg) and anti-HCV were detected using the standard serological tests. The antibody to HIV infection was tested using the national HIV rapid tests algorithms.
Results
A total of 481 adults comprised of 51% females with median age of 25 years took part in the study. Overall, 7.5% (95% CI: 5.5–10.2%) of adult population were infected either with HBV, HCV and HIV. The prevalence of HBV was 15 (3.1%) and for HIV was 16 (3.3%). The seroprevalence of HCV was five (1.0%). HIV-HCV co-infection was found to be two (0.4%). HIV prevalence was higher in non-educated population than their counter parts (P = 0.001). HIV prevalence was high in housewives (6.0%) and merchants (4.7%).
Conclusions
This study revealed an intermediate HBV prevalence and low prevalence of HCV in adult population at community level. HIV prevalence is still a major public health problem in the area. To have the national data, we recommend further study on genotypes of HBV and HCV including local risk factors for transmissions. Moreover, health education on HBV, HCV and HIV transmission should be an intervention measure in the community.
Similar content being viewed by others


Backgrounds
Infection with HBV, HCV and HIV are still a major public health problem worldwide, particularly in developing countries [1]. HBV and HCV infections can cause both acute and chronic liver disease, including cirrhosis and hepatocellular carcinoma (HCC). Studies showed that 80% of HCC was caused by active replication of chronic HBV and HCV infections [2, 3]. For instance, about 686, 000 people die every year due to complications of HBV infection (cirrhosis and HCC) [4].
According to the World Health Organization (WHO) report, 34 million people are HIV positive worldwide [5]. In Ethiopia, the prevalence of HIV infection differs significantly among regions and different population groups. WHO estimated that 753,100 people are living with HIV in Ethiopia [6, 7]. However, the national HIV prevalence declined from 1.5 to 1.1% in 2015 [6, 7]. Urban populations are more affected with HIV than rural areas while females are twice affected than male population [6]. Globally, about 400 million and 170 million people are chronically infected with HBV and HCV, respectively [8]. Approximately 1 million people die each year from hepatitis B and C virus infections [9].
In Ethiopia, there is lack of information on the prevalence of HBV, HCV and HIV in the general population. This is due to the fact that virtually all prevalence data on HBV, HCV and HIV have been obtained in selected group of people with risk factors such as pregnant women, military personnel and patients with liver disease [10–12]. For instance, the prevalence of HBV and HCV in pregnant women was between 4.4 and 0.26%, respectively [13]. Therefore, the prevalence of HBV, HCV and HIV infections at the community level is not known. The present study was therefore conducted to determine the prevalence of HBV, HCV and HIV infections among adults at house hold level in the community in East and West Gojjam zones in Amhara region, Ethiopia.
Methods
Study design and period
We conducted a community-based cross sectional study in East and West Gojjam administrative zones in Amhara region between October 01 and November 30, 2015. From each household, only one adult who gave consent to participate in the study were involved in the study.
Source and study population
The source population was all apparently healthy adult population in East and West Gojjam Zones in the Amhara region. Apparently healthy adults with age ≥ 18 years of both sexes from the selected households in the study area were deemed a study population.
Sample size and sampling
The sample size was calculated using single population proportion formula. It was calculated by taking a proportion of 0.5 by assuming that the mean (μ) population for each parameter is known to be 50%, 2% marginal error, and 95% confidence levels. Therefore, the sample size of 481 was determined. The households from each district were selected using systematic random sampling technique after getting the nth value by dividing the total number of households with the total number of selected households.
Data collection
Trained laboratory technicians interview study participants and collected data on demographic, monthly income, education and marital status were collected by face to face interview using a structured questionnaire.
Detection of HBsAg and anti-HCV and anti-HIV
Trained laboratory technicians collected 5 ml of whole blood aseptically from vein by puncture. The collected blood was allowed to clot then serum was separated by centrifugation at room temperature. Antibody to HIV infection was tested using the national HIV rapid diagnostic tests algorithm. Initially, HIV infection was screened using KHB (Bio-Engineering, Shanghai, Kehua). The HIV positive samples were re-tested with STAT PAK (Chembio diagnostic, Newyork, USA). HIV positive serums which showed discordant results between the first test (KHB) and the second test (STAT PAK) were tested with Unigold (Trinity Biotech Bray, Ireland) as tie breaker.
The presence of hepatitis B surface antigens (HBsAg) in serum was detected using advanced quality One Step Rapid Test per instructions of the manufacturer (Zhejiang Orient Gene Biotech, Zhejiang, China). The anti-HCV antibody was detected using One Step Rapid Test per instructions of the manufacturer (Zhejiang Orient Gene Biotech, Zhejiang, China). The samples found to be positive for HBV and HCV had been re-tested in duplicate. The HIV positive samples were re-tested with STAT PAK per the manufacturers’ instruction. To ensure the reliability and quality of data, positive and negative control sera were run following the manufacturer recommendations alongside the test kits.
Data analysis
Data was entered into Statistical Package for Social Science (IBM Corp. Released 2011. IBM SPSS Statistic Armonk, NY: IBM Corp). A categorical variable were tested using the Chi-square tests. All statistical tests were two-tailed, and the significance level was set at P < 0.05.
Ethical clearance
The Research Ethics Review Committee of the College of Medicine and Health Sciences of Bahir Dar University has approved the ethical clearance. Written consent was obtained from each study participants to provide blood for HBV, HCV and HIV determination for research purpose. The study participants found to be positive for HBV, HCV and HIV were reported to physicians and/or health officers for treatment and counselling. Information obtained at any course of the study was kept confidential.
Results
Socio-demographic profiles
A total of 481 adults comprised of 245 (51%) of females and 236 (49%) males from the community participated in the study. The median age of the study participants was 25 years (ranged 18–60 years). Assessment of education showed that 153 (31.8%) of the participants did not have formal education. The majority (97.1%) of participants were urban residents. Table 1 depicts the marital status, monthly income and occupation of the study participants.
Prevalence of HBV, HCV and HIV infection
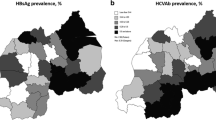
Overall, 7.5% (95% CI: 5.5–10.2%) of adult population at the community were infected either with hepatitis B or C viruses and HIV. Of these, HBV prevalence accounted for 3.1%. The seroprevalence of HCV was 5 (1.0%). The prevalence of HIV was 3.3%. In this study, only two (0.4%) adults were co-infected with HCV and HIV. However, HBV and HIV co-infection was not found. Table 2 illustrated the prevalence of HBV, HCV and HIV infections.
Risk factor for HBV, HCV and HIV prevalence
In the present study, no statistical significant differences were observed for HBV and HCV infections in terms of age, sex, residence and marital status. However, HIV prevalence was in higher in females than males (P = 0.001). Furthermore, HIV prevalence was higher in non-educated population than their counter parts (P = 0.001) (Table 3). Considering occupations of adults, HIV prevalence was higher in merchants (4.7%) than others.
Discussion
This study showed the prevalence of HBV, HCV and HIV infections among adult population at the community level. Overall, 7.5% of the adult population was infected either with hepatitis B or C viruses and HIV. This indicated that HBV, HCV and HIV infections are the major public health problems in Ethiopia. HIV prevalence in the present study (3.3%) is higher than the national adult HIV prevalence which is 1.1% [14]. Furthermore, HIV prevalence in females (5.2%) was higher than the national HIV prevalence among females (1.4%) [3]. Like other reports, the prevalence of HIV was significantly higher in females than males (P = 0.001) [14–16].
In this study, a statistically significant association was observed between HIV prevalence and educational levels. HIV prevalence was higher among non-educated adults (P = 0.001). Likewise, studies indicated that HIV prevalence in developing countries was higher among less educated groups [8, 17]. It is well documented that in the early stage of HIV pandemic, the prevalence of HIV infection was higher among well educated people in urban areas than non-educated people. However, in later stage, due to the availability of information on prevention of HIV transmission, it decreases in educated people [17]. Furthermore, the prevalence of HIV was higher in merchants. This conforms to a study conducted in Ethiopia which stated that merchants had higher odds of being HIV positive than others [18].
This study showed an intermediate (3.1%) prevalence of HBV in adults at community level compared to 5–10% HBV prevalence in adult population in sub-Saharan Africa [9]. Likewise, a study conducted in Libya reported 2.2% HBV prevalence in a general population [19]. In contrast, it is lower compared to other studies conducted in various part of Ethiopia. For instance, 3.8 to 4.4% of HBV prevalence was reported among pregnant women and military person [10, 13, 20]. A statistically significant association was not observed between HBV positive and risk factors. Although, it was not statistically significant, adults with low monthly income (<500 birr) had higher HBV prevalence (3.7 vs 1.9%) compared to those adults with better income (P = 0.22).
Hepatitis C virus (HCV) prevalence in adult population was low (1.0%). Similarly, low prevalence (0.6 to 0.7%) of HCV was reported in pregnant women [11, 21]. In contrast, higher prevalence of HCV was documented among attendants of voluntary counseling and testing for HIV in Ethiopia. For instance, 9.1, 6.0 and 4.3% HCV prevalence were reported in Hawassa, Mekelle and Adwa, respectively [22–24]. This clearly showed that HCV in the general population is low while higher in risk group of the population.
People with HIV infection are often co-infected with chronic viral hepatitis by HBV and HCV due to common modes of transmission. Two (0.4%) adults were co-infected by HCV and HIV. However, a study conducted on selected risk group of people reported higher co-infection of HIV-HBV (34%), HIV-HCV (8.0%) and HBV-HCV (2%) [25]. Moreover, 5.6% HIV-HBV and 5% HIV-HCV co-infections were documented in HIV positive individuals [26]. These differences might be due to the study population differences. The Quantative-real time polymerase chain reaction (qRT-PCR) was not used to confirm the positive samples. Therefore, this deemed to be a certain limitation for this study.
Conclusion
This study showed an intermediate prevalence for HBV and low for HCV in adult population at community level. However, HIV prevalence was higher in non-educated adults at community levels. We recommend further national wide studies on the prevalence and genotypes of HBV and HCV including risk factors in the general population.
Abbreviations
- HbsAg:
-
Hepatitis B surface antigen
- HBV:
-
Hepatitis B virus
- HCV:
-
Hepatitis C virus and HIV human immune deficiency virus
- HHC:
-
Hepatocellular carcinoma
References
United Nation program on HIV/AIDS. AIDS epidemic update. Switzerland: WHO; 2009.
Karoney MJ, Siika AM. Hepatitis C virus (HCV) infection in Africa: a review. Pan Afr Med J. 2013;14:44.
Bane A, Patil A, Khatib M. Healthcare cost and access to care for viral hepatitis in Ethiopia. IJIAS. 2014;9(4):1718–23.
Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013. A systematic analysis for the Global Burden of Disease Study 2013. The Lancet. 2015;385:117 171. doi:http://dx.doi.org/10.1016/S0140-6736(14)61682-2.
World Health Organization. Global HIV/AIDS Response – Epidemic update and health sector progress towards universal access-Progress report. 2011. WHO, Geneva. http://www.who.int/. Accessed Jan 2017
HIV/AIDS Estimate and projections in Ethiopia, 2011–2016. www.etharc.org. Accessed 20 Nov 2016.
World Health Organization. HIV/AIDS progress in 2014. Update March 2015. Geneva: WHO. http://www.who.int/. Accessed Jan 2017
Lai CL, Ratziu V, Yuen MF, Poynard T. Viral hepatitis B. Lancet. 2003;362:2089–94.
World Health Organization (WHO). Hepatitis B updates 2016. http://www.who.int/mediacentre/factsheets/fs204/en/. Accessed 22 Oct 2016.
Zenebe Y, Mulu W, Yimer M, Abera B. Sero-prevalence and risk factors of hepatitis B virus and human immunodeficiency virus infection among pregnant women in bahir Dar city, northwest Ethiopia: a cross sectional study. BMC Infect Dis. 2014;14:118. doi:10.1186/1471-2334-14-118.
Abate M, Wolde T. Seroprevalence of human immunodeficiency virus, hepatitis B virus, hepatitis C virus, and syphilis among blood donors at jigjiga blood bank, eastern Ethiopia. Ethiop J Health Sci. 2016;26(2):153–60.
Abera B, Zenebe Y, Mulu W, Kibret M, Kahsu G. Seroprevalence of hepatitis B and C viruses and risk factors in HIV infected children at the felgehiwot referral hospital, Ethiopia. BMC Res Notes. 2014;7:838.
Molla S, Munshea A, Nibret E. Seroprevalence of hepatitis B surface antigen and anti HCV antibody and its associated risk factors among pregnant women attending maternity ward of felege hiwot referral hospital, northwest Ethiopia: a cross-sectional study. Virol J. 2015;12:204.
HIV/AIDS Estimate and projections in Ethiopia: 2011–2016. www.etharc.org. Accessed 15 Nov 2016.
Mulu W, Abera B, Yimer M. Prevalence of human immunodeficiency virus infection and associated factors among students at bahir Dar university. Ethiop J Health Dev. 2014;28(3):170–7.
Federal Ministry of Health (FMOH). Country progress report on HIV/AIDS response. Addis Ababa: National HIV/AIDS Prevention and Control office; 2012.
Hargreaves JR, Glynn JR. Educational attainment and HIV-1 infection in developing countries: a systematic review. Trop Med Int Health. 2002;7:489–98.
Lakew Y, Benedict S, Haile D. Social determinants of HIV infection, hotspot areas and subpopulation groups in Ethiopia: evidence from the national demographic and health survey in 2011. BMJ Open. 2015;5:e008669. doi:10.1136/bmjopen-2015-008669.
Daw MA, El-Bouzedi A. Prevalence of hepatitis B and hepatitis C infection in Libya: results from a national population based survey. BMC Infect Dis. 2014;14:17.
Birku T, Gelaw B, Moges F, Assefa A. Prevalence of hepatitis B and C viruses infection among military personnel at bahir Dar armed forces general hospital, Ethiopia. BMC Res Notes. 2015;8:737.
Zenebe Y, Mulu W, Yimer M, Abera B. Sero-prevalence and risk factors of hepatitis C virus infection among pregnant women in bahir Dar city, northwest Ethiopia: cross sectional study. Pan Afr Med J. 2015;21:158. doi:10.11604/pamj.2015.21.158.6367.
Alemayehu A, Tassachew Y, Sisay Z, Shimelis T. Prevalence and risk factors of hepatitis C among individuals presenting to HIV testing centers, hawassa city, southern Ethiopia. BMC Res Notes. 2011;4:193.
Hadush H, Gebre-Selassie S, Mihret A. Hepatitis C virus and human immunodeficiency virus coinfection among attendants of voluntary counseling and testing centre and HIV follow up clinics in mekelle hospital. Pan Afr Med J. 2013;14:107. doi:10.11604/pamj.2013.14.107.2302.
Atsbaha AH, Dejen TA, Belodu R, Getachew K, Saravanan M, Wasihun AG. Sero‑prevalence and associated risk factors for hepatitis C virus infection among voluntary counseling testing and anti retroviral treatment clinic attendants in Adwa hospital, northern Ethiopia. BMC Res Notes. 2016;9:121.
Tessema B, Yismaw G, Kassu A, Amsalu A, Mulu A, Emmrich F, et al. Seroprevalence of HIV, HBV, HCV and syphilis infections among bloo donors at Gondar university teaching hospital, northwest Ethiopia: declining trends over a period of five years. BMC Infect Dis. 2010;10:111.
Wondimeneh Y, Alem M, Asfaw F, Belyhun Y. HBV and HCV seroprevalence and their correlation with CD4 cells and liver enzymes among IV positive individuals at university of Gondar teaching hospital, northwest Ethiopia. Virol J. 2013;10:171.
Acknowledgements
The authors deeply acknowledge all the study participants for their willingness to be part of the study group. We also thank the support of Bahir Dar Regional Health Research Laboratory Centre for facilitating the research process.
Funding
This study was financed by Biotechnology Research Institute of Bahir University.
Availability of data and materials
Please request the author for data and materials related to this manuscript via bayeabera15@gmail.com.
Authors’ contributions
BA: Conceived the research idea, designed the study, analyzed data and write up the manuscript. YA: Involved in data collection.WM: designed the study, proposed the research idea, and involved in data entry. MY, YZ and ZM: involved in study design and collected data and proposed the research idea. All authors revised the manuscript and approved for publication.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The Research Ethics Review Committee of the College of Medicine and Health Sciences of Bahir Dar University has approved the ethical clearance. We obtained written informed consent from all study participants to provide blood for HBV, HCV and HIV determination to participate in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Abera, B., Adem, Y., Yimer, M. et al. Community seroprevalence of hepatitis B, C and human immunodeficiency virus in adult population in gojjam zones, northwest Ethiopia. Virol J 14, 21 (2017). https://doi.org/10.1186/s12985-017-0696-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12985-017-0696-6