
Abstract
Background
Damage to the central nervous system during HIV infection can lead to variable neurobehavioral dysfunction termed HIV-associated neurocognitive disorders (HAND). There is no clear consensus regarding the neuropathological or cellular basis of HAND. We sought to study the potential contribution of aging to the pathogenesis of HAND. Aged (range = 14.7–24.8 year) rhesus macaques of Chinese origin (RM-Ch) (n = 23) were trained to perform cognitive tasks. Macaques were then divided into four groups to assess the impact of SIVmac251 infection (n = 12) and combined antiretroviral therapy (CART) (5 infected; 5 mock-infected) on the execution of these tasks.
Results
Aged SIV-infected RM-Ch demonstrated significant plasma viremia and modest CSF viral loads but showed few clinical signs, no elevations of systemic temperature, and no changes in activity levels, platelet counts or weight. Concentrations of biomarkers of acute and chronic inflammation such as soluble CD14, CXCL10, IL-6 and TNF-α are known to be elevated following SIV infection of young adult macaques of several species, but concentrations of these biomarkers did not shift after SIV infection in aged RM-Ch and remained similar to mock-infected macaques. Neither acute nor chronic SIV infection or CART had a significant impact on accuracy, speed or percent completion in a sensorimotor test.
Conclusions
Viremia in the absence of a chronic elevated inflammatory response seen in some aged RM-Ch is reminiscent of SIV infection in natural disease resistant hosts. The absence of cognitive impairment during SIV infection in aged RM-Ch might be in part attributed to diminishment of some facets of the immunological response. Additional study encompassing species and age differences is necessary to substantiate this hypothesis.
Similar content being viewed by others

Background
Combined antiretroviral therapy (CART) has completely or almost completely suppressed HIV replication translating to significant reductions in mortality and morbidity in infected individuals. Along with better long-term outcomes and decreased frequency of AIDS-related illness among HIV-infected patients taking suppressive CART, deaths attributable to HIV infection have decreased by 48% since the peak in 2005 [1]. Nevertheless, non-AIDS defining illnesses including neurocognitive deficits normally associated with aging are often observed in the HIV-infected population.
The term HIV-Associated Neurocognitive Disorders (HAND) is used to describe a spectrum of clinical disorders ranging from asymptomatic neurocognitive impairment to mild neurocognitive disorder to HIV-associated dementia (HAD), the clinical correlate of HIV encephalitis [2]. Although CART has been found to prevent or delay these neurocognitive sequelae, less severe neurocognitive dysfunction remains a common comorbidity. Anywhere from 25 to 50% of the HIV-infected population on successful long-term CART experience mild-moderate HAND [3,4,5,6,7,8,9] and as this population ages, they are two to seven times more likely to have mild cognitive impairment than their seronegative peers [10,11,12,13,14]. Other comorbidities and behavioral traits have been reported to be risk factors for HAND such as cardiovascular-related conditions [15, 16], obesity [17], diabetes [16, 17], hyperlipidemia [16], tobacco use [16], hepatitis C co-infection [18], alcohol and substance abuse [14, 19], education [20, 21], poverty [21], sleep disorders [14], and psychiatric comorbidities [14]. Many of these conditions are typically associated with aging and contribute to the assumption that HIV-infected individuals undergo a premature aging process. This theory has much traction, but it has been questioned whether available data support the theory of accelerated aging [22]. Regardless, the risk of developing HAND is likely confounded by many of these variables and will be challenging to tease apart, especially with older age.
We know little about the pathogenesis of HAND and why it persists in the presence of CART [23]. Before CART was introduced, HAD was associated with increased HIV RNA in the cerebrospinal fluid (CSF) in patients with severe immunosuppression, arguing for a direct effect due to viral replication in the central nervous system (CNS) [24,25,26,27]. However, in populations with access to CART, there is no strong correlation between HIV RNA in the CSF and neurocognitive impairment [28, 29]. Together, these observations suggest that a constellation of immune and viral processes contributes to cognitive dysfunction. Potential mechanisms include comorbidities, “hit and run” effect of HIV entering the CNS early and causing long term neurodegenerative damage [30,31,32,33,34], chronic inflammation in the periphery and/or CNS, substance abuse, age and CART neurotoxicity.
HIV-infected individuals experience complications associated with age earlier than non-infected individuals [35]. Treated HIV-infected individuals experience chronic inflammation, hypercoagulation, and an increased risk of non-AIDS-related morbidity and mortality [36]. There are few preclinical models that can address the cellular and system bases of age-related neurocognitive dysfunction during HIV infection. Since non-human primate (NHP) brains are highly concordant with cortical and subcortical architecture of humans, they can be employed to study neurological abnormalities and neuropathogenesis in conjunction with aging. Human and NHP have different but comparable lifespans where the effects of aging on complex immune and nervous system function can be studied. Thus, SIV infection of NHPs offers a valid model to study the effects of aging and chronic lentiviral infection.
To model the less severe forms of HAND, we trained aged Chinese-origin rhesus macaques (RM-Ch) to perform cognitive tests and then assigned them to four performance-matched experimental groups. Half of the RM-Ch were then infected with SIVmac251. Cognitive function along with clinical and virological assessments were followed for 8 months, at which point half of the infected and half of the mock-infected RM-Ch were administered CART for an additional 6 months. Since RM-Ch are reported to have lower viremic peaks and set points, greater maintenance of CD4 T cell counts, and significantly longer survival times than rhesus macaques of Indian origin [37,38,39], we anticipated a slow disease progression that could recapitulate neurological abnormalities observed during HIV infection.
Methods
Subjects
Aged (13.5–23.5 year at beginning of study) female rhesus macaques of Chinese origin (n = 23) (RM-Ch) with no previous behavioral training were used for the present study. Macaques were housed and maintained according to American Association of Laboratory Animal Care standards. The University of Pittsburgh’s Institutional Animal Care and Use Committee approved all experimentation. Following acquisition, animals were habituated to pole and collar handling and placement in a behavioral primate chair (Primate Products, Immokalee, FL). Collars were fitted with compact accelerometers (Actical, Philips Respironics, Murrysville, PA) to detect sleep and activity patterns. Temperature sensor monitors (DST micro-T temperature logger, Star-Oddi, Iceland) were implanted in the mid-scapular region. To learn to accept water reinforcement rewards, subjects were trained to use a sipper tube attached to the chair. Water was regulated 7 days/week and supplemented (weekly average of 20 ml/kg/d) at the end of each day after training and testing and over the weekend.
For antibody response determination, additional plasma from 9 young adult rhesus macaques (3–11 year old) infected with SIVmac251 for a median of 153 days post-infection was used. Five of these macaques were classified as controllers of infection, while four macaques were classified as progressors.
Water reinforcement rewards
During cognitive testing, water rewards were given to reinforce positive responses to stimuli. Animals with > 20% weight loss from commencement of water regulation were removed from water restriction until weights rebounded to acceptable levels before continuing water regulation. During the study period, nine animals (5 SIV-infected; 4 mock-infected) required temporary removal from water restriction lasting from 18 to 89 days in duration. These animals were not dehydrated or losing weight because of SIV infection, rather the animals were overweight when water regulation was initiated. Four SIV-infected macaques were also removed from water restriction due to illness prior to euthanasia for SIV-related (n = 1) or other (n = 3) reasons. Cognitive assessment data was not obtainable during these periods.
Cognitive assessments
Cognitive assessments took place in a sound attenuated chamber (model AB4240, Eckel Industries, Cambridge, MA) fitted with a 40 W light and white-noise generator. The E-prime software suite (Psychology Software Tools, Sharpsburg, PA) coupled with a CarrollTouch infrared touch screen (Elo Touch Solutions, Milpitas, CA) was used for all stimulus presentation, response recording, and data processing. Baseline measures for cognitive tasks were evaluated at the end of the training period to establish performance and age-matched experimental groups using a grade assessment statistic as indicated in Table 1. Cognitive assessments were conducted Monday through Thursday.
Speeded motor task
On each cognitive assessment day, a stimulus was presented on a touchscreen to start each trial of a 200 trial session. After pressing and holding the stimulus, the trial was advanced to presentation of a new stimulus. Attending correctly to the new stimulus resulted in a water reward and removal of the stimulus (scored a correct response). No water reward was offered upon an incorrect response and the stimulus was removed. Reward levels were amplified with speed of response. Accuracy, response time and percent completion were recorded. Eight animals did not acquire the ability to hold the stimulus to advance the trial, so their task was modified. For these animals, each trial began with presentation of the second stimulus, and a successful touch of that stimulus was scored as accurate, with the response time determined as the duration between presentation of the stimulus and an accurate touch. Analyses were binned by every 2 weeks post-infection (wpi).
Plasma and CSF draws
Plasma and CSF draws were performed/attempted prior to SIV inoculation and every 2 wpi. Samples were drawn at the conclusion of the week’s cognitive tasks to provide for recovery before tasks were resumed. Samples were aliquoted and stored at − 80 °C.
SIV inoculation
Macaques were inoculated with SIVmac251 (obtained from the Vaccine and Prevention Research Program, Division of AIDS, National Institute of Allergy and Infectious Diseases and Quality Biological Inc., Gaithersburg, MD from Dr. Ronald Desrosiers) by intravenous injection at 0 wpi. Macaques were observed daily for clinical signs of anorexia, weight loss, lethargy, or diarrhea. When deemed necessary by an examining veterinarian, animals with poor health were euthanized before completing the study. Due to age-related conditions such as congestive heart failure, kidney disease, and obstructive blood clots, euthanasia was necessary in both SIV-infected (5/12 animals) and mock-infected macaques (2/11 animals).
Antiretroviral therapy
Beginning 38 wpi, animals in the antiretroviral treatment groups received daily subcutaneous injections of reverse transcriptase inhibitors bis{[(isopropoxycarbonyl)oxy]methyl}({[(2R)-1-(6-amino-9H-purin-9-yl)-2 propanyl]oxy}methyl)phosphonate (TDF,Tenofovir disoproxil; 5.1 mg/kg) and 4-amino-5-fluoro-1-[(2R,5S)-2-(hydroxymethyl)-1,3-oxathiolan-5-yl]-1,2-dihydropyrimidin-2-one (FTC, emtricitabine, 50 mg/kg). Animals in no treatment groups received saline injections. TDF and FTC were generously provided by Gilead Sciences, Inc. (Foster City, CA) through Material Transfer Agreements.
Quantitation of SIV RNA in plasma and CSF
Virions from 1 ml of plasma or 200–500μl of CSF were pelleted by centrifugation at 23,586×g for 1 h, 4 °C. Total RNA was extracted from the pellet using Trizol reagent (Invitrogen, ThermoFisher Scientific, Waltham, MA). A standard quantitative RT-PCR was performed with 10μl RNA for each sample based on amplification of conserved sequences in gag [40].
Tissue collection and processing
At the conclusion of the study, animals were euthanized and perfused with phosphate buffered saline. Brain, spinal cord, spleen, liver, thymus, mesenteric and axial lymph nodes, lung, small bowel, colon, heart, ovary, quadriceps muscles, and kidney were collected. Portions of each tissue were fixed in 10% buffered formalin and paraffin embedded. After making coronal sections (~ 5 mm), every other section of the right brain hemisphere was fixed, while remaining sections were snap frozen in ~ 100 mg pieces of midfrontal cortex, caudate, putamen, hippocampus and cerebellum.
Quantitation of SIV RNA in brain tissue
Approximately 100 mg midfrontal cortex was disrupted in Trizol reagent using a Mini BeadBeater (Glen Mills, Inc., Clifton, NJ) to isolate RNA. SIV gag copy numbers were determined as described previously [40, 41] except the total amount of RNA was used to normalize the samples. Total RNA was quantitated using Quant-iT Ribogreen RNA Assay Kit (Invitrogen, ThermoFisher Scientific).
Histological assessment
Formalin fixed paraffin embedded sections from brain and other organs were processed for hematoxylin and eosin staining and CD68 and GFAP immunohistochemistry as described before [42]. To assess distribution and abundance of SIV infected cells, in situ hybridization (ISH) was performed as previously described [43] using riboprobes targeting portions of gag, pol, and env of the molecular clone of SIVmacBK28 [44].
Flow cytometry
After overnight shipment, 100 ml aliquots of EDTA-anticoagulated whole blood were incubated with a mastermix of fluorochrome-conjugated antibodies against a lymphocyte panel or a monocyte panel. The lymphocyte panel included antibodies against the following surface molecules: CD20 (L27, AlexaFluor 700), CD45 (D058-1283, PerCP), CD4 (SK3, PE-Cy7), CD8 (SK1, AmCyan), CD3 (SP34-2, PE-CF594). The monocyte panel included antibodies against the following surface molecules: HLA-DR (L243, APC-Cy7), CD45 (D058-1283, PerCP), CD3 (SP34-2, PE-CF594), CD20 (L27, AlexaFluor 700), CD14 (M5E2, FITC), CD16 (3G8, PacificBlue). All antibodies were from BD Biosciences (San Jose, CA). After lysing red blood cells, samples were acquired on a BD LSRII at Immunology Services unit of the Wisconsin National Primate Research Center (University of Wisconsin, Madison, WI). Data analysis was performed using FlowJo version 9.6.2 (Tree Star, Inc., Ashland, OR).
sCD14 ELISA
Plasma soluble CD14 concentrations were measured in duplicate using the Human CD14 Quantikine ELISA kit (R&D Systems, Minneapolis, MN) according to the manufacturer’s protocol.
Multiplex analysis of plasma inflammation markers
ProcartaPlex Multiplex Immunoassays (Affymetrix eBioscience, San Diego, CA) were used to detect non-human primate IL-6, IL-18, CXCL10 and TNF-α at the following time points: baseline (0 wpi), acute infection (2 and 4 wpi), and prior to initiation of CART (34/36 wpi). The 4 wpi time point was not measured in mock –infected macaques. Samples were read by the University of Pittsburgh Cancer Institute LUMINEX Facility using the Luminex 100 reader (Luminex Corporation, Austin, TX).
Humoral responses
ELISA analyses of the humoral immune responses to SIV envelope protein were tested at baseline, ~ 24 wpi, and necropsy as previously described [45] with modifications. A reference plasma with strong anti-Env antibody concentrations was aliquoted and stored at − 80 °C. A batch of EIA/RIA high binding plates were coated overnight with 0.08 μg/ml of rgp130 SIV mac251 (ImmunoDx, Woburn, MA) in PBS (pH 7.4) using 100 μl/well at 4 °C. Plates were blocked with 200 μl B3T buffer (150 mM NaCl, 50 mM Tris–HCl, 1 mM EDTA, 3.3% fetal bovine serum, 2% bovine serum albumin, 0.07% Tween 20) for 1 h at 37 °C. An aliquot of the reference plasma and test plasmas were serially diluted in B3T buffer and added to the plate in duplicate at 100 μl/well for 1 h at 37 °C. 100 μl of horseradish peroxidase-conjugated goat anti-monkey IgG (Rockland Immunochemicals, Inc., Limerick, PA) at 1:10,000 was added for 1 h at 37 °C. Plates were washed 6× with 0.1% Tween 20 in PBS after each step then developed using SureBlue TMB 1-Component Microwell Peroxidase Substrate (SeraCare Life Sciences, Milford, MA) for approximately 25 min. A TMB Stop Solution (SeraCare) was added and plates were read at 450 nm. The OD values for the reference plasma were used to interpolate relative values of anti-Env antibody concentrations using Prism 7 software (GraphPad Software, Inc.).
Statistical analysis
Mann–Whitney tests were used to compare mock-infected controls with SIV-infected macaques. For time course comparisons to baseline values, Kruskal–Wallis tests followed by Dunn’s multiple comparison tests were performed. Statistical analyses were performed with Prism 6 (GraphPad Software, San Diego, CA).
Results
Modeling HAND in aged SIV-infected macaques
A group of 23 aged macaques (age range at time of infection = 14.7–24.8 year; median age = 18.6 year) underwent a cognitive training period of 18 months to acclimate and teach the following: pole and collar handling, placement in a behavioral primate chair, water rewards, and cognitive tasks. Initially, it was planned to train the animals for a sensorimotor speeded response task and two executive function tasks. However, within the 18-month training period, this was not possible due to difficulties in training aged animals that had never undergone behavioral training (subjects were retired former breeders). Subjects began training with the speeded motor task, which was continued for the remainder of the study. Behavioral performance was assessed as detailed in Fig. 1a.

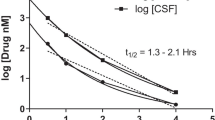
SIV-infection of aged macaques of Chinese origin has significant viremia. Timeline of cognitive testing, infection and CART (a). The proportion of CD4+ lymphocytes declines slightly in aged macaques of Chinese origin but recovers after CART. Longitudinal median ± standard error of peripheral blood proportions for CD4+ lymphocytes (b) and CD8+ lymphocytes (c) in SIV-infected and mock-infected aged RM-Ch. Plasma (d) and CSF (g) SIV viral loads from 7 SIV-infected macaques that did not receive treatment show significant viral replication. Plasma (e) and CSF (h) SIV viral loads from 5 SIV-infected macaques that received CART at 38 wpi show decreased viral replication during the treatment period. Median plasma (f) and mean CSF (i) SIV viral load of SIV-infected macaques that received CART compared to macaques that did not. The bars in (f) represent the upper and lower values. Asterisks indicate P < 0.05 for indicated time points. Kruskal–Wallis tests were used for (b), (c), (f), and (i). The green shaded area represents the period macaques received CART
Using baseline measurements for the speeded motor task (grade assessment statistic), four performance and aged-matched groups were established at the end of the training period (Table 1): SIV-infected, no treatment (initially n = 6); mock-infected, no treatment (initially n = 5); mock-infected CART treated (initially n = 6); and SIV-infected, CART treated (initially n = 6). Aged adults were difficult to train to interact with the touchscreens. Training techniques utilized in the past with younger animals, such as target training then bridging into a new behavior were often unsuccessful with this cohort. Eight aged RM-Ch did not reach the final stage of training for the final task at the end of the training period, so the task was modified accordingly for these animals. For comparison with past younger animals, the number of training sessions to learn to interact with the touchscreen ranged from 18 to 90 sessions for the aged RM-Ch, while 100% of a group of 14 young adult males successfully learned the task in half the time (11–46 sessions).
Acute RM-Ch infected with SIV were clinically asymptomatic
Macaques were infected with SIVmac251 at the end of the 18-month training period. Similar to individuals with acute HIV infection, infection of macaques with SIV sometimes results in an acute febrile response accompanied by development of a maculopapular rash, lymphadenopathy, diarrhea, weight loss, transient platelet decrease, and changes in sleep and motor activity [38, 46,47,48,49,50,51]. Surprisingly, the aged SIV-infected RM-Ch exhibited minimal to no clinical signs of infection; however, some other studies have observed that RM-Ch exhibit fewer clinical signs than RM of Indian origin [37]. Acute changes in weight from baseline after SIV-inoculation were similar to mock-infected animals for the first 2 wpi (Additional file 1: Fig. S1). At 3 and 4 wpi, SIV-infected animals showed greater weight loss than mock-infected RM-Ch, but since the variation in weight changes observed pre-infection was frequent and of similar amplitude, this change could not be attributed to SIV infection. There was no change in body temperature or platelet counts (Additional file 1: Figs. S2 and S3), and no lymphadenopathy was palpable. Comparison of temperature to plasma and CSF viral loads for individual SIV-infected animals are shown in Additional file 1: Fig. S6. Finally, activity counts and sleep patterns were similar to pre-infection levels and between the SIV-infected and mock-infected animals (data not shown).
Aged RM-Ch infected with SIV showed significant viremia
Despite absence of clinical signs during acute infection, aged SIV-infected RM-Ch had a median plasma viral load at 2 wpi of 9.65 × 106 copies/ml (range, 5.88 × 105–1.43 × 108 copies/ml) (Fig. 1). The viral load remained elevated in animals that did not receive CART through the remainder of the experiment with median viral loads at 107 copies/ml at several time points; however, some macaques exhibited significant variation over the course of infection. CART lowered median plasma viral load 2–3 logs during the 6-month treatment period (Fig. 1f). CSF viral load had an acute peak at 2 wpi (median, 1.23 × 106 copies/ml; range, 2.54 × 105–3.67 × 106 copies/ml) (Fig. 1i). Two SIV-infected macaques had undetectable to low levels of CSF virus after acute infection (Fig. 1g), while the remaining SIV-infected animals maintained CSF viral loads that ranged from 103 to 106 copies/ml. Three of the eight SIV-infected macaques that died before the end of the study showed elevated CSF viral load. Two of these animals demonstrated SIV encephalitis (#211; necropsy CSF viral load = 3.3 × 108 copies/ml) or SIV meningoencephalitis (#201; necropsy CSF viral load = 1.9 × 106 copies/ml), while the other macaque had a bacterial meningitis with infrequent SIV-infected cells in the spinal cord but not in the brain (#202; necropsy CSF viral load = 4.68 × 106 copies/ml). In macaques that received CART, detection of viral RNA in the CSF was completely eliminated in two macaques, decreased one log in one macaque, and showed a small decrease in one macaque that died a few weeks following CART initiation. One macaque showed increased viral RNA in the CSF with CART, but since few samples could be collected for this animal, effectiveness of CART throughout the treatment period was unknown.
Changes in peripheral blood cell populations in aged RM-Ch infected with SIV
The proportion of CD4+ T cells in SIV-infected macaques dropped from a median of 62–41% of T cells at 2 wpi, with a reciprocal increase in proportion of CD8+ T cells (Fig. 1a, b). This proportion decrease remained steady throughout the length of infection, although during the treatment period, animals receiving CART began to show T cell proportions similar to baseline and non-infected macaques. Absolute CD4+ T cell counts also decreased after infection, but the decrease was only significant at 32 and 34 wpi. Total CD8+ T cell counts were transiently increased during acute infection and at various time points thereafter (P < 0.05 at 22, 26, 40 and 52 wpi). NK cell counts followed a similar transient increase pattern (P < 0.05 at 26 and 52 wpi). Total cell counts for CD4+ and CD8+ T cells, NK cells and especially B cells showed transient fluctuations in the non-infected groups as well. T and NK cell counts tended to increase in non-infected macaques, while B cell counts decreased over time for all groups (Additional file 1: Fig. S4). Comparison of CD4+ T cell and CD8+ T-cell counts to plasma and CSF viral loads for individual SIV-infected animals are shown in Additional file 1: Fig. S7. Monocyte subset populations were also followed to examine expansion of inflammatory monocytes (Additional file 1: Fig. S5). The first few measurements after infection were not readable, so baseline cell counts of monocyte subsets were not available. There was little difference in median cell counts of classical monocyte populations (CD14 + CD16−). Intermediate or inflammatory monocytes (CD14 + CD16 +) showed transient increases at 12, 22, and 26 wpi, but the proportion of these cells was similar in SIV-infected and non-infected macaques.
Effect of age on survival and CNS infection
Five of the twelve (41%) aged SIV-infected macaques required euthanasia prior to the conclusion of the experiment, while two of the eleven (18%) non-infected macaques did not finish the study (Table 1). The SIV-infected macaques that did not complete the study had a higher median plasma viremia and CSF viral load at euthanasia than the SIV-infected macaques who completed the study (at the last time point prior to treatment, plasma: 5.3 × 108 copies/ml vs 1.82 × 107 copies/ml; CSF: 1.9 × 106 copies/ml vs 3.80 × 102 copies/ml). SIV-infection could be attributed as the reason for euthanasia in one macaque that developed SIV pneumonitis and encephalomyelitis. The other infected macaques succumbed to obstructed blood flow to the bowel, pneumonia, rhesus cytomegalovirus infection and bacterial meningitis. Using in situ hybridization, SIV infected cells were detected in the brains of three SIV-infected macaques at necropsy. Two macaques (#201 and #211) had infected lesions in every region examined, while one had infrequent infected cells in the caudate and putamen (#215) (Table 1). An additional two macaques (#202 and #208) also showed infrequent infected cells in the spinal cord. SIV RNA was detected in midfrontal cortex of four of the SIV-infected macaques that required euthanasia prior to the conclusion of the experiment and one that finished the study (median, 51.6 copies/μg RNA; range, 0.4–3.5 × 105 copies/μg RNA) (Table 1). Other neuropathological findings included mild to moderate deep white matter microgliosis, corticospinal tract degeneration, and chronic infarcts, but these findings were not exclusively associated with infection status. In the periphery, SIV-infected cells were detected in several organs of the non-treated SIV-infected macaques. While SIV infected cells were detected in treated SIV-infected macaques, the frequency and range was less than the non-treated macaques.
Neither SIV infection nor CART elicited changes in aged RM-Ch sensorimotor behavioral testing outcome
Baseline performances of each macaque were assigned a grade assessment statistic to create performance and age-matched groups. In these aged RM-Ch, there was a range of performance ability that did not correlate with age of the animal or any other observed variable. The median response time and percent accuracy in the speeded motor test was similar in SIV-infected and non-infected groups in the 12 weeks prior to infection (Fig. 2). During the acute infection period, both SIV-infected and non-infected groups showed improvements in response time and percent accuracy. This was attributed to the aged macaques slowly continuing to acquire proficiency/skill in the given task. After approximately 10 wpi, the response time and percent accuracy began to plateau. Neither infection or treatment had a significant effect on response time or percent accuracy (Fig. 2). Comparison of reaction time and accuracy to plasma and CSF viral loads for individual SIV-infected animals are shown in Additional file 1: Fig. S8, while the reaction time and accuracy of individual mock-infected macaques are shown in Additional file 1: Fig. S9. These results suggest that aged RM-Ch are capable of learning and improving tasks even during acute SIV-infection.

Neither infection or CART impacted performance on a speeded motor task in aged Chinese macaques. Comparison of median response times and accuracy did not show significant differences. Shown here are between group comparisons of mean ± standard error speeded motor performance response time (a) and accuracy (b). Analyses for response time and accuracy were binned by every 2 wpi over the course of training period, SIVmac251 or mock infection and CART. Differences between SIV-infection without CART versus SIV-infection with CART (SIV-Infected), Mock-infection without CART versus Mock-infection with CART (No Infection), SIV-infected versus Mock-Infected (Infection vs Noninfection), and CART versus PBS (treatment vs no treatment) are shown for a and b. Kruskal–Wallis tests were used to compare results displayed in each graph, but no statistically significant differences were found. The green shaded area represents the period macaques received CART
SIV-infection of aged RM-Ch was characterized by minimal inflammation
Pathogenic HIV/SIV infection is characterized by acute and persistent inflammation. To assess whether aged SIV-infected RM-Ch showed indications of a typical inflammatory response during infection, plasma sCD14, IL-6, IL-18, CXCL10 and TNF-α concentrations were assessed during the acute time points and prior to initiation of therapy. sCD14 levels were similar in both SIV-infected and non-infected macaques at all time points examined (Fig. 3a). IL-6, CXCL10 and TNF-α concentrations were undetectable in many of the animals regardless of infection status. However, IL-18 was significantly increased in SIV-infected macaques at 2 wpi (Fig. 3c). Overall, these results suggest that aged macaques of Chinese origin do not respond to SIV infection in the inflammatory manner characteristic of younger macaques and patients with HIV infection [52,53,54,55,56,57].

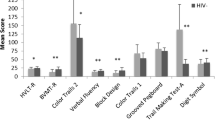
No elevation of hallmarks of chronic inflammation during lentiviral infection in aged SIV-infected Chinese macaques. IL-18 is elevated in aged SIV-infected macaques of Chinese origin during acute infection, but other hallmarks of chronic inflammation during lentiviral infection remain stable. Median plasma concentrations of soluble CD14 (sCD14) (a), IL-6 (b), IL-18 (c), CXCL10 (d), and TNF-α (e) at 0, 2, 4 wpi and 34 or 36 wpi or necropsy (34/36/nec). 0 wpi represents baseline, 2 and 4 wpi represent acute infection and 34/36/nec represent chronic infection. Kruskal–Wallis tests were used to analyze differences between groups. *P < 0.05. **P < 0.01
To address an aspect of the adaptive immune response in SIV-infected aged RM-Ch, we compared anti-Env antibody responses to SIV-infected young RM of Indian origin. It has been reported that RM-Ch generate stronger antibody responses them RM of Indian origin [55]. The majority of SIV-infected aged macaques generated detectable anti-Env antibody responses (Fig. 4). Two aged SIV-infected RM-Ch (#211 and #201) that required euthanasia prior to completion of the study failed to generate detectable anti-Env antibodies similar to two young adult progressor macaques. Three of four of the young adult animals with disease progression generated minimal if any anti-Env responses. Two of the remaining three aged SIV-infected macaques that required euthanasia prior to the conclusion of the experiment also showed minimal anti-Env antibody responses, while the animal that succumbed to obstructed blood flow to the bowel developed substantial anti-Env antibody responses. The aged SIV-infected macaques that completed the study generated variable anti-Env antibody responses similar to the young adult controller macaques.

Aged SIV-infected Chinese macaques generate antibody responses similar to progressors and less than controllers. Median Gp130 Env antibody response determined by ELISA. Kruskal–Wallis tests were used to compare each time point
Discussion
To understand processes contributing to HAND and aging, our objective was to model HAND in aged NHP in order to dissect the pathological and eventually mechanistic basis of this range of neurocognitive disorders. SIV infection of aged RM-Ch was quite different than reported for young adults [37, 38, 51, 57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. They showed minimal to no clinical signs upon infection, with no elevations of systemic temperature and no changes in activity levels, platelet counts or weight. Yet, the aged macaques demonstrated significant plasma viremia and modest CSF viral loads. Neither acute nor chronic SIV infection nor CART had a significant impact on accuracy, speed or percent completion in a speeded motor test. Since this study did not include young adult RM-Ch, we have used historic data that were not generated in the same conditions for comparisons. Although this does not detract from the findings, it will be important to perform additional study encompassing species and age differences to substantiate our conclusions.
Modeling human age-related neurological degeneration
Our study plan was to obtain macaques with brains similar in age to 50-year-old humans that could be trained for cognitive assessment and evaluated during chronic infection. Reasoning on the basis of proportional chronology, we estimated the 14–20-year-old macaques used in this study were roughly analogous to 50–60-year-old humans. It has been reported that macaques over 20 years of age show neuropathological changes of ageing analogous to those seen in humans over 60 years of age [73]. In our experience, only the most aged of nonhuman primates (~ 30 years old) have shown amyloid beta accumulation (a hallmark of pathological aging in humans commencing at 60–65 years of age but observed at younger ages in early onset neurodegenerative disease).
As different macaque species have variable susceptibility to SIV disease progression, it was important to choose a macaque species that was resilient to rapid disease progression and thus permit long-term study. We reasoned this would enable the animals to survive the training and testing paradigm and mitigate conditions that would confound the behavioral studies. The RM-Ch subspecies best fit these requirements.
We had several difficulties modeling the current commonly described forms of HAND in aging individuals beginning with training the 14–20-year-old macaques to learn cognitive tasks. Compared to past young adults, the aged macaques were recalcitrant to training, and despite increasing the training period, the macaques were only able to reliably perform the speeded motor task. Then after SIV infection, the aged RM-Ch failed to show clinical signs and we could not discriminate differences in neurocognitive performance. Despite matching groups for baseline cognitive task performance, the heterogeneous responses of the small groups of outbred aged RM-Ch further limited the ability to sensitively discern cognitive impairment. This highlights the difficulty and limitations of experimentally modeling the issues facing aviremic HIV-infected patients on effective long-term CART, yet experiencing HAND, in aged macaques. Might a different experimental approach or model be more suitable? This will have to be interrogated systematically in order to develop a system to address how chronic inflammation impacts cognition in the face of effective viral suppression.
Aged SIV-infected RM-Ch showed marked levels of plasma viremia
Juvenile and adult RM-Ch are reported to have innate resistance to SIV infection compared to rhesus macaques of Indian origin [37, 38, 58]. Levels of viral replication in RM-Ch tend to be lower than in macaques of Indian origin, but significant inter-individual variation in disease progression has been reported [59, 60]. Surveying the literature for plasma viremia in younger SIV-infected RM-Ch, peak viremia ranges from 103 to 108 copies/ml with an approximate mean of 5 × 107 copies/ml, while set point viremia ranges from 103 to 107 copies/ml [37, 38, 51, 57, 59,60,61,62,63,64,65,66,67,68,69,70,71,72]. Although viral strain and route of inoculation influence direct comparison of viral loads, the median plasma viremia of the aged RM-Ch in this study was in line with these published values at 9.65 × 106 copies/ml; however, the set point viremia was maintained at a median of 107 copies/ml, which is similar to the high end of the reported set point range.
Aged RM-Ch showed minimal clinical signs of SIV infection
Despite this viral load, little clinical evidence of infection was apparent. Some investigators have made similar observations with young RM-Ch showing fewer clinical signs of infection than RM of Indian origin and little appreciable weight loss [37]. However, others have observed that approximately half of young RM-Ch present with lymphadenopathy and experience weight loss, wasting, and diarrhea [38, 51]. Weight in the SIV-infected aged RM-Ch was similar to non-infected macaques. Temperature also remained remarkably stable, even during acute infection. This is contrary to infection of younger rhesus macaques that demonstrate hyperthermia during acute infection that lasts approximately 3 months [50], though these RM were most likely of Indian origin. Declines in platelet counts are reported to be an indicator of disease progression in HIV and SIV infection [49, 74], yet the aged macaques in this study did not show any alterations in platelet counts. Activity and sleep disturbances are also associated with SIV infection [50, 75, 76], but activity counts during day and night periods were similar to pre-infection and mock-infected animals. The absence of change in these clinical parameters suggests that SIV infection of aged RM-Ch is more analogous to SIV infection in the natural host (e.g. sooty mangabeys and African green monkeys), potentially for the same reason that some aspects of the immunological response to SIV such as type I IFN expression is less robust in the natural host than observed in other macaques [77]. Yet, this is a complex hypothesis to test, especially with the considerable variability observed in clinical parameters and immune activation of SIV infection of young RM-Ch [38, 51, 57, 66, 77].
Supporting the hypothesis that aged RM-Ch are refractory to clinical SIV-related disease, CD14 + CD16 + monocyte subset proportions and counts were similar in infected and non-infected macaques throughout the course of infection suggesting absence of an inflammatory environment that promotes this phenotype. Monocyte subsets are known to undergo dynamic changes as a function of duration of HIV/SIV infection and are variably reported to correlate or not with development of SIV encephalitis or HAND [78,79,80,81,82]. However, SIV-infected aged RM-Ch did show a decrease in the proportion of CD4+ T cells during acute infection. This population remained decreased throughout the length of infection (or until treatment). The absolute median CD4+ T cell count was also decreased but was not observed in every animal and was variable. There is no consensus reported for loss of CD4+ T cells in young adult RM-Ch. While a few reports observe stable CD4 counts [62, 68] or transient CD4 loss [70], several others detect significant CD4+ T cell loss [51, 59, 60, 71, 72].
Aged RM-Ch did not show significant sensorimotor deficits with SIV infection or CART
Despite our extensive experience training young adult rhesus macaques to perform a variety of complex neurobehavioral tasks, aged RM-Ch proved recalcitrant to training. Nevertheless, we were successful in training aged macaques for a speeded motor task where we could reliably assess their reaction time, touch screen accuracy and percent completion. Others have shown that young adult SIV-infected macaques show neurological abnormalities that can be documented through a variety of behavioral and neurophysiological tests. Motor skills, discrimination learning, discrimination retention, recognition, recency memory and attention impairments are observed early and during the chronic phase of SIV infection in adult rhesus macaques [83,84,85,86,87,88]. Some performance impairments were characterized by gradual deteriorations throughout the course of infection, while others showed sharp declines. In comparison, the aged RM-Ch did not show any significant changes on response time or percent accuracy during a speeded motor task. Why did SIV infection fail to induce neurological abnormalities in aged RM-Ch? Without the ability to test multiple realms of cognition, it is impossible to rule out deficits in other types of memory, e.g. executive function. As an alternative hypothesis, HAND could be a consequence of chronic inflammation, with the absence of sensorimotor impairment in aged RM-Ch being a reflection of the diminished clinical and immunological response.
Neuropathology of SIV infection and CART in aged RM-Ch
Neuropathological examination did not show any overt signs of neurodegeneration in SIV-infected or mock-infected aged macaques (Table 1). Remarkably, little fluctuation in the cognitive task was observed from baseline to chronic infection. This was also true in animals with CNS-related pathology; however, these animals typically required respite from cognitive testing shortly before succumbing to an illness. While SIV RNA in the midfrontal cortex was detectable in only a few animals, the CSF SIV RNA load remained moderate in the majority of animals, so there were presumably low levels of viral replication in the CNS. While non-quantitative neuropathological assessment did not demonstrate age-related differences between infected and mock-infected aged RM-Ch, more sensitive quantitative pathological and gene expression assessments are planned.
Virological responses of aged RM-Ch to CART
In SIV-infected animals, administration of TDF and FTC for 6 months was effective at decreasing plasma and CSF viral load in most animals. More interesting, treatment had neither a discernable positive or negative effect on neurobehavioral performance tasks for either infected or mock-infected animals. This is consistent with some human studies that have not documented neurobehavioral impairments in patients treated with CART [89]. However, it has been postulated that CART regimens potentially contribute to neurocognitive deficits by reducing dendritic arborization [90, 91].
SIV infection in aged RM-Ch shows lack of inflammatory environment
The lack of clinical signs and cognitive impairment drove us to examine the inflammatory response in aged SIV-infected Ch-RM. A hallmark of HIV and SIV infection is chronic inflammation and activated coagulation. This increased proinflammatory state is thought to drive alterations and senescence in immune cell populations [92] and increase availability of infectable cells [93]. Increased levels of D-dimer, IL-6, sCD14, CXCL10, TNF-α, IL-18, and CCL2 among others have been shown to be increased during acute infection or chronically increased throughout infection [52,53,54]. Many of these inflammatory markers are also increased in aged individuals, and it has been hypothesized that HIV infection accelerates aging [36, 94]. We did not discern any elevation in these markers during infection compared to baseline measurements and mock-infected aged RM-Ch. Plasma IL-18 (an IL-1 superfamily protein produced by activated macrophages) was elevated in SIV-infected RM-Ch during acute infection, but returned to baseline during the chronic phase of infection.
Interrogation of anti-Env antibody responses showed SIV infection was not inherently immunologically silent. Most of the young adult SIV-infected progressors generated minimal to no detectable anti-Env IgG suggesting antibody responses play a role in disease progression characteristics. Overall, the aged Ch-RM generated antibody responses similar to progressors or less than young adult controllers. SIV-neutralizing antibody titers were not determined, so it is unclear whether the binding IgG detected by ELISA was functional. A comprehensive investigation of innate and adaptive immune responses during the course of SIV infection in aged Ch-RM and controls deserves further exploration to examine potential causes for the lack of clinical signs.
The overall lack of an overt inflammatory response during either acute or chronic infection is similar to that observed during nonpathogenic SIV infections in their natural hosts [95,96,97]. Both natural hosts and macaques respond to SIV infection with strong upregulation of type I interferon-stimulated genes (ISG) [98]. Whereas ISG levels in natural hosts are quickly restored to baseline, upregulation of ISGs become chronic in younger Ch-RM. Although ISG expression was not assessed here, no increase in CXCL10 was observed suggesting lack of sustained ISG response in aged Ch-RM.
Another potential reason for the diminished immune response in aged RM-Ch could be immune senescence. Aged macaques have been reported to show characteristics of immune senescence with increased proinflammatory status and altered immune cell populations [92]. In fact, we have noted that aged macaques have variable, delayed, and significantly weaker anti-beta-amyloid IgG levels in response to beta-amyloid immunization [73].
An elevated inflammatory milieu, such as increased sCD14 and sCD163 along with low CD4 T-cell count nadirs are also reported to predict development of HAND [99,100,101,102,103]. It could be hypothesized that absence of robust inflammation during acute infection, absence of many clinical signs of infection or disease and lack of chronic inflammation in the face of substantive viral replication obviate neurological damage. Although these observations warrant verification with controls demonstrating cognitive impairment concurrently with inflammation, our data are consistent with the hypothesis that HAND may be related to a chronic immune response to infection rather than the infection itself.
Conclusions
We show that aged RM-Ch present with minimal clinical signs during SIV infection despite substantial viremia. Along with absence of indicators of disease, aged SIV-infected RM-Ch do not display deficits in cognitive tests and do not demonstrate chronic inflammation. SIV infection of aged RM-Ch did not bring about histological signs of neurodegeneration. Although these conclusions will need to be substantiated encompassing species and age differences, the observations suggest that these characteristics are reminiscent of SIV infection in natural disease resistant hosts.
Abbreviations
- AIDS:
-
acquired immune deficiency syndrome
- CART:
-
combined antiretroviral therapy
- CNS:
-
central nervous system
- CSF:
-
cerebrospinal fluid
- EDTA:
-
ethylenediaminetetraacetic acid
- EIA/RIA:
-
enzyme immunoassay/radioimmunoassay
- ELISA:
-
enzyme-linked immunosorbent assay
- FTC:
-
emtricitabine
- HAD:
-
HIV-associated dementia
- HAND:
-
HIV-associated neurocognitive disorders
- HIV:
-
human immunodeficiency virus
- ISG:
-
interferon-stimulated genes
- ISH:
-
in situ hybridization
- NHP:
-
nonhuman primate
- OD:
-
optical density
- rgp130:
-
recombinant glycoprotein 130
- RM-Ch:
-
rhesus macaques of Chinese origin
- sCD14:
-
soluble CD14
- SIV:
-
simian immunodeficiency virus
- SIVmac:
-
SIV from macaques
- TDF:
-
Tenofovir disoproxil
- TMB:
-
tetramethylbenzidine
- wpi:
-
week(s) post-infection
References
World Health Organization. Fact sheet—latest statistics on the status of the AIDS epidemic. http://www.unaids.org/en/resources/fact-sheet. Accessed 20 Nov 2017.
Achim CL, Wang R, Miners DK, Wiley CA. Brain viral burden in HIV infection. J Neuropathol Exp Neurol. 1994;53:284–94.
Boisse L, Gill MJ, Power C. HIV infection of the central nervous system: clinical features and neuropathogenesis. Neurol Clin. 2008;26:799–819.
Heaton RK, Clifford DB, Franklin DR Jr, Woods SP, Ake C, Vaida F, et al. HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study. Neurology. 2010;75:2087–96.
Heaton RK, Franklin DR, Ellis RJ, McCutchan JA, Letendre SL, Leblanc S, et al. HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: differences in rates, nature, and predictors. J Neurovirol. 2011;17:3–16.
Tozzi V, Balestra P, Bellagamba R, Corpolongo A, Salvatori MF, Visco-Comandini U, et al. Persistence of neuropsychologic deficits despite long-term highly active antiretroviral therapy in patients with HIV-related neurocognitive impairment: prevalence and risk factors. J Acquir Immune Defic Syndr. 2007;45:174–82.
Ances BM, Clifford DB. HIV-associated neurocognitive disorders and the impact of combination antiretroviral therapies. Curr Neurol Neurosci Rep. 2008;8:455–61.
Simioni S, Cavassini M, Annoni JM, Rimbault Abraham A, Bourquin I, Schiffer V, et al. Cognitive dysfunction in HIV patients despite long-standing suppression of viremia. AIDS. 2010;24:1243–50.
Sacktor N, Skolasky RL, Seaberg E, Munro C, Becker JT, Martin E, et al. Prevalence of HIV-associated neurocognitive disorders in the Multicenter AIDS Cohort Study. Neurology. 2016;86:334–40.
Sheppard DP, Ludicello JE, Bondi MW, Doyle KL, Morgan EE, Massman PJ, et al. Elevated rates of mild cognitive impairment in HIV disease. J Neurovirol. 2015;21:576–84.
Valcour V, Shikuma C, Shiramizu B, Watters M, Poff P, Selnes O, et al. Higher frequency of dementia in older HIV-1 individuals: the Hawaii Aging with HIV-1 Cohort. Neurology. 2004;63:822–7.
Fazeli PL, Crowe M, Ross LA, Wadley V, Ball K, Vance DE. Cognitive functioning in adults aging with HIV: a cross-sectional analysis of cognitive subtypes and influential factors. J Clin Res HIV AIDS Prev. 2014;1:155–69.
Joska JA, Westgarth-Taylor J, Hoare J, Thomas KG, Paul R, Myer L, et al. Neuropsychological outcomes in adults commencing highly active anti-retroviral treatment in South Africa: a prospective study. BMC Infect Dis. 2012;12:39.
Saylor D, Dickens AM, Sacktor N, Haughey N, Slusher B, Pletnikov M, et al. HIV-associated neurocognitive disorder—pathogenesis and prospects for treatment. Nat Rev Neurol. 2016;12:234–48.
Becker JT, Kingsley L, Mullen J, Cohen B, Martin E, Miller EN, et al. Vascular risk factors, HIV serostatus, and cognitive dysfunction in gay and bisexual men. Neurology. 2009;73:1292–9.
Fabbiani M, Ciccarelli N, Tana M, Farina S, Baldonero E, Di Cristo V, et al. Cardiovascular risk factors and carotid intima-media thickness are associated with lower cognitive performance in HIV-infected patients. HIV Med. 2013;14:136–44.
McCutchan JA, Marquie-Beck JA, Fitzsimons CA, Letendre SL, Ellis RJ, Heaton RK, et al. Role of obesity, metabolic variables, and diabetes in HIV-associated neurocognitive disorder. Neurology. 2012;78:485–92.
Vivithanaporn P, Nelles K, DeBlock L, Newman SC, Gill MJ, Power C. Hepatitis C virus co-infection increases neurocognitive impairment severity and risk of death in treated HIV/AIDS. J Neurol Sci. 2012;312:45–51.
Weber E, Morgan EE, Iudicello JE, Blackstone K, Grant I, Ellis RJ, et al. Substance use is a risk factor for neurocognitive deficits and neuropsychiatric distress in acute and early HIV infection. J Neurovirol. 2013;19:65–74.
Becker JT, Kingsley LA, Molsberry S, Reynolds S, Aronow A, Levine AJ, et al. Cohort profile: recruitment cohorts in the neuropsychological substudy of the Multicenter AIDS Cohort Study. Int J Epidemiol. 2015;44:1506–16.
Tedaldi EM, Minniti NL, Fischer T. HIV-associated neurocognitive disorders: the relationship of HIV infection with physical and social comorbidities. Biomed Res Int. 2015;2015:641913.
Fisher M, Cooper V. HIV and ageing: premature ageing or premature conclusions? Curr Opin Infect Dis. 2012;25:1–3.
Gelman BB. Neuropathology of HAND with suppressive antiretroviral therapy: encephalitis and neurodegeneration reconsidered. Curr HIV/AIDS Rep. 2015;12:272–9.
Brew BJ, Pemberton L, Cunningham P, Law MG. Levels of human immunodeficiency virus type 1 RNA in cerebrospinal fluid correlate with AIDS dementia stage. J Infect Dis. 1997;175:963–6.
Ellis RJ, Moore DJ, Childers ME, Letendre S, McCutchan JA, Wolfson T, et al. Progression to neuropsychological impairment in human immunodeficiency virus infection predicted by elevated cerebrospinal fluid levels of human immunodeficiency virus RNA. Arch Neurol. 2002;59:923–8.
Ho DD, Rota TR, Schooley RT, Kaplan JC, Allan JD, Groopman JE, et al. Isolation of HTLV-III from cerebrospinal fluid and neural tissues of patients with neurologic syndromes related to the acquired immunodeficiency syndrome. N Engl J Med. 1985;313:1493–7.
Sonnerborg AB, Ehrnst AC, Bergdahl SK, Pehrson PO, Skoldenberg BR, Strannegard OO. HIV isolation from cerebrospinal fluid in relation to immunological deficiency and neurological symptoms. AIDS. 1988;2:89–93.
Brew BJ, Letendre SL. Biomarkers of HIV related central nervous system disease. Int Rev Psychiatry. 2008;20:73–88.
Tyler KL, McArthur JC. Through a glass, darkly: cerebrospinal fluid viral load measurements and the pathogenesis of human immunodeficiency virus infection of the central nervous system. Arch Neurol. 2002;59:909–12.
Nath A, Conant K, Chen P, Scott C, Major EO. Transient exposure to HIV-1 Tat protein results in cytokine production in macrophages and astrocytes. A hit and run phenomenon. J Biol Chem. 1999;274:17098–102.
Tansey MG, McCoy MK, Frank-Cannon TC. Neuroinflammatory mechanisms in Parkinson’s disease: potential environmental triggers, pathways, and targets for early therapeutic intervention. Exp Neurol. 2007;208:1–25.
Langston JW, Forno LS, Tetrud J, Reeves AG, Kaplan JA, Karluk D. Evidence of active nerve cell degeneration in the substantia nigra of humans years after 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine exposure. Ann Neurol. 1999;46:598–605.
Jang H, Boltz D, Sturm-Ramirez K, Shepherd KR, Jiao Y, Webster R, et al. Highly pathogenic H5N1 influenza virus can enter the central nervous system and induce neuroinflammation and neurodegeneration. Proc Natl Acad Sci USA. 2009;106:14063–8.
Galloway DA, McDougall JK. The oncogenic potential of herpes simplex viruses: evidence for a ‘hit-and-run’ mechanism. Nature. 1983;302:21–4.
Desquilbet L, Jacobson LP, Fried LP, Phair JP, Jamieson BD, Holloway M, et al. HIV-1 infection is associated with an earlier occurrence of a phenotype related to frailty. J Gerontol A Biol Sci Med Sci. 2007;62:1279–86.
Deeks SG, Tracy R, Douek DC. Systemic effects of inflammation on health during chronic HIV infection. Immunity. 2013;39:633–45.
Trichel AM, Rajakumar PA, Murphey-Corb M. Species-specific variation in SIV disease progression between Chinese and Indian subspecies of rhesus macaque. J Med Primatol. 2002;31:171–8.
Ling B, Veazey RS, Luckay A, Penedo C, Xu K, Lifson JD, et al. SIV(mac) pathogenesis in rhesus macaques of Chinese and Indian origin compared with primary HIV infections in humans. AIDS. 2002;16:1489–96.
Joag SV, Stephens EB, Adams RJ, Foresman L, Narayan O. Pathogenesis of SIVmac infection in Chinese and Indian rhesus macaques: effects of splenectomy on virus burden. Virology. 1994;200:436–46.
Cline AN, Bess JW, Piatak M Jr, Lifson JD. Highly sensitive SIV plasma viral load assay: practical considerations, realistic performance expectations, and application to reverse engineering of vaccines for AIDS. J Med Primatol. 2005;34:303–12.
Venneti S, Bonneh-Barkay D, Lopresti BJ, Bissel SJ, Wang G, Mathis CA, et al. Longitudinal in vivo positron emission tomography imaging of infected and activated brain macrophages in a macaque model of human immunodeficiency virus encephalitis correlates with central and peripheral markers of encephalitis and areas of synaptic degeneration. Am J Pathol. 2008;172:1603–16.
Bissel SJ, Wang G, Ghosh M, Reinhart TA, Capuano S 3rd, Stefano Cole K, et al. Macrophages relate presynaptic and postsynaptic damage in simian immunodeficiency virus encephalitis. Am J Pathol. 2002;160:927–41.
Bonneh-Barkay D, Bissel SJ, Kofler J, Starkey A, Wang G, Wiley CA. Astrocyte and macrophage regulation of YKL-40 expression and cellular response in neuroinflammation. Brain Pathol. 2012;22:530–46.
Fuller CL, Choi YK, Fallert BA, Capuano S 3rd, Rajakumar P, Murphey-Corb M, et al. Restricted SIV replication in rhesus macaque lung tissues during the acute phase of infection. Am J Pathol. 2002;161:969–78.
Wu X, Yang ZY, Li Y, Hogerkorp CM, Schief WR, Seaman MS, et al. Rational design of envelope identifies broadly neutralizing human monoclonal antibodies to HIV-1. Science. 2010;329:856–61.
Baskin GB, Murphey-Corb M, Watson EA, Martin LN. Necropsy findings in rhesus monkeys experimentally infected with cultured simian immunodeficiency virus (SIV)/delta. Vet Pathol. 1988;25:456–67.
Benveniste RE, Morton WR, Clark EA, Tsai CC, Ochs HD, Ward JM, et al. Inoculation of baboons and macaques with simian immunodeficiency virus/Mne, a primate lentivirus closely related to human immunodeficiency virus type 2. J Virol. 1988;62:2091–101.
Letvin NL, Desrosiers RC. Simian immunodeficiency virus. Berlin: Springer; 1994.
Metcalf Pate KA, Lyons CE, Dorsey JL, Shirk EN, Queen SE, Adams RJ, et al. Platelet activation and platelet-monocyte aggregate formation contribute to decreased platelet count during acute simian immunodeficiency virus infection in pig-tailed macaques. J Infect Dis. 2013;208:874–83.
Horn TF, Huitron-Resendiz S, Weed MR, Henriksen SJ, Fox HS. Early physiological abnormalities after simian immunodeficiency virus infection. Proc Natl Acad Sci USA. 1998;95:15072–7.
Wei Q, Liu L, Cong Z, Wu X, Wang H, Qin C, et al. Chronic ∆(9)-tetrahydrocannabinol administration reduces IgE(+)B cells but unlikely enhances pathogenic SIVmac251 infection in male rhesus macaques of Chinese origin. J Neuroimmune Pharmacol Off J Soc NeuroImmune Pharmacol. 2016;11:584–91.
Kuller LH, Tracy R, Belloso W, De Wit S, Drummond F, Lane HC, et al. Inflammatory and coagulation biomarkers and mortality in patients with HIV infection. PLoS Med. 2008;5:e203.
Paiardini M, Muller-Trutwin M. HIV-associated chronic immune activation. Immunol Rev. 2013;254:78–101.
Stacey AR, Norris PJ, Qin L, Haygreen EA, Taylor E, Heitman J, et al. Induction of a striking systemic cytokine cascade prior to peak viremia in acute human immunodeficiency virus type 1 infection, in contrast to more modest and delayed responses in acute hepatitis B and C virus infections. J Virol. 2009;83:3719–33.
Ling B, Veazey RS, Penedo C, Xu K, Lifson JD, Marx PA. Longitudinal follow up of SIVmac pathogenesis in rhesus macaques of Chinese origin: emergence of B cell lymphoma. J Med Primatol. 2002;31:154–63.
Ling B, Rogers L, Kaushal D, Morici L, Lackner A, Pahar B, et al. SIV specific immune responses and gene regulations in SIV-infected long-term nonprogressing rhesus macaques. http://www2.tulane.edu/asvpr/upload/Ling-Abstract-2010.pdf (2010) Accessed 15 Dec 2017.
Zhou Y, Bao R, Haigwood NL, Persidsky Y, Ho WZ. SIV infection of rhesus macaques of Chinese origin: a suitable model for HIV infection in humans. Retrovirology. 2013;10:89.
Trask JS, Garnica WT, Malhi RS, Kanthaswamy S, Smith DG. High-throughput single-nucleotide polymorphism discovery and the search for candidate genes for long-term SIVmac nonprogression in Chinese rhesus macaques (Macaca mulatta). J Med Primatol. 2011;40:224–32.
Cong Z, Xue J, Xiong J, Yao N, Wang W, Jiang H, et al. Correlation of central memory CD4+ T-Cell decrease in the peripheral blood with disease progression in SIVmac251-infected Chinese rhesus macaques. J Med Primatol. 2015;44:175–82.
Zhang LT, Tian RR, Zheng HY, Pan GQ, Tuo XY, Xia HJ, et al. Translocation of microbes and changes of immunocytes in the gut of rapid- and slow-progressor Chinese rhesus macaques infected with SIVmac239. Immunology. 2016;147:443–52.
Liu H, Xiao QH, Liu JB, Li JL, Zhou L, Xian QY, et al. SIV Infection Impairs the Central Nervous System in Chinese Rhesus Macaques. J Neuroimmune Pharmacol Off J Soc NeuroImmune Pharmacol. 2016;11:592–600.
Tian RR, Zhang MX, Zhang LT, Zhang XL, Zheng HY, Zhu L, et al. High immune activation and abnormal expression of cytokines contribute to death of SHIV89.6-infected Chinese rhesus macaques. Arch Virol. 2015;160:1953–66.
Ling B, Rogers L, Johnson AM, Piatak M, Lifson J, Veazey RS. Effect of combination antiretroviral therapy on Chinese rhesus macaques of simian immunodeficiency virus infection. AIDS Res Hum Retrovir. 2013;29:1465–74.
Monceaux V, Viollet L, Petit F, Cumont MC, Kaufmann GR, Aubertin AM, et al. CD4+ CCR5 + T-cell dynamics during simian immunodeficiency virus infection of Chinese rhesus macaques. J Virol. 2007;81:13865–75.
Elbim C, Monceaux V, Mueller YM, Lewis MG, Francois S, Diop O, et al. Early divergence in neutrophil apoptosis between pathogenic and nonpathogenic simian immunodeficiency virus infections of nonhuman primates. J Immunol. 2008;181:8613–23.
Cumont MC, Diop O, Vaslin B, Elbim C, Viollet L, Monceaux V, et al. Early divergence in lymphoid tissue apoptosis between pathogenic and nonpathogenic simian immunodeficiency virus infections of nonhuman primates. J Virol. 2008;82:1175–84.
Sanders-Beer B, Babas T, Mansfield K, Golightly D, Kramer J, Bowlsbey A, et al. Depo-Provera does not alter disease progression in SIVmac-infected female Chinese rhesus macaques. AIDS Res Hum Retrovir. 2010;26:433–43.
Marcondes MC, Penedo MC, Lanigan C, Hall D, Watry DD, Zandonatti M, et al. Simian immunodeficiency virus-induced CD4+ T cell deficits in cytokine secretion profile are dependent on monkey origin. Viral Immunol. 2006;19:679–89.
Xia HJ, Zhang GH, Ma JP, Dai ZX, Li SY, Han JB, et al. Dendritic cell subsets dynamics and cytokine production in SIVmac239-infected Chinese rhesus macaques. Retrovirology. 2010;7:102.
Ling B, Piatak M Jr, Rogers L, Johnson AM, Russell-Lodrigue K, Hazuda DJ, et al. Effects of treatment with suppressive combination antiretroviral drug therapy and the histone deacetylase inhibitor suberoylanilide hydroxamic acid; (SAHA) on SIV-infected Chinese rhesus macaques. PLoS ONE. 2014;9:e102795.
Bao R, Zhuang K, Liu J, Wu J, Li J, Wang X, et al. Lipopolysaccharide induces immune activation and SIV replication in rhesus macaques of Chinese origin. PLoS ONE. 2014;9:e98636.
Chen S, Lai C, Wu X, Lu Y, Han D, Guo W, et al. Variability of bio-clinical parameters in Chinese-origin Rhesus macaques infected with simian immunodeficiency virus: a nonhuman primate AIDS model. PLoS ONE. 2011;6:e23177.
Kofler J, Lopresti B, Janssen C, Trichel AM, Masliah E, Finn OJ, et al. Preventive immunization of aged and juvenile non-human primates to beta-amyloid. J Neuroinflamm. 2012;9:84.
Nicolle M, Levy S, Amrhein E, Schmitt MP, Partisani M, Rey D, et al. Normal platelet numbers correlate with plasma viral load and CD4+ cell counts in HIV-1 infection. Eur J Haematol. 1998;61:216–7.
Fox HS, Weed MR, Huitron-Resendiz S, Baig J, Horn TF, Dailey PJ, et al. Antiviral treatment normalizes neurophysiological but not movement abnormalities in simian immunodeficiency virus-infected monkeys. J Clin Invest. 2000;106:37–45.
Huitron-Resendiz S, Marcondes MC, Flynn CT, Lanigan CM, Fox HS. Effects of simian immunodeficiency virus on the circadian rhythms of body temperature and gross locomotor activity. Proc Natl Acad Sci USA. 2007;104:15138–43.
Campillo-Gimenez L, Laforge M, Fay M, Brussel A, Cumont MC, Monceaux V, et al. Nonpathogenesis of simian immunodeficiency virus infection is associated with reduced inflammation and recruitment of plasmacytoid dendritic cells to lymph nodes, not to lack of an interferon type I response, during the acute phase. J Virol. 2010;84:1838–46.
Bissel SJ, Wang G, Trichel AM, Murphey-Corb M, Wiley CA. Longitudinal analysis of activation markers on monocyte subsets during the development of simian immunodeficiency virus encephalitis. J Neuroimmunol. 2006;177:85–98.
Burdo TH, Soulas C, Orzechowski K, Button J, Krishnan A, Sugimoto C, et al. Increased monocyte turnover from bone marrow correlates with severity of SIV encephalitis and CD163 levels in plasma. PLoS Pathog. 2010;6:e1000842.
Pulliam L, Gascon R, Stubblebine M, McGuire D, McGrath MS. Unique monocyte subset in patients with AIDS dementia. Lancet. 1997;349:692–5.
Gama L, Shirk EN, Russell JN, Carvalho KI, Li M, Queen SE, et al. Expansion of a subset of CD14highCD16negCCR2low/neg monocytes functionally similar to myeloid-derived suppressor cells during SIV and HIV infection. J Leukoc Biol. 2012;91:803–16.
Kim WK, Sun Y, Do H, Autissier P, Halpern EF, Piatak M Jr, et al. Monocyte heterogeneity underlying phenotypic changes in monocytes according to SIV disease stage. J Leukoc Biol. 2010;87:557–67.
Weed MR, Gold LH, Polis I, Koob GF, Fox HS, Taffe MA. Impaired performance on a rhesus monkey neuropsychological testing battery following simian immunodeficiency virus infection. AIDS Res Hum Retrovir. 2004;20:77–89.
Prospero-Garcia O, Gold LH, Fox HS, Polis I, Koob GF, Bloom FE, et al. Microglia-passaged simian immunodeficiency virus induces neurophysiological abnormalities in monkeys. Proc Natl Acad Sci USA. 1996;93:14158–63.
Weed MR, Hienz RD, Brady JV, Adams RJ, Mankowski JL, Clements JE, et al. Central nervous system correlates of behavioral deficits following simian immunodeficiency virus infection. J Neurovirol. 2003;9:452–64.
Murray EA, Rausch DM, Lendvay J, Sharer LR, Eiden LE. Cognitive and motor impairments associated with SIV infection in rhesus monkeys. Science. 1992;255:1246–9.
Gold LH, Fox HS, Henriksen SJ, Buchmeier MJ, Weed MR, Taffe MA, et al. Longitudinal analysis of behavioral, neurophysiological, viral and immunological effects of SIV infection in rhesus monkeys. J Med Primatol. 1998;27:104–12.
Marcario JK, Raymond LA, McKiernan BJ, Foresman LL, Joag SV, Raghavan R, et al. Motor skill impairment in SIV-infected rhesus macaques with rapidly and slowly progressing disease. J Med Primatol. 1999;28:105–17.
Winston A, Vera JH. Can antiretroviral therapy prevent HIV-associated cognitive disorders? Curr Opin HIV AIDS. 2014;9:11–6.
Robertson K, Liner J, Meeker RB. Antiretroviral neurotoxicity. J Neurovirol. 2012;18:388–99.
Tovar-y-Romo LB, Bumpus NN, Pomerantz D, Avery LB, Sacktor N, McArthur JC, et al. Dendritic spine injury induced by the 8-hydroxy metabolite of efavirenz. J Pharmacol Exp Ther. 2012;343:696–703.
Willette AA, Coe CL, Birdsill AC, Bendlin BB, Colman RJ, Alexander AL, et al. Interleukin-8 and interleukin-10, brain volume and microstructure, and the influence of calorie restriction in old rhesus macaques. Age (Dordr). 2013;35:2215–27.
Haase AT. Targeting early infection to prevent HIV-1 mucosal transmission. Nature. 2010;464:217–23.
Singh T, Newman AB. Inflammatory markers in population studies of aging. Ageing Res Rev. 2011;10:319–29.
Pandrea I, Apetrei C. Where the wild things are: pathogenesis of SIV infection in African nonhuman primate hosts. Curr HIV/AIDS Rep. 2010;7:28–36.
Evans DT, Silvestri G. Nonhuman primate models in AIDS research. Curr Opin HIV AIDS. 2013;8:255–61.
Pandrea I, Silvestri G, Apetrei C. AIDS in african nonhuman primate hosts of SIVs: a new paradigm of SIV infection. Curr HIV Res. 2009;7:57–72.
Jacquelin B, Mayau V, Targat B, Liovat AS, Kunkel D, Petitjean G, et al. Nonpathogenic SIV infection of African green monkeys induces a strong but rapidly controlled type I IFN response. J Clin Invest. 2009;119:3544–55.
Beck SE, Queen SE, Witwer KW, Metcalf Pate KA, Mangus LM, Gama L, et al. Paving the path to HIV neurotherapy: predicting SIV CNS disease. Eur J Pharmacol. 2015;759:303–12.
Burdo TH, Weiffenbach A, Woods SP, Letendre S, Ellis RJ, Williams KC. Elevated sCD163 in plasma but not cerebrospinal fluid is a marker of neurocognitive impairment in HIV infection. AIDS. 2013;27:1387–95.
Lyons JL, Uno H, Ancuta P, Kamat A, Moore DJ, Singer EJ, et al. Plasma sCD14 is a biomarker associated with impaired neurocognitive test performance in attention and learning domains in HIV infection. J Acquir Immune Defic Syndr. 2011;57:371–9.
Marcotte TD, Deutsch R, Michael BD, Franklin D, Cookson DR, Bharti AR, et al. A concise panel of biomarkers identifies neurocognitive functioning changes in HIV-infected individuals. J Neuroimmune Pharmacol Off J Soc NeuroImmune Pharmacol. 2013;8:1123–35.
Ellis RJ, Badiee J, Vaida F, Letendre S, Heaton RK, Clifford D, et al. CD4 nadir is a predictor of HIV neurocognitive impairment in the era of combination antiretroviral therapy. AIDS. 2011;25:1747–51.
Authors’ contributions
SJB designed the project, helped perform the experiments, consolidated and analyzed the data, prepared the figures and tables, interpreted the data, and wrote the manuscript; KG provided supervision, helped perform the experiments, consolidated and analyzed the data, and participated in the writing of the manuscript; HPJ analyzed and interpreted the data; NFS processed samples and generated, graphed and interpreted PCR data; GW helped perform the experiments; CWB designed the project, interpreted the data, provided supervision, and participated in the writing of the manuscript; CAW conceived and designed the project, provided supervision, interpreted the data, and participated in the writing of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
We thank Nicole Nania for valuable veterinary assistance and Chris Janssen and Anita Trichel for veterinary care. We thank Simon M. Barratt-Boyes for rhesus macaque blood samples. We thank Arlene Carbone-Wiley, Mark Stauffer and Dana Weber for valuable technical assistance and preparation of histological specimens. We thank ABL Inc. and the Vaccine Research Program, Division of AIDS, NIAID for providing the viral inoculum. We thank Eva Rakasz at the Immunology Services unit of the Wisconsin National Primate Research Center for flow cytometry analysis.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Ethics approval and consent to participate
All animal experiments were approved and permitted by the University of Pittsburgh’s Institutional Animal Care and Use Committee. Experiments were conducted in accordance to the Animal Welfare Act, PHS Animal Welfare Policy, and the standards of American Association of Laboratory Animal Care.
Funding
This work was supported by National Institutes of Health (NIH) grants MH097476 to S.J.B., C.B., and C.A.W. The viral inoculum was provided by ABL Inc. and the Vaccine Research Program, Division of AIDS, NIAID. Flow cytometry analysis was supported in part by an NIH grant to the Immunology Services unit of the Wisconsin National Primate Research Center (5P51OD011106). Luminex analyses were supported in part by and NIH award P30CA047904 to the UPCI Cancer Biomarkers Facility: Luminex Core Laboratory. Tenofovir disoproxil and emtricitabine were generously provided by Gilead Sciences, Inc. (Foster City, CA) through Material Transfer Agreements. The funding bodies had no role in study design, data collection, analysis, and interpretation, or the decision to write up and submit the work for publication.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1: Figure S1.
Effect of age and SIV-infection on weight. In comparison to mock-infected macaques, SIV-infection of aged Chinese rhesus macaques does not impact weight. Animals were weighed on a weekly basis. Median longitudinal weight (kg) over the course of infection for each group (A). Change in median weight (kg) from baseline in SIV-infected (red) and mock-infected (blue) macaques during the acute phase of infection (B). Both SIV-infected and mock infected macaques lost weight at 2 and 3 wpi. At 4 wpi, SIV-infected macaques lost a small amount of mass while mock-infected macaques slightly gained mass. Change in median weight (kg) from baseline in SIV-infected (red) and mock-infected (blue) macaques at time of necropsy (C). Mock-infected macaques gained over 1 kg by the end of the study whereas SIV-infected macaques were similar to their starting weight. Figure S2. Effect of age, SIV-infection and cART on body temperature. There were no changes in body temperature after SIV-infection in aged Chinese rhesus macaques. Body temperature was recorded at least once a day and the median temperature determined in two week intervals. Baseline temperature (week 0 post-infection) was the average of 12 weeks of preinoculation measurements. Time course of body temperature in SIV-infected macaques and controls (A). Lines represent median values. Time course of change in temperature (Δ °C) from baseline (B). Change in temperature from baseline during the first 4 weeks post-infection (C). Change in temperature from baseline at necropsy (D). Figure S3. Effect of age, SIV-infection and cART on platelet counts. Platelet counts are not significantly altered during acute SIV infection in aged rhesus macaques of Chinese origin. Time course of median platelet counts during the duration of infection (A). Lines represent median values. Platelet counts of SIV-infected and mock-infected macaques during the first 4 weeks post-infection (B). Figure S4. Total cell counts during the course of SIV infection. Total CD4+ T-cell counts decrease during SIV infection in aged rhesus macaques of Chinese origin. Total CD8+ T-cell and NK-cell counts shown an elevation during acute infection then fall to similar levels as mock-infected macaques. Time course change in CD4+ T-cell (A), CD8+ T-cell (B), NK-cell (C), and B-cell counts (D) during SIV and mock infection. Lines represent median values. Figure S5. Total monocyte subset counts during the course of SIV infection. CD14+CD16- (A), CD14+CD16+ (B), CD14-CD16+ (C) monocyte subset counts during SIV infection in aged rhesus macaques of Chinese origin. Lines represent median values. Figure S6. Plasma and CSF viral load versus temperature in individual SIV-infected macaques. Each graph shows the time course of plasma SIV loads, CSF SIV loads and temperature in an individual aged Chinese rhesus macaque during SIV infection. Graphs of SIV-infected macaques that did not receive treatment (Group 1) are shown in (a) and graphs of SIV-infected macaques that were treated with CART (Group 4) are shown in (b). The green shaded area represents the period macaques received CART or saline. Figure S7. Plasma and CSF viral load versus CD4+ and CD8+ T-cell count in SIV-infected macaques. Each graph shows the time course of plasma SIV loads, CSF SIV loads, CD4+ T-cell counts, and CD8+ T-cell counts in an individual aged Chinese rhesus macaque during SIV infection. Graphs of SIV-infected macaques that did not receive treatment (Group 1) are shown in (a) and graphs of SIV-infected macaques that were treated with CART (Group 4) are shown in (b). The green shaded area represents the period macaques received CART or saline. Figure S8. Plasma and CSF viral load versus reaction time and accuracy in SIV-infected macaques. Each graph shows the time course of plasma SIV loads, CSF SIV loads, reaction time (RT), and percent accuracy (Acc) in an individual aged Chinese rhesus macaque during SIV infection. Graphs of SIV-infected macaques that did not receive treatment (Group 1) are shown in (a) and graphs of SIV-infected macaques that were treated with CART (Group 4) are shown in (b). The green shaded area represents the period macaques received CART or saline. Figure S9. Time and accuracy in mock-infected macaques. Each graph shows the reaction time (RT) and percent accuracy (Acc) in a speeded motor task for an individual aged Chinese rhesus macaque over the study period. Graphs of mock-infected macaques that did not receive treatment (Group 2) are shown in (a) and graphs of mock-infected macaques that were treated with CART (Group 3) are shown in (b). The green shaded area represents the period macaques received CART or saline.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Bissel, S.J., Gurnsey, K., Jedema, H.P. et al. Aged Chinese-origin rhesus macaques infected with SIV develop marked viremia in absence of clinical disease, inflammation or cognitive impairment. Retrovirology 15, 17 (2018). https://doi.org/10.1186/s12977-018-0400-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12977-018-0400-y