
Abstract
Background
The dose–effect relationship of Long-snake-like moxibustion for chronic fatigue syndrome (CFS) remains poorly understood. In order to address this gap, we designed this trial to assess the association between different treatment duration of Long-snake-like moxibustion and its effects on CFS based on the combination measurements of the subjective patient-reported scales with objective medical infrared imaging technology─Thermal Texture Maps (TTM).
Methods
From December 2020 to January 2022, 60 female CFS patients were recruited and equally allocated to two groups: Group A, receiving 60-min Long-snake-like moxibustion per treatment, and Group B, receiving 30-min Long-snake-like moxibustion per treatment. The treatment was administered 3 times per week for a total of 4 weeks. The primary outcome was defined as the improvement of symptoms measured by the Fatigue scale-14 (FS-14), and secondary outcomes were designated as the improvement in Symptoms Scale of Spleen-Kidney Yang Deficiency, Self-rating depression scale, and Self-rating anxiety scale. TTM scanning was employed twice for CFS patients (before and after 4-week treatment) and once for Healthy control subjects (HCs).
Results
At week 4, the scores of FS-14 and Symptoms Scale of Spleen-Kidney Yang Deficiency in Group A were significantly lower than those in Group B (physical fatigue: 5.00 vs. 6.00, with 95%CI − 2.00 to 0.00, p = 0.003; FS-14 total score: 8.00 vs. 9.00, with 95%CI − 3.00 to 0.00, p = 0.012; total score of Symptoms Scale of Spleen-Kidney Yang Deficiency: 9.80 vs. 13.07, with 95%CI − 5.78 to − 0.76, P = 0.012). All thermal radiation values of the two groups increased, and statistical differences in ΔTs between Group A and HCs were not obtained. More significant correlations between symptoms improvements and ΔT changes were observed in Group A, and its ΔT changes in Upper Jiao, Shenque (CV8), Zhongwan (CV12), Danzhong (CV17), Zhiyang (GV9), Dazhui (GV14), upper arm, thoracic segments, lumbar segments, renal region, popliteal fossa strongly correlated with the improvement of Spleen-Kidney Yang Deficiency symptoms.
Conclusions
In the same course of treatment, the positive dose–effect relationship was found between the treatment duration of Long-snake-like moxibustion and CFS effect assessment. 60-min Long-snake-like moxibustion per treatment were associated with optimal clinical response and TTM improvement.
Trial registration
Chinese Clinical Trail Registry (No. ChiCTR2000041000, date of registration: 16 December 2020), http://www.chictr.org.cn/showproj.aspx?proj=62488
Similar content being viewed by others

Background
Chronic fatigue syndrome (CFS) is a condition characterized by persistent and debilitating fatigue lasting for at least 6 months, which is not relieved by rest [1]. The fatigue and its accompanied symptoms, including sleep disturbance, pain, sore throat, impaired short-term memory and concentration, greatly affect patients’ quality of life and ability to work. CFS has a global prevalence of 40% and is more prevalent in women than in men [2]. Despite its widespread occurrence, the medical cause of CFS is still unclear, resulting in a lack of specific pharmacological treatment recommendations. However, several promising approaches, including acupuncture [3], moxibustion [4], yoga [5], cognitive behavioral therapy), and graded exercise therapy [6,7,8] have shown potential for treating CFS.
According to the theory of traditional Chinese Medicine (TCM), fatigue is the result of Yang deficiency. Yang, or Yang-qi, an important concept in TCM, represents the vital energy of life. Yang deficiency refers to a pathological state characterized by a deficiency of Yang qi, representing the impaired functions of warming and promotion. Consequently, when organ function declines, the symptoms such as decreased vitality, listlessness, aversion to cold and preference for warmth, and reduced metabolism will manifest. The most typical affected Zang and Fu of Yang deficiency is Spleen-Kidney Yang. Moxibustion has the ability to produce Yang-warming effect and improve deficient Yang for Zang and Fu. Although the precise mechanism by which moxibustion treats CFS is not fully explained, moxibustion therapy has been shown to be effective in relieving symptoms [9, 10]. Long-snake-like moxibustion, also known as Du moxibustion, involves applying a large range of moxa cones or sticks over herbs or ginger on the Governor Vessel from GV14 to GV2 to generate a powerful warming stimulation. Compared to general moxibustion therapies, Long-snake-like moxibustion has a wider treatment area and utilizes the medicinal properties of moxa wool and ginger. It has a greater effect of warming yang, supplementing qi, promoting the circulation of qi and blood, and harmonizing yin and yang. Currently, there are a variety of Long-snake-like moxibustion applications. It has been applied to rheumatic immune diseases [11], osteoarthropathy [12], digestive disorders [13], etc. The mechanisms behind the therapeutic effects of Long-snake-like moxibustion on these diseases may involve the regulation of immune imbalance, reduction of immune response, acceleration of blood circulation, alleviation of tissue edema, and reduction of gastrointestinal burden. In our previous study [14], we improved the Long-snake-like moxibustion technique through applying moxa boxes placed over ginger slices on the back from GV14 to GV2, as well as on the same level of the first lateral line of Bladder Meridian. This modification enhanced clinical operability and improved the therapeutic effect.
We searched several databases (PubMed, Embase, Web of Science, Chinese National Knowledge Infrastructure Database, Wanfang Database, China Science and Technology Journal Database, etc.) from their respective inception dates to January 31, 2020. The search was performed using keywords such as ‘moxibustion’, ‘moxibustion therapy’, ‘moxibustion treatment’, ‘dose’, ‘moxibustion dose’, ‘dose–effect relationship’, ‘moxibustion effect’, etc. The searching results found that moxibustion is influenced by various factors that affect its therapeutic efficacy, such as moxibustion dose, which includes moxibustion duration, treatment frequency, moxibustion amount-size, and the number of moxa cones used [15,16,17,18]. Therefore, we conducted this trial to investigate the relationship between the duration of Long-snake-like moxibustion and its effect on CFS by using both subjective scales and objective measurements for assessment.
So far, CFS trials evaluating the efficacy and safety of therapies have employed self-reported subjective measurements, including the Chalder Fatigue Scale, Short Form 36 Health Survey Questionnaire, Anxiety and Depression Scale, and Visual Analogue Pain Rating Scale, to evaluate improvements in physical function, anxiety, depression, and pain [19]. In addition, biological markers and imaging techniques, such as MRI, have also been used to support clinical diagnosis and evaluate treatment effects [20, 21]. In this trial, we used Thermal Texture Maps (TTM), a thermography technique that evaluates thermal signatures of the body through a holistic interpretation of infrared images, to aid in CFS diagnosis and moxibustion dose–effect assessment.
Methods
Design
The single-center, randomized, controlled trial was conducted at the Center of Preventive Medicine, Hospital of Chengdu University of TCM. This trial strictly adhered to the rules of the Declaration of Helsinki and the Good Clinical Practice Guidelines, and it was registered with a unique registration number (ChiCTR2000041000) at http://www.chictr.org.cn. The protocol received approval from the Ethics Committee of Affiliated Hospital of Chengdu University of TCM in 2020 (No.2020KL-046). Written informed consent was obtained from all participants, which included 60 female patients with CFS and 30 healthy control subjects (HCs).
The CFS patients were randomly allocated to either the 60-min Long-snake-like moxibustion group (Group A) or the 30-min Long-snake-like moxibustion group (Group B) in a 1:1 ratio, with a treatment period of 4 weeks consisting of 3 times per week, every other day.
Subjects
Patients were recruited from multiple sources, including the hospital as well as electronic posters on WeChat and physical posters displayed in hospitals and communities. Face-to-face interviews were conducted by the clinical trial coordinator to ensure that all patients met the inclusion criteria. The inclusion and exclusion criteria for patients and HCs are shown in Table 1.
Randomization and blinding
Eligible CFS patients were randomly allocated to either Group A or Group B. Random numbers were generated by Statistics Analysis System, and then placed in opaque envelopes. A research assistant, who was uninvolved in the assessment or treatment, was responsible for keeping the original random allocation sequences, printing serial numbers on the outside of the envelopes, and sealing the envelopes. All envelopes were put into a plastic container in numerical order. Once patients were assessed to meet the inclusion criteria and provided informed consent, investigators opened the envelopes in turn. To ensure blinding, the outcome assessors and statistical analysts were blinded to the intervention assignments throughout the trial.
Intervention
Practitioners: Certified acupuncturists with TCM license and more than 2-year clinical experience were trained to administer Long-snake-like moxibustion. The training focused on the correct manipulation of the moxibustion technique.
Group A: 60-min Long-snake-like moxibustion. Patients were positioned prone with their entire back exposed and received ginger-indirect moxibustion on the Governor Vessel and Bladder Meridian. Ginger slices, 2 mm in thickness, were placed on the back from GV14 to GV2, covering the area of the Governor Vessel and the first lateral line of the Bladder Meridian (Fig. 1). Five or six 3-hole moxa boxes (depending on the patient’s height, Fig. 2) were then placed on top of the ginger slices, with a distance of 4.8 cm between the centers of the nearby holes to ensure the moxa sticks’ temperature (pure-mugwort moxa stick; 20 cm in length and 18 mm in diameter; Hwato, Suzhou, China, PRC) covered the Governor Vessel and the first lateral line of the Bladder Meridian. The depth of moxa sticks was regulated every 5 min during 60-min treatment to maintain full combustion and obtain equal warm stimulation. Patients received 12 sessions of moxibustion treatment over a 4-week period (1 session per day, 3 sessions per week, every other day).

Ginger slices were placed on the back from GV14 to GV2

Five or six 3-hole moxa boxes were put on the participants of two groups
Group B: 30-min Long-snake-like moxibustion. The treatment process was the same as in Group A, with a moxibustion duration of 30 min.
Outcome measures
Primary outcome: In this trial, the improvement in fatigue severity assessed by Fatigue scale-14 (FS-14) was set as the primary outcome. FS-14 is a standardized questionnaire reflecting physical and mental fatigue and comprises 14 questions. Each question has two options (yes or no) and a score of 0 to 1 (0 = no, 1 = yes), resulting in a total score ranging from 0 to 14 [22, 23]. Higher scores indicate a higher level of chronic fatigue. The assessment using FS-14 was conducted at baseline and at the end of the 4-week treatment period (week 4).
Secondary outcome: The secondary outcome measures included the scores of the Symptoms Scale of Spleen-Kidney Yang Deficiency, the Self-rating depression scale (SDS), and the Self-rating anxiety scale (SAS). The Symptoms Scale of Spleen-Kidney Yang Deficiency is a 4-rate scale designed to evaluate symptoms based on TCM syndrome differentiation. It consists of primary symptoms with scores ranging from 0 to 6, including fear of cold and cold extremities, lassitude and lack of strength, shortness of breath and laziness to speak, reduced food intake, soreness and weakness of waist and knees. It also includes secondary symptoms with scores ranging from 0 to 3, including lumbar cold pain, abdominal fullness and distention, loose stool, cold and more urine volume during night. Higher scores indicate a higher level of Spleen-Kidney Yang Deficiency. Both the SDS and SAS are 20-item scales designed to measure depression/anxiety with scores ranging from 20 to 80. Higher scores indicate a higher level of depression and anxiety. All secondary outcomes were assessed at baseline and at the end of the 4-week treatment period (week 4).
TTM scanning: 90 eligible participants (30 female CFS patients in Group A, 30 female CFS patients in Group B, and 30 HCs) received TTM (Digital Medical Infrared Imaging System, MTI-ex pro-2013, Chongqing, China) scanning at baseline, and only patients in Groups A and B received a second TTM scanning after the 4-week treatment period. To weaken the influence of external thermo-source on the moxibustion effect assessment, the second TTM scanning was employed 5 days after the end of treatment. To minimize the impact of outside temperature, all the scanning was executed in the morning at the health examination center of the Affiliated Hospital of Chengdu university of TCM. The scanning room was maintained at a controlled temperature of 21℃ ± 2℃ and a humidity level of 50% ± 10%. The subjects were positioned in an environment with no direct ventilation, sunlight, or infrared radiation source [24, 25]. The TTM scanning process and relevant precautions are detailed in Table 2, and the image area definitions based on the Three-Jiao theory in TCM (Upper Jiao, Middle Jiao, and Lower Jiao) are shown in Table 3 [26, 27].
Sample size
Based on our preliminary study [28], which demonstrated an improvement of 2.45 in the FS-14 score following 60 min of Long-snake-like moxibustion therapy, we expected a mean improvement difference of 0.4 in the FS-14 score. With a desired power of 0.9 and a significance of 0.05, the estimated sample size required was 27 participants per group. Considering a dropout rate of 10%, the total number of patients was 60, while the total number of HCs was 30.
Statistical methods
The data was analyzed by an independent statistician. Quantitative data were described by mean with standard deviation (SD) or median with percentile (Q1, Q3). All the statistical analyses were performed with SPSS software version 25.0 (SPSS Inc, IBM Corporation, Chicago, Illinois, USA). The correlation analysis and visualization were performed with R language version 4.2.0 (R Development Core Team, Vienna, Austria). A two-sided test was applied for all available data, and a P-value < 0.05 was considered statistically significant.
The main analysis was based on an intention-to-treat population, and missing data at random were replaced by the multiple imputation method. The primary outcome of FS-14 score was analyzed by Mann-Whitney U-test. For secondary outcomes, including the score of Symptoms Scale of Spleen-Kidney Yang Deficiency, SDS score and SAS score, we conducted independent sample T test or Mann-Whitney U test (used in non-normally distributed variables) to compare the scores after 4 -week treatment between Groups A and B.
TTM analysis: Disease-related areas, specific regions or acupoints were acquired through comparing HCs with CFS patients in the whole-body thermal map. The relative thermal radiation value difference was defined as the temperature difference between the local temperature and the average temperature of the front or back of the trunk. It was automatically detected by TTM. Median differences and 95% confidence intervals of the temperature difference (ΔT) comparison between Group A or B and HCs at the end of 4-week treatment in the above area or acupoints were calculated by Hodges-Lehmann method.
Attrition analyses: Considering the possible effect from visit lost on results, we added 10% more sample size for each group in recruitment to hedge against expected attrition. For incomplete outcome data, we used multiple imputation method to replace random missing data. Sensitivity analysis using the per protocol set was performed and compared with the intention-to-treat analysis results.
Data collection and quality control
The original data were recorded in paper case report form (CRF) and then filled in a spreadsheet. An independent investigator checked the original data to ensure the consistency of CRF and spreadsheet. Only the principal investigators and clinical investigators were qualified to review the data. Before the start of trial, all involved researchers underwent training to guarantee the full understanding of study protocol, research process and CRF-filling. Additionally, once the eligible participants were enrolled, full communication about possible benefits and risks were made and a comfortable treatment environment was provided to ensure participants’ compliance. For participants with poor compliance, investigators contacted them by phone to acquire the outcome data, inquire about possible reasons for non-compliance, and encourage them to complete the study.
Results
Patient characteristics
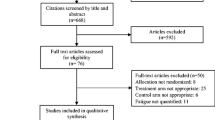
From December 2020 to January 2022, a total of 101 patients were screened, and 60 patients were included with a median age of 30.50 (Q1, Q3: 24.00, 40.75) years and a median CFS duration of 31.00 (Q1, Q3: 12.00, 60.00) months. The study flowchart is shown in Fig. 3. There were no significant differences between the two groups with respect to baseline demographic and clinical characteristics (P > 0.05). These results suggested that the two groups were comparable (Table 4).

Patient flowchart. ITT intention-to-treat
Primary outcome
After 12 treatment sessions within 4 weeks, physical fatigue score and FS-14 total score decreased in both groups compared to baseline (Fig. 4). Group A showed significantly lower scores at the end of treatment (physical fatigue: 5.00 vs. 6.00, 95%CI − 2.00 to 0.00, p = 0.003; FS-14 total score: 8.00 vs. 9.00, 95%CI − 3.00 to 0.00, p = 0.012) (Table 5).
Secondary outcomes
Symptoms scale of spleen-kidney Yang Deficiency
The scores of Symptoms Scale of Spleen-Kidney Yang Deficiency decreased after 4-week treatment (Fig. 4). Compared with Group B, Group A showed significantly lower scores in fear of cold and cold extremities (2.00 vs. 4.00, 95%CI − 2.00 to 0.00, P = 0.034), shortness of breath and laziness to speak (2.00 vs. 2.00, 95%CI − 1.00 to 0.00, P = 0.045), soreness and weakness of waist and knees (0.00 vs. 2.00, 95%CI − 2.00 to 0.00, P = 0.033), lumbar cold pain (1.00 vs. 1.00, 95%CI − 1.00 to 0.00, P = 0.028), loose stool (0.00 vs. 1.00, 95%CI − 1.00 to 0.00, P = 0.028), cold and more urine volume during night(0.00 vs. 0.00, 95%CI 0.00 to 0.00, P = 0.046) and total score (9.80 vs. 13.07, 95%CI − 5.78 to − 0.76, P = 0.012) (Table 6).

Effects of Long-snake-like moxibustion at baseline and week 4. Data in a, b, c were shown by the median with interquartile range and data in d, e, f were shown by mean with error bar represented standard deviation; a Physical fatigue score at baseline and week 4; b Mental fatigue score at baseline and week 4; c Total score of FS-14 at baseline and week 4; d Symptoms scale score of spleen-kidney Yang deficiency at baseline and week 4; e SDS score at baseline and week 4; f SAS score at baseline and week 4
SDS and SAS
SDS and SAS scores of both groups decreased after treatment (Fig. 4), and there were no statistical differences between groups (Table 7).
TTM outcome
When comparing with HCs, statistical differences in ΔT of Groups A and B were obtained at baseline in Middle Jiao (Group A vs. HCs − 0.22 vs. 0.07, 95%CI 0.10 to 0.64; Group B vs. HCs − 0.33 vs. 0.07, 95%CI 0.15 to 0.79), Lower Jiao (Group A vs. HCs − 0.67 vs. − 0.38, 95%CI 0.06 to 0.76; Group B vs. HCs − 0.81 vs. − 0.38, 95%CI 0.18 to 0.82), Shenque (CV8) (Group A vs. HCs 0.57 vs. 1.17, 95%CI 0.34 to 1.13; Group B vs. HCs 0.57 vs. 1.17, 95%CI 0.31 to 1.11), neck (Group A vs. HCs 0.68 vs. 1.41, 95%CI 0.29 to 1.46; Group B vs. HCs 0.41 vs. 1.41, 95%CI 0.66 to 1.56), upper arm (Group A vs. HCs − 0.42 vs. 0.24, 95%CI 0.04 to 0.93; Group B vs. HCs − 0.42 vs. 0.24, 95%CI 0.20 to 1.00), thoracic segments (Group A vs. HCs 0.33 vs. 0.76, 95%CI 0.17 to 0.77; Group B vs. HCs 0.31 vs. 0.76, 95%CI 0.31 to 0.93).
After 4-week treatment, statistical differences in ΔT between Group A and HCs were not obtained at the aforementioned sites, while statistical differences in ΔT between Group B and HCs were still obtained in neck (0.85 vs. 1.41, 95%CI 0.09 to 0.88), upper arm (− 0.25 vs. 0.24, 95%CI 0.01 to 0.85) (Table 8).
Correlation with symptoms and TTM
The two groups had significant correlations between score changes and ΔT changes in TTM (Fig. 5). In Group A, the score change of fear of cold and cold extremities was negatively correlated with ΔT changes of upper arm (r = − 0.43, p = 0.019), thoracic segments (r = − 0.43, p = 0.019), lumbar segments (r = − 0.46, p = 0.010), renal region (r = − 0.44, p = 0.016), popliteal fossa (r = − 0.46, p = 0.011); the score change of lassitude and lack of strength was negatively correlated with ΔT changes of Upper Jiao (r = − 0.42, p = 0.022), Danzhong (CV17) (r = − 0.49, p = 0.006), Zhiyang (GV9) ( r = − 0.44, p = 0.016), Dazhui (GV14) (r = − 0.42, p = 0.023); the score change of shortness of breath and laziness to speak was negatively correlated with ΔT change of Zhongwan (CV12) (r = − 0.46, p = 0.011); the score change of lumbar cold pain was negatively correlated with ΔT change of thoracic segments (r = − 0.38, p = 0.041); the score change of abdominal fullness and distention was negatively correlated with ΔT changes of Shenque (CV8) (r = − 0.42, p = 0.022), thoracic segments (r = − 0.37, p = 0.047); the total score change of Spleen-Kidney Yang Deficiency Symptoms Scale was negatively correlated with ΔT change of thoracic segments (r = − 0.44, p = 0.016). In Group B, only the score change of fear of cold and cold extremities was negatively correlated with ΔT change of Zhiyang (GV9) (r = − 0.41, p = 0.024).

Correlations with score changes and ΔT changes. Score change = week 4-baseline;ΔT change = week 4-baseline; ΔT: temperature difference; a Correlations in Group A; b Correlations in Group B; Spearman’s correlation was calculated and displayed as corrplot graphs using R package “corrplot”. r ranges between − 1 and 1, where − 1 ≤ r < 0 means negative correlation, r = 0 means no correlation, and 0 < r ≤ 1 means positive correlation. Blue circles represent positive correlation and red circles represent negative correlation. The darker the color and the larger the circle, the stronger is the correlation
Sensitivity analysis
Sensitivity analysis performed by the per protocol set showed similar results as the intention-to-treat analysis (Additional file 1).
Discussion
Due to the non-organic pathophysiology, CFS is associated with suboptimal health status [29]. The present treatment of CFS is given based on limited or even contradictory evidence from clinical studies [30,31,32]. CFS is named as fatigue syndrome in TCM theory and its main reason is believed to be Yang-qi deficiency. Especially Spleen and Kidney Yang are thought to be the vital motivity, and organs will become hypofunctional once Yang qi decreases. Therefore, Spleen-Kidney Yang Deficiency Syndrome is a commonly used visceral pattern in clinical diagnosis of CFS [33, 34]. Moxibustion therapy has been applied in Yang deficiency patients for thousands of years in China and it is used widely to relieve fatigue symptoms [35]. A systematic review has suggested that moxibustion has more advantages than acupuncture and drugs in relieving fatigue symptoms and improving clinical efficacy [36]. As a unique traditional moxibustion therapy, Long-snake-like moxibustion has shown to be a safe and effective therapy for relieving fatigue and improving Yang deficiency constitution [14, 37].
The dose–effect relationship is a crucial issue in the moxibustion research, with key factors such as treatment duration, frequency, extent, and amount of moxa cones/sticks determining the moxibustion dose. However, the relationship between the dose of moxibustion stimulation and the resulting therapeutic efficacy has not yet been established. Previous studies have shown that the above dose factors affect efficacy to varying degrees in different diseases. For instance, in the study of treating diarrhea-predominant irritable bowel syndrome, aconite cake-separated moxibustion with a treatment regimen of 3 sessions per week and 1 cone per session appeared to produce better therapeutic effects compared to a regimen of 6 sessions per week and 2 cones per session [18]. Another study on suspended moxibustion for focal cerebral ischemia/reperfusion injury found that 35-min moxibustion indicated a greater anti-apoptotic effect than 15-min moxibustion [17]. In the treatment of depression-like behavior disorder in rats, prolonged duration of moxibustion under optimal extent could increase the level of 5-HT [16]. Furthermore, in the treatment of chronic neck pain using direct moxibustion with small moxa cones, there was a trend of improved effectiveness with an increase in the amount of moxa cones when the other dose factors were constant [15].
The duration of Long-snake-like moxibustion is a key factor in optimizing efficacy, but the treatment duration for CFS varies [38, 39]. In our 4-week trial with 3 treatments per week, we compared the dose–effect relationship of the therapy using treatment durations of 30 and 60 min. Our findings suggest that 60-min Long-snake-like moxibustion is more effective in relieving fatigue and improving symptoms of Spleen-Kidney Yang Deficiency compared to 30-min Long-snake-like moxibustion. Specifically, the fatigue was relieved primarily by improving physical fatigue rather than improving mental fatigue, and the TCM pattern was improved primarily by alleviating main symptoms (such as fear of cold and cold extremities, soreness and weakness of waist and knees, lumbar cold pain, etc.), suggesting that 60-min Long-snake-like moxibustion therapy has a better ability to tonify Yang qi and improve the fatigue state. However, there was no statistically significant between-group difference in lassitude and lack of strength in the Symptoms Scale of Spleen-Kidney Yang Deficiency, which was different from the result obtained with FS-14. This discrepancy may be due to the fact that fatigue is a multidimensional and subjective sense of physical, mental, or emotional tiredness [40]. Lassitude and lack of strength is only a component item in the Symptoms Scale of Spleen-Kidney Yang Deficiency and it is relatively simple and unidimensional. In contrast, FS-14 is an internationally recognized measurement tool for evaluating fatigue symptoms in clinics, providing a more comprehensive reflection of fatigue severity [22, 41]. It could measure fatigue across multiple dimensions with better reliability and validity, offering a clearer understanding of the type of fatigue experienced and improved assessment precision compared to single-item measures [42]. Besides, statistically significant between-group differences in SDS and SAS were not observed, which may be associated with the relatively short course of treatment and no follow-up period. The moxibustion effects on mental fatigue and mental distress require further study.
A large body of evidence has showed that diseases or deviation from normal functioning are accompanied by temperature changes in the body, which, in turn, affect the temperature of the skin. Infrared imaging (IR) has proven to be a useful method for diagnosing signs of certain diseases by measuring the local skin temperature. As a new medical IR technology, TTM enables contactless and non-invasive identification of abnormal heat sources within the human body by analyzing thermographic data and surface temperature distribution [43]. Since its invention, TTM has been applied in disease diagnosis such as oncology (breast, skin, etc.), vascular disorders (diabetes, deep venous thrombosis), and monitoring the efficacy of therapeutic drugs, etc. [44,45,46,47,48]. Therefore, we combined measurements of the subjective patient-reported scales with objective TTM technology in this trail. Unlike previous study that only used objective technique to quantify muscle fatigue [49], our trial took a comprehensive approach. We not only employed subjective scales to evaluate fatigue levels and Spleen-Kidney Yang Deficiency symptoms before and after treatment but also utilized objective technique (TTM) to assess thermal energy metabolism changes in CFS patients and compared them with those of HCs. The aim of this trial was to quantify the therapeutic effect of Long-snake-like moxibustion, evaluate the thermal energy metabolism under different physiological/pathological conditions and different durations of moxibustion, and obtain the optimal dose–effect of Long-snake-like moxibustion.
According to the results, most thermal radiation values in CFS patients were obviously lower than those in HCs at baseline, and the ΔTs in CFS patients were statistically different from those of HCs in Middle Jiao, Lower Jiao, Shenque (CV8), neck, upper arm, thoracic segments. Some studies have shown that irregularities in energy metabolism [50], impaired cell metabolism [51], activated immune system [52], viral infection [53], impaired functioning in the hypothalamic-pituitary-adrenal axis and neuroendocrine dysregulation [54] have been considered possible causes of CFS. An animal experiment indicated that fatigued rats would have a deterioration in energy metabolism [55]. Since TTM images present the level of energy metabolism by displaying the thermal radiation value distribution [56], we found that most CFS patients were in a state of low energy metabolism. After 4-week Long-snake-like moxibustion, thermal radiation values increased at both directly and indirectly stimulated sites by moxibustion, indicating that Long-snake-like moxibustion could transfer and penetrate heat to far and deep sites, increase metabolic heat in different sites and regions of the body, and improve the low energy metabolism state. This heat energy transfer may be the underlying mechanism of moxibustion therapy [57]. Moreover, at the end of 4-week treatment, there were no statistically significant differences in ΔTs between the 60-min Long-snake-like moxibustion group and HCs in the above sites, whereas the ΔTs in neck and upper arm still showed statistically significant differences between the 30-min Long-snake-like moxibustion group and HCs. This suggests that 60-min Long-snake-like moxibustion has a more pronounced ability to increase thermal radiation values and demonstrates a closer trend to that of HCs. The TTM results were consistent with the subjective scales results, suggesting that 60-min Long-snake-like moxibustion had a more significant effect than 30-min moxibustion.
It is worth mentioning that ΔT changes were negatively correlated with the score changes, indicating that the more thermal radiation values increased, the better the CFS symptoms improved. This suggests that the increase in thermal radiation values may be an indirect reflection of warming and tonifying Yang. ΔT changes in Upper Jiao, Shenque (CV8), Zhongwan (CV12), Danzhong (CV17), Zhiyang (GV9), Dazhui (GV14), upper arm, thoracic segments, lumbar segments, renal region, popliteal fossa strongly correlated with the improvement of Spleen-Kidney Yang Deficiency symptoms. This suggests that Zhiyang (GV19), Dazhui (GV14), thoracic segments, lumbar segments, renal region on the Governor vessel are key acupoints and regions with the Yang-tonifying effect. Other randomized controlled trials have also shown that moxibustion on the Governor vessel has good therapeutic effects on Yang deficiency diseases [13, 58]. The improvement of Yang deficiency symptoms is also related to the fact that Long-snake-like moxibustion stimulates Yang of the whole body to a greater extent by transferring heat to the extremities and penetrating heat to Upper Jiao and acupoints on the Conception vessel. This heat transfer and penetration of moxibustion are considered manifestations of Deqi [59, 60], which is believed to be an important parameter in acupuncture and moxibustion treatment [61]. The number of correlations was significantly greater in the 60-min Long-snake-like moxibustion group than in the 30-min Long-snake-like moxibustion group. Specifically, there were correlations between Upper Jiao, Shenque (CV8), Zhongwan (CV12), Danzhong (CV17), Zhiyang (GV9), Dazhui (GV14), upper arm, thoracic segments, lumbar segments, renal region, popliteal fossa and fear of cold and cold extremities, lassitude and lack of strength, shortness of breath and laziness to speak, lumbar cold pain, abdominal fullness and distention, symptoms total score in the 60-min Long-snake-like moxibustion group. However, there was only one correlation between Zhiyang (GV9) and fear of cold and cold extremities in the 30-min Long-snake-like moxibustion group. This result suggests that the longer the duration of moxibustion, the greater the dose of heat stimulation. As the heat transfers further and penetrates deeper, more acupoints and regions are mobilized to tonify Yang. In the same course of treatment, 60-min duration generates a greater dose of moxibustion and a stronger effect on tonifying Yang.
One of the limitations of our trial is the small sample size. Considering the pathogenesis characteristic of CFS [2], only female subjects were recruited and examined. Further trials could enlarge the sample size or recruit male subjects to reduce the selection bias. Another limitation is that there were only two time points for TTM scanning in this trial. Increasing the course of treatment and adding additional scanning time points in further trials may be beneficial for analyzing the dynamic changes of dose–effect of Long-snake-like moxibustion and helping deeply explore the saturated dose rule of Long-snake-like moxibustion.
Conclusions
This trial evaluated the effect difference of Long-snake-like moxibustion with different dose of 60-m and 30-m duration, measured by subjective traditional scales and objective medical infrared imaging technology. In the same treatment course, 60-min Long-snake-like moxibustion is superior to 30-min Long-snake-like moxibustion in relieving physical fatigue and overall fatigue status, improving Spleen-Kidney Yang Deficiency symptoms, and raising the low heat state to the level of healthy people. This trial provides evidence for selecting the appropriate treatment duration for Long-snake-like moxibustion in treating CFS, and enriches the content of dose–effect research on moxibustion therapy.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CFS:
-
Chronic fatigue syndrome
- TCM:
-
Traditional Chinese medicine
- GV:
-
Governor Vessel
- TTM:
-
Thermal texture maps
- HCs:
-
Healthy control subject
- FS-14:
-
Fatigue scale-14
- SDS:
-
Self-rating depression scale
- SAS:
-
Self-rating anxiety scale
- SD:
-
Standard deviation
- Q1:
-
25th percentile
- Q3:
-
75th percentile
- CI:
-
Certificate interval
- CRF:
-
Case report form
- ITT:
-
Intention-to-treat
- BMI:
-
Body mass index
- CV:
-
Conception vessel
- T:
-
Thermal radiation value
References
Reeves WC, Lloyd A, Vernon SD, et al. Identification of ambiguities in the 1994 chronic fatigue syndrome research case definition and recommendations for resolution. BMC Health Serv Res. 2003;3(1):25–33. https://doi.org/10.1186/1472-6963-3-25.
Capelli E, Zola R, Lorusso L, et al. Chronic fatigue syndrome/myalgic encephalomyelitis: an update. Int J Immunopathol Pharmacol. 2010;23(4):981–9. https://doi.org/10.1177/039463201002300402.
Ng SM, Yiu YM. Acupuncture for chronic fatigue syndrome: a randomized, sham-controlled trial with single-blinded design. Altern Ther Health Med. 2013;19(4):21–6.
Tingting M, Jie W, Lijie Y, et al. Ginger-indirect moxibustion plus acupuncture versus acupuncture alone for chronic fatigue syndrome: a randomized controlled trial. J Tradit Chin Med. 2022;42(2):242–9. https://doi.org/10.19852/j.cnki.jtcm.20211214.003.
Oka T, Tanahashi T, Chijiwa T, et al. Isometric yoga improves the fatigue and pain of patients with chronic fatigue syndrome who are resistant to conventional therapy: a randomized, controlled trial. Biopsychosoc Med. 2014;8(1):27–35. https://doi.org/10.1186/s13030-014-0027-8.
Price JR, Mitchell E, Tidy E, et al. Cognitive behaviour therapy for chronic fatigue syndrome in adults. Cochrane Database Syst Rev. 2008;2008(3):CD001027. https://doi.org/10.1002/14651858.
White PD, Goldsmith KA, Johnson AL, et al. Comparison of adaptive pacing therapy, cognitive behaviour therapy, graded exercise therapy, and specialist medical care for chronic fatigue syndrome (PACE): a randomised trial. Lancet. 2011;377(9768):823–36. https://doi.org/10.1016/S0140-6736(11)60096-2.
Van Cauwenbergh D, De Kooning M, Ickmans K, et al. How to exercise people with chronic fatigue syndrome: evidence-based practice guidelines. Eur J Clin Invest. 2012;42(10):1136–44. https://doi.org/10.1111/j.1365-2362.2012.02701.x.
Kim HG, Yoo SR, Park HJ, et al. Indirect moxibustion (CV4 and CV8) ameliorates chronic fatigue: a randomized, double-blind, controlled study. J Altern Complement Med. 2013;19(2):134–40. https://doi.org/10.1089/acm.2011.0503.
Shu Q, Wang H, Litscher D, et al. Acupuncture and moxibustion have different Effects on fatigue by regulating the autonomic nervous system: a pilot controlled clinical trial. Sci Rep. 2016;6:37846. https://doi.org/10.1038/srep37846.
Zuo Z, Liu Z, Yuan K, et al. Effects and mechanism of the long-snake moxibustion on ankylosing spondylitis based on Th17/Treg/Th1 immune imbalance. Zhongguo Zhen Jiu. 2018;38(10):1053–7. https://doi.org/10.13703/j.0255-2930.2018.10.006.
Zhang W, Chen M, Hu J. Long-snake moxibustion for rheumatoid arthritis: a randomized controlled trial. Zhongguo Zhen Jiu. 2016;36(7):694–8. https://doi.org/10.13703/j.0255-2930.2016.07.005.
Xuan YC, Liu J, Huang YY, et al. Therapeutic effect of long-snake moxibustion combined with western medication on diarrhea type irritable bowel syndrome of spleen and kidney yang deficiency. Zhongguo Zhen Jiu. 2021;41(2):133–6. https://doi.org/10.13703/j.0255-2930.20191225-k0003.
Huang LR. Treating chronic fatigue syndrome with modified long snake moxibustion combined with acupuncture, a randomized controlled clinical study [D]. Chengdu: Chengdu University of Traditional Chinese Medicine; 2018.
Lu L, Fu JM, Feng FY, et al. Dose–effect relationship in treatment of chronic neck pain with the direct moxibustion of small moxa cone. Zhongguo Zhen Jiu. 2019;39(7):734–8. https://doi.org/10.13703/j.0255-2930.2019.07.015.
Li H, Sang L, Xia X, et al. Therapeutic duration and extent affect the effect of moxibustion on depression-like behaviour in rats via regulating the brain tryptophan transport and metabolism. Evid Based Complement Alternat Med. 2019;2019:7592124. https://doi.org/10.1155/2019/7592124.
Xiao AJ, He L, Ouyang X, et al. Comparison of the anti-apoptotic effects of 15- and 35-minute suspended moxibustion after focal cerebral ischemia/reperfusion injury. Neural Regen Res. 2018;13(2):257–64. https://doi.org/10.4103/1673-5374.226396.
Zhao JM, Wu LY, Liu HR, et al. Factorial study of moxibustion in treatment of diarrhea-predominant irritable bowel syndrome. World J Gastroenterol. 2014;20(37):13563–72. https://doi.org/10.3748/wjg.v20.i37.13563.
Hives L, Bradley A, Richards J, et al. Can physical assessment techniques aid diagnosis in people with chronic fatigue syndrome/myalgic encephalomyelitis? A diagnostic accuracy study. BMJ Open. 2017;7(11):e017521. https://doi.org/10.1136/bmjopen-2017-017521.
Twisk FN. The status of and future research into myalgic encephalomyelitis and chronic fatigue syndrome: the need of accurate diagnosis, objective assessment, and acknowledging biological and clinical subgroups. Front Physiol. 2014;5:109. https://doi.org/10.3389/fphys.2014.00109.
Almutairi B, Langley C, Crawley E, et al. Using structural and functional MRI as a neuroimaging technique to investigate chronic fatigue syndrome/myalgic encephalopathy: a systematic review. BMJ Open. 2020;10(8):e031672. https://doi.org/10.1136/bmjopen-2019-031672.
Chalder T, Berelowitz G, Pawlikowska T, et al. Development of a fatigue scale. J Psychosom Res. 1993;37(2):147–53. https://doi.org/10.1016/0022-3999(93)90081-p.
Jing MJ, Lin WQ, Wang Q, et al. Reliability and construct validity of two versions of chalder fatigue scale among the general population in Mainland China. Int J Environ Res Public Health. 2016;13(1):147. https://doi.org/10.3390/ijerph13010147.
Fernández-Cuevas I, Bouzas-Marins JC, Arnáiz-Lastras J, et al. Classification of factors influencing the use of infrared thermography in humans: a review. Infrared Phys Technol. 2015;71:28–55. https://doi.org/10.1016/j.infrared.2015.02.007.
Thermography Guidelines (TG)., Standards and protocols in clinical thermographic imaging. 2002. http://www.iact-org.org/professionals/thermog-guidelines.html.
Sun D. Study on infrared thermography characterization of liver qi stagnation syndrome population surface partition attachment: overview of medical infrared thermal imaging technology [D]. Chengdu: Chengdu University of Traditional Chinese Medicine; 2017.
Chen ZJ. Preliminary study on infrared thermography characteristics of Wagner grade 0 diabetic foot patients from the perspective of traditional chinese medicine[D]. Beijing: Beijing University of Traditional Chinese Medicine; 2021.
Ding GJ. The study on the correlation between moxibustion sensation and curative effect in treating chronic fatigue syndrome by needling LU7, KI6 combined with modified long snake moxibustion [D]. Chengdu: Chengdu University of Traditional Chinese Medicine; 2019.
Wang W, Russell A, Yan Y, Global Health Epidemiology Reference Group (GHERG). Traditional Chinese medicine and new concepts of predictive, preventive and personalized medicine in diagnosis and treatment of suboptimal health. EPMA J. 2014;5(1):4. https://doi.org/10.1186/1878-5085-5-4.
National Collaborating Centre for Primary Care (UK). Chronic fatigue syndrome/myalgic encephalomyelitis (or encephalopathy): diagnosis and management of chronic fatigue syndrome/myalgic encephalomyelitis (or encephalopathy) in adults and children. London: Royal College of General Practitioners (UK); 2007.
Yancey JR, Thomas SM. Chronic fatigue syndrome: diagnosis and treatment. Am Fam Physician. 2012;86(8):741–6.
Vink M, Vink-Niese A. Cognitive behavioural therapy for myalgic encephalomyelitis/chronic fatigue syndrome is not effective. Re-analysis of a cochrane review. Health Psychol Open. 2019;6(1):2055102919840614. https://doi.org/10.1177/2055102919840614.
Son CG. Analysis of patients visiting an oriental hospital with idiopathic chronic fatigue or chronic fatigue syndrome. J Korean Med. 2013;34:119–25.
Kwak KK, Cho JH, Son CG. Study on chronic fatigue syndrome from oriental medicine point of view. Korean J Orient Int Med. 2008;29:962–9.
Wang T, Xu C, Pan K, et al. Acupuncture and moxibustion for chronic fatigue syndrome in traditional chinese medicine: a systematic review and meta-analysis. BMC Complement Altern Med. 2017;17(1):163. https://doi.org/10.1186/s12906-017-1647-x.
You J, Ye J, Li H, et al. Moxibustion for chronic fatigue syndrome: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2021;2021:6418217. https://doi.org/10.1155/2021/6418217.
Hu XW, Deng CY, Tang LM, et al. Ginger-separated Snake Moxibustion improves Yang deficiency constitution by up-regulating serum adrenocorticotropic hormone and cortisol levels in Yang Deficiency Constitution volunteers. Zhen Ci Yan Jiu. 2018;43(12):773–6. https://doi.org/10.13702/j.1000-0607.180513.
Huang P, Deng CY, Jiang XM, et al. Observation on the clinical effect of long snake-like moxibustion in treating chronic fatigue syndrome of deficiency of heart and spleen. Guangming J Chin Med. 2020;35(13):2028–31.
Zheng SH, Zheng SZ, Wu YJ, et al. Clinical efficacy of long snake moxibustion on chronic fatigue syndrome with spleen and kidney Deficiency Type and its Effect on Cytokines. Chin Arch Tradit Chin Med. 2013;31(11):2555–7. https://doi.org/10.13193/j.issn.1673-7717.2013.11.036.
Billones RR, Kumar S, Saligan LN. Disentangling fatigue from anhedonia: a scoping review. Transl Psychiatry. 2020;10(1):273. https://doi.org/10.1038/s41398-020-00960-w.
Schwartz JE, Jandorf L, Krupp LB. The measurement of fatigue: a new instrument. J Psychosom Res. 1993;37(7):753–62. https://doi.org/10.1016/0022-3999(93)90104-n.
Başoğlu F, Öncü J, Kuran B, et al. The reliability and validity of the turkish version of multidimensional fatigue Inventory-20 for the evaluation of different dimensions of fatigue in patients with fibromyalgia. Turk J Phys Med Rehabil. 2020;66(4):436–43.
Shang Z, Jiang G. Fundamental theoretic research of thermal texture maps Isimulation and analysis of the relation between the depth of inner heat source and surface temperature distribution in isotropy tissue. Conf Proc IEEE Eng Med Biol Soc. 2004;2004:5271–3. https://doi.org/10.1109/IEMBS.2004.1404471.
Huth TK, Eaton-Fitch N, Staines D, et al. A systematic review of metabolomic dysregulation in chronic fatigue syndrome/myalgic encephalomyelitis/systemic exertion intolerance disease (CFS/ME/SEID). J Transl Med. 2020;18(1):198. https://doi.org/10.1186/s12967-020-02356-2.
Cortes Rivera M, Mastronardi C, Silva-Aldana CT, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: a comprehensive review. Diagnostics (Basel). 2019;9(3):91. https://doi.org/10.3390/diagnostics9030091.
Herman C, Cetingul MP. Quantitative visualization and detection of skin cancer using dynamic thermal imaging. J Vis Exp. 2011;51:2679. https://doi.org/10.3791/2679.
Bauer J, Hoq MN, Mulcahy J, et al. Implementation of artificial intelligence and non-contact infrared thermography for prediction and personalized automatic identification of different stages of cellulite. EPMA J. 2020;11(1):17–29. https://doi.org/10.1007/s13167-020-00199-x.
Murthy JN, van Jaarsveld J, Fei J, et al. Thermal infrared imaging: a novel method to monitor airflow during polysomnography. Sleep. 2009;32(11):1521–7. https://doi.org/10.1093/sleep/32.11.1521.
Guguvcevski L. Muscle fatigue in temporomandibuar disorder patients evaluated by electromyography. Adv Biology Earth Sci. 2017;2(1):117–21.
Armstrong CW, McGregor NR, Butt HL, et al. Metabolism in chronic fatigue syndrome. Adv Clin Chem. 2014;66:121–72. https://doi.org/10.1016/b978-0-12-801401-1.00005-0.
Mandarano AH, Maya J, Giloteaux L, et al. Myalgic encephalomyelitis/chronic fatigue syndrome patients exhibit altered T cell metabolism and cytokine associate-ons. J Clin Invest. 2020;130(3):1491–505. https://doi.org/10.1172/JCI132185.
Sotzny F, Blanco J, Capelli E, et al. Myalgic encephalomyelitis/chronic fatigue syndrome-evidence for an autoimmune disease. Autoimmun Rev. 2018;17(6):601–9. https://doi.org/10.1016/j.autrev.2018.01.009.
Bansal AS, Bradley AS, Bishop KN, et al. Chronic fatigue syndrome, the immune system and viral infection. Brain Behav Immun. 2012;26(1):24–31. https://doi.org/10.1016/j.bbi.2011.06.016.
Klimas NG, Broderick G, Fletcher MA. Biomarkers for chronic fatigue. Brain Behav Immun. 2012;26(8):1202–10. https://doi.org/10.1016/j.bbi.2012.06.006.
Kume S, Yamato M, Tamura Y, et al. Potential biomarkers of fatigue identified by plasma metabolome analysis in rats. PLoS ONE. 2015;10(3):e0120106. https://doi.org/10.1371/journal.pone.0120106.
Lin C, Sa ZY, Zhong XL, et al. Effect of deqi induced by needling sanyinjiao (SP6) on energy metabolism indicators in patients with primary Dysmenorrhea in cold and dampness stagnation pattern. Fujian J Tradit Chin Med. 2021;52(11):10–4. https://doi.org/10.13260/j.cnki.jfjtcm.012360.
Li Y, Sun C, Kuang J, et al. An invitro and numerical study of moxibustion therapy on biological tissue. IEEE Trans Biomed Eng. 2018;65(4):779–88. https://doi.org/10.1109/TBME.2017.2719633.
Hong XE, Zhang LY, Lin W, et al. Governor vessel moxibustion combined with warming acupuncture for knee osteoarthritis with yang deficiency and cold congelation based on the supporting-yang theory. Zhongguo Zhen Jiu. 2022;42(12):1357–62. https://doi.org/10.13703/j.0255-2930.20220617-k0002.
Chen R, Chen M, Xiong J, et al. Comparative effectiveness of the deqi sensation and non-deqi by moxibustion stimulation: a multicenter prospective cohort study in the treatment of knee osteoarthritis. Evid Based Complement Alternat Med. 2013;2013:906947. https://doi.org/10.1155/2013/906947.
Xie D, Liu Z, Hou X, et al. Heat sensitisation in suspended moxibustion: features and clinical relevance. Acupunct Med. 2013;31(4):422–4. https://doi.org/10.1136/acupmed-2013-010409.
Lv Z, Liu Z, Huang D, et al. The characterization of deqi during moxibustion in stroke rats. Evid Based Complement Alternat Med. 2013;2013:140581. https://doi.org/10.1155/2013/140581.
Acknowledgements
The authors would like to thank all the patients who agreed to participate in this trial. They also thank all the participants and staff who conducted and assisted in this trial.
Funding
This trial was externally supported by the government funding—Science and Technology Support Program of Science & Technology Department of Sichuan Province (No. 2020YFS0378).
Author information
Authors and Affiliations
Contributions
TM conceptualized and designed the study, provided study materials/patients, participated in the writing of the original draft and its review and editing. JW worked on the conceptualization and administrative support. RG and RZ worked on collection and assembly of data. JT worked on data analysis and interpretation. HL worked on the formal analysis, visualization, drafting/revision of the manuscript, reviewing, and editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The trial was conducted in accordance with the Declaration of Helsinki (as revised in 2013). Research ethics approval was attained from the Ethics Committee of Teaching Hospital of Chengdu University of TCM (No.2020KL-046). Informed consent was obtained from each patient.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Sensitivity analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Luo, H., Gong, R., Zheng, R. et al. Dose–effect of long-snake-like moxibustion for chronic fatigue syndrome: a randomized controlled trial. J Transl Med 21, 430 (2023). https://doi.org/10.1186/s12967-023-04250-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-023-04250-z