
Abstract
Background
There is increasing evidence demonstrating the importance of the neighbourhood built environment in supporting physical activity. Physical activity provides numerous health benefits including improvements in health-related fitness (i.e., muscular, cardiorespiratory, motor, and morphological fitness). Emerging evidence also suggests that the neighbourhood built environment is associated with health-related fitness. Our aim was to summarize evidence on the associations between the neighbourhood built environment and components of health-related fitness in adults.
Methods
We undertook a systematic review following PRISMA guidelines. Our data sources included electronic searches in MEDLINE, Embase, CINAHL, Web of Science, SPORTDiscus, Environment Complete, ProQuest Dissertations and Theses, and Transport Research International Documentation from inception to March 2021. Our eligibility criteria consisted of observational and experimental studies estimating associations between the neighbourhood built environment and health-related fitness among healthy adults (age ≥ 18 years). Eligible studies included objective or self-reported measures of the neighbourhood built environment and included either objective or self-reported measures of health-related fitness. Data extraction included study design, sample characteristics, measured neighbourhood built environment characteristics, and measured components of health-related fitness. We used individual Joanna Briggs Institute study checklists based on identified study designs. Our primary outcome measure was components of health-related fitness (muscular; cardiorespiratory; motor, and morphological fitness).
Results
Twenty-seven studies (sample sizes = 28 to 419,562; 2002 to 2020) met the eligibility criteria. Neighbourhood destinations were the most consistent built environment correlate across all components of health-related fitness. The greatest number of significant associations was found between the neighbourhood built environment and morphological fitness while the lowest number of associations was found for motor fitness. The neighbourhood built environment was consistently associated with health-related fitness in studies that adjusted for physical activity.
Conclusion
The neighbourhood built environment is associated with health-related fitness in adults and these associations may be independent of physical activity. Longitudinal studies that adjust for physical activity (including resistance training) and sedentary behaviour, and residential self-selection are needed to obtain rigorous causal evidence for the link between the neighbourhood built environment and health-related fitness.
Trial registration
Protocol registration: PROSPERO number CRD42020179807.
Similar content being viewed by others

Background
Participation in regular physical activity is associated with a reduced risk of developing diabetes [1], cardiovascular disease [2], certain cancers [3] and premature mortality [4]. Notably, physical activity is also positively associated with health-related fitness [5]. Health-related fitness reflects physiological attributes that delay the onset of morbidity from diseases that may result from living a physically inactive lifestyle [6]. Traditional definitions of health-related fitness (i.e., cardiorespiratory endurance, muscular endurance, muscular strength, body composition and flexibility) [7] have since been updated to be more encompassing [8]. Current definitions of health-related fitness are multidimensional and include morphologic (e.g., body composition or flexibility) muscular (e.g., grip strength or endurance), cardiorespiratory (e.g., \(\dot{V}{O}_2\ \mathit{\max}\) or sustained cardiorespiratory capacity), motor (e.g., balance or proprioceptive activity), and metabolic (e.g., blood lipid or glucose levels) components [6]. After controlling for body mass index (BMI) and waist circumference, objective measures of body composition (including the distribution of adipose tissue) have been linked to incident cardiovascular disease [9]. Findings from a meta-analysis demonstrated that decreases in grip strength were associated with an increased risk of all-cause and cardiovascular mortality [10]. Associations between lower grip strength in mid-life with functional limitations and disability in older adulthood have also been observed [11]. Cardiorespiratory fitness, has been shown to be associated with cardiovascular disease risk in adults [12].
Higher intensity physical activity can improve muscular [13], cardiorespiratory [13], and morphological fitness [14]; however, even lower intensity activities, such as walking, may improve health-related fitness [15]. Qualitative [16] and quantitative [17] evidence consistently demonstrates links between neighbourhood built environment and physical activity. Key built environment features that support physical activity include density (i.e., residential or population), connectivity (i.e., many potential routes, short block sizes, many intersections), and land uses (i.e., recreational and utilitarian destinations) [16, 17]. Giles-Corti et al. developed [18] and later expanded [19] a framework positing potential pathways by which the local built environment is associated with physical activity and health. The framework highlights important built characteristics including design (e.g., street layout and connectivity), density (e.g., compactness of residential population), transit (e.g., proximity and access), destination proximity (e.g., distance to local destinations), diversity (e.g., mixed residential, commercial, and recreational destinations), desirability (e.g., safety and aesthetics) and distributed features (e.g., resources equitably distributed across different populations) [18, 19]. Given the connections between the built environment and physical activity, and physical activity and health-related fitness, neighbourhood built environments may play a vital role in supporting health-related fitness in adults.
Health-related fitness can be influenced by genetic factors, lifestyle behaviours, personal attributes, and physical and social environments [8]. Notably, some evidence suggests that associations between the built environment and health-related fitness remain after controlling for physical activity [20,21,22,23]. The persistent relationship may reflect the presence of independent pathways between the built environment and health-related fitness, the existence of other mediators (e.g., sedentary behavior and diet), or inadequate adjustment for physical activity. For example, studies have found the availability of food destinations to be associated with morphological fitness [24] and sedentary time to be association with functional-related fitness in older adults [25]. Both sedentary behaviour and diet are associated with built environment [26,27,28].
While several studies have found significant associations between some features of the neighbourhood built environment and health-related fitness [23, 29,30,31], this literature has not been systematically synthesized nor critically evaluated. Therefore, the aim of this study is two-fold: (1) to summarize and critically appraise the existing literature on the associations between the neighbourhood built environment and health-related fitness in the adult general population, and; (2) to identify and summarize studies estimating the associations between the neighbourhood built environment and health-related fitness that also control for physical activity.
Methods
This systematic review is based on a published study protocol [32], was registered in the International prospective register of systematic reviews (PROSPERO; ID number: CRD42020179807), and follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary material; S1) [33]. We deviated from the protocol by having only one reviewer (LF) screen all initial titles and abstracts, however, two reviewers (LF and CC) screened the potentially relevant full-texts and collaboratively extracted study data (i.e., through a consensus approach).
Search strategy
Databases were searched from inception to March 2021 with no language or location restrictions. MEDLINE (Ovid), Embase (Ovid), CINAHL (EBSCO), Web of Science, SPORTDiscus (EBSCO), and Environment Complete (EBSCO) were search for published evidence (Supplementary material; S2). Our search was supplemented with an exploration of unpublished evidence from ProQuest Dissertations and Theses. Finally, Transport Research International Documentation was also explored for relevant unpublished and published evidence.
Study selection
Citations were collated and uploaded into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org) and duplicates were removed.
Eligibility criteria
Types of studies
We included observational and experimental studies that reported on quantitative results. Our review excluded qualitative studies and literature reviews.
Participants
We included studies undertaken with healthy adults (≥18 years of age). We excluded studies undertaken with children or adolescents, athletes, or clinical populations.
Exposure(s)
Exposure variables eligible for inclusion were built environment characteristics measured using objective (e.g., Geographical Information Systems or environmental audits) or self-reported (e.g., questionnaire) approaches.
Outcomes
Eligible studies included objective (e.g., researcher-administered field tests or laboratory testing) or self-reported measures (e.g., survey questionnaires) of health-related fitness. Health-related fitness included any measures of muscular, cardiorespiratory, motor, and morphological fitness. We excluded metabolic fitness because compared to the other components of health-related fitness, recent systematic reviews have summarized the associations between the built environment and cardio-metabolic health [34,35,36,37,38,39]. Within morphological fitness, outcomes of body composition were included if studies distinguished between fat and fat-free mass (e.g., body fat percentage), but they were excluded if they could not (e.g., BMI and waist-to-hip-ratio).
Data extraction
Data extraction included title, author, year of study, journal, study design, geographical location, sample size, mean age and age range, participant sex/gender distribution, data collection date, study duration, statistical technique, and estimate type(s), whether the built environment was objectively-measured or self-reported, whether the components of health-related fitness were objectively-measured or self-reported, the built environment characteristics measured, the component of health-related fitness measured, built environment exposure, covariates present in the adjusted results, whether adjustment was made for physical activity, and the main study findings.
Assessment of study quality
Study quality was assessed using the Joanna Briggs Institute (JBI) critical appraisal tools for cross-sectional [40] (8 items), quasi-experimental [41] (9-items) or cohort [40] (12-items) studies. We used three specific study quality tools to accommodate the different studies designs that we expected to encounter in this literature [17, 42,43,44].
Data synthesis
A narrative synthesis was completed by categorizing perceived or objectively measured individual (e.g., street connectivity) or index (e.g., walkability) built environment measures as well as perceived or objectively measured components of health-related fitness (e.g., cardiorespiratory fitness). Using an established framework [18, 19], built environment characteristics were grouped into one of seven feature categories (i.e., design, density, transit, destination proximity, diversity, desirability, and distributed). We also added an eighth category – “Composite or Other” features – which included measures that combined individual built environment features into a single index or score (e.g., “walkability”) or where a single built environment variable spanned multiple features (e.g., urban infrastructure improvement). Statistically significant positive, negative, and non-significant associations were summarized.
Results
Study identification
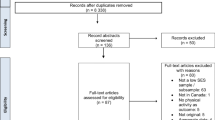
After removal of duplicates, 27,100 records were screened. After reviewing 881 full-text reports, 25 reports were included [20,21,22,23,24, 29,30,31, 45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61]. Two of the included reports each included two different studies [24, 50] within the same paper and the findings of each study were reported separately; thus, 27 studies were included in the final narrative synthesis (Fig. 1).

PRISMA flow diagram
Characteristics of included studies
Study design
Table 1 shows the characteristics of the included studies. The majority (n = 21) of studies used cross-sectional designs [21, 23, 24, 29,30,31, 46,47,48,49,50,51,52,53, 55,56,57,58,59,60,61], with the remainder including cohort [20, 22, 24, 50, 54] (n = 5) or quasi-experimental [45] (n = 1) designs. Approximately half of studies (n = 14) were undertaken in the United States of America (USA) [22, 24, 29,30,31, 46, 48, 50, 51, 54, 56, 57] with the remainder undertaken in Japan [20, 49, 61] (n = 3), the United Kingdom (UK) [47, 58, 59] (n = 3), Canada [23, 55] (n = 2), France [45, 52] (n = 2), Brazil [53] (n = 1), China [21] (n = 1), and the Czech Republic [60] (n = 1). Sample sizes across studies ranged from 28 [45] to 419,562 [59]. Six studies included older adults (≥ 60 years) only [20, 22, 45, 49, 53, 61]. Six studies included female-only samples [45, 50, 51, 54, 60], while the remainder included multi-sexed/gendered samples [20,21,22,23,24, 29,30,31, 46,47,48,49, 52, 53, 55,56,57,58,59, 61].
Built environment measures
Among the 17 studies that included an objective measure of the built environment, neighbourhood geography was either operationalized using ego-centric spatially-defined buffers (or polygons) or distances around or from participants geo-located residential households [20, 29, 49,50,51,52, 55, 58, 59, 61] (n = 11) or by administrative boundaries [22, 24, 30, 45, 50, 53] (n = 6). The size of the buffers used ranged from 500m [58] to 1600 m [29, 49], with 800m [29, 49,50,51, 59] (n = 6) being the most commonly used definition. Among the 10 studies that included a measure of self-reported built environment, four used the Neighborhood Environment Walkability Scale (NEWS) [21, 48, 59, 60], two studies captured perceptions about places in the neighbourhood to be active [54, 57], one study used the Physical Activity Neighborhood Environment Scale (PANES) [23], one study each captured perceived neighbourhood disorder [46], perceived neighbourhood quality [47], and perceived safety [56].
The most common neighbourhood built environment characteristics measured included desirability (n = 13) [21, 22, 24, 29, 31, 47, 48, 50, 51, 53, 56, 58, 60], followed by diversity (n = 12) [21, 24, 29, 31, 48,49,50,51, 54, 57, 60, 61], design (n = 10) [20, 21, 24, 29, 31, 48,49,50,51, 60] and composite or other features (n = 10) [21, 23, 30, 31, 45, 46, 49, 50, 57, 60], density (n = 9) [20, 21, 29, 48, 49, 52, 59,60,61], destination proximity (n = 6) [20, 29, 48, 54, 55, 60] and transit (n = 2) [20, 49] features. No study measured distributed features. The most common built environment elements measured under diversity features included the availability or presence of specific destination types [20, 21, 24, 29, 31, 48, 49, 51, 52, 55, 57, 59,60,61]. Street connectivity and residential density were the most common built environment elements under design and density, respectively [20, 21, 24, 29, 31, 48, 49, 51, 52, 59,60,61]. For desirability features, both greenspace and perceived neighbourhood aesthetics were the most common elements measured [21, 24, 29, 31, 48, 51,52,53, 58, 60]. Desirability also included measures of safety [21, 31, 48, 50, 51, 53, 56, 60]. Walkability was the most common element under composite or other features [21, 23, 30, 31, 49, 60].
Health-related fitness measures
With the exception of two studies [23, 57], all health-related fitness measurements were objectively measured [20,21,22, 24, 29,30,31, 45,46,47,48,49,50,51,52,53,54,55,56, 58,59,60,61]. There was a total of eight studies that included at least one measure of muscular fitness [20,21,22,23, 31, 46, 49, 61]. Six studies included grip strength [20,21,22, 46, 49, 61], while a timed curl-up test [21], a maximal repetition curl up test (up to 75 repetitions) [31], timed push-up [31], a 5-repetion sit-to-stand test [61], and self-reported muscular strength were each reported in individual studies [23]. Among the 12 studies measuring cardiorespiratory fitness, six used an estimation of \(\dot{V}{O}_2\ \mathit{\max}\) [29,30,31, 50, 55, 57], three included habitual walking speed [22, 49, 61], two included timed distance tests [45, 54], and one included self-reported cardiorespiratory fitness [23]. Among the four studies measuring motor fitness, three used the Timed Up-and-Go test [49, 53, 61] and two used a timed one-foot standing test [21, 49]. There was a total of 16 studies that included at least one measure of morphological fitness [20, 21, 23, 24, 31, 45, 47, 48, 50,51,52, 54, 56, 58,59,60]. Fourteen studies included measurements of body composition [20, 21, 24, 31, 47, 48, 50,51,52, 54, 56, 58,59,60], two studies used Sit-and-Reach tests [21, 45], and one reported perceived flexibility [23].
Study quality
Most studies (n = 17) were assessed to have the highest methodological quality score possible for their respective study design (cross-sectional, cohort or quasi-experiments). Cross-sectional studies of lower methodological quality tended to inadequately describe the sample design and setting and the reliability or validity of the built environment measures, and/or they did not control for confounders [31, 47, 48, 55, 56, 60]. Quasi-experiments of lower quality tended to provide unclear descriptions of their follow-up data collection [45]. Lower quality cohort studies tended to inadequately describe the follow-up data collection or the reliability or validity of the built environment measures, and/or they did not control for confounders [20, 24, 54].
Adjustment for physical activity
Out of the 27 studies, eleven (40.7%) adjusted for physical activity. Physical activity was adjusted for in four of the eight studies that assessed muscular fitness [20, 21, 23, 61], in five of the twelve studies that assessed cardiorespiratory fitness [23, 29, 30, 50, 61], in two of the four studies that assessed motor fitness [21, 61], and in the eight of the sixteen studies that assessed morphological fitness [20, 21, 23, 47, 50, 52, 56, 59].
Associations between the neighbourhood built environment and health-related fitness
Muscular fitness
Table 2 summarizes the associations between neighbourhood built features and muscular fitness. Excluding distributed features, all other built features were examined in relation to muscular fitness. Across these features, all but two studies found either positive or null associations with muscular fitness.
Self-reported street connectivity was positively associated with curl-up performance in a cross-sectional study of Chinese women [21] while topography (i.e., slope steepness) was positively associated with grip strength in a cohort of Japanese males [20]. No studies found neighbourhood safety to be associated with muscular fitness [21, 31]. Brown et al. [22] found positive associations between neighbourhood architecture and grip strength, while Sun et al. [21] found positive associations between self-reported neighbourhood aesthetics and curl-up performance in males. In a cross-section of older Japanese adults, having more utilitarian destinations (men and women), recreational facilities (men and women), and medical facilities (men only) in the neighbourhood was associated with better performance in the Sit-to-Stand test [61]. Moreover, among women, a greater number of neighbourhood utilitarian destinations and medical facilities was positively associated with grip strength [61]. Among a cohort of older Japanese women, neighbourhood bus stop density was negatively associated with grip strength [20]. Composite features were also associated with muscular fitness. In a cross-sectional sample of adults from the USA, neighbourhood physical disorder (vandalism/graffiti, rubbish/litter, vacant/deserted homes, and crime) was negatively associated with grip strength, although the study did not adjust for physical activity [46]. In a cross-sectional study of Canadian adults, self-reported neighbourhood walkability was positively associated with perceived muscle strength [23].
Adjusting for physical activity, there were five positive, one negative and ten null associations between built environment features and muscular fitness. Although attenuated, after adjustment for self-reported frequency of achieving sufficient MVPA (≥30 minutes/day) in the past week and self-reported days of resistance training in a usual week, perceived overall neighbourhood walkability was still positively associated perceived muscular fitness in a Canadian population [23]. After adjusting for self-reported physically activity habit (yes/no), land slope remained positively associated and bus stop density negatively associated, with objectively measured grip strength in Japanese adults [20]. In another Japanese sample, the number of neighbourhood destinations were positively associated with objectively measured grip strength after adjusting for self-reported total (i.e., occupation, household, and leisure) physical activity [61]. In a sample of Chinese adults, after adjustment for self-reported total MVPA (i.e., weekly MET-minutes), for men perceived neighbourhood aesthetics and for women street connectivity, were positively associated with curl-up performance [21].
Cardiorespiratory fitness
Table 3 summarizes the associations between the neighbourhood built environment and cardiorespiratory fitness. Excluding distributed features, all other built features were examined in relation to cardiorespiratory fitness. Among these, transit features were not associated with cardiorespiratory fitness, while the other features were found to have positive or null associations with cardiorespiratory fitness.
A cross-sectional analysis of American adults, found that intersection density was positively associated with maximal metabolic equivalent of task (MET) values [29]. In older Japanese adults, population density was positively associated with an increased walking speed [61]. No studies found neighbourhood safety to be associated with cardiorespiratory fitness [31, 49, 50]. A cross-sectional study found that a front facing architecture type (including porches, stoops, and buildings built above grade) was positively associated with gait speed in a cohort of older Hispanic Americans [22]. Further, Hoehner et al. [29] found positive cross-sectional associations between a greater proportion of vegetation in the neighbourhood and maximal METs. In cross-sectional associations, the number of private exercise facilities, and community centres were positively associated with maximal METs and habitual walking speed, in samples of American [29] and Japanese [61] adults, respectively. In three separate cross-sectional samples, distance to dance studios and baseball diamonds was positively associated with \(\dot{V}{O}_2\ \mathit{\max}\) in Canadian adults [55], perception of places to walk in the neighbourhood was positively correlated with 1-mile walk scores in American women [54], and perceptions of convenient neighbourhood facilities was positively associated with estimated \(\dot{V}{O}_2\ \mathit{\max}\) in American adults [57]. Composite built environment associations with cardiorespiratory fitness included an intervention of older French women, where an improved urban environment consisting of a pedestrian circuit, improved roadway accessibility and rehabilitation of a central square, was positively associated with 6-minute walk scores [45]. In a cross-section of American adults, more walkable neighbourhoods, and non-auto commuting neighbourhoods, were positively associated with maximal METs for males and females, and males only, respectively [30]. In a cross-section of Canadian adults, self-reported neighbourhood walkability was positively associated with perceived cardiorespiratory fitness [23].
Among studies that adjusted for physical activity, there were seven positive and nine null associations between built environment features and cardiorespiratory fitness. Although attenuated, after adjusting for self-reported weekly MET-minutes of outdoor physical activity, traditional core neighbourhoods remained positively associated with maximal metabolic equivalents obtained through a treadmill test in American adults [19]. In another sample of American adults, after adjustment for self-reported weekly MET-minutes of MVPA, associations between and intersection density and maximal MET were no longer statistically significant; however, associations between greenspace (positive), the number of exercise facilities in the neighbourhood (positive), and distance to the closest city center (negative) remained significant [29]. Moreover, after adjustment for self-reported MVPA (≥30 minutes/day) in the past week and self-reported days of resistance training in a usual week, perceived overall neighbourhood walkability remained positively associated with self-reported cardiorespiratory fitness in a sample of Canadian adults [23]. Further, in a sample of Japanese older adults, population density and the number of community centers in the neighbourhood remained positively associated with walking speed after adjusting for total (i.e. occupational, household and leisure) self-reported physical activity measured using the Physical Activity Scale for the Elderly [61].
Motor fitness
Table 4 summarizes the associations between the neighbourhood built environment and motor fitness. Excluding distributed and destination features proximity, all other built features were examined in relation to motor fitness. Across these features, transit, desirability, and composite or other features were not found to be associated with motor fitness while design, density, and diversity were found to be positively or not associated with motor fitness.
A cross-sectional study of older Japanese males, population density within a 1600 m neighbourhood buffer, and intersection density within an 800 m neighbourhood buffer was positively associated with timed one-legged stance scores (with eyes open) [49]. Although the study did not adjust for physical activity. There were no associations between safety [21, 53] or aesthetics [21, 53] of the neighbourhood built environment and motor fitness. In the same sample of older Japanese males, availability of destinations within the 1600 m neighbourhood buffer were positively associated with timed one-legged stance scores (with eyes open) [49]. There were no associations between composite built environment measures and motor fitness [21, 49].
Associations between the built environment and motor fitness were not statistically significant after adjustment for physical activity [21, 61].
Morphological fitness
Table 5 summarizes the associations between the neighbourhood built environment and morphological fitness. Excluding distributed features, all other built features were examined in relation to morphological fitness. Among these features, for morphological fitness negative associations were found for transit, null associations found for destinations, negative and null associations found for design, and negative, null, and positive associations found for density, diversity, desirability, and composite or other features.
A cohort study of American adults found intersection density negatively associated with changes in visceral adipose tissue [24]. A cross-sectional study of French adults found residential density negatively associated with both fat mass index and percent fat mass in males [52]. A cross-sectional study in the UK found a curvilinear relationship between residential density and body fat [59]. Specifically, residential density was positively associated with body fat ≤1800 units per km [2] then negatively associated with body fat > 1800 units per km2 [59]. Perceptions of neighbourhood safety were negatively associated with visceral adipose tissue in a cross-section of African American females [56]. A cross-sectional study of Chinese adults found that perceived pedestrian and traffic safety was negatively associated with sit-and-reach scores in males [21]. Lee et al. [24] found that greenspace was positively associated with change in visceral adipose tissue in a cohort of American adults. Conversely, in a cross-sectional sample of UK adults, residential greenness was negatively associated with body fat [58].
A cross-sectional study of American university students found perceptions of access to destinations was negatively associated with body fat percentage in males [48]. A cross-sectional study of ethnic minority American women found objectively measured neighbourhood amenities were negatively associated with body fat percentage [51]. Lee et al. [24] found that total food stores, full-service restaurants, fast food restaurants, supermarkets, and convenience stores was negatively associated with a change in visceral adipose tissue. Bus stop density was negatively associated with skeletal mass index in a cohort of Japanese males [20]. Perceptions of neighbourhood access to services and land use mix diversity were negatively associated with sit-and-reach scores in Chinese males [21].
For composite features, an intervention including older French women found an improved urban environment consisting of a pedestrian circuit, improved roadway accessibility and rehabilitation of a central square, to be positively associated with sit-and-reach test scores [45]. In cross-sectional analyses of three different cohorts, Ellaway et al. [47] found that an index of perceived neighbourhood problems (vandalism, litter, crime, youth disorderly conduct, and foul odor) was positively associated with change in body fat percentage over time. In Canadian adults, McCormack, et al. [23] found that perceptions of neighbourhood walkability and a park quality score were positively associated with perceived flexibility.
Adjusting for physical activity there were five positive, four negative and fourteen null associations with morphological fitness. After adjusting for the self-reported number of days per week performing vigorous exercise (≥20 minutes continuous), body fat percent remained positively associated with perceived neighbourhood problems [47]. Further, after adjusting for different levels of activity in varying occupations, residential density was inversely associated with fat mass index and percent fat mass in males [52]. Moreover, after adjustment for self-reported weekly MVPA (≥30 minutes/day) and self-reported days of resistance training in a usual week, perceived overall neighbourhood walkability remained positively associated with self-reported flexibility among Canadian adults [23]. Among Japanese older males, bus stop density was negatively associated with skeletal muscle index after adjusting self-reported physically active habit [20]. Adjusting for physical activity measured via an active living index (i.e., frequency and duration of physical activities minus frequency and duration of sedentary behavior), neighbourhood safety was positively associated with visceral and total adipose tissue in premenopausal women [56]. In in a large UK sample, after adjustment for self-reported physical activity (weekly MET hours), population density was found to have a non-linear association with objectively measured whole body fat [59]. Among Chinese males, perceived neighbourhood destinations and safety was negatively associated with sit and reach performance, after adjustment for self-reported MVPA in weekly MET minutes [21].
Discussion
We found 27 different studies that estimated the relationship between the neighbourhood built environment and health-related fitness. The reviewed evidence suggests that specific built environment features are more often than not to have either a positive or no association with health-related fitness. Moreover, this evidence suggests that associations between the built environment and health-related fitness persist, albeit attenuated, after controlling for physical activity. Using the updated built environment framework by Giles-Corti et al. [19] we found specific built characteristics associated with design, density, diversity, and desirability features to be the most commonly studied; while no studies examined built characteristics associated with distributed features.
The most common component of health-related fitness investigated was morphological fitness, with an emphasis on body composition. The negative associations between the built environment and body composition found in our review tend to support findings from previous reviews summarizing evidence related to built environment and weight outcomes [42, 43, 62]. Our findings suggest that having multiple, easily accessible destinations within a neighbourhood may favorably influence body composition. This result is congruent with longitudinal findings suggesting that having multiple, easily accessible destinations within a neighbourhood is linked to favorable changes in physical activity behaviour [17, 63].
The second most common association between the neighbourhood built environment and health-related fitness category was with cardiorespiratory fitness, and in general, measurements of estimated maximal aerobic capacity. Given the link between physical activity and cardiorespiratory fitness, our findings tend to support those that have been found previously between the built environment and physical activity [17, 63]. Similar to associations between the built environment and morphological fitness, having multiple destinations within a neighbourhood that are easily accessible was associated with favorable cardiorespiratory fitness. There are multiple lines of evidence, including cross-sectional [17, 44], longitudinal [63], and natural experiments [63], indicating favorable changes in physical activity behaviour with improvements in neighbourhood destinations.
Overall, the results of our review indicate that physical activity likely mediates, at least partially, associations between the neighbourhood built environment and health-related fitness. There are numerous explanations as to the mechanisms explaining how the built environment might be positively associated with health-related fitness. For example, carrying heavy loads in the hands is related to forearm musculature activity [64] and muscular fitness, therefore, in areas with a higher land-use mix, residents may walk to complete daily errands and carry items back to their residence, which may slow impairments to activities of daily living [65]. Recreational facilities located within walking distance of home, where resistance or aerobic training might be performed, may explain positive associations between the neighbourhood built environment and cardiorespiratory and muscular fitness. Increases in motor fitness has been shown through proprioceptive exercises such as wobble boards or unstable activities [66]. Speculatively, neighbourhoods with high population density, street connectivity, and land use mix, may provide opportunities to manoeuvre around obstacles (i.e., people, benches, traffic bollards etc.), which may emulate some movements undertaken during structured proprioceptive exercises. Among older adults, more frequent falls, which are associated with motor fitness [67], have been found in peripheral areas compared with city areas [68]. There is also consistent evidence demonstrating associations between neighbourhood walkability and walking [69, 70], which subsequently could result in improved cardiovascular [71], and morphological fitness [72].
However, other pathways may exist linking built environment with fitness that are not mediated by physical activity. For example, traffic density, which is associated with the built environment (e.g., air pollution) [19], can have detrimental effects on cardiorespiratory fitness [73, 74]. Diet, which is associated with morphological fitness [75], is also associated with the built environment (e.g., proximity and availability of fast food restaurants, supermarkets, and convenience stores) [62, 76].
Our findings suggest that the built environment may have effects on health-related fitness independent of physical activity. However, studies adjusting for physical activity did so using self-reported physical activity, which may not accurately capture the total volume nor intensities of physical activity undertaken. Moreover, among these studies few included measures of transport-related physical activity that may be more strongly associated with the built environment [77].
Strengths and weaknesses
A strength of our review is the overall breadth of included exposures, outcomes, and study designs. Capturing multiple components of health-related fitness allowed for a broader scope of the literature to be evaluated and to better theorize the multiple ways in which the built environment might impact health-related fitness. However, our broader research objective may have contributed to heterogeneous sample of studies included in our review which together with their dissimilar sample designs and methods, limited our ability to conduct a meta-analysis.
Limitations common in the literature exploring the relationships between physical activity and the neighbourhood built environment were also present in studies included this review. The lack of control for residential exposure time [78] and residential self-selection [79] was pronounced in our summary. In our review, we only found two of studies that controlled for length of residential exposure time [49, 50]. The lack of control for residential self-selection is also an important variable in neighbourhood built environment research; however, we found no studies controlling for this potential confounder. This confounder is potential important because individual who undertake physical activity for the main purpose of improving or maintaining their health-related fitness may choose to reside in neighbourhoods that have built features that support desired physical activities (e.g., access to parks, pathways, recreational facilities). Speculatively, not adjusting for residential self-selection could lead to over-estimates of the association between the built environment and health-related fitness, especially in cross-sectional studies [79]. Further, our study quality tools assessed the quality of reporting limiting our ability to assess bias. Moreover, as many of the identified studies were cross-sectional in design assessment of causality is limited.
Future directions
Evidence suggests that the built environment, through its potential influence on physical activity, is associated with a range of health outcomes such as cardiovascular disease, overweight and obesity, and type 2 diabetes [36]. Findings from our review suggest that health-related fitness is another important factor that should be considered when exploring the role of the built environment in supporting health, especially given its relationships both with physical activity [5] and chronic disease [6]. Future research is needed to examine the causal pathways between the built environment and health-related fitness, not only via physical activity but also other potential mediators (e.g., sedentary behaviour, air pollution). To generate rigorous evidence for informing urban design and public health policy and interventions, this future research should include longitudinal, experimental, and quasi-experimental study designs that incorporate objective measures of the built environment, health-related fitness, and physical activity (and other mediators).
Conclusion
The neighbourhood built environment appears to be associated with all components of health-related fitness (i.e., muscular, cardiorespiratory, motor, and morphological fitness). Somewhat expectedly, our findings of the built environment-health-related fitness relationship tend to mirror the built environment-physical activity evidence in that a more supportive neighbourhood built environments can support higher levels of physical activity [17, 63]. However, while physical activity might be an important mediator between the built environment and health-related fitness, our findings suggest there are potentially behaviours or factors other than physical activity that might explain some of the association between the neighbourhood built environment and health-related fitness. The relationship between the neighbourhood built environment and health-related fitness may be a promising area to improve public health. However, to make firm policy, practice, and design recommendations, future research on the associations between the neighbourhood environment and health-related fitness that controls for important confounders is needed (e.g., objectively-measured physical activity, resistance training, sedentary behaviour, diet, neighbourhood exposure, and residential self-selection).
Built environment definitions were adapted from Giles-Corti et al. [18] and Giles-Corti et al. [19]
Health-related fitness definitions were adapted from Caspersen et al. [80], Shephard [8], and Vanhees et al. [6]
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- JBI:
-
Joanna Briggs Institute
- MET:
-
Metabolic equivalent of task
- USA:
-
United States of America
- UK:
-
United Kingdom
- NEWS:
-
Neighborhood Environment Walkability Scale
- PANES:
-
Physical Activity Neighborhood Environment Scale
- MVPA:
-
Moderate-to-vigorous physical activity
References
Aune D, Norat T, Leitzmann M, Tonstad S, Vatten LJ. Physical activity and the risk of type 2 diabetes: a systematic review and dose-response meta-analysis. Eur J Epidemiol. 2015;30(7):529–42.
Wahid A, Manek N, Nichols M, Kelly P, Foster C, Webster P, et al. Quantifying the association between physical activity and cardiovascular disease and diabetes: a systematic review and meta-analysis. J Am Heart Assoc. 2016;5(9):e002495.
Kyu HH, Bachman VF, Alexander LT, Mumford JE, Afshin A, Estep K, et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: systematic review and dose-response meta-analysis for the global burden of disease study 2013. BMJ. 2016;354:i3857.
Ekelund U, Tarp J, Steene-Johannessen J, Hansen BH, Jefferis B, Fagerland MW, et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta-analysis. BMJ. 2019;366:l4570.
Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ. 2006;174(6):801–9.
Vanhees L, Lefevre J, Philippaerts R, Martens M, Huygens W, Troosters T, et al. How to assess physical activity? How to assess physical fitness? Eur J Cardiovasc Prev Rehabil. 2005;12(2):102–14.
Ivory VC, Blakely T, Pearce J, Witten K, Bagheri N, Badland H, et al. Could strength of exposure to the residential neighbourhood modify associations between walkability and physical activity? Soc Sci Med. 2015;147:232–41.
Shephard RJ. Physical activity, fitness, and health: the current consensus. Quest. 1995;47(3):288–303.
Chen GC, Arthur R, Iyengar NM, Kamensky V, Xue X, Wassertheil-Smoller S, et al. Association between regional body fat and cardiovascular disease risk among postmenopausal women with normal body mass index. Eur Heart J. 2019;40(34):2849–55.
Lee J. Associations between handgrip strength and disease-specific mortality including Cancer, cardiovascular, and respiratory diseases in older adults: a meta-analysis. J Aging Phys Act. 2020;28(2):320–31.
Rantanen T, Guralnik JM, Foley D, Masaki K, Leveille S, Curb JD, et al. Midlife hand grip strength as a predictor of old age disability. JAMA. 1999;281(6):558–60.
Blair SN, Cheng Y, Holder JS. Is physical activity or physical fitness more important in defining health benefits? Med Sci Sports Exerc. 2001;33(6 Suppl):S379–99 discussion S419-20.
Menz V, Marterer N, Amin SB, Faulhaber M, Hansen AB, Lawley JS. Functional Vs. running low-volume high-intensity interval training: effects on VO2max and muscular endurance. J Sports Sci Med. 2019;18(3):497–504.
Rosique-Esteban N, Babio N, Diaz-Lopez A, Romaguera D, Alfredo Martinez J, Sanchez VM, et al. Leisure-time physical activity at moderate and high intensity is associated with parameters of body composition, muscle strength and sarcopenia in aged adults with obesity and metabolic syndrome from the PREDIMED-plus study. Clin Nutr. 2019;38(3):1324–31.
Fuzeki E, Engeroff T, Banzer W. Health benefits of light-intensity physical activity: a systematic review of accelerometer data of the National Health and nutrition examination survey (NHANES). Sports Med. 2017;47(9):1769–93.
Salvo G, Lashewicz BM, Doyle-Baker PK, McCormack GR. Neighbourhood built environment influences on physical activity among adults: a systematized review of qualitative evidence. Int J Environ Res Public Health. 2018;15(5):897.
Barnett DW, Barnett A, Nathan A, Van Cauwenberg J, Cerin E, Council on E, et al. Built environmental correlates of older adults' total physical activity and walking: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2017;14(1):103.
Giles-Corti B, Vernez-Moudon A, Reis R, Turrell G, Dannenberg AL, Badland H, et al. City planning and population health: a global challenge. Lancet. 2016;388(10062):2912–24.
Giles-Corti B, Moudon AV, Lowe M, Cerin E, Boeing G, Frumkin H, et al. What next? Expanding our view of city planning and global health, and implementing and monitoring evidence-informed policy. Lancet Glob Health. 2022;10(6):e919–e26.
Okuyama K, Abe T, Yano S, Sundquist K, Nabika T. Neighborhood environment and muscle mass and function among rural older adults: a 3-year longitudinal study. Int J Health Geogr. 2020;19(1):51.
Sun Y, He C, Zhang X, Zhu W. Association of Built Environment with physical activity and physical fitness in men and women living inside the City Wall of Xi'an, China. Int J Environ Res Public Health. 2020;17(14):4940.
Brown SC, Mason CA, Perrino T, Lombard JL, Martinez F, Plater-Zyberk E, et al. Built environment and physical functioning in Hispanic elders: the role of "eyes on the street". Environ Health Perspect. 2008;116(10):1300–7.
McCormack GR, Frehlich L, Blackstaffe A, Turin TC, Doyle-Baker PK. Active and fit communities. Associations between neighborhood walkability and health-related fitness in adults. Int J Environ Res Public Health. 2020;17(4):1131.
Lee JJ, Hwang SJ, Mutalik K, Corey D, Joyce R, Block JP, et al. Association of built environment characteristics with adiposity and glycaemic measures. Obes Sci Pract. 2017;3(3):333–41.
Santos DA, Silva AM, Baptista F, Santos R, Vale S, Mota J, et al. Sedentary behavior and physical activity are independently related to functional fitness in older adults. Exp Gerontol. 2012;47(12):908–12.
Koohsari MJ, Shibata A, Ishii K, Kurosawa S, Yasunaga A, Hanibuchi T, et al. Built environment correlates of objectively-measured sedentary behaviours in densely-populated areas. Health Place. 2020;66:102447.
Nichani V, Turley L, Vena JE, McCormack GR. Associations between neighbourhood built characteristics and sedentary behaviours among Canadian men and women: findings from Alberta's tomorrow project. Prev Med. 2021;150:106663.
Dixon BN, Ugwoaba UA, Brockmann AN, Ross KM. Associations between the built environment and dietary intake, physical activity, and obesity: a scoping review of reviews. Obes Rev. 2021;22(4):e13171.
Hoehner CM, Allen P, Barlow CE, Marx CM, Brownson RC, Schootman M. Understanding the independent and joint associations of the home and workplace built environments on cardiorespiratory fitness and body mass index. Am J Epidemiol. 2013;178(7):1094–105.
Hoehner CM, Handy SL, Yan Y, Blair SN, Berrigan D. Association between neighborhood walkability, cardiorespiratory fitness and body-mass index. Soc Sci Med. 2011;73(12):1707–16.
Shaffer K, Bopp M, Papalia Z, Sims D, Bopp CM. The relationship of living environment with behavioral and fitness outcomes by sex: an exploratory study in college-aged students. Int J Exerc Sci. 2017;10(3):330–9.
Frehlich L, Christie C, Ronksley P, Turin TC, Doyle-Baker P, McCormack G. Association between neighborhood built environment and health-related fitness: a systematic review protocol. JBI Evid Synth. 2021;19(9):2350–8.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Chandrabose M, Rachele JN, Gunn L, Kavanagh A, Owen N, Turrell G, et al. Built environment and cardio-metabolic health: systematic review and meta-analysis of longitudinal studies. Obes Rev. 2019;20(1):41–54.
Leal C, Chaix B. The influence of geographic life environments on cardiometabolic risk factors: a systematic review, a methodological assessment and a research agenda. Obes Rev. 2011;12(3):217–30.
Malambo P, Kengne AP, De Villiers A, Lambert EV, Puoane T. Built environment, selected risk factors and major cardiovascular disease outcomes: a systematic review. PLoS One. 2016;11(11):e0166846.
McCormack GR, Cabaj J, Orpana H, Lukic R, Blackstaffe A, Goopy S, et al. A scoping review on the relations between urban form and health: a focus on Canadian quantitative evidence. Health Promot Chronic Dis Prev Can. 2019;39(5):187–200.
den Braver NR, Lakerveld J, Rutters F, Schoonmade LJ, Brug J, Beulens JWJ. Built environmental characteristics and diabetes: a systematic review and meta-analysis. BMC Med. 2018;16(1):12.
Dendup T, Feng X, Clingan S, Astell-Burt T. Environmental risk factors for developing type 2 diabetes mellitus: a systematic review. Int J Environ Res Public Health. 2018;15(1):78.
Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. Australia: JBI; 2020. Available from https://synthesismanual.jbi.global.
Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp L. Chapter 3: Systematic reviews of effectiveness. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. Australia: JBI; 2020. Available from https://synthesismanual.jbi.global.
Ding D, Gebel K. Built environment, physical activity, and obesity: what have we learned from reviewing the literature? Health Place. 2012;18(1):100–5.
Feng J, Glass TA, Curriero FC, Stewart WF, Schwartz BS. The built environment and obesity: a systematic review of the epidemiologic evidence. Health Place. 2010;16(2):175–90.
Ferdinand AO, Sen B, Rahurkar S, Engler S, Menachemi N. The relationship between built environments and physical activity: a systematic review. Am J Public Health. 2012;102(10):e7–e13.
Bailly L, d'Arripe-Longueville F, Fabre R, Emile M, Valbousquet J, Ferre N, et al. Impact of improved urban environment and coaching on physical condition and quality of life in elderly women: a controlled study. Eur J Pub Health. 2019;29(3):588–93.
Duchowny KA, Glymour MM, Cawthon PM. Is perceived neighbourhood physical disorder associated with muscle strength in middle aged and older men and women? Findings from the US health and retirement study. J Epidemiol Community Health. 2020;74(3):240–7.
Ellaway A, Dundas R, Olsen JR, Shiels PG. Perceived Neighbourhood problems over time and associations with adiposity. Int J Environ Res Public Health. 2018;15(9):1854.
Johnson LG. Physical activity behavior of university students: an ecological approach. US: Louisiana State University and Agricultural & Mechanical College; 2006.
Koohsari MJ, McCormack GR, Nakaya T, Shibata A, Ishii K, Yasunaga A, et al. Walking-friendly built environments and objectively measured physical function in older adults. J Sport Health Sci. 2020;9:651–6.
Leach HJ. The influence of neighborhood environment on risk factors for cardiovascular disease in African American women. US: University of Houston; 2013.
Lee RE, Mama SK, Adamus-Leach HJ. Neighborhood street scale elements, sedentary time and cardiometabolic risk factors in inactive ethnic minority women. PLoS One. 2012;7(12):e51081.
Lewin A, Pannier B, Meline J, Karusisi N, Thomas F, Chaix B. Residential neighborhood, geographic work environment, and work economic sector: associations with body fat measured by bioelectrical impedance in the RECORD study. Ann Epidemiol. 2014;24(3):180–6.
Nascimento CFD, Duarte YAO, Lebrao ML, Chiavegatto Filho ADP. Individual and neighborhood factors associated with functional mobility and falls in elderly residents of Sao Paulo, Brazil: a multilevel analysis. J Aging Health. 2018;30(1):118–39.
Nies MA, Chruscial HL. Neighborhood and physical activity outcomes in women: regional comparisons. Nurs Clin North Am. 2002;37(2):295–301 vii.
Petrella RJ, Kennedy E, Overend TJ. Geographic determinants of healthy lifestyle change in a community-based exercise prescription delivered in family practice. Environ Health Insights. 2008;1:51–62.
Pham DQ, Ommerborn MJ, Hickson DA, Taylor HA, Clark CR. Neighborhood safety and adipose tissue distribution in African Americans: the Jackson heart study. PLoS One. 2014;9(8):e105251.
Rodriguez AX. Perceived environmental correlates of fitness and physical activity in a multi-ethnic sample of college students: University of Houston; 2003.
Sarkar C. Residential greenness and adiposity: findings from the UK biobank. Environ Int. 2017;106:1–10.
Sarkar C, Webster C, Gallacher J. Association between adiposity outcomes and residential density: a full-data, cross-sectional analysis of 419 562 UK biobank adult participants. Lancet Planet Health. 2017;1(7):e277–e88.
Sofkova T, Pridalova M, Mitas J, Pelclova J. The level of neighborhood walkability in a place of residence and its effect on body composition in obese and overweight women. Cent Eur J Public Health. 2013;21(4):184–9.
Soma Y, Tsunoda K, Kitano N, Jindo T, Tsuji T, Saghazadeh M, et al. Relationship between built environment attributes and physical function in Japanese community-dwelling older adults. Geriatr Gerontol Int. 2017;17(3):382–90.
Drewnowski A, Buszkiewicz J, Aggarwal A, Rose C, Gupta S, Bradshaw A. Obesity and the built environment: a reappraisal. Obesity (Silver Spring). 2020;28(1):22–30.
Karmeniemi M, Lankila T, Ikaheimo T, Koivumaa-Honkanen H, Korpelainen R. The built environment as a determinant of physical activity: a systematic review of longitudinal studies and natural experiments. Ann Behav Med. 2018;52(3):239–51.
Pratt J, Hoffman A, Grainger A, Ditroilo M. Forearm electromyographic activity during the deadlift exercise is affected by grip type and sex. J Electromyogr Kinesiol. 2020;53:102428.
McGrath R, Erlandson KM, Vincent BM, Hackney KJ, Herrmann SD, Clark BC. Decreased handgrip strength is associated with impairments in each autonomous living task for aging adults in the United States. J Frailty Aging. 2019;8(3):141–5.
Eckardt N. Lower-extremity resistance training on unstable surfaces improves proxies of muscle strength, power and balance in healthy older adults: a randomised control trial. BMC Geriatr. 2016;16(1):191.
Cadore EL, Rodriguez-Manas L, Sinclair A, Izquierdo M. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: a systematic review. Rejuvenation Res. 2013;16(2):105–14.
Plaut P, Shach-Pinsly D, Schreuer N, Kizony R. The reflection of the fear of falls and risk of falling in walking activity spaces of older adults in various urban environments. J Transp Geogr. 2021;95:103152.
Farkas B, Wagner DJ, Nettel-Aguirre A, Friedenreich C, McCormack GR. Evidence synthesis - a systematized literature review on the associations between neighbourhood built characteristics and walking among Canadian adults. Health Promot Chronic Dis Prev Can. 2019;39(1):1–14.
Hajna S, Ross NA, Brazeau AS, Belisle P, Joseph L, Dasgupta K. Associations between neighbourhood walkability and daily steps in adults: a systematic review and meta-analysis. BMC Public Health. 2015;15:768.
Duncan JJ, Gordon NF, Scott CB. Women walking for health and fitness. How much is enough? JAMA. 1991;266(23):3295–9.
Murphy MH, Nevill AM, Murtagh EM, Holder RL. The effect of walking on fitness, fatness and resting blood pressure: a meta-analysis of randomised, controlled trials. Prev Med. 2007;44(5):377–85.
Cakmak S, Dales R, Leech J, Liu L. The influence of air pollution on cardiovascular and pulmonary function and exercise capacity: Canadian health measures survey (CHMS). Environ Res. 2011;111(8):1309–12.
Kargarfard M, Poursafa P, Rezanejad S, Mousavinasab F. Effects of exercise in polluted air on the aerobic power, serum lactate level and cell blood count of active individuals. Int J Prev Med. 2011;2(3):145–50.
Johns DJ, Hartmann-Boyce J, Jebb SA, Aveyard P. Behavioural weight management review G. diet or exercise interventions vs combined behavioral weight management programs: a systematic review and meta-analysis of direct comparisons. J Acad Nutr Diet. 2014;114(10):1557–68.
Lam TM, Vaartjes I, Grobbee DE, Karssenberg D, Lakerveld J. Associations between the built environment and obesity: an umbrella review. Int J Health Geogr. 2021;20(1):7.
Smith M, Hosking J, Woodward A, Witten K, MacMillan A, Field A, et al. Systematic literature review of built environment effects on physical activity and active transport - an update and new findings on health equity. Int J Behav Nutr Phys Act. 2017;14(1):158.
Drewnowski A, Arterburn D, Zane J, Aggarwal A, Gupta S, Hurvitz PM, et al. The moving to health (M2H) approach to natural experiment research: a paradigm shift for studies on built environment and health. SSM Popul Health. 2019;7:100345.
Baar J, Romppel M, Igel U, Brahler E, Grande G. The independent relations of both residential self-selection and the environment to physical activity. Int J Environ Health Res. 2015;25(3):288–98.
Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public health reports. 1985;100(2):126.
Acknowledgements
Not applicable.
Funding
This work is supported by the Canadian Institutes of Health Research (FDN − 154331). The funders have no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
LF and GRM conceived and designed the study. LF ran the searches. LF screened titles and abstracts. LF and CDC screened full texts. LF and CDC extracted data from included studies. LF drafted the manuscript. LF, CDC, PER, TCT, PD, GRM contributed to interpretation of the data, revisions, and the final manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: S1.
PRISMA checklist. S2. Full search strategies
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Frehlich, L., Christie, C.D., Ronksley, P.E. et al. The neighbourhood built environment and health-related fitness: a narrative systematic review. Int J Behav Nutr Phys Act 19, 124 (2022). https://doi.org/10.1186/s12966-022-01359-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-022-01359-0