
Abstract
Background
Globally, significant efforts have focused on increasing physical activity and reducing sedentary behaviour in youth and adults across a range of settings (e.g., schools, workplaces, community, and home). Despite this, interventions have had varied efficacy and typically have failed to sustain changes in behaviours over time. One explanation that has been put forth to explain the mixed success of interventions is activity compensation. However, little is known about activity compensation, including whether compensation occurs, and perceptions and potential mechanisms of activity compensation. Understanding activity compensation would assist in tailoring and targeting of potential intervention strategies. The primary aim of this review was to synthesise research that has investigated activity compensation in youth and adults. The secondary aim was to identify potential reasons for and/or awareness of compensatory changes that may have occurred.
Methods
An electronic search of the EBSCOhost (via Academic Search Complete, CINAHL Complete, Education Source, Health Source: Nursing/Academic Edition, PsycINFO, SPORTdiscus with Full Text), MEDLINE Complete, Global Health, EMBASE, Scopus and Web of Science databases up to May 2021 was conducted. Quality assessment of included quantitative studies used a modified compensation-specific McMaster Quality Assessment Tool.
Results
A total of 44 studies met the inclusion criteria (22 = adult populations; 22 = youth populations) and were classified as (1) quantitative (n = 31); (2) combination of quantitative and behavioural (n = 11); (3) behavioural only (n = 1); and (4) qualitative (n = 1). Of the 42 studies that included a quantitative component, 11 (26%) reported compensation occurred. Within the 13 studies examining specific behaviours, 35 behaviours were assessed, and evidence of compensation was inconsistent. Compensation mechanisms included fatigue, time constraints, lack of motivation, drive to be inactive, fear of overexertion, and autonomous motivation.
Conclusion
Little evidence of compensation was reported in the included quantitative studies; however, inconsistencies between studies makes comparisons difficult. There was considerable variability in the types of behaviours assessed in quantitative studies, and few studies examined potential compensatory mechanisms. Future research, using compensation specific study designs, methods, and analytic techniques, within different population sub-groups, should address these evidence gaps.
Similar content being viewed by others


Introduction
Regular engagement in physical activity confers physical and mental health benefits in both youth (5–18 years old) and adult populations, including favourable cardiometabolic biomarkers, improved cognition and well-being [1, 2], and among adults, lower risk of all-cause mortality [3, 4]. Conversely, higher levels of sedentary behaviours such as screen time are associated with negative physical and mental health outcomes in youth [5], as well as cardiometabolic diseases, cancer incidence, and depression in adults [6, 7]. Globally, 75% of countries participating in the Active Healthy Kids Global Alliance on physical activity for children and youth (n = 49) reported that over 80% of children did not meet the daily moderate- to vigorous-intensity physical activity (MVPA) guidelines of 60 min per day [8]. Moreover, a pooled analysis of 1.6 million adolescents and of 1.9 million adults found 81% [9] and 28% [10], respectively, failed to meet their specific physical activity guidelines [11]. Significant efforts have focused on increasing physical activity and reducing sedentary behaviour across all age groups and in a range of settings (e.g., schools, work places, community, and home) [12–15], yet interventions have had varied efficacy and have typically failed to sustain changes in behaviours over time [13, 16–18].
One potential explanation for such varied intervention efficacy is activity compensation. It has been hypothesised that activity levels may be under some degree of biological control (an ‘activitystat’), which operates in the same way as the homeostatic mechanisms that regulate body temperature, blood pH, and fluid balance within the body [19]. Specifically, the activitystat hypothesis posits that physical activity levels are kept within tolerable activity levels or energy expenditure ranges (activity set-points), meaning that intensity, frequency, duration and/or load of activity may increase or decrease in response to a perturbation (e.g., an activity intervention) to compensate for the additional (or lack thereof) activity [20]. It is crucial to highlight the importance of such changes occurring in response to a perturbation, as this is what sets compensatory responses apart from habitual activity. In addition, as all activity intensities would contribute to the total activity set-point, the compensatory responses would be expected to occur across the activity spectrum (i.e. sedentary behaviour [SED], light physical activity [LPA], and MVPA) [21]. Upon removal of the perturbation, activity levels are hypothesised to return their original levels [22]. This may explain why interventions have limited efficacy for sustained change in activity levels. Despite this, past behavioural activity research has mostly focused on the impact of social and environmental variables on behaviours, largely neglecting the potential biological basis for activity [19, 23].
In a 2013 review of studies examining activity compensation, Gomersall and colleagues [24] reported that 63% (5/8) of child studies, 40% (6/15) of adult studies and 80% (4/5) of elderly studies indicated compensation had occurred [24]. Whilst Gomersall and colleagues [24] focused on experimental and intervention studies, which enables changes in activity levels to be examined under controlled conditions [24], observational studies that can provide insights into individual day-to-day variability in activity were excluded [25]. Further, though compensation is hypothesised to be a biological response, the way in which any responses are observed or potential reasons for occurring has not been reviewed to date. Specifically, it is unknown what behaviours may change and the potential mechanisms underlying such changes. Consequently, there is a need to synthesise activity compensation evidence with methodological considerations and examine any potential reasons as to why compensation may occur (if at all).
The primary aim of this systematic review was to synthesise research that has investigated activity compensation in youth and adults. The secondary aim was to identify and examine any reasons for and/or awareness of compensatory changes that may have occurred.
Methods
Protocol and registration
The systematic review was registered with PROSPERO (CRD42019133914). The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [26]. The PRISMA Checklist is provided in Supplementary Information 1.
Search strategy
An electronic search of the EBSCOhost (via Academic Search Complete, CINAHL Complete, Education Source, Health Source: Nursing/Academic Edition, PsycINFO, SPORTdiscus with Full Text), MEDLINE Complete, Global Health, EMBASE, Scopus and Web of Science databases up to May 2021 was conducted. The search strategy was developed in conjunction with a research librarian with key words in the following areas: activity compensation ([compensation and physical activity or sedentary or exercise or energy expenditure or energy balance] or [ActivityStat or EnergyStat or energy displacement]) and age ([child or youth or adolescent] or [adult]). The full search strategy, including proximity search strategy functions and truncations, for the different databases can be found in Supplementary Information 2. All titles and abstracts were screened in full and independently by two reviewers (B.S., and S.V. or N.R) using the Cochrane review production platform Covidence (Veritas Health Innovation; Melbourne, Australia). Discrepancies were recorded through Covidence and reviewed by three researchers (B.S., S.V. and N.R.) until a consensus was reached. In the case that a consensus could not be reached, discrepancies were discussed with the research team. Agreement between reviewers in the title/abstract stage was 91%. Full text articles that met the initial screening criteria were then independently screened for eligibility to be included in the review by two researchers (B.S. and S.V.), and inconsistencies were again discussed and resolved with the research team where required. Agreement between reviewers was 72%. The reference lists of studies deemed eligible for inclusion were searched for additional relevant studies for potential inclusion [27].
Eligibility criteria
All original study designs were considered for inclusion. Studies were eligible if they met the following criteria: (a) participant’s mean age was 5–65 years; (b) focused on the general population, i.e., the target population did not solely focus on participants with chronic conditions, athletes, or overweight/obesity (as they may have different compensation ‘drivers’ such as chronic pain, muscular atrophy, etc.); (c) the study explicitly undertook analyses designed to examine activity compensation or compensatory responses, or explored compensatory responses as part of their methods (i.e., study was designed to examine changes in activity across the activity spectrum, or between settings, and used compensation when describing their results); (d) was published in English; and (e) was published between January 1999 to May 2021. The start date was selected to align with the first publication outlining the activitystat hypothesis (1999) [19]. Quantitative studies that, for example, were not designed to look at similarities or differences in activity between settings or time periods, but rather used compensation as a discussion point were not included. Quantitative and qualitative studies were included if they discussed potential mechanisms, reasons, or insights into activity compensation. Articles that were published ahead of print and had a DOI were also eligible for inclusion. Abstracts, conferences, reviews, study protocols, and dissertations were not eligible for inclusion.
Data extraction
For this review, studies were classified into four categories: 1) Quantitative only (i.e. measuring compensation quantitatively); 2) Quantitative and behavioural (i.e. quantitative compensation studies that also recorded behaviours, this included studies measuring mechanisms/perceptions of compensation); 3) Behavioural only (i.e. a non-qualitative assessment of behaviours, perceptions of compensation, or mechanisms); and 4) Qualitative only. This approach was used to distinguish between studies that were eligible for inclusion in this review but examined different aspects of activity compensation. Quantitative data were extracted by one reviewer (B.S). For consistency purposes, 15% of articles were extracted and reviewed by another reviewer (S.V.). Data were extracted using a standardised form and included: study/participant characteristics (e.g. mean age, study design, % male/female, % overweight/obesity, etc.), outcomes examined (e.g. sedentary time), activity assessment method (e.g. pedometer, accelerometer), study design (e.g. cross-sectional), activity compensation methodological considerations (e.g. timeframe examined, analytical approach), reported results (e.g. compensation reported), and behavioural assessments (if any; e.g. sitting time in different locations, active transport, etc.). The authors then reviewed the information extracted and clarified where any differences in information were identified. Support was provided via discussion with the remaining authors if clarifications were required (e.g., what analytical approaches were used). The remaining data were re-checked and verified by one reviewer (B.S.). Qualitative data were extracted by one reviewer using thematic synthesis (B.S.) [28].
Quality assessment
A quality assessment tool, derived from the McMaster Quality Assessment Tool [29] and compensation specific criteria as defined by Rowlands [30], was developed by the research team. The tool was used to assess the included quantitative studies only (categories 1, 2, and 3). Nine compensation specific criteria were developed [30] and included: study design (i.e. experimental design as the ‘gold standard’), implementing activity during inactive times and/or restricting activity during inactive times (i.e. when perturbation occurred), measuring activity across settings, sensitivity of measurement tools, analytical approach (e.g. within-group), and assessed the whole activity spectrum (i.e. SED to MVPA) [21]. In total, 16 criteria, including general and compensation-specific items, were used to assess quality across six overarching categories of (a) selection bias (e.g. is the sample representative); (b) study design; (c) data collection (e.g. is the measurement tool objective, valid and reliable); (d) withdrawals and dropouts (e.g. % of dropouts reported); (e) exposure integrity (e.g. % of participants receiving allocated exposure/intervention); and (f) analyses (e.g. within/between-person analyses). The compensation specific criteria were included across all categories except the withdrawals/dropouts. For category 1, 2, and 3 studies, a quality rating of strong, moderate, or weak was given to each component, except for dichotomous variables that were rated strong or weak. In the event a component could not be clearly determined from the paper, a weak rating was given. No overall study quality score was given in line with current recommendations [31]. Category 4 papers were assessed using the McMaster Qualitative Review Form [32]. The category 4 paper was not given a rating according to the review form guidelines [32]. The full quality assessment tools can be found in the Supplementary Information 3 and 4.
Results
Description of included studies
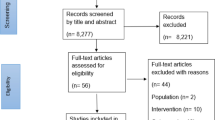
Extracted data were analysed between May 2021–July 2021. Of the studies initially identified, 109 full-text studies were screened, and 44 studies were included in the review. Of these, 31 were classified as quantitative only (category 1) [20, 21, 33–61], 11 assessed quantitative outcomes but included subjective behavioural components (category 2) [62–72], one examined self-reported behaviours only (category 3) [73], and one qualitative study examined mechanisms and perceptions of compensation (category 4) [74]. The PRISMA flowchart can be found in Fig. 1.

PRISMA Flow Diagram. 2020 PRISMA flow diagram [26] of studies assessed for eligibility and included in review
The characteristics of the included studies are found in Table 1. Studies were conducted in 10 different countries (see Table 1), with the majority occurring in the USA (n = 13), the UK (n = 13) and Australia (n = 9). The age of participants ranged between 5 [72] to 63 [67] years, with 50% studies specifically focusing on children and/or adolescents (n = 22; [20, 21, 33, 36, 39, 41–44, 47–52, 55, 58, 63–65, 71, 72]) and 50% focusing on adults (n = 22; [34, 35, 37, 38, 40, 45, 46, 53, 54, 56, 57, 59–62, 66–70, 73, 74]). Study sample sizes ranged from 16 participants [35, 45] to 12,969 [69] participants. Of the 44 studies included, the primary or secondary aim of 30 [20, 21, 33, 35–39, 41–44, 48, 50–56, 59, 64, 66, 68–74] and eight studies [34, 38, 40, 47, 57, 58, 62, 63], respectively, was to examine activity compensation. The remaining six were ‘unspecified’ (e.g., results included compensation analyses but this was not a specified aim) [45, 46, 49, 60, 61, 67]. Studies were primarily cross-sectional (52%), followed by experimental (randomised crossover n = 7; randomised experiment n = 2; pre-post n = 1; two-phase single case n = 1) (25%), and randomised controlled trials or intervention studies (18%). There was one longitudinal [69] and one qualitative study [74] included in the review.
Quantitative study overview (categories 1 & 2)
Of the 31 quantitative studies and 11 quantitative/behavioural studies, 11 studies reported evidence of compensation [21, 37, 46, 50, 52, 56, 57, 64, 69, 71, 72], 29 studies reported no evidence of compensation [20, 34–36, 38–45, 47–49, 51, 53–55, 58–63, 65, 66, 68, 70] and two studies had mixed [33] or unclear results [67] (see Table 2).
Evidence of compensation
Of the 11 studies reporting evidence of compensation, six were in youth [21, 50, 52, 64, 71, 72] and five were in adult [37, 46, 56, 57, 69] populations. The time frame of compensation included within-day (n = 4; [33, 52, 56, 71]) to between-day (n = 5; [21, 50, 52, 57, 72]), to between-weeks (e.g. baseline to end of intervention) (n = 2; [37, 46]) to between-seasons [64]. All studies used accelerometers, except for one longitudinal study in adults, which assessed compensation within-day at two timepoints (4 years apart) and used the Physical Activity Questionnaire (PAQ) [69]. Outcome variables included energy expenditure [37], steps [57], counts per minute [64] and counts per day [46], LPA [71] and MVPA [64, 71] (Table 2). Only two studies, both conducted with youth, examined compensatory changes across the full waking activity spectrum (SED, LPA, MVPA) [21, 50]. Six studies used a within-person design [21, 33, 37, 50, 52, 71], whilst three studies used between group analyses [64, 69, 72]. Three studies used both within-person and between-person or between- group analyses [46, 56, 57]. One study (adolescent population) [33], reported that compensation only occurred ‘between locations’ (Table 2).
No evidence of compensation
Of the 29 studies reporting no evidence of compensation, 15 were conducted in youth populations [20, 36, 39, 41–44, 47–49, 51, 55, 58, 63, 65] whilst 14 were conducted in adult populations [34, 35, 38, 40, 45, 53, 54, 59–62, 66, 68, 70]. The time frame examined varied from within-day (n = 9; [34, 36, 39, 41, 44, 58, 62, 63, 66]) and (n = 6; [20, 40, 48, 51, 53, 54])/or between-day (n = 5; [42, 47, 49, 59, 65]) to between-weeks (e.g. pre, mid, and post intervention (n = 3; [38, 43, 70]). The majority (90%) of studies used device-based measures of activity, primarily accelerometers (n = 23; [20, 34–36, 38–45, 48, 49, 51, 53–55, 59, 60, 63, 65, 70]) and pedometers (n = 3; [47, 58, 62]). Two studies subjectively measured adults’ physical activity using surveys [67, 68]. Five studies (three in youth, two in adults) examined the whole activity spectrum [34, 35, 42, 51, 55]. One study, conducted with adolescents, examined the activity spectrum where LPA was classified as non-exercise activity thermogenesis (NEAT) [44]. Five studies examined changes in MVPA [58, 65], moderate-intensity physical activity (MPA), and/or vigorous-intensity physical activity (VPA) only [40, 41, 63], while another assessed both MVPA and energy expenditure [38]. Other outcome variables included energy expenditure (e.g. activity energy expenditure) [43, 45, 48] and time use variables (e.g. sitting time) [59, 61, 62, 66]. The analytical approach for studies that reported no evidence of compensation included 11 within-person analyses [20, 36, 41, 42, 48, 49, 51, 58, 61, 63, 68] and 12 between-group analyses [38, 39, 43, 45, 47, 53–55, 59, 60, 62, 66], whilst six used both analytical approaches [34, 35, 40, 44, 65, 70]. One study with mixed results (adolescent population) [33], reported that no compensation occurred in the location-based MVPA or overall MVPA component of their data (see Table 2).
Behavioural studies (categories 2, 3 & 4)
Thirteen studies measured specific behaviours [62, 64–72], perceptions of compensation [63, 74], and/or mechanisms of compensation [73, 74] (see Table 3). Five studies were conducted with youth populations [63–65, 71, 72] and eight with adults [62, 66–70, 73, 74]. Ten quantitative studies contained a behavioural component recorded via a survey [63, 65–69, 71, 73] or activity diary [62, 64]. Two studies examined perceptions of compensation [63, 74], and two assessed potential mechanisms of compensation [73, 74].
Behaviours
The numbers of behaviours assessed ranged from 1 [64]-26 [65] and included passive and active travel [62, 66–68, 72], out-of-school activities [64, 65], leisure-time or personal activities [62, 64–67, 69, 70], occupational activity [62, 66, 67, 69], recreational walking [68], and screen time [70–72]. Behaviours were typically assessed using activity diaries and surveys, though one study combined a survey that was cross-checked with MVPA data collected using an accelerometer in settings [65] (see Table 3). In one study, it was unclear how behaviours were measured [72].
Of the 10 quantitative studies that included a behavioural component, four reported evidence of compensation [64, 69, 71, 72]. However, in three of these studies it was not clear whether compensation occurred in specific behaviours (i.e. data only reported the quantitative activity measures) [64, 71, 72]. In the remaining study, Nooijen and colleagues reported that adults who moved to a higher activity occupation compensated by decreasing their leisure-time exercise [69]. No evidence of compensation was reported in six studies (one in youth and five in adults) [62, 65–68, 70]. Based on time-use assessment, Jans et al. reported that those who had highly sedentary occupations did not compensate by decreasing leisure-time sedentary behaviour [66]. Further, Goodman et al. reported that there was no evidence of compensation in children aged 8–13 in any of the 26 MVPA behaviours assessed (e.g. MVPA in school lessons, P.E./games, active travel, etc. [65]) (see Table 3).
Mechanisms of compensation
Two studies examined potential mechanisms of compensation [73, 74]. In a sample of purposely selected participants who were identified as compensating their non-exercise physical activity during a 4-week structured activity intervention, reasons for activity compensation included fatigue, time constraints, lack of motivation, drive to be inactive (i.e. more activity means you can do less activity later), and fear of overexertion [74]. The second study, which examined the association between physical inactivity and compensatory health behaviours in young adults, reported that young adults with strong autonomous motivation believed that they could compensate their sedentary time by using the stairs later [73].
Perceptions of compensation
Two studies examined perceptions of compensation. Costigan and colleagues reported that compensation had not occurred when assessed using accelerometers, yet 13% of participants self-reported that their participation in the high intensity interval training (HIIT) sessions had made them less active during school breaks, and 19.4% thought they were less active after school [63]. In a qualitative study, Gray and colleagues reported that 56% of participants were unaware that they had compensated their activity [74].
Quality assessment
The quality assessment for each study is shown in Table 4. The majority of studies (80%; n = 35) used device-based assessments, of which 24 studies included devices that were considered valid and reliable (54%). Examining activity across settings was evident in 72% of studies (n = 32). However, 86% of studies did not include an exposure (e.g. perturbation) as part of their design or did not deliver > 60% [29] of the exposure as intended (n = 13). Only two studies restricted activity during a time that would normally be active [36, 51], with one imposing activity during a time where children are normally inactive (i.e. timing of perturbation) [51]. Only 9 (20%) studies examined compensation across the activity spectrum [20, 21, 34, 35, 42, 45, 50, 51, 55].
Discussion
This systematic review aimed to synthesise research that has investigated activity compensation in youth and adults and identify reasons for and/or awareness of compensatory changes that may have occurred. In general, this review did not find clear evidence that activity compensation occurs in either youth or adults. This may be due to the diverse approaches used to assess activity compensation, including different timeframes and study designs. However, 91% of the studies that reported evidence of compensation (n = 11), included assessing compensation as a primary (n = 9) or secondary (n = 1) aim, suggesting that purpose-designed studies are required to examine compensatory responses. Few studies examined perceptions and mechanisms of compensation, however; the results also suggested that while compensatory changes may occur, there was a lack of awareness of such responses in youth and adults.
This review builds on a previous review [24] through the inclusion of observational, experimental and intervention study designs. Interestingly, regardless of the study design utilised, no clear evidence of compensatory responses were observed, similar to a previous review, where mixed evidence of compensation was reported in children and adults [24]. It is worth noting that whilst 29 studies reported no evidence of compensation, 21% (n = 6) [35, 43, 53–55, 59] included a dietary compensation component, of which 67% (n = 4) [35, 53, 54, 59] reported some level of dietary compensation. As such, it could be that compensatory responses occur through the energy intake rather than energy expenditure. Further research is needed to examine the potential relationship between dietary and activity compensation. Another potential reason for the inconsistent results could be due to the way that compensatory changes were analysed. A range of analytical approaches were used by included studies to examine whether compensation occurs, including within-person and/or between person/group analyses. At least one-quarter of the observational studies [39, 47, 53, 54, 59, 62, 64, 66, 69, 72], interventions [38, 43, 60] and experimental studies [45, 55] only utilised between-person/group analyses, despite the activitystat hypothesis being a within-person hypothesis [19]. As such, this may impact the interpretation of findings. Studies should consider a within-person rather than between-group analytic approach to assess activity compensation given this is an individual response [19, 30]. Interestingly, of the studies that used between-group analyses, 25% reported evidence of compensation, whilst 35% of studies using within-person analyses reported evidence of compensation, indicating that when a purpose-driven methodological design is utilised, higher evidence of compensation is reported.
The time frame within which compensation would be expected to occur has been debated, with some suggesting that compensation would be unlikely to occur within-days [24], whilst others reporting that within-day compensatory changes were observed [52]. In this review, there was no clear evidence of a compensation time frame. Some studies reported evidence of compensation within [71] and/or between-days [52, 57], whilst others reported that compensation was evident over a longer period of time, such as between-seasons [37, 64, 69]. In contrast, some studies found no compensation within-day [36] and/or between-days [20, 42] or over longer periods of time [38, 43]. For intervention and experimental studies, when analysing two time points for compensation the days should be ‘comparable’ (i.e. structured similarly) to determine whether the changes observed may be attributed to compensatory responses [75] or variations driven by other factors (e.g. timetabling). However, few included studies reported considering the temporal nature of activity data in this way, and of those that did, only short time frames (e.g. < 24 h) were examined [51]. A previous review [24] suggested that compensation duration was synonymous with intervention duration, ranging from within-day to 4 years. However, it is unclear whether this reflects maintenance or changes in activity behaviours rather than compensation, as from a biological perspective, homeostatic processes could be expected to occur acutely. Future research assessing the time frame of compensation should initially examine acute responses before assessing changes over longer time periods.
The study design and compensation timeframe period are important when considering the perturbation of activity. Whilst a few studies examined the effect of a stimulus on participants’ activity [49, 55], the dose was not always reported. Few studies reported whether the stimulus occurred during a time when children were already active (e.g. during recess), making it difficult to determine whether the stimulus is eliciting a compensatory response or displacing usual activity [22, 30]. Only two studies restricted activity during normally active times (e.g. recess) [36, 51], despite compensatory responses being hypothesised to occur under such conditions [30]. A third study, which imposed sedentary time on children for an 8-h period, will have imposed inactivity on active periods of a child’s day. However, the amount of usual activity that was restricted during the imposed 8-h sedentary time period was not reported [55]. Lastly, 55% of the included quantitative studies were observational. Whilst observational studies may provide insights into intra-individual variability, the type and dose of perturbation were not described. As such, it is difficult to determine whether the dose of imposed activity and/or inactivity was outside the normal day-to-day variability (i.e. habitual activity patterns), to illicit a compensatory response [30]. In addition, it limits conclusions that any behaviour compensation was purely a biological response, or conversely a response influenced by the environments in which a person lives (e.g. structure of the day) [72]. Overall, future research should aim to report intra-individual variability to determine whether the perturbation exceeds such variability [76], and report the duration and activity intensity of the perturbation during the day.
Few studies (26%) considered changes in activity across the whole activity spectrum [20, 21, 34, 35, 42, 44, 45, 50, 51, 55, 67], despite the co-dependency of activity intensities occurring within a finite period (e.g. 24 h) [77]. The main activity intensity examined in both youth and adult populations was MVPA, which enables the assessment of changes in this intensity only. Arguably, responses to perturbation across activity intensities would be expected to occur across the whole activity spectrum, as all intensities would contribute to a daily set-point [21]. Given MVPA only constitutes 5% of a child’s waking hours [5] and 3% of an adult’s total day [78], if compensation were to occur, it is very likely to occur in lower intensities of the activity spectrum (LPA and SED) and not just in the intensity measured. Furthermore, it is possible that the findings generalised to other/daily behaviours, nor other population sub-groups. For example, some studies examined specific population groups (e.g. army cadets [40], office workers [66]), and outcomes reported were specific to those target groups (e.g. impact on MVPA, sitting time, etc.). Such findings are therefore specific to that population group and behaviour/intensity. Future studies should focus on assessment of compensation across the entire activity spectrum, and use statistical analyses that appropriately deal with co-dependency between these behaviours, such as compositional data analysis [77], to explore whether compensations may occur across the activity spectrum rather than within a single intensity. Further, future studies could consider sub-group analyses to see how compensation may occur across population groups.
Given the mixed findings and variability in methods and approaches it is difficult to draw conclusions concerning the existence of an activitystat and whether compensation occurs. While the one study [51] that scored ‘moderate’ or ‘strong’ across all compensation specific criteria of the quality assessment reported that compensation had occurred, this study was limited as participants did not participate in all three experimental conditions (imposed moderate- to vigorous physical activity, imposed light physical activity, and restricted physical activity) that is arguably needed to fully test the activitystat hypothesis. As some findings did report compensatory changes, this indicated that such responses do need to be considered in intervention designs moving forward. While compensation may not necessarily be harmful, it may depend on the response to a perturbation. Past literature has suggested that a new equilibrium around activity would indicate that individuals were able to modulate physical activity upwards and subsequently adjust the setpoint for physical activity [22, 72]. However, the issue therein, is that once a perturbation has been removed, there is little evidence to suggest that the modulated physical activity continues at that higher level [22]. These questions are important, yet complex to answer, without a clear understanding of whether compensation occurs (or not). As such, experimental studies are needed to determine what the impact of compensation is on health and whether different types of compensation have different health effects.
This systematic review was the first to examine mechanisms of or potential reasons for compensatory responses. Understanding how compensation may manifest behaviourally may enable researchers to specifically target behaviours at risk of compensatory changes. Ten studies examined potential compensatory changes in ~ 35 behaviours, yet few behaviours were consistently studied or clearly included in the compensatory analysis. Indeed, studies used different methods, such as temporal associations [65] and time use [66, 67], and MVPA in-school/out-of-school [65] and in different locations [64]. The one study that focused on a specific behaviour reported that adults who moved to a higher activity occupation compensated by decreasing their leisure-time exercise [69]. However, while two within-day measurements were analysed, the measurement time points were 4 years apart, making it difficult to understand whether this is truly a compensatory response, or if other factors (e.g., the environment) may also explain the results [69]. Overall, it is challenging to understand whether compensatory changes to behaviours occur, and if they do occur, how these may manifest between (e.g., walking to school, then public transportation home) or within behaviours (e.g., less active during a sports session). Future research should consider the use of purpose-designed surveys to examine time-use in different behaviours across settings, in conjunction with device-based assessments measurements.
Few studies examined potential mechanisms or reasons for compensatory behaviours. Fatigue, time constraints, lack of motivation, drive to be inactive, fear of overexertion, and perceived effort were identified as potential reasons or mechanisms of compensation in older adults [74]. Similarly, perceived effort to compensate combined with a drive to be inactive seemed prevalent in a study in young adults who reported that SED time could be compensated by a healthy behaviour such as taking the stairs [73]. To date, no studies have examined potential mechanisms (e.g., behavioural, psychological, or physiological mechanisms) of compensation in children. Despite this, results indicate that compensation may manifest in different ways within different population groups. Whilst qualitative research, for example, cannot determine whether compensatory changes occurred, it provides unique insights into potential mechanisms that could then be targeted by future interventions that aim to minimise such responses.
Lastly, few studies examined perceptions or awareness of any potential compensatory responses. In the qualitative study by Gray et al. [74], over half (56%) of participants (older adults) were unaware that they had compensated. Only one study measured self-reported perceived compensation [63]. Whilst most adolescent participants did not believe they compensated their activity because of the HIIT sessions, some thought they did compensate during (13%) or after school (19%) [63]. However, no further analyses were performed to see if their subjective experience matched the objective measurements or what traits, if any, these participants shared. It is unknown whether those that thought they compensated their activity actually did so, though it appears that, to some degree, people are aware that compensation may occur after activity. Future research should assess perceptions of activity compensation and examine differences across age groups (for example) and behaviour intensities. Understanding individual awareness of compensation, and any potential reasons for it, may identify why past activity interventions have had limited effectiveness, and inform the development of targeted interventions in the future.
Strengths and limitations
This systematic review was the first to consider potential reasons for any compensatory changes observed. This review included all study designs, as well as behavioural studies, and was able to highlight a number of gaps in activitystat/activity compensation research. However, a few limitations must be acknowledged. Whilst the inclusion criteria were broad to reflect the way in which compensation has been examined to date, it was difficult to compare studies given the diverse range of approaches used and lack of standardised approaches (e.g., different statistical methods [within/between subjects], study designs [experimental, observational], etc.). This review aimed to synthesise all available activity compensation research; however, it was unable to draw firm conclusions as to the existence of activity compensation, and how it may manifest, given the variability in the methodology of studies that have examined this research area.
Conclusion
Overall, this review found that compensation was observed in approximately one-third (32%) of youth and one-quarter (23%) of adult studies that utilised quantitative methods to examine the activitystat hypothesis. There was some evidence of compensation reported in studies where behaviours were assessed. However, there was substantial variability in study designs, time frames assessed, analytical approaches used, and behaviours examined in both the youth and adult studies, making it difficult to draw firm conclusions to the existence of the activitystat. Future research should consider focusing on experimental designs (with the type, timing and dose of perturbation reported), examining the whole activity spectrum, utilising a within-person analysis design across short and acute timeframes to assess whether compensation responses have occurred. Additionally, potential mechanisms of compensatory changes, and whether participants are aware of their compensation, should be assessed. This would provide valuable insights into what behaviours may be targeted in future interventions to negate compensatory changes.
Abbreviations
- MVPA:
-
Moderate- to vigorous-intensity physical activity
- SED:
-
Sedentary behaviour
- LPA:
-
Light physical activity
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PAQ:
-
Physical Activity Questionnaire
- NEAT:
-
Non-exercise activity thermogenesis
- MPA:
-
Moderate-intensity physical activity
- VPA:
-
Vigorous-intensity physical activity
- HIIT:
-
High intensity interval training
References
Donnelly JE, Hillman CH, Castelli D, Etnier JL, Lee S, Tomporowski P, et al. Physical activity, fitness, cognitive function, and academic achievement in children: a systematic review. Med Sci Sports Exerc. 2016;48(6):1197–222.
Poitras VJ, Gray CE, Borghese MM, Carson V, Chaput J-P, Janssen I, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41(6 (Suppl. 3)):S197–239.
Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–29.
U.S. Department of Health and Human Services. Physical activity guidelines for Americans. Washington, D.C.: US; 2018.
Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput JP, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. 2016;41(6):S240–S65.
Biswas A, Oh PI, Faulkner GE, Bajaj RR, Silver MA, Mitchell MS, et al. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults. Ann Intern Med. 2015;162(2):123–32.
Saunders TJ, McIsaac T, Douillette K, Gaulton N, Hunter S, Rhodes RE, et al. Sedentary behaviour and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S197–217.
Aubert S, Barnes JD, Abdeta C, Abi Nader P, Adeniyi AF, Aguilar-Farias N, et al. Global matrix 3.0 physical activity report card grades for children and youth: results and analysis from 49 countries. J Phys Act Health. 2018;15(Supplement 2):S251–S73.
Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. 2020;4(1):23–35.
Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 2018;6(10):e1077–e86.
World Health Organization. Global recommendations on physical activity for health. 2010.
Biddle SJ, Petrolini I, Pearson N. Interventions designed to reduce sedentary behaviours in young people: a review of reviews. Br J Sports Med. 2014;48(3):182–6.
Metcalf B, Henley W, Wilkin T. Effectiveness of intervention on physical activity of children: systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54). BMJ. 2012;345(e5888):1-11.
Murray JM, Brennan SF, French DP, Patterson CC, Kee F, Hunter RF. Effectiveness of physical activity interventions in achieving behaviour change maintenance in young and middle aged adults: a systematic review and meta-analysis. Soc Sci Med. 2017;192:125–33.
Owen N, Healy GN, Dempsey PC, Salmon J, Timperio A, Clark BK, et al. Sedentary behavior and public health: integrating the evidence and identifying potential solutions. Annu Rev Public Health. 2020;41(1):265–87.
Sallis JF, Bull F, Guthold R, Heath GW, Inoue S, Kelly P, et al. Progress in physical activity over the Olympic quadrennium. Lancet. 2016;388(10051):1325–36.
Altenburg TM, Kist-Van Holthe J, Chinapaw MJM. Effectiveness of intervention strategies exclusively targeting reductions in children’s sedentary time: a systematic review of the literature. Int J Behav Nutr Phys Act. 2016;13(1):1–8.
Van Sluijs EM, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ. 2007;335(7622):703.
Rowland TW. The biological basis of physical activity. Med Sci Sports Exerc. 1998;30(3):392–9.
Baggett CD, Stevens J, Catellier DJ, Evenson KR, McMurray RG, He K, et al. Compensation or displacement of physical activity in middle-school girls: the trial of activity for adolescent girls. Int J Obes. 2010;34(7):1193–9.
Ridgers ND, Timperio A, Cerin E, Salmon JO. Compensation of physical activity and sedentary time in primary school children. Med Sci Sports Exerc. 2014;46(8):1564–9.
Wilkin T. Can we modulate physical activity in children? No. Int J Obes. 2011;35(10):1270.
Eisenmann JC, Wickel EE. The biological basis of physical activity in children: revisited. Pediatr Exerc Sci. 2009;21(3):257–72.
Gomersall SR, Rowlands AV, English C, Maher C, Olds TS. The activitystat hypothesis: the concept, the evidence and the methodologies. Sports Med. 2013;43:135–49.
Rowlands AV, Gomersall SR, Tudor-Locke C, Bassett DR, Kang M, Fraysse F, et al. Introducing novel approaches for examining the variability of individuals’ physical activity. J Sports Sci. 2015;33(5):457–66.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Horsley T, Dingwall O, Sampson M. Checking reference lists to find additional studies for systematic reviews. Cochrane Database Syst Rev. 2011;2011(8):MR000026.
Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45.
National Collaborating Centre for Methods and Tools. Quality assessment tool for quantitative studies. Hamilton: McMaster University; 2008.
Rowlands AV. Methodological approaches for investigating the biological basis for physical activity in children. Pediatr Exerc Sci. 2009;21(3):273–8.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. Hoboken: John Wiley & Sons; 2019.
Letts L, Wilkins S, Law M, Stewart D, Bosch J, Westmorland M. Critical review form–qualitative studies (version 2.0): McMaster University; 2007.
Carlson JA, Mitchell TB, Saelens BE, Staggs VS, Kerr J, Frank LD, et al. Within-person associations of young adolescents’ physical activity across five primary locations: is there evidence of cross-location compensation? Int J Behav Nutr Phys Act. 2017;14:1–9.
Clemes SA, O'Connell SE, Edwardson CL. Office workers’ objectively measured sedentary behavior and physical activity during and outside working hours. Int J Occup Med Environ Health. 2014b;56(3):298–303.
Cull BJ, Haub MD, Rosenkranz RR, Lawler T, Rosenkranz SK. The seated inactivity trial (SIT): physical activity and dietary outcomes associated with 8 weeks of imposed sedentary time. J Phys Act Health. 2016;13(3):249–56.
Dale D, Corbin CB, Dale KS. Restricting opportunities to be active during school time: do children compensate by increasing physical activity levels after school? Res Q Exerc Sport. 2000;71(3):240–8.
Di Blasio A, Ripari P, Bucci I, Di Donato F, Izzicupo P, D'Angelo E, et al. Walking training in postmenopause: effects on both spontaneous physical activity and training-induced body adaptations. Menopause. 2012;19(1):23–32.
Gomersall SR, Maher C, English C, Rowlands AV, Dollman J, Norton K, et al. Testing the activitystat hypothesis: a randomised controlled trial. BMC Public Health. 2016;16(1):1–14.
Jakubec L, Frömel K, Chmelík F, Groffik D. Physical activity in 15–17-year-old adolescents as compensation for sedentary behavior in school. Int J Environ Res Public Health. 2020;17(9):3281.
Liguori G, Schuna JM Jr, Tucker J, Fountaine CM. Impact of prescribed exercise on physical activity compensation in young adults. J Strength Cond Res. 2017;31(2):503–8.
Long MW, Sobol AM, Cradock AL, Subramanian SV, Blendon RJ, Gortmaker SL. School-day and overall physical activity among youth. Am J Prev Med. 2013;45(2):150–7.
Mackintosh KA, Ridgers ND, McNarry MA. Compensatory changes in physical activity and sedentary time in children and adolescents with cystic fibrosis. J Sports Sci. 2019;37(13):1–6.
Massie R, Smallcombe J, Tolfrey K. Effects of a 12-week exercise intervention on subsequent compensatory behaviors in adolescent girls: an exploratory study. Pediatr Exerc Sci. 2019;1(aop):1–10.
Matthews-Ewald MR, Kelley GA, Gurka M, Frost SS, Moore LC, Harris CV, et al. Looking within the school day: does activity compensation occur with light physical activity? Int J Child Adolesc Health. 2014;7(1):45–52.
McLaughlin R, Malkova D, Nimmo MA. Spontaneous activity responses to exercise in males and females. Eur J Clin Nutr. 2006;60(9):1055–61.
Meijer EP, Westerterp KR, Verstappen FTJ. Effect of exercise training on total daily physical activity in elderly humans. Eur J Appl Physiol Occup Physiol. 1999;80(1):16–21.
Morgan CF, Beighie A, Pangrazi RP. What are the contributory and compensatory relationships between physical education and physical activity in children? Res Q Exerc Sport. 2007;78(5):407.
O'Sullivan MP, Nagy MR, Block SS, Tooley TR, Robinson LE, Colabianchi N, et al. Acute compensatory responses to interrupting prolonged sitting with intermittent activity in preadolescent children. Pediatr Exerc Sci. 2018;30(2):259–65.
Penning A, Okely AD, Trost SG, Salmon J, Cliff DP, Batterham M, et al. Acute effects of reducing sitting time in adolescents: a randomized cross-over study. BMC Public Health. 2017;17:1–11.
Ridgers ND, Barnett LM, Lubans DR, Timperio A, Cerin E, Salmon J. Potential moderators of day-to-day variability in children's physical activity patterns. J Sports Sci. 2018a;36(6):637–44.
Ridgers ND, Lamb KE, Timperio A, Brown H, Salmon J. Investigating children’s short-term responses to imposed or restricted physical activity. J Phys Act Health. 2018b;15(4):239–46.
Ridgers ND, Timperio A, Cerin E, Salmon J. Within- and between-day associations between children’s sitting and physical activity time. BMC Public Health. 2015;15(1):1–7.
Rocha J, Paxman J, Dalton C, Winter E, Broom D. Effects of an acute bout of aerobic exercise on immediate and subsequent three-day food intake and energy expenditure in active and inactive men. Appetite. 2013;71:369–78.
Rocha J, Paxman J, Dalton C, Winter E, Broom D. Effects of an acute bout of aerobic exercise on immediate and subsequent three-day food intake and energy expenditure in active and inactive pre-menopausal women taking oral contraceptives. Appetite. 2015;89:183–91.
Saunders TJ, Chaput JP, Goldfield GS, Colley RC, Kenny GP, Doucet E, et al. Children and youth do not compensate for an imposed bout of prolonged sitting by reducing subsequent food intake or increasing physical activity levels: a randomised cross-over study. Br J Nutr. 2014;111(4):747–54.
Schubert MM, Palumbo E, Seay RF, Spain KK, Clarke HE. Energy compensation after sprint- and high-intensity interval training. PLoS One. 2017;12(12):e0189590.
Schutz Y, Nguyen DMT, Byrne NM, Hills AP. Effectiveness of three different walking prescription durations on total physical activity in normal- and overweight women. Obes Facts. 2014;7(4):264–73.
Stylianou M, van der Mars H, Kulinna PH, Adams MA, Mahar M, Amazeen E. Before-school running/walking club and student physical activity levels: an efficacy study. Res Q Exerc Sport. 2016;87(4):342–53.
Tigbe WW, Lean ME, Granat MH. A physically active occupation does not result in compensatory inactivity during out-of-work hours. Prev Med. 2011;53(1/2):48–52.
Turner JE, Markovitch D, Betts JA, Thompson D. Nonprescribed physical activity energy expenditure is maintained with structured exercise and implicates a compensatory increase in energy intake. Am J Clin Nutr. 2010;92(5):1009–16.
Vandelanotte C, Duncan MJ, Short C, Rockloff M, Ronan K, Happell B, et al. Associations between occupational indicators and total, work-based and leisure-time sitting: a cross-sectional study. BMC Public Health. 2013;13:1110.
Clemes SA, Patel R, Mahon C, Griffiths PL. Sitting time and step counts in office workers. Occup Med. 2014a;64(3):188–92.
Costigan SA, Ridgers ND, Eather N, Plotnikoff RC, Harris N, Lubans DR. Exploring the impact of high intensity interval training on adolescents’ objectively measured physical activity: findings from a randomized controlled trial. J Sports Sci. 2018;36(10):1087–94.
Fremeaux AE, Mallam KM, Metcalf BS, Hosking J, Voss LD, Wilkin TJ. The impact of school-time activity on total physical activity: the activitystat hypothesis (EarlyBird 46). Int J Obes. 2011;35(10):1277–83.
Goodman A, Mackett RL, Paskins J. Activity compensation and activity synergy in British 8-13 year olds. Prev Med. 2011;53(4/5):293–8.
Jans MP, Proper KI, Hildebrandt VH. Sedentary behavior in Dutch workers: differences between occupations and business sectors. Am J Prev Med. 2007;33(6):450–4.
Matthews CE, Keadle SK, Saint-Maurice PF, Moore SC, Willis EA, Sampson JN, et al. Use of time and energy on exercise, prolonged TV viewing, and work days. Am J Prev Med. 2018;55(3):e61–e9.
McCormack G, Giles-Corti B. Does participation in recommended levels of vigorous-intensity physical activity decrease participation in moderate-intensity physical activity? J Phys Act Health. 2004;1(1):45–55.
Nooijen CFJ, Del Pozo-Cruz B, Nyberg G, Sanders T, Galanti MR, Forsell Y. Are changes in occupational physical activity level compensated by changes in exercise behavior? Eur J Pub Health. 2018;28(5):940–3.
Siddique J, de Chavez PJ, Craft LL, Freedson P, Spring B. The effect of changes in physical ativity on sedentary behavior: results from a randomized lifestyle intervention trial. Am J Health Promot. 2017;31(4):287–95.
Tanaka C, Tanaka M, Okuda M, Inoue S, Aoyama T, Tanaka S. Association between objectively evaluated physical activity and sedentary behavior and screen time in primary school children. BMC Res Notes. 2017;10:1–8.
Wilkin TJ, Mallam KM, Metcalf BS, Jeffery AN, Voss LD. Variation in physical activity lies with the child, not his environment: evidence for an ‘activitystat’ in young children (EarlyBird 16). Int J Obes. 2006;30(7):1050–5.
Radtke T, Rackow P. Autonomous motivation is not enough: the role of compensatory health beliefs for the readiness to change stair and elevator use. Int J Environ Res Public Health. 2014;11(12):12412–28.
Gray P, Murphy M, Gallagher A, Simpson EEA. A qualitative investigation of physical activity compensation among older adults. Br J Health Psychol. 2018;23(1):208–24.
Beets MW, Okely A, Weaver RG, Webster C, Lubans D, Brusseau T, et al. The theory of expanded, extended, and enhanced opportunities for youth physical activity promotion. Int J Behav Nutr Phys Act. 2016;13(1):1–5.
Rowlands AV, Pilgrim EL, Eston RG. Seasonal changes in children's physical activity: an examination of group changes, intra-individual variability and consistency in activity pattern across season. Ann Hum Biol. 2009;36(4):363–78.
Dumuid D, Pedišić Ž, Palarea-Albaladejo J, Martín-Fernández JA, Hron K, Olds T. Compositional data analysis in time-use epidemiology: what, why, how. Int J Environ Res Public Health. 2020;17(7):2220.
Australian Bureau of Statistics. National health survey: first results 2018–2018. 2018.
Acknowledgments
The authors acknowledge Samuel Lai for his contribution to the data extraction.
Funding
The presented work received financial funding through National Heart Foundation of Australia Future Leader Fellowship (Award ID 101895) awarded to NDR. BAS is a Deakin University Postgraduate Research Scholarship Recipient. JS is supported by a National Health and Medical Research Council Leadership Level 2 Fellowship (GNT1176885). LA is supported by an Australian Research Council Discovery Early Career Researcher Award (DE220100847). NDR is supported by a NHFA Future Leader Fellowship (Award ID 101895). The content of this manuscript is the responsibility of the authors and does not necessarily reflect the views of the funding bodies.
Author information
Authors and Affiliations
Contributions
BS and NR conceptualised the review. BS conducted the database searches. BS, SV, and NR screened the titles, abstracts, and full-text papers. BS and SV extracted the data. NR was consulted for full text inclusion. BS and SV conducted the methodological quality assessment. NR, JS, and LA were consulted for decision making. BS drafted the initial manuscript. All authors reviewed and revised the manuscript, and approved the final manuscript as submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
N/A
Consent for publication
N/A
Competing interests
The authors have no conflicts of interest or competing interests. The authors had no financial relationships with any organisations that might have an interest in the presented work in the previous 3 years; no other relationships or activities that could appear to have influenced the presented work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA 2020 Checklist.
Additional file 2.
Search strategy.
Additional file 3.
Modified McMaster Quality Assessment Tool for Quantitative Activity Compensation Studies.
Additional file 4.
Critical Review Form – Qualitative Studies (Version 2.0).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Swelam, B.A., Verswijveren, S.J.J.M., Salmon, J. et al. Exploring activity compensation amongst youth and adults: a systematic review. Int J Behav Nutr Phys Act 19, 25 (2022). https://doi.org/10.1186/s12966-022-01264-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-022-01264-6