
Abstract
Background
Regular physical activity is associated with physical, social and mental health benefits, whilst insufficient physical activity is associated with several negative health outcomes (e.g. metabolic problems). Population monitoring of physical activity is important to gain insight into prevalence of compliance to physical activity recommendations, groups at risk and changes in physical activity patterns. This review aims to provide an overview of all existing studies that measure physical activity in youth, in cross-European studies, to describe the variation in population levels of physical activity and to describe and define challenges regarding assessment methods that are used.
Methods
A systematic search was performed on six databases (PubMed, EMBASE, CINAHL, PsycINFO, SportDiscus and OpenGrey), supplemental forward- and backward tracking was done and authors’ and experts’ literature databases were searched to identify relevant articles. Journal articles or reports that reported levels of physical activity in the general population of youth from cross-European studies were included. Data were reviewed, extracted and assessed by two researchers, with disagreements being resolved by a third researcher. The review protocol of this review is published under registration number CRD42014010684 in the PROSPERO database.
Results
The search resulted in 9756 identified records of which 30 articles were included in the current review. This review revealed large differences between countries in prevalence of compliance to physical activity recommendations (i.e. 60 min of daily moderate- to vigorous-intensity physical activity (MVPA)) measured subjectively (5–47 %) and accelerometer measured minutes of MVPA (23–200 min). Overall boys and children were more active than girls and adolescents. Different measurement methods (subjective n = 12, objective n = 18) and reported outcome variables (n = 17) were used in the included articles. Different accelerometer intensity thresholds used to define MVPA resulted in substantial differences in MVPA between studies conducted in the same countries when assessed objectively.
Conclusions
Reported levels of physical activity and prevalence of compliance to physical activity recommendations in youth showed large variation across European countries. This may reflect true variation in physical activity as well as variation in assessment methods and reported outcome variables. Standardization across Europe, of methods to assess physical activity in youth and reported outcome variables is warranted, preferably moving towards a pan-European surveillance system combining objective and self-report methods.
Similar content being viewed by others


Background
Recommendations published by the World Health Organization (WHO) state that children and adolescents should accumulate at least 60 min of moderate- to vigorous-intensity physical activity (MVPA) daily. Additionally, within these 60 min, vigorous-intensity physical activity (VPA) should be incorporated at least three times per week [1]. Such levels of physical activity are associated with physical, social and mental health benefits [2–4]. Besides, physical activity in childhood and adolescence is positively related to adult physical activity [4, 5] and health [4, 6].
To establish accurate prevalence data and to monitor changes in physical activity in youth, valid and reliable measures are required [7, 8]. Physical activity can either be measured objectively or subjectively. Traditionally, physical activity is assessed by means of self-report questionnaires, especially in larger population studies [9, 10]. Because such self-report measures are prone to bias, recently more objective assessment methods (e.g. pedometers or accelerometers) are also being used [11]. However, such objective methods come with their own challenges. For example, consensus still has to be reached regarding the accuracy of steps recorded by different pedometers [12], as well as the specific accelerometer intensity thresholds [11, 13] that correspond with low intensity physical activity (LPA), MVPA or VPA in youth. Furthermore, pedometer and accelerometer assessments do not provide information regarding the context of physical activity [14].
In 2013, twelve European Member States established a Knowledge Hub on DEterminants of DIet and Physical ACtivity (DEDIPAC) through a joint Programming Initiative. One of DEDIPAC’s aims is: “enabling a better standardised and more continuous pan-European ‘needs analysis’, i.e. to monitor dietary, physical activity and sedentary behaviours and changes in these behaviours across the life course and within populations to identify targets and target populations for (policy) interventions” [15].
Providing an overview of the existing cross-European (i.e. more than one European country involved) studies that monitor physical activity and sedentary behaviour levels, and their reported population levels, was identified as the first step towards standardisation in population surveillance. In 2010 the WHO [16] published an extensive report, with an overview of existing national and international studies on physical activity levels in European countries. Unfortunately, this report did not provide country specific physical activity levels. Also, it was concluded that national studies used various methods and often non-standardized instruments which led to non-comparable data. Therefore, this systematic review gives an update of cross-European surveillance systems, and reports physical activity levels per country in order to enable comparison of physical activity levels between countries.
Within DEDIPAC, four systematic literature reviews have been conjointly performed to study the variation in population levels of 1) physical activity in youth (the current review) 2) sedentary behaviour in youth [17], 3) physical activity in adults [18] and 4) sedentary behaviour in adults [19]. The purpose of this systematic review is to provide an overview of existing cross-European studies on physical activity in European youth (<18 years), to describe the variation in population levels of physical activity in European youth and in assessment methods used to assess physical activity in cross-European studies, and to define challenges regarding the assessment and reporting methods. These results will be discussed in relation to possible harmonization of physical activity measurement and monitoring across Europe.
Methods
As described in the introduction this systematic literature review is part of a set of four reviews. Because the four systematic reviews originate from the same project, have similar objectives (although for different behaviours and/or age groups) and share their methodology, the introduction-, methods- and discussion sections of the review articles have obvious similarities. The search, article selection, data extraction and quality assessment were conducted conjointly for all four reviews. Subsequently, the included articles were allocated to the appropriate review. One article could be included in multiple reviews. If an article included both youth (<18 years) and adults (≥18 years) and presented stratified results, those stratified results were used in the appropriate review. If the article did not present stratified results, the article was allocated to the most appropriate review, based on the mean age (and age distribution) of the study sample. Before the search commenced, review protocols were written based on the “Centre for Reviews and Dissemination’s guidance for undertaking reviews in health care” [20], and registered in the PROSPERO database [21]. The review protocol of this review on physical activity in youth is published under registration number CRD42014010684. The reporting of this systematic review adheres to the preferred reporting items of the PRISMA-P checklist (Additional file 1).
Search strategy
The search was conducted in June 2014 and updated in February 2016. Six databases (PubMed, EMBASE, CINAHL, PsycINFO, SportDiscus and OpenGrey) were searched using similar search strategies, adapted to each database. The following search terms were used: ‘Physical activity’ OR ‘Sedentary behaviour’ AND ‘Europe’ (including all individual country names) AND ‘Countries’/’Multi-country’/’International’. Both the index terms and the title and abstract were searched and synonyms (e.g. for physical activity: physically active and physical exercise) were used. The complete search string can be found in Additional file 2. Based on the in- and exclusion criteria described below, search filters of the databases were used when possible, for example to select the appropriate publication period or language.
In addition, complementary search strategies were used. After the full-text review phase, the reference lists of the included articles were scanned (backward tracking) and a citation search was performed for the included articles (forward tracking) to identify potentially appropriate articles. Also, several experts in the field of physical activity and sedentary behaviour were contacted to provide additional articles. Finally, all authors involved in the four reviews were asked to search their own literature databases for appropriate articles. All additionally retrieved articles underwent the same selection process as the original articles - as described below.
Article selection
All retrieved records were imported into Reference Manager 12 (Thomson Reuters, New York). Duplicates were hand-searched and removed. Records were included if they were journal articles, reports or doctoral dissertations (further referred to as ‘articles’) written in English. To be included articles needed to report on observational studies conducted after 01-01-2000 (to avoid reporting outdated data) in the general, healthy population. In addition, articles were only included if they provided data for two or more European countries (as defined by the Council of Europe) [22]. With regard to physical activity, articles were included if they reported total physical activity (e.g. minutes/day or meeting recommendations), and/or physical activity in leisure time. Articles that only reported on transport, occupational or household physical activity were excluded. Both subjective (e.g. questionnaires) and objective (e.g. accelerometers) measures were included.
Three researchers (AL,LVH,MV) were involved in the article selection, data extraction and quality assessment. For the title selection, the three researchers each independently reviewed 1/3 of the titles of the retrieved articles. For the abstract and the full-text selection, data extraction and quality assessment, the three researchers each covered 2/3 of the articles, so that each article was independently reviewed, extracted and assessed by two different researchers. Disagreement between the two researchers was resolved by the third researcher.
Data extraction
A standardized data extraction file was used to extract data regarding the study characteristics, the study sample, the assessment methods, the reported outcomes, and the findings. We did not obtain the original data. The complete data extraction file can be found in Additional file 3. To present the data more clearly and to allow for comparisons between age groups, the results are presented and discussed separately for children (age 0–12) and adolescents (age 13–18). When a study reported on a sample that covered both childhood and adolescence (e.g. 9–15 year olds), the data was presented in both sections in this manuscript.
Quality assessment
A quality score was used to provide a general overview of the quality of the included articles. The ‘Standard quality assessment criteria for evaluating primary research papers from a variety of fields’ [23] was used for the assessment. The checklist consists of fourteen items to be scored ‘Yes’ (2 points), ‘Partial’ (1 point), ‘No’ (0 points) and ‘Not applicable’. The summary score was calculated as follows: Total sum ((number of ‘Yes’ x 2) + (number of ‘Partial’ x 1))/Total possible sum (28 – (number of ‘Not applicable’ x 2)). This instrument was chosen because it provides the opportunity to assess and compare the quality of different study designs, focuses on both the research and the reporting, and allows researchers to indicate that an item is not applicable, without affecting the total quality score. The complete quality assessment file can be found in Additional file 4.
Results
Overview of the existing cross-European studies on physical activity in youth
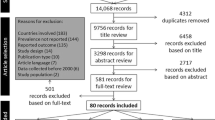
Our search (original and update combined) resulted in 9756 articles, after exclusion of duplicates. After the titles and abstracts were screened, 581 full texts were obtained and reviewed. This resulted in 80 articles, of which 30 articles reported data on physical activity in youth [24–53]. The three main reasons for exclusion for the four reviews together were: (a) fewer than two countries involved (n = 183), (b) outcome not reported per country (n = 144), and (c) suitability of the reported outcome variables, for example when only active transportation was reported (n = 135) (Fig. 1).

Flowchart of the combined review process
We only included articles published between 2000 and 2016 but 80 % (n = 24) were published after 2008. All articles except two had a cross-sectional design: Ortega et al. [37] used a longitudinal design, but only follow up data of this study were included in the review, because baseline data were collected before 2000 and Ekelund et al. [47] pooled data from cross-sectional and longitudinal studies. The number of European countries included in these articles, ranged from 2 to 36. All articles included data from boys and girls and sample size ranged from 301 to 479,674 participants. The quality score ranged from 0.68 to 1 (maximum score = 1). A short summary of the articles including demographic characteristics of the sample, assessment methods and reported outcome variables per article is presented in Table 1.
Variation in population levels of physical activity in European Youth
Levels of physical activity are presented by European country for children (0–12 years) in Table 2 and for adolescents (13–18 years) in Table 3. Most articles included in this review provided data from datasets of larger European studies such as the ENERGY-, EPAPA-, EYHS, HBSC-, ICAD-, IDEFICS, ISCOLE- or TOYBOX-study. To describe the variation in population levels of physical activity in youth (Tables 2 and 3; Figs. 2 and 3), not all articles were included to avoid presenting results from the same data twice. If there was more than one article per study reporting exactly the same outcome variable in a similar way in the same sample, the article with the largest amount of information was chosen [28–30, 32, 38, 39, 42, 44, 46, 47, 49, 50]. No data were available for the following countries: Andorra, Azerbaijan, Bosnia and Herzegovina, Cyprus (no data for adolescents), Georgia, Liechtenstein, Monaco, Montenegro, San Marino and Serbia. These countries (n = 10) represent 21 % of the 47 European countries but less than 3 % of the European population [54]. For clarity, values presented in the tables are for the total sample numbers, except where the articles reported data for boys and girls separately. For the Health Behaviour in School Children (HBSC study), the most recent data was presented in the tables (survey13/14). The values of the 11 year olds were included in Table 2 and the values for the 15 year olds in Table 3.

Average daily counts per minute in children across countries based on different articles. When data were reported separately for boys and girls [30, 38], the mean was reported. Ekelund et al. [47] reported on pooled data from different studies and cleaned and processed the data together. In the Figure the original study is mentioned in the legend: ENERGY = European energy balance research to prevent excessive weight gain among youth; EYHS = European Youth Heart Study; ICAD = International Children’s Accelerometry Database; CSCIS = Copenhagen School Child Intervention Study; ALSPAC = Avon Longitudinal Study of Parents and Children; PEACH = Personal and Environmental Associations with Children’s Health; SPEEDY = Sport, Physical activity and Eating behaviour, Environmental Determinants in Young People; MAGIC = Movement and Activity Glasgow Intervention in Children; KISS = Kindersportstudie; Verloigne et al. [30] reported counts per 15 s, to harmonize results, this was multiplied by four to obtain counts per minute

Average daily counts per minute in adolescents across countries based on different articles. When data were reported separately for boys and girls [37, 38], the mean was reported. Ekelund et al. [47] reported on pooled data from different studies and cleaned and processed the data together. In the Figure the original study is mentioned in the legend: EYHS = European Youth Heart Study; ICAD = International Children’s Accelerometry Database; ALSPAC = Avon Longitudinal Study of Parents and Children; PEACH = Personal and Environmental Associations with Children’s Health; KISS = Kindersportstudie
Generally, boys were more active than girls independent of the measurement method or reported outcome variables, and children tended to be more active than adolescents (Tables 2 and 3). Moreover, in most European countries, less than 50% of children and adolescents complied with the recommended levels of physical activity, regardless of the measurement method. However, there was a large variation between countries. The HBSC study was arguably the best option to compare PA levels in youth between European countries, because it included data from 36 countries. Self-reported data from HBSC 2016 [46] indicated that among 11-year-olds Italy (13 %), Denmark (15 %) and Greece (16 %) had the lowest prevalence of children meeting recommended physical activity levels, while Finland (41 %), Ireland (38 %) and Bulgaria (36 %) had the highest prevalence. However, self-report data are likely to provide less valid data of compliance to physical activity recommendations [55].
Comparison of physical activity levels among youth in European countries using objective measurement methods
For effective comparison of physical activity levels among youth between articles, the same physical activity outcome variables have to be reported and data have to be cleaned and processed the same way. The best comparable outcome reported in the included articles (i.e. not influenced by the specific intensity thresholds that are used), was accelerometer measured average daily counts per minute (CPM). In Figs. 2 and 3, accelerometer derived average daily CPM are presented for children and adolescents. Average daily counts per minute varied between 492 CPM and 804 CPM for children and between 486 and 647 CPM for adolescents. Some differences between countries can be observed for the data in children, for example within one study [38] an average CPM of 804 was reported for Norway compared with an average CPM of 670 for Denmark. Furthermore, some variation within countries can be observed, for example one study [47] reported an average CPM of 711 for 9–10 year old Norwegians, whereas another study [38] reported an average CPM of 804 for Norwegian 9-year-olds. In adolescents more similar results between and within countries were found.
The objectively measured outcome that was reported most frequently was “minutes of MVPA per day”. Figure 4 shows minutes of MVPA per day in children for articles reporting accelerometer derived data. Different intensity thresholds for converting accelerometer-based CPM to minutes per day of MVPA were used across the articles. These cut-off decisions resulted in different classifications of activity levels. For example Riddoch et al. [38] reported 179 min of MVPA in children per day in Portugal, compared to 29 min reported by Ekelund et al. [47]. This resulted in a difference of 150 min of MVPA per day in the same country, even though these articles used the same dataset from the EYHS study. The high values of MVPA across any country reported in the articles of Riddoch et al. [38] and Nilsson et al. [36] can be attributed to the low intensity thresholds that were used to define MVPA (respectively >1000 CPM and >2000 CPM) compared to the intensity threshold used in the other articles [30, 31, 47] (>3000 CPM).

Minutes per day of accelerometer based MVPA in children across countries based on different articles. When data were reported separately for boys and girls [30, 38] or week and weekend day [36], the mean was reported. Ekelund et al. [47] reported on pooled data from different studies and cleaned and processed the data together. In the Figure the original study is mentioned in the legend. ENERGY = European energy balance research to prevent excessive weight gain among youth, EYHS = European Youth Heart Study; ICAD = International Children’s Accelerometry Database; CSCIS = Copenhagen School Child Intervention Study; ALSPAC = Avon Longitudinal Study of Parents and Children; PEACH = Personal and Environmental Associations with Children’s Health, SPEEDY = Sport, Physical activity and Eating behaviour, Environmental Determinants in Young People, KISS = Kindersportstudie; ISCOLE = The international study of childhood obesity, lifestyle and the environment
Figure 5 shows minutes of MVPA per day in adolescents for articles reporting accelerometer derived data. The same pattern can be observed as in children. Minutes of MVPA per day in the articles of Riddoch et al. [38] and Nilsson et al. [36] were markedly higher in each country than the values reported in the article of Ekelund et al. [47] due to the intensity thresholds that were used (respectively >1000 CPM and >2000 CPM and >3000 CPM). However, Ortega et al. [37] and Nilsson et al. [36] used the same intensity threshold (>2000 CPM) but did not report similar levels of MVPA due to differences in age of participants and period of data collection: participants in the article of Nilsson et al. [36] were 15 years old compared to 18 years in the article of Ortega et al. [37] and data used by Nilsson et al. [36] was collected between 1997 and 2000 and the data reported by Ortega et al. [37] was collected in 2007. This indicates that variation in levels of physical activity reported in different articles is not only due to the intensity thresholds that were used, but also to sample characteristics and data collection periods.

Minutes per day of accelerometer based MVPA in adolescents across countries based on different articles. When data were reported separately for boys and girls [37, 38] or week and weekend day [36], the mean was reported. Ekelund et al. [47] reported on pooled data from different studies and cleaned and processed the data together. In the Figure the original study is mentioned in the legend. EYHS = European Youth Heart Study; ICAD = International Children’s Accelerometry Database; ALSPAC = Avon Longitudinal Study of Parents and Children; PEACH = Personal and Environmental Associations with Children’s Health
Comparison of physical activity levels among youth in European countries using subjective measurement methods
In Fig. 6 subjectively measured percentage of children meeting the guidelines is presented for 5 countries. ENERGY data reported by Jimenez-Pavon et al. [29] and data from the most recent HBSC report 2016 [46] (survey 09/10) are compared. Data from both studies included about 50 % girls and age groups were comparable (11 year olds [44] and 10–12 years olds [29]). The HBSC study [46] included one single item question on the number of days over the ‘past’ week that participants were physically active for a total of at least 60 min per day. This included sport participation, active transportation, physical activity at school and physical activity at home. The ENERGY study [29] on the other hand included questions on sports participation (2 questions) and active transport (4 questions) in a ‘usual’ week. The two studies reported different amounts of children meeting the guidelines of 60 min of daily MVPA within each European country. For Spain, Greece, Belgium, Hungary (only girls), The Netherlands (only girls) and Switzerland (only girls) the HBSC study [46] reports higher percentages of compliance to physical activity guidelines compared to the ENERGY study [29], whereas for Norway, Slovenia, Switzerland (only boys) and Hungary (only boys) the ENERGY study [29] reports higher percentages of children meeting guidelines compared to the HBSC study [46].

Questionnaire based percentage of boys and girls engaging in MVPA for ≥ 60 min daily in 8 countries across Europe. ENERGY = European energy balance research to prevent excessive weight gain among youth; HBSC = health behaviour in school-aged children
Variation in assessment methods and reported outcome variables
Because there was a large variation in measurement methods and reported outcome variables, an overview is presented in Table 4. Measurement of physical activity was done either objectively (with accelerometers) or subjectively (e.g. with questionnaires or ecological momentary assessment). More than half (n = 16) of the articles included in this review used accelerometers, two used pedometers, ten articles used a questionnaire and two articles used ecological momentary assessment. All questionnaires were self-administered. Eight articles asked questions regarding physical activity in the seven days prior to questionnaire administration and two asked questions regarding an “average week”. The outcomes were reported in seventeen different ways (for example one article [35] reported “% of total time spent in MVPA”, whereas another [37] reported “MVPA in minutes per day”). Of these reported outcomes “% meeting the guidelines on physical activity” (n = 15) and “minutes per day of MVPA” (both measured objectively and subjectively) (n = 11) were used most often. Five different intensity thresholds were used to define MVPA measured with accelerometers in children ranging from >1000 CPM to >3000 CPM and four different intensity thresholds were used in adolescents ranging from >1500 CPM to >2296 CPM. Several accelerometer models were used in the included articles: the EYHS study [34–38] used an older ActiGraph model (MTI7164), whereas in the EPAPA study [32, 33], study by Ramirez-Rico et al. [26] and ISCOLE study [52] more recent ActiGraph models were used (GT1M and GTX3). In the ENERGY study [30, 31], IDEFICS study [49–51] and ICAD study [47, 48] a combination of different models was used: the ENERGY-study used one old (Actitrainer) and two new (GT1M, GT3X) ActiGraph models, the IDEFICS-study used one old (Actitrainer) and one newer ActiGraph model (GT1M) and the ICAD-study pooled studies that used three different models (two older models: 7164, 71256 and one newer model: GT1M).
Another notable feature was, that all accelerometers used in studies included in this review were from one manufacturer (ActiGraph). This shows that research is making progress to more standardized measures, and these data from the same accelerometer may be more easily comparable [56].
Discussion
The aim of this systematic literature review was to provide an overview of the current literature on the population levels of physical activity in youth in cross-European studies, to present population levels of physical activity in European youth, to provide an overview of methods used in cross-European studies and discuss the impact of different assessment methods. Thirty articles were included, in which the number of European countries included ranged from 2 to 36.
Regarding the reported levels of physical activity across European countries, several observations can be made. First of all, there is substantial variability between countries in overall levels of physical activity and in the prevalence of compliance to recommended physical activity levels in youth. In European countries for which data was reported in the included articles, 5 to 47% of children and adolescents complied with the recommended levels of physical activity when measured subjectively, which was consistent with previous research [55]. The objectively measured data ranged from 0 to 60% of youth meeting physical activity recommendations; depending on the intensity thresholds that were used. In previous reviews, results suggested prevalence data between 0 and 100% [55, 56]. Generally, boys were more active than girls and younger children were more active than adolescents. This is consistent with previous literature [57].
These differences may partly be caused by differences in assessment methods used or in sampling methods, but may also be partly caused by true differences in national physical activity levels. This can be illustrated for accelerometer data by the ICAD study, which cleaned, reduced and processed data the same way (and thereby reduced the amount of variability caused by the measurement methods) and found substantial variation between countries [47, 48]. For subjectively measured physical activity, the HBSC study, which collected and processed data the same way, provides an overview of true variation of compliance to physical activity guidelines in 36 European countries [46]. These differences can possibly be caused by cultural differences or differences in physical activity policies between countries (e.g. not all European countries provide the same amount of physical education lessons in school [58]).
A large number of assessment methods have been used in cross-European studies, when assessing physical activity. The use of different methods likely explain some, but not all, of the variability between countries in overall levels of physical activity. For example subjective measurements tend to overestimate measures of physical activity compared to objectively measured physical activity [55]. Nevertheless, subjective measurement methods remain important to measure the context in which physical activity takes place. In this systematic review the subjectively measured data revealed some variability when data were reported in min per day of MVPA. This might well be due to the discrepancy in the questions used to examine total amount of MVPA daily. For example, to examine the total amount of physical activity some questionnaires included more domains (such as: leisure time physical activity, active transportation, physical activity at school) of physical activity than others. Therefore, a minimum requirement for cross-country comparisons include the use of validated, reliable, back-translated, culturally adapted and standardised questions when assessing population levels of physical activity in youth.
Additionally the objectively measured data revealed that when data are presented in minutes per day of MVPA, substantial variation in the reported levels of MVPA in youth is observed. A major factor in this variation are the different intensity thresholds used in the different articles to define MVPA from the accelerometer data. Five different intensity thresholds were used to define MVPA measured with accelerometers in children ranging from >1000 CPM to >3000 CPM and four different intensity thresholds were used in adolescents ranging from >1500 CPM to >3000 CPM. Therefore, different conclusions will be drawn on levels of physical activity in youth depending on which intensity threshold is used. In a previous review a similar range, of intensity thresholds to define MVPA, was reported [56]. Nevertheless, most articles published after 2011 used the intensity thresholds defined by Evenson et al. [59] which were recommended by Trost et al. [13]. This clearly illustrates that research is evolving to more similar methodologies regarding intensity thresholds used for ActiGraph accelerometers.
Consequently, average daily counts per minute (CPM) is a more comparable measurement outcome, as this is not influenced by the specific intensity thresholds that are used. However, this outcome is influenced by data reduction methods, such as the definition of non-wear time and wear protocol (e.g. overnight). Furthermore, this outcome needs calibration in order to be converted into a meaningful outcome such as minutes spent in MVPA [60].
Additionally, different types and models of the same type of accelerometer may produce different results for the same acceleration which need to be considered when interpreting accelerometer derived physical activity data [61]. However, others have concluded that different models of the Actigraph accelerometer yield comparable results [62–66].
No data were available for some countries. These countries should be included in future international studies. Only articles based on HBSC data [39–46] included a broad range of countries (27–36), with all other articles reporting on less than 10 countries. This implies that the HBSC study is the only study that reports reasonably comprehensive data on physical activity levels of youth across Europe. The HBSC survey (01/02) asked about physical activity level with one question on physical activity in the previous week (i.e. “Over the past 7 days, on how many days were you physically active for a total of at least 60 min per day?”) and one on a typical week (i.e. “Over a typical or usual week, on how many days are you physically active for a total of at least 60 min per day?”). In the HBSC studies conducted in 04/05, 09/10 and 13/14 only one question remained (i.e. “On how many days over the past week were you physically active for a total of at least 60 min per day”). These questions (developed by Prochaska et al. [67]) were stated to be a reliable (ICC: 0.77) tool to measure total MVPA in youth and were found to relate significantly with accelerometer data (r = 0.40, p < 0.001) [67].
Strengths and limitations
A possible limitation of this systematic literature review was that only articles in English were included, thereby possibly missing on relevant articles written in another language. The choice of the databases that were searched and additional search strategies could have led to possible missed articles. In this review only articles reporting on total physical activity and leisure time physical activity were included. A selection of other domains such as active transportation or sport participation may have provided a different result.
We only included studies comprising at least two European countries, thereby excluding all national studies. This was decided as national studies often do not use standardised self-report instruments and data reduction and processing methods are diverse, which limits comparability between countries [16, 68]. Objectively measured physical activity data from national studies may have been better comparable than subjectively measured physical activity data. However, differences in sampling methods and data cleaning and –reduction procedures may limit cross-country comparisons. Harmonization of data prior to comparison between countries is possible and should be the recommended practice [16]. Another limitation of this systematic review was that we excluded all articles that measured physical activity in youth in multiple European countries but did not report levels of physical activity separately per country. Such an example is the HELENA-study (Healthy lifestyle in Europe by nutrition in adolescence) [69].
The most important strengths of this review are its systematic character and profound review process. The search protocol was not adjusted throughout the entire review process. The search was performed for the four reviews (on physical activity in youth, physical activity in adults, sedentary time in youth and sedentary time in adults) together. This provided a solid search strategy with the maximum likelihood of capturing all relevant articles. The study selection, data extraction process, and quality assessment were performed by two researchers, with initial disagreement being resolved by a third researcher.
Recommendations for future research
This review shows that there is an urgent need for international consensus regarding data-cleaning, reduction and processing rules for accelerometer data and for standardization of questions used to assess physical activity in youth. This can be done by building on previous work, for example the International Children’s Accelerometry Database (ICAD) project pooled individual accelerometer data files and cleaned, reduced and processed it using standardized methods [70]. This can be used as a good starting point for future international guidelines on cleaning, reducing and processing accelerometer data, to assure that outcome variables across studies can easily be compared. Additionally consensus regarding intensity thresholds for defining different levels of physical activity intensity based on accelerometer data is needed. Trost et al. [13] evaluated the validity of 5 different intensity thresholds used to define MVPA with ActiGraph accelerometers in youth and used indirect calorimetry as reference. They recommend to use the intensity threshold as proposed by Evenson et al. [59] (i.e. 2296 CPM) to define MVPA measured with ActiGraph accelerometers in children and adolescents. As currently, most researchers are already using this intensity threshold, this could be a point of departure for future international consensus on ActiGraph accelerometer intensity thresholds. Furthermore, many recent accelerometers have the capacity to store the raw acceleration data in non-compressed form, eliminating the loss of precision caused by data compression methods including the use of “counts” or “epochs”. Thereby removing the need for “counts” based intensity thresholds, and allowing the possibility of identifying specific activities from the accelerometer data using neural networking or machine learning to identify activities followed by the use of “look up” tables to find an associated energy cost [71, 72].
Additionally there is a wide range of questionnaires available to assess physical activity and all questionnaires have inherent limitations. There are still many differences in data administration, data cleaning and which domains of physical activity (such as: active travel, leisure time, physical activity at school) are questioned. Therefore harmonization is needed and valid and reliable questionnaires should be used in future research.
When guidelines are used to define prevalence rates of physical activity, we recommend to use the WHO [1] guidelines of 60 min MVPA per day (including vigorous-intensity physical activities at least three times a week). Additionally, we recommend future research to report data separately per country to enable comparison between countries.
Conclusion
The present review shows that the available cross-European studies on physical activity in youth used widely varying objective and subjective physical activity assessment methods, different definitions of intensity of physical activity, and various outcome variables. Substantial variation in levels of physical activity and low compliance to physical activity recommendations in youth between countries were reported for subjectively and objectively measured physical activity. The objectively assessed physical activity data varied substantially among articles due to the intensity thresholds used. The results highlight the need to standardize or harmonize data reduction methods, methods to assess physical activity and outcome measures used in physical activity research among youth across Europe. A Pan-European surveillance system should be aimed for, combining accelerometer-based measures of physical activity with domain specific physical activity questionnaires to gain information on the type and context of physical activity.
Abbreviations
- ALSPAC:
-
Avon Longitudinal Study of Parents and Children
- B:
-
Boys
- BMI:
-
Body mass index
- BTS:
-
Bouts
- CH:
-
Cohort
- CPM:
-
Counts per minute
- CS:
-
crosssectional
- CSCIS:
-
Copenhagen School Child Intervention Study
- DEDIPAC:
-
DEterminants of DIet and Physical ACtivity
- E.M.A.:
-
Ecological momentary assessment
- ENERGY:
-
European energy balance research to prevent excessive weight gain among youth
- ENG:
-
England
- EPAPA:
-
Evaluation and Promotion of Adolescent Physical Activity
- EYHS:
-
European Youth Heart Study
- FAS:
-
Family affluence scale
- FL:
-
Flanders
- Ft:
-
Full-time employed mother
- FYRM:
-
The former Yugoslav Republic of Macedonia
- G:
-
Girls
- HBSC:
-
Health behaviour in school-aged children
- ICAD:
-
International Children’s Accelerometry Database
- IDEFICS:
-
Identification and prevention of dietary and lifestyle induced health effects in children and infants
- ISCED:
-
International Standard Classification of Education
- ISCOLE:
-
The international study of childhood obesity, lifestyle and the environment
- KISS:
-
Kinder Sportstudie
- LPA:
-
light-intensity physical activity
- LT:
-
Longitudinal
- MAGIC:
-
Movement and Activity Glasgow Intervention in Children
- min:
-
minutes
- MPA:
-
moderate-intensity physical activity
- MVPA:
-
Moderate- to vigorous-intensity physical activity
- n:
-
non-employed mother
- n. r.:
-
not reported
- PEACH:
-
Personal and Environmental Associations with Children’s Health
- PEL:
-
Parental education level
- Pt:
-
Part-time employed mother
- SC:
-
Scotland
- SES:
-
Socio-economic status
- SPEEDY:
-
Sport, Physical activity and Eating behaviour, Environmental Determinants in Young People
- UEM:
-
University Education Mother
- VPA:
-
Vigorous-intensity physical activity
- WAL:
-
Wales
- WHO:
-
World Health Organisation
- WR:
-
Walloon Region
References
WHO. Global recommendations on physical activity for health. 2010.
Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. Cmaj. 2006;174(6):801–9. doi:10.1503/cmaj.051351.
Janssen I, Leblanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7:40. doi:10.1186/1479-5868-7-40.
Hallal PC, Victora CG, Azevedo MR, Wells JC. Adolescent physical activity and health: a systematic review. Sports Med. 2006;36(12):1019–30.
Telama R, Yang X, Viikari J, Valimaki I, Wanne O, Raitakari O. Physical activity from childhood to adulthood: a 21-year tracking study. Am J Prev Med. 2005;28(3):267–73. doi:10.1016/j.amepre.2004.12.003.
Kohrt WM, Bloomfield SA, Little KD, Nelson ME, Yingling VR. American College of Sports Medicine Position Stand: physical activity and bone health. Med Sci Sports Exerc. 2004;36(11):1985–96.
Caspersen CJ, Nixon PA, DuRant RH. Physical activity epidemiology applied to children and adolescents. Exerc Sport Sci Rev. 1998;26:341–403.
Trost SG. Objective measurement of physical activity in youth: current issues, future directions. Exerc Sport Sci Rev. 2001;29(1):32–6.
Sirard JR, Pate RR. Physical activity assessment in children and adolescents. Sports Med. 2001;31(6):439–54. doi:10.2165/00007256-200131060-00004.
Corder K, Ekelund U, Steele RM, Wareham NJ, Brage S. Assessment of physical activity in youth. J Appl Physiol (1985). 2008;105(3):977–87.
Guinhouya CB, Hubert H, Soubrier S, Vilhelm C, Lemdani M, Durocher A. Moderate-to-vigorous physical activity among children: discrepancies in accelerometry-based cut-off points. Obesity (Silver Spring). 2006;14(5):774–7. doi:10.1038/oby.2006.89.
Schneider PL, Crouter S, Bassett DR. Pedometer measures of free-living physical activity: comparison of 13 models. Med Sci Sports Exerc. 2004;36(2):331–5. doi:10.1249/01.MSS.0000113486.60548.E9.
Trost SG, Loprinzi PD, Moore R, Pfeiffer KA. Comparison of accelerometer cut points for predicting activity intensity in youth. Med Sci Sports Exerc. 2011;43(7):1360–8. doi:10.1249/MSS.0b013e318206476e.
Dollman J, Okely AD, Hardy L, Timperio A, Salmon J, Hills AP. A hitchhiker’s guide to assessing young people’s physical activity: Deciding what method to use. J Sci Med Sport. 2009;12(5):518–25. doi:10.1016/j.jsams.2008.09.007.
Lakerveld J, van der Ploeg HP, Kroeze W, Ahrens W, Allais O, Andersen LF, et al. Towards the integration and development of a cross-European research network and infrastructure: the DEterminants of DIet and Physical ACtivity (DEDIPAC) Knowledge Hub. Int J Behav Nutr Phys Act. 2014;11:143. doi:10.1186/s12966-014-0143-7.
WHO. Review of physical activity surveillance data sources in European Union Member States. 2010 Contract No.: Report no. 6.
Verloigne M, Loyen A, Van Hecke L, Lakerveld J, Hendriksen I, De Bourdheaudhuij I, et al. Variation in population levels of sedentary time in European children and adolescents: a systematic review within DEDIPAC. Int J Behav Nutr Phy. Under review. doi:10.1186/s12966-016-0395-5.
Loyen A, Van Hecke L, Verloigne M, Hendriksen I, Lakerveld J, Steene-Johanessen J, et al. Variation in population levels of physical activity in European adults: a systematic literature review within DEDIPAC. Int J Behav Nutr Phy. Under review. doi:10.1186/s12966-016-0398-2.
Loyen A, Verloigne M, Van Hecke L, Hendriksen I, Lakerveld J, Steene-Johannessen J, et al. Variation in population levels of sedentary time in European adults: a systematic literature review within DEDIPAC. Int J Behav Nutr Phy. Under review. doi:10.1186/s12966-016-0397-3.
Centre for Reviews and Dissemination. Systematic reviews: CRD's guidance for undertaking reviews in health care. 2008. CRD, University of York, York.
PROSPERO. http://www.crd.york.ac.uk/PROSPERO/. Accesed 11 Nov 2015.
Council of Europe. http://www.coe.int/en/web/about-us/our-member-states Accesed 11 Nov 2015
Kmet LM, Lee RC, Cook LS. Standard quality assessment criteria for evaluating primary research papers from a variety of fields. 2004. Alberta Heritage Foundation for Medical Research.
Biddle SJH, Soos I, Hamar P, Sandor I, Simonek J, Karsai I. Physical activity and sedentary behaviours in youth: Data from three Central-Eastern European countries. European Journal of Sport Science. 2009;9(5):295–301. doi:10.1080/17461390902829234.
Duncan MJ, Birch SL, Eyre E, Bryant E, Rutten C, Boen F, et al. Comparisons in ambulatory physical activity in children from the United Kingdom and Belgium. Ann Hum Biol. 2015;42(3):290–2. doi:10.3109/03014460.2014.944568.
Ramirez-Rico E, Hilland TA, Foweather L, Fernandez-Garcia E, Fairclough SJ. Weekday and weekend patterns of physical activity and sedentary time among Liverpool and Madrid youth. European Journal of Sport Science. 2014;14(3):287–93. doi:10.1080/17461391.2013.827242.
Soos I, Biddle S, Ling J, Hamar P, Sandor I, Boros-Balint I, et al. Physical activity, sedentary behaviour, use of electronic media, and snacking among youth: an international study. Kinesiology. 2014;46(2):155–63.
Fernandez-Alvira JM, De Bourdeaudhuij I, Singh AS, Vik FN, Manios Y, Kovacs E, et al. Clustering of energy balance-related behaviors and parental education in European children: the ENERGY-project. Int J Behav Nutr Phy. 2013;10. doi: 10.1186/1479-5868-10-5.
Jimenez-Pavon D, Fernandez-Alvira JM, te Velde SJ, Brug J, Bere E, Jan N, et al. Associations of parental education and parental physical activity (PA) with children’s PA: the ENERGY cross-sectional study. Prev Med. 2012;55(4):310–4. doi:10.1016/j.ypmed.2012.07.011.
Verloigne M, Van Lippevelde W, Maes L, Yildirim M, Chinapaw M, Manios Y, et al. Levels of physical activity and sedentary time among 10- to 12-year-old boys and girls across 5 European countries using accelerometers: an observational study within the ENERGY-project. Int J Behav Nutr Phys Act. 2012;9:34. doi:10.1186/1479-5868-9-34.
Yildirim M, Schoeni A, Singh AS, Altenburg TM, Brug J, De Bourdeaudhuij I, et al. Daily variations in weather and the relationship with physical activity and sedentary time in European 10- to 12-year-olds: The ENERGY-Project. J Phys Act Health. 2014;11(2):419–25. doi:10.1123/jpah.2012-0102.
Aibar A, Bois JE, Generelo E, Zaragoza Casterad J, Paillard T. A cross-cultural study of adolescents’ physical activity levels in France and Spain. European Journal of Sport Science. 2013;13(5):551–8. doi:10.1080/17461391.2012.746733.
Aibar A, Bois JE, Zaragoza Casterad J, Generelo E, Paillard T, Fairclough S. Weekday and weekend physical activity patterns of French and Spanish adolescents. European Journal of Sport Science. 2014;14(5):500–9. doi:10.1080/17461391.2013.829127.
Andersen LB, Harro M, Sardinha LB, Froberg K, Ekelund U, Brage S, et al. Physical activity and clustered cardiovascular risk in children: a cross-sectional study (The European Youth Heart Study). Lancet. 2006;368(9532):299–304. doi:10.1016/s0140-6736(06)69075-2.
Ekelund U, Sardinha LB, Anderssen SA, Harro M, Franks PW, Brage S, et al. Associations between objectively assessed physical activity and indicators of body fatness in 9- to 10-y-old European children: a population-based study from 4 distinct regions in Europe (the European Youth Heart Study). Am J Clin Nutr. 2004;80(3):584–90.
Nilsson A, Anderssen SA, Andersen LB, Froberg K, Riddoch C, Sardinha LB, et al. Between- and within-day variability in physical activity and inactivity in 9- and 15-year-old European children. Scand J Med Sci Sports. 2009;19(1):10–8. doi:10.1111/j.1600-0838.2007.00762.x.
Ortega FB, Konstabel K, Pasquali E, Ruiz JR, Hurtig-Wennlof A, Maestu J, et al. Objectively measured physical activity and sedentary time during childhood, adolescence and young adulthood: a cohort study. PLoS One. 2013;8(4):e60871. doi:10.1371/journal.pone.0060871.
Riddoch CJ, Andersen LB, Wedderkopp N, Harro M, Klasson-Heggebo L, Sardinha LB, et al. Physical activity levels and patterns of 9-and 15-years-old European children. Med Sci Sports Exerc. 2004;36(1):86–92. doi:10.1249/01.Mss.0000106174.43932.92.
Janssen I, Katzmarzyk PT, Boyce WF, Vereecken C, Mulvihill C, Roberts C, et al. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes Rev. 2005;6(2):123–32. doi:10.1111/j.1467-789X.2005.00176.x.
Currie Cea. Young people’s health in context. Health behavior in school aged children (HBSC): international report from the 2001/2002 survey. 2004
Haug E, Rasmussen M, Samdal O, Iannotti R, Kelly C, Borraccino A, et al. Overweight in school-aged children and its relationship with demographic and lifestyle factors: results from the WHO-Collaborative Health Behaviour in School-aged Children (HBSC) study. International Journal of Public Health. 2009;54 Suppl 2:167–79. doi:10.1007/s00038-009-5408-6.
Currie Cea. Inequalities in young people’s health. Health behavior in school aged children (HBSC): international report from the 2005/2006 survey. 2008.
Ramos P, Brooks F, Garcia-Moya I, Rivera F, Moreno C. Eating habits and physical activity in dieter and non-dieter youth: A gender analysis of English and Spanish adolescents. Social Science Journal. 2013;50(4):575–82. doi:10.1016/j.soscij.2013.09.017.
Currie Cea. Social determinants of health and well-being among young people. Health behavior in school aged children (HBSC): international report from the 2009/2010 survey. 2010.
Kalman M, Inchley J, Sigmundova D, Iannotti RJ, Tynjala JA, Hamrik Z, et al. Secular trends in moderate-to-vigorous physical activity in 32 countries from 2002 to 2010: a cross-national perspective. Eur J Pub Health. 2015;25 Suppl 2:37–40. doi:10.1093/eurpub/ckv024.
Inchley J, Currie D, Young T, Samdal O, Torsheim T, Augustson L, et al. Growing up unequal: gender and socioeconomic differences in young people’s health and well-being. International report from the 2013/2014 survey. 2016.
Ekelund U, Luan JA, Sherar LB, Esliger DW, Griew P, Cooper A, et al. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA. 2012;307(7):704–12. doi:10.1001/jama.2012.156.
Hildebrand M, Kolle E, Hansen BH, Collings PJ, Wijndaele K, Kordas K, et al. Association between birth weight and objectively measured sedentary time is mediated by central adiposity: data in 10,793 youth from the International Children’s Accelerometry Database. Am J Clin Nutr. 2015;101(5):983–90. doi:10.3945/ajcn.114.103648.
Gwozdz W, Sousa-Poza A, Reisch LA, Ahrens W, Eiben G, Fernandez-Alvira JM, et al. Maternal employment and childhood obesity - A European perspective. J Health Econ. 2013;32(4):728–42. doi:10.1016/j.jhealeco.2013.04.003.
Konstabel K, Veidebaum T, Verbestel V, Moreno LA, Bammann K, Tornaritis M, et al. Objectively measured physical activity in European children: the IDEFICS study. Int J Obes. 2014;38 Suppl 2:S135–43. doi:10.1038/ijo.2014.144.
Kovacs E, Hunsberger M, Reisch L, Gwozdz W, Eiben G, De Bourdeaudhuij I, et al. Adherence to combined lifestyle factors and their contribution to obesity in the IDEFICS study. Obes Rev. 2015;16 Suppl 2:138–50. doi:10.1111/obr.12349.
Katzmarzyk PT, Barreira TV, Broyles ST, Champagne CM, Chaput JP, Fogelholm M, et al. Physical activity, sedentary time, and obesity in an international sample of children. Med Sci Sports Exerc. 2015;47(10):2062–9. doi:10.1249/MSS.0000000000000649.
De Craemer M, Lateva M, iotova V, De Decker E, Verloigne M, De Bourdeaudhui I et al. Differences in Energy Balance-Related Behaviours in European Preschool Children: The ToyBox-Study. PLoS One. 2015;10(3).
Eurostat. European statistics. http://ec.europa.eu/eurostat/. Accessed 02 Nov 2015.
Ekelund U, Tomkinson G, Armstrong N. What proportion of youth are physically active? Measurement issues, levels and recent time trends. Br J Sports Med. 2011;45(11):859–65. doi:10.1136/bjsports-2011-090190.
Guinhouya BC, Samouda H, de Beaufort C. Level of physical activity among children and adolescents in Europe: a review of physical activity assessed objectively by accelerometry. Public Health. 2013;127(4):301–11. doi:10.1016/j.puhe.2013.01.020.
Trost SG, Pate RR, Sallis JF, Freedson PS, Taylor WC, Dowda M, et al. Age and gender differences in objectively measured physical activity in youth. Med Sci Sports Exerc. 2002;34(2):350–5.
Physical Education and Sport at School in Europe Eurydice Report. European Commission/EACEA/Eurydice, 2013.
Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sports Sci. 2008;26(14):1557–65. doi:10.1080/02640410802334196.
Cliff DP, Reilly JJ, Okely AD. Methodological considerations in using accelerometers to assess habitual physical activity in children aged 0–5 years. J Sci Med Sport. 2009;12(5):557–67. doi:10.1016/j.jsams.2008.10.008.
Grydeland M, Hansen BH, Ried-Larsen M, Kolle E, Anderssen SA. Comparison of three generations of ActiGraph activity monitors under free-living conditions: do they provide comparable assessments of overall physical activity in 9-year old children? BMC Sports Sci Med Rehabil. 2014;6:26. doi:10.1186/2052-1847-6-26.
Robusto KT, Trost SG. Comparison of three generations of ActiGraph™ activity monitors in children and adolescents. J Sports Sci. 2012;30(13):1429–35.
Kozey SL, Staudenmayer JW, Troiano RP, Freedson PS. Comparison of the ActiGraph 7164 and the ActiGraph GT1M during self-paced locomotion. Med Sci Sports Exerc. 2010;42(5):971–6. doi:10.1249/MSS.0b013e3181c29e90.
John D, Tyo B, Bassett DR. Comparison of four ActiGraph accelerometers during walking and running. Med Sci Sports Exerc. 2010;42(2):368–74. doi:10.1249/MSS.0b013e3181b3af49.
Lee KY, Macfarlane DJ, Cerin E. Comparison of three models of actigraph accelerometers during free living and controlled laboratory conditions. European Journal of Sport Science. 2013;13(3):332–9. doi:10.1080/17461391.2011.643925.
Vanhelst J, Mikulovic J, Bui-Xuan G, Dieu O, Blondeau T, Fardy P, et al. Comparison of two ActiGraph accelerometer generations in the assessment of physical activity in free living conditions. BMC research notes. 2012;5:187. doi:10.1186/1756-0500-5-187.
Prochaska JJSJ, Long B. A physical activity screening measure for use with adolescents in primary care. Archives of Paediatrics and Adolescent Medicine. 2001;155:554–9.
Rutten A, Ooijendijk WT, Schena F, Sjostrom M, Stahl T, Vanden Auweele Y, Welshman J, Ziemainz H. Physical activity monitoring in Europe. The European Physical Activity Sur veillance System (EUPASS) approach and indicator testing. Public Health Nutr. 2003;6(4):377–84.
Moreno LA, De Henauw S, Gonzalez-Gross M, Kersting M, Molnar D, Gottrand F, et al. Design and implementation of the Healthy Lifestyle in Europe by Nutrition in Adolescence Cross-Sectional Study. Int J Obes. 2008;32 Suppl 5:S4–11. doi:10.1038/ijo.2008.177.
Sherar LB, Griew P, Esliger DW, Cooper AR, Ekelund U, Judge K, et al. International children’s accelerometry database (ICAD): design and methods. BMC Public Health. 2011;11:485. doi:10.1186/1471-2458-11-485.
Staudenmayer J, Pober D, Crouter S, Bassett D, Freedson P. An artificial neural network to estimate physical activity energy expenditure and identify physical activity type from an accelerometer. J Appl Physiol (1985). 2009;107(4):1300–7. doi:10.1152/japplphysiol.00465.2009.
Mannini A, Sabatini AM. Machine learning methods for classifying human physical activity from on-body accelerometers. Sensors. 2010;10(2):1154–75. doi:10.3390/s100201154.
Acknowledgements
Not applicable
Funding
“The preparation of this paper was supported by the DEterminants of DIet and Physical ACtivity (DEDIPAC) knowledge hub. This work is supported by the Joint Programming Initiative ‘Healthy Diet for a Healthy Life’. The funding agencies supporting this work are (in alphabetical order of participating Member State): Belgium: Research Foundation – Flanders; Ireland: The Health Research Board (HRB); The Netherlands: The Netherlands Organisation for Health Research and Development (ZonMw); Norway: The Research Council of Norway, Division for Society and Health.”
Availability of data and supporting materials
Not applicable.
Authors’ contributions
MV, AL and LvH conducted the search, article selection, data extraction and quality assessment and drafted the manuscript. JL, IH, IDB, BD, AD, UE, JB, HvdP conceptualized and designed the study. All authors were involved in critically revising the manuscript for important intellectual content and have read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional files
Additional file 1:
PRISMA checklist. Checklist for systematic review according to PRISMA guidelines. (DOCX 25 kb)
Additional file 2:
The complete search string. (DOCX 11 kb)
Additional file 3:
Data extraction file. The complete data extraction file. (XLSX 91 kb)
Additional file 4:
Quality assessment file. (DOCX 17 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Van Hecke, L., Loyen, A., Verloigne, M. et al. Variation in population levels of physical activity in European children and adolescents according to cross-European studies: a systematic literature review within DEDIPAC. Int J Behav Nutr Phys Act 13, 70 (2016). https://doi.org/10.1186/s12966-016-0396-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-016-0396-4