
Abstract
Background
An individual’s occupational activity (OA) may contribute significantly to daily physical activity (PA) and sedentary behavior (SB). However, there is little consensus about which occupational categories involve high OA or low OA, and the majority of categories are unclassifiable with current methods. The purpose of this study was to present population estimates of accelerometer-derived PA and SB variables for adults (n = 1112, 20–60 years) working the 40 occupational categories collected during the 2003–2004 National Health and Nutrition Examination Survey (NHANES).
Methods
ActiGraph accelerometer-derived total activity counts/day (TAC), activity counts/minute, and proportion of wear time spent in moderate-to-vigorous PA [MVPA], lifestyle, and light PA organized by occupational category were ranked in ascending order and SB was ranked in descending order. Summing the ranks of the six accelerometer-derived variables generated a summary score for each occupational category, which was re-ranked in ascending order. Higher rankings indicated higher levels of OA, lower rankings indicated lower levels of OA. Tertiles of the summary score were used to establish three mutually exclusive accelerometer-determined OA groupings: high OA, intermediate OA, and low OA.
Results
According to their summary score, ‘farm and nursery workers’ were classified as high OA and ‘secretaries, stenographers, and typists’ were classified as low OA. Consistent with previous research, some low OA occupational categories (e.g., ‘engineers, architects, and scientists’, ‘technicians and related support occupations’, ‘management related occupations’, ‘executives, administrators, and managers’, ‘protective services’, and ‘writers, artists, entertainers, and athletes’) associated with higher education and income had relatively greater amounts of MVPA compared to other low OA occupational categories, likely due to the greater percentage of men in those occupations and/or the influence of higher levels of leisure time PA. Men had more TAC, activity counts/minute and time in MVPA, but similar proportions of SB compared to women in all three OA groupings.
Conclusions
Objectively measured PA allowed for a more precise estimate of the amount of PA and SB associated with different occupations and facilitated systematic classification of the 40 different occupational categories into three distinct OA groupings. This information provides new opportunities to explore the relationship between OA and health outcomes.
Similar content being viewed by others


Background
The benefits of regular physical activity (PA), including lowered mortality rates, improved function and enhanced quality of life, are widely recognized [1–4]. An individual can accumulate daily PA through occupational demands, transportation, household tasks, or engagement in leisure time PA (LTPA) [5, 6]. Higher levels of LTPA have been promoted as health enhancing, [2, 3] while the effects of occupational activity (OA) on health remain inconclusive [7–9]. Many studies have shown high levels of OA to be associated with improved health, [7, 10–13] and the detrimental effects of large amounts of occupational sitting [14, 15]. In contrast, other studies have found high levels of OA to have deleterious health effects [9, 16–19].
Due to the substantial amount of time relegated to paid work in today’s society [20–22], an individual’s occupation likely has a strong influence on daily PA and sedentary behaviors (SB) (e.g., does their job require mostly sitting, standing, walking, engaging in repetitive tasks, or heavy labor) [23]. Also OA and LTPA patterns are profoundly different in varying occupations. Blue collar workers may be highly physically active during work, and highly sedentary during leisure, while white collar workers may engage in greater LTPA, after a sedentary day at the office [24, 25]. While extensive research on the comparison of physical demands between different occupations has been performed for decades [26–28], the incorporation of OA into the measurement of daily PA is still evolving [29, 30]. Including OA in addition to LTPA will allow a better understanding of the prevalence of daily PA, and inform interventions aimed to improve health, increase productivity, and reduce work-related injury of the employed population.
Based on self-reported occupation, the National Health and Nutrition Examination Survey (NHANES) III used the 1980 U.S. Census Bureau Classification Codes to classify respondents into 40 defined and diverse occupational categories according to work performed, required skills, education, training, and credentials [31] (Table 1). Previously King et al. [32] used the occupation descriptions of the U.S. Department of Labor as a reference to assign each of the 40 occupational categories to one of three broad OA groupings: (a) high amounts of OA, (b) low amounts of OA, or (c) unclassifiable amounts of OA [32]. Seven of the 40 occupational categories were considered to represent high amounts of OA (e.g., ‘cleaning and building service’, ‘construction laborers’) and 10 were considered to represent low amounts of OA (e.g., ‘secretaries’, ‘teachers’). The remaining 23 occupational categories were considered too ambiguous to classify as either high or low OA and thus were labeled as unclassifiable OA (e.g., ‘health services’, ‘sales workers, retail and personal services’) (Table 1). These three general groupings have been used previously by other researchers [12, 21, 33], with analyses focused primarily on the two more extreme and certain groupings. Since the unclassifiable OA group contains the majority of the occupational categories, (23 of the 40 categories) limiting analysis to only the high and low OA groupings restricts what can be inferred about the relationship between OA and health outcomes.
The 2003–2004 NHANES contained the same 40 occupational categories, and included objectively measured PA and SB collected with accelerometry. This serendipitous coupling presented an opportunity to categorize individuals into new OA groupings using objective data. Therefore, the purpose of this analysis of the 2003–2004 NHANES occupation and accelerometry data was to classify the 40 occupational categories into high OA, intermediate OA, and low OA groupings based on objectively measured PA and SB.
Methods
As a continuous surveillance program conducted by the National Center for Health Statistics (NCHS), the NHANES assesses the health and nutritional status of non-institutionalized U.S. civilians [34]. Complex, multi-stage sampling was used to obtain a nationally representative sample. This analysis focused on a subgroup of the total population; specifically, employed individuals aged 20–60 years. The NCHS Research Ethics Review Board approved all protocols and each participant provided informed consent [34]. Data from the occupational questionnaire, interview, examination, and accelerometry components of NHANES 2003–2004 were used in this analysis. Subsequent NHANES cycles did not use similar occupational categories so the analysis herein is necessarily limited to the 2003–2004 cycle.
Study population
From a potential sample of 2904 participants aged 20–60 years with complete data for all indicated variables (see Table 2 below), participants who reported working at a job or business but not at work (n = 114), going to school or retired (n = 354), having limitations keeping them from working (n = 280), those who did not report an occupational category (n = 231), and those who reported less than full-time work (<35 h/week) [35] were excluded (n = 351) because of the uncertainty in their employment, or mobility status during the activity monitoring period [36]. Keeping with previous analysis, participants with less than 4 valid days (of ≥10 h/day of wear time) of accelerometer data [37] were also excluded (n = 462). The analysis sample ultimately comprised 1112 adults employed full-time in one of 40 occupational categories and with at least 4 days of valid accelerometer data.
Accelerometry
In 2003 NHANES added the PA monitor component to objectively assess participants greater than 6 years of age. NHANES participants received standardized instructions to wear the uniaxial ActiGraph AM-7164 accelerometer (ActiGraph, Fort Walton Beach, FL) over the right hip attached by an elasticized belt for seven consecutive days, and to remove the monitor during sleeping, bathing, and other aquatic activities. The ActiGraph AM-7164 assesses accelerations ranging from 0.05 to 2.0 g that are band limited with a frequency response of 0.25–2.5 Hz. It was programmed to record information in 1 min epochs and measured vertical acceleration transformed to “activity counts/minute,” a proprietary unit of movement and its intensity. After 7 days participants returned the accelerometers to the NHANES data center by pre-paid mail. Prior to its release, the accelerometer data was examined by NHANES staff for unreasonable values and to confirm that instruments remained calibrated. Unreliable data were clearly marked and not used in this analysis. Additional details about the data collection protocol are available on-line at http://www.cdc.gov/nchs/data/nhanes/meccomp.pdf [38].
Data processing followed previously established standards [37]. Specifically, non-wear time was defined as ≥60 consecutive minutes of zero activity counts/minute, allowing for up to 2 min with activity counts/minute between 0 and 100 [37]. To determine valid days (≥10 h/day of wear time), non-wear time was subtracted from 24 h [39]. For participants with at least 4 days, (week or weekend day, consecutive or not) total activity counts/day (TAC) [40] and wear time mean activity counts/minute (indicators of PA volume that capture varying movement intensities throughout the day) were calculated for each day. Accelerometer wear time data were also classified into activity intensity levels using cut points previously established for NHANES (0–99 counts = sedentary; 100–759 counts = light; 760–2019 counts = lifestyle; ≥ 2020 counts = moderate-to-vigorous PA [MVPA]) [37, 41]. The proportion of time in each activity intensity level was determined by dividing minutes spent in each intensity by minutes of wear time. Steps/day were not released for the 2003–2004 NHANES cycle, so they are not considered in this analysis.
Population estimates of PA and SB for occupational categories and establishing OA groupings
Mean and standard error (SE) of the six accelerometer-derived variables (TAC, activity counts/minute, proportion of wear time spent in MVPA, lifestyle, light, and SB) accumulated during an average day were calculated for the individuals within each of the 40 occupational categories. The relative standard error for each variable was less than 30 % in accordance with NCHS standards for reporting, unless otherwise noted [42]. Analyses were conducted using SAS software (Research Triangle Park, NC). To account for the complex sampling design utilized by the NHANES, a 2-year sampling weight was calculated and used for analyses following the recommended guidelines from the NCHS.
The 40 occupational categories from NHANES 2003–2004 were ranked (1–40) in ascending order according to each accelerometer-derived variable, except for SB, which was ranked in descending order. A high rank (e.g., 1) was reflective of having greater amounts of OA, while a low rank (e.g., 40) indicated lower amounts of OA. By summing the rank of all six accelerometer-derived variables, a summary score was assigned to each occupational category. Occupational categories were subsequently ranked in ascending order by their summary scores and three mutually exclusive accelerometer-determined OA groupings were created by splitting the ordered summary scores into tertiles: 1) high OA (top tertile of the summary scores, n = 13), 2) intermediate OA (middle tertile, n = 13), and 3) low OA (bottom tertile, n = 14). Considering that the majority of jobs require little OA we chose to allocate 14 occupational categories to the low OA group [20, 21]. Results are presented for men and women by occupational category and OA grouping.
Differences in the characteristics of high OA, intermediate OA, and low OA individuals were analyzed by chi-square test (categorical variables), and analysis of variance (ANOVA) (continuous variables). Adjusted means and standard error (SE) were calculated for accelerometer-derived PA variables and wear time, and ANOVA with Bonferroni correction (alpha = 0.05/7) were used to compare PA variables between men and women in high OA, intermediate OA, and low OA groupings. For the purposes of a comparison other than between OA groupings, TAC of men and women within each OA grouping were compared to age-matched sex-specific population-referenced TAC percentiles (25th, 50th, and 75th) previously determined from NHANES 2003–2006 [40]. Sensitivity analyses were conducted comparing accelerometer-derived PA variables (activity counts/minute, proportion of wear time spent in MVPA, lifestyle, light, and SB) between high, intermediate, and low OA groupings during traditional working hours (9 am–5 pm) and after work (5–10 pm) using ANOVA with Bonferroni correction (alpha = 0.05/5).
Results
Characteristics of adults by OA groupings
A large number of adults were excluded from the analytic sample because of inclusion criteria. Compared to the analytical sample (n = 1112), those excluded from the study (n = 1792) were significantly younger, had lower wear time, accumulated significantly less activity counts/minute and TAC, spent a lower proportion of time in MVPA, lifestyle, and light, and more time sedentary, were more likely to have less than a high school education, to be non-Hispanic black, female, current smokers, single, and lower income (<25 K). We compared subgroups of excluded participants to identify any specific biases—for instance excluded part-time workers were younger, worked less hours, had less lifestyle PA, accelerometer wear time, and TAC than full-time workers. Some occupational categories ‘personal service occupations’, ‘sales workers, retail and personal’, ‘private household occupations’, and ‘waiters and waitresses’ had more part-time than full-time workers. Excluded participants with less than 4 valid days of accelerometer data [37] were younger, had less accelerometer wear time, and total counts. In an effort to maximize generalizability we decided restrict our analysis to full-time workers with good accelerometer wear time compliance.
There were significant differences in sex, age, race/ethnicity, education, income, and smoking status between OA groupings (Table 2). A greater proportion of those grouped as having high and intermediate OA were men. For example, only 13 % of the high OA group were women, whereas 58 % of the low OA group were women. On average, participants grouped as having low OA were significantly older, more educated, had higher household income, and were not current smokers compared to those who were grouped as having high or intermediate OA. A higher proportion of Mexican Americans worked in high and intermediate OA occupations than in low OA occupations. There were no significant differences in BMI, marital status, or accelerometer wear time (884.93 min/day) between any OA groupings.
Tables 4, 5, 6, 7, 8 and 9 highlight the number of men and women sampled from each occupational category. Several occupational categories were represented exclusively by one sex. ‘Related agricultural, forestry, and fishing (n = 21)’, ‘construction laborers (n = 9)’, ‘other mechanics and repairers (n = 37)’, and ‘vehicle and mobile equipment mechanics and repairers (n = 15)’ were occupational categories with 100 % men; while ‘private household (n = 9)’, ‘records processing (n = 33)’, and ‘secretaries, stenographers, and typists (n = 21)’ were only represented by women. Sixteen of the 40 occupational categories were represented by less than 20 individuals, and seven occupational categories were represented by less than 10 individuals. In the smallest occupational category, ‘laborers, except construction’ there were only data available for three individuals (1 man, 2 women). Because of the small numbers and sex imbalances of certain occupational categories we chose not to run statistical comparisons within or between the 40 occupational categories.
Low, intermediate, and high OA
Mean and standard error (SE) for the six accelerometer-derived variables in rank order for each of the 40 occupational categories are presented in Tables 4, 5, 6, 7, 8 and 9. ‘Secretaries, stenographers, and typists’ had the lowest TAC, and activity counts/minute followed by ‘records processing occupations.’ ‘Related agricultural, forestry, and fishing occupations’ had the highest TAC, activity counts/minute, and the largest proportion of MVPA (8 %). ‘Engineers, architects and scientists’ had the largest proportion of monitored time spent in SB (65 %), and the smallest proportion of time spent in light (23 %) and lifestyle PA (8 %). Conversely, ‘waiters and waitresses’ had the smallest proportion of time spent in SB (40 %), and largest proportion of time spent in light PA (43 %).
Table 3 presents an overall summary of the six accelerometer-derived variables assembled in Tables 4, 5, 6, 7, 8 and 9. Specifically, the 40 occupational categories are ranked in ascending order according to their summary score, and the three accelerometer-determined OA groupings derived from the tertile split of the summary score are labelled. The high, and intermediate OA groupings included 13 occupational categories, while 14 occupational categories were assigned to the low OA grouping. The corresponding rank for each accelerometer-derived variable is presented for each occupational category. ‘Secretaries, stenographers, and typists’ and ‘records processing occupations’ were consistently in the lower ranks for most accelerometer-derived variables, while ‘farm and nursery workers’, ‘other helpers, equipment cleaners, hand packagers, and laborers’, ‘construction laborers’, and ‘related agricultural, forestry, and fishing occupations’ were consistently near the top for most accelerometer-derived variables and were the four highest ranked occupational categories according to the summary score.
Among the three OA groupings most of the individual accelerometer-derived variables aligned closely with the summary scores (Table 3). Scrutinizing the low OA grouping revealed several notable exceptions. For example, some low OA occupational categories (e.g., ‘engineers, architects, and scientists’, ‘technicians and related support occupations’, ‘management related occupations’, ‘executives, administrators, and managers’, ‘protective services’, and ‘writers, artists, entertainers, and athletes’) displayed relatively higher rankings for the proportion of time in MVPA. To be clear, their time in MVPA was higher than what was expected given their relatively lower summary score.
Within each OA grouping men accumulated significantly more TAC, activity counts/minute, and had a greater proportion of time in MVPA than women (Table 10). Within the intermediate OA and low OA groupings, women spent a significantly greater proportion of time in light PA than men. Men grouped in low OA had a significantly greater proportion of time spent in lifestyle PA than women in the same OA grouping. There were no differences in the proportion of time spent in SB or wear time between men and women in any OA grouping. Sensitivity analyses showed significant differences in activity counts/hour, and all activity intensity levels between OA groupings during traditional working hours (9 am–5 pm). The high OA grouping accumulated more activity counts/minute, MVPA, lifestyle, and light PA, and less SB, followed by intermediate and low OA occupations. There were no differences in accelerometer-derived PA and SB variables between OA groupings after work (5–10 pm).
OA groupings compared to age-matched, sex-specific population-referenced TAC percentiles
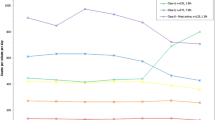
When the PA levels of our sample were compared with a larger sample of U.S. men and women of similar age, men with low OA accumulated TAC slightly below the 50th percentile, while women in low OA had TAC values similar to the 50th percentile (Fig. 1). Men and women in intermediate OA occupations accumulated TAC slightly above the 50th percentile, and men and women in high OA occupations had TAC values above the 50th percentile and close to the 75th percentile compared to sex-and age-matched TAC of U.S. adults.

TAC of men and women by OA category against population-referenced TAC percentiles [21]. TAC total activity counts per day, High OA high occupational activity, Intermediate OA intermediate occupational activity, Low OA low occupational activity. TAC percentiles (25th, 50th and 75th) for men and women 40 years of age determined from NHANES 2003–2006 [21]
Discussion
This study is the first to report observed accelerometer-derived PA and SB variables for a wide variety of occupational categories in U.S. adults. Accelerometry provides an objective measure of movement in everyday life and thus should yield a more valid and reproducible ranking of OA than that achieved earlier by researchers’ best estimates [32]. The information in the paper provides future researchers with detailed measures of the volume and intensity of PA and SB variables that can be compared across the 40 occupational categories based on the 1980 U.S. Census Bureau Classification Coding System. These data also highlight the importance of occupation as a determinant of daily PA and SB.
Previously, occupational categories with indeterminate levels of PA and/or those known to have high variability in PA requirements were considered to be unclassifiable in terms of OA [32]. In fact, more than half (23 of 40) of the occupational categories within NHANES 2003–2004 were considered too ambiguous to classify based on the occupation descriptions of the U.S. Department of Labor [32]. For example firefighters, a specific occupation within the ‘protective services’ category, may be very active when fighting a fire, but the majority of their time may be spent sedentary or in light intensity PA while waiting for a call. Despite the high levels of PA required to be an athlete, they were included in the occupational category ‘writers, artists, entertainers, and athletes’ which was previously categorized as “unclassifiable” due to the assumed lower levels of PA of the other occupations in the category. In our new grouping ‘writers, artists, entertainers, and athletes’ belongs to the low OA grouping, which would suggest that overall number of professional athletes sampled was low. These examples highlight some limitations of relying on job classification as an index of PA [43, 44]. Due to the uncertainty of PA levels of many occupational categories, researchers have predominantly limited their analyses to the occupational categories assumed to have more consistently very high or low levels of OA [12, 21, 45]. The ability to quantify the PA and SB of individuals working in a diverse spectrum of occupational categories with accelerometer data allows for more data-driven grouping into low, intermediate, and high OA. While our tertile approach is arbitrary, it logically splits the occupational categories into three equivalent OA groupings, and avoids having the majority of occupations being considered unclassifiable. Accounting for the variation in PA within each occupational category is still a challenge to overcome, however these data-driven OA groupings may enhance researchers ability to rely on occupational categories as an index of PA, and improve our capability to identify relationships between OA, daily PA and health [46].
In the past relying on occupational categories as a proxy for OA has be useful when gathering information on daily PA of various occupations that involve large amounts of sedentary time or greater amounts of physical labor [32, 46]. The use of objectively measured PA and SB provides data to support the use of occupational categories as a proxy for OA differences. Our study corroborates the utility of the original high and low OA groupings established by King et al. [32]. Only three of the 17 occupational categories previously classified as having high, or low OA were differently categorized using objectively measured PA and SB. ‘Laborers, except construction’ went from high to intermediate OA, ‘material recording, scheduling, and distributing clerks’ went from low to intermediate OA, and ‘motor vehicle operators’ went from low to high OA.
Due to the variety of occupations within some occupational categories PA levels may be quite heterogeneous within an occupational category. Also there is no information regarding the breakdown of all the occupations within each of the 40 occupational categories (i.e., there may have been only one athlete in the ‘writers, artists, entertainers, and athletes’ category). Even within the same occupation variability of PA can be large. For example, cross-country truck drivers spend considerably greater amounts of time sitting compared to local delivery truck drivers who spend a significant amount of time unloading [43]. Additionally, this analysis was not restricted to actual working hours due to the inability to isolate work from non-work time using the data as it was originally acquired. Information regarding regular working hours, shift work or alternative work schedules was not available. Because we were unable to account for variability in occupations within occupational categories, and unable to stratify PA and SB taking place during work or leisure time these limitations could result in non-differential exposure misclassification [47], and limits the ability to accurately interpret these data and ultimately make recommendations about changing behaviors within specific domains.
This study provides benchmark values for accelerometer-derived PA and SB variables, organized by occupation category, which will facilitate comparisons between and across studies using the same classification scheme. Creating tertiles of the summary score from all six accelerometer-derived variables to objectively classify the 40 occupational categories into low OA, intermediate OA, and high OA groupings does have limitations. In some cases, solely focusing on the summary score obscured interesting differences only apparent when closely considering the concurrent rankings of all accelerometer-derived variables between all occupational categories. For example, and consistent with previous research, some low OA occupational categories (e.g., ‘engineers, architects, and scientists’, ‘technicians and related support occupations’, ‘management related occupations’, ‘writers, artists, entertainers, and athletes’, and ‘executives, administrators, and managers’) associated with higher education (>80 % had more than a high school education) and higher income (>70 % earned more than 45K/ year) accumulated relatively higher amounts of MVPA, likely due to increased engagement in leisure time exercise [24, 25, 48]. The higher amount of MVPA relative to the lower summary score in the ‘protective service occupations’ (e.g., firefighters, police and sheriff’s patrol officers, fish and game wardens) was likely due to a combination of increased time spent in vigorous leisure time PA and OA [49]. Because we were unable to separate LTPA from OA, such implications are purely speculative. Although the tertile approach is data-driven, it was possible for two occupations with very similar summary scores to end up in separate OA groupings, for example, ‘motor vehicle operators’ with a summary score of 87 in the high OA group, and ‘supervisors and proprietors, sales occupations’ with a summary score of 89 in the intermediate OA group. Because there was no clear break in the categories, we made an arbitrary split between the 14th and 15th summary scores, despite the small difference in summary score.
In line with previous research, we showed that men were more active (inferred from higher values for TAC, activity counts/minute, and MVPA) than women [37, 40, 50, 51] within the same OA groupings after adjusting for characteristics known to be related to PA. In addition our data highlighted differences in PA of men and women within the same occupational category, and showed obvious differences in the proportion of men and women employed in specific occupational categories. For example, in our sample, only men were employed in many high OA occupational categories, while several low OA occupational categories were 100 % women. Due to gender differences in PA, the proportion of women in an occupational category may affect the results. The proportion of men and women employed as ‘engineers, architects, and scientists’, ‘technicians and related support occupations’, ‘management related occupations’, ‘executives, administrators, and managers’, protective services’, and ‘writers, artists, entertainers, and athletes’ may be another explanation for why these low OA occupational categories had higher than expected MVPA relative to their summary score. These six low OA occupational categories contained 60 % men, while the remaining eight low OA occupational categories comprised only 25 % men.
A number of additional analytical limitations to this analysis must be acknowledged. Operating under the assumption that OA is a major determinant of PA for many adults, the sample was restricted to adults working full-time, therefore the results may not be generalizable to populations employed part-time. Because of numerous exclusion criteria a large proportion of the adult population was excluded from the analysis, therefore the study population may not be entirely representative of the U.S. adult population. Of the 40 occupational categories, 16 were represented by less than 20 individuals. Therefore, the expected accelerometer-derived variables for some occupational categories should be interpreted with caution as they may not reflect national estimates of workers in these categories. We considered only reporting the accelerometer-derived variables for the 24 categories with a sample size greater than 20, as recommended by the NCHS [52]. However, despite these relatively small sample sizes, the majority of accelerometer-derived variables displayed a relative standard error (the standard error as a percent of the measure itself, much like the coefficient of variation) within the range deemed acceptable (<30 %) by the NCHS [42]. Thus, we opted for a more comprehensive presentation of all 40 occupational categories. We clearly indicated when violations to the relative standard error rule occurred and presented the sample size of each occupational category within the tables. Because of sample size limitations we chose to present a more conservative descriptive epidemiology of accelerometer-derived variables rather than conducting statistical comparisons between occupational categories, and men and women. However, showing the number of men and women in each category of the current sample was informative, especially in cases where the whole category was men, or exclusively women. As the number of women entering the work force has grown in the last half century, it would be useful to develop sex-specific estimates for OA in different occupational categories. Unfortunately, the occupational categories for NHANES 2005–2006 were different, so enlargement of the sample by incorporation of multiple waves of NHANES was not possible.
A major strength of this study was the use of accelerometers to objectively measure PA. At the time of data collection, uniaxial accelerometers were the method of choice, and weaknesses related to uniaxial, count-based PA measurement must be acknowledged. Accelerometers do not capture all types of PA, nor do they provide information on the type of PA performed, and their ability to accurately identify time spent in specific intensity categories has been questioned [53–55]. When worn at the waist accelerometers are most sensitive to ambulatory PA, and therefore the additional intensity of carrying loads, or other upper body movements is not captured [37]. This instrument has been validated against measured activity energy expenditure [56, 57], however it has not been validated for capturing the PA patterns characterizing OA in different occupations. The PA patterns characterizing OA (e.g., mostly sitting, and standing, with little walking, engaging in repetitive tasks) differ significantly from LTPA patterns which usually involve dynamic movements that engage large muscle groups resulting in increased whole-body metabolism and cardiac output, and are often emphasized for their the health-promoting capacity [16]. Considering the diverse movement requirements of different occupations (e.g., degree of static work, upper body work, standing, moving, lifting and loading occupations) [16], the observed differences in PA between the occupational categories may be more a reflection of the ambulatory movement captured by the uniaxial waist worn accelerometer than differences in other forms of OA. If carrying loads and upper body movements (e.g., food trays, pitchers/pots for ‘waiters and waitresses’ who had the largest proportion of light PA) were considered, the PA intensity may have been considerably higher.
The movement captured by the accelerometer reflects the accumulation of PA at home, in transit, during leisure time, in addition to time at work [37]. The differences in accelerometer-derived PA and SB variables between OA groupings occurred during traditional work hours (9 am–5 pm). Outside of traditional work hours OA groupings had similar levels of PA and SB. This supports our analytical assumption that the majority of workers were working a traditional day shift, and that the differences in accelerometer-derived PA and SB variables were likely due to OA. However, we must acknowledge our inability to separate PA and SB taking place during work and leisure time, and previous research which indicates that OA and LTPA is profoundly different in varying occupations. Blue collar workers with physically strenuous occupations and frequent overtime work are significantly less likely to engage in LTPA, while white collar workers may engage in greater LTPA, after a sedentary day at work [24, 25, 48].
An additional concern regarding waist worn, uniaxial accelerometers is their inability to accurately differentiate between sitting and standing postures [58–60], which can result in the misclassification of standing-light work, a light intensity PA, as sedentary [61–63]. Some occupations traditionally spend much of the work day in an upright posture, standing and/or moving around in light intensity behaviors (e.g., teachers, cooks, retail, waiters and waitresses). The increased energy expenditure and postural demands of standing compared with sitting may be an important distinction to consider when evaluating health outcomes [60, 64]. For assessing and differentiating between sitting and standing postures between different occupations, a thigh-mounted accelerometer like the ActivPAL monitor [65] or Actigraph [66], or triaxial accelerometer (ActiGraph GT3X+) at the thigh or hip may provide greater accuracy [67].
Conclusions
Objectively measured PA allowed for a more precise estimate of the amount of PA and SB associated with different occupational categories, and made it possible to systematically classify 40 different occupational categories into three distinct OA groupings. An individual’s occupational category appeared to have a great influence on daily PA and SB. This information provides new opportunities to explore the relationship between OA and health outcomes. It is also important for the design and implementation of programs and policies to improve health, productivity, and reduce work related injury of the employed population. Future occupational epidemiological research is needed to understand how variations in OA, LTPA, transportation, and household PA interact to influence engagement in beneficial amounts of daily PA, and influence health [17]. In addition, future research should continue to refine recommendations of maximal levels of OA, because strenuous OA can have health-detrimental impacts such as musculoskeletal disorders, decreased work ability and absence due to work related sickness or injury [68]. The results reported here highlight the scarcity of the data available for certain occupational categories to conduct and inform such studies. A larger sampling of underrepresented occupational categories, and a wide range of unique occupational categories would benefit future research concerned with the impact of occupation on PA and SB. The observed values presented in this paper are an important resource that should be expanded and refined as future changes occur in OA and as occupational categorization systems evolve.
Abbreviations
- OA:
-
Occupational activity
- PA:
-
Physical activity
- SB:
-
Sedentary behavior
- NHANES:
-
National Health and Nutrition Examination Survey
- TAC:
-
Total activity counts/day
- MVPA:
-
Moderate-to-vigorous physical activity
- NCHS:
-
National Center for Health Statistics
- SE:
-
Standard error
References
Blair SN, Morris JN. Healthy hearts–and the universal benefits of being physically active: physical activity and health. Ann Epidemiol. 2009;19(4):253–6.
Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39(8):1423–34.
Leitzmann MF, Park Y. Physical activity recommendations and decreased risk of mortality. Arch Intern Med. 2007;167(22):2453–60.
Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008. 2008.
Owen N, Sugiyama T, Eakin EE, Gardiner PA, Tremblay MS, Sallis JF. Adults’ sedentary behavior determinants and interventions. Am J Prev Med. 2011;41(2):189–96.
U. S. Department of Health and Human Services. Physical activity guidelines for Americans (Report). 2008. p. 1–4.
Barengo NC, Hu G, Lakka TA, Pekkarinen H, Nissinen A, Tuomilehto J. Low physical activity as a predictor for total and cardiovascular disease mortality in middle-aged men and women in Finland. Eur Heart J. 2004;25(24):2204–11.
Holtermann A, Mortensen OS, Burr H, Sogaard K, Gyntelberg F, Suadicani P. The interplay between physical activity at work and during leisure time–risk of ischemic heart disease and all-cause mortality in middle-aged Caucasian men. Scand J Work Environ Health. 2009;35(6):466–74.
Krause N, Brand RJ, Kaplan GA, Kauhanen J, Malla S, Tuomainen TP, et al. Occupational physical activity, energy expenditure and 11-year progression of carotid atherosclerosis. Scand J Work Environ Health. 2007;33(6):405–24.
Paffenbarger RS, Hale WE. Work activity and coronary heart mortality. N Engl J Med. 1975;192:545–50.
Choi B, Schnall PL, Yang H, Dobson M, Landsbergis P, Israel L, et al. Sedentary work, low physical job demand, and obesity in US workers. Am J Ind Med. 2010;53(11):1088–101.
Steeves JA, Bassett Jr DR, Thompson DL, Fitzhugh EC. Relationships of occupational and non-occupational physical activity to abdominal obesity. Int J Obes (Lond). 2012;36(1):100–6.
Hammermeister J, Page RM, Dolny D, Burnham T. Occupational physical activity as an indicator of health and fitness. Percept Mot Skills. 2001;92(1):121–7.
Brown WJ, Miller YD, Miller R. Sitting time and work patterns as indicators of overweight and obesity in Australian adults. Int J Obes Relat Metab Disord. 2003;27(11):1340–6.
Mummery WK, Schofield GM, Steele R, Eakin EG, Brown WJ. Occupational sitting time and overweight and obesity in Australian workers. Am J Prev Med. 2005;29(2):91–7.
Holtermann A, Hansen JV, Burr H, Sogaard K, Sjogaard G. The health paradox of occupational and leisure-time physical activity. Br J Sports Med. 2012;46(4):291–5.
Krause N. Physical activity and cardiovascular mortality–disentangling the roles of work, fitness, and leisure. Scand J Work Environ Health. 2010;36(5):349–55.
Holtermann A, Mortensen OS, Burr H, Sogaard K, Gyntelberg F, Suadicani P. Physical demands at work, physical fitness, and 30-year ischaemic heart disease and all-cause mortality in the Copenhagen Male Study. Scand J Work Environ Health. 2010;36(5):357–65.
Andersen JH, Haahr JP, Frost P. Risk factors for more severe regional musculoskeletal symptoms: a two-year prospective study of a general working population. Arthritis Rheum. 2007;56(4):1355–64.
Parry S, Straker L. The contribution of office work to sedentary behaviour associated risk. BMC Public Health. 2013;13:296.
Van Domelen DR, Koster A, Caserotti P, Brychta RJ, Chen KY, McClain JJ, et al. Employment and physical activity in the U.S. Am J Prev Med. 2011;41(2):136–45.
Church TS, Thomas DM, Tudor-Locke C, Katzmarzyk PT, Earnest CP, Rodarte RQ, et al. Trends over 5 decades in U.S. occupation-related physical activity and their associations with obesity. PLoS ONE. 2011;6(5):e 19657.
Morris JN, Crawford MD. Coronary heart disease and physical activity of work. Br Med J. 1958;2(5111):1485–96.
Salmon J, Owen N, Bauman A, Schmitz MK, Booth M. Leisure-time, occupational, and household physical activity among professional, skilled, and less-skilled workers and homemakers. Prev Med. 2000;30(3):191–9.
Burton NW, Turrell G. Occupation, hours worked, and leisure-time physical activity. Prev Med. 2000;31:673–81.
Sluiter JK. High-demand jobs: age-related diversity in work ability? Appl Ergon. 2006;37(4):429–40.
Sluiter JK, Frings-Dresen MH, van der Beek AJ, Meijman TF, Heisterkamp SH. Neuroendocrine reactivity and recovery from work with different physical and mental demands. Scand J Work Environ Health. 2000;26(4):306–16.
Tudor-Locke C, Ainsworth BE, Washington TL, Troiano RP. Assigning metabolic equivalent values to the 2002 census occupational classification system. JPAH. 2011;8:581–6.
Hu G, Tuomilehto J, Borodulin K, Jousilahti P. The joint associations of occupational, commuting, and leisure-time physical activity, and the Framingham risk score on the 10-year risk of coronary heart disease. Eur Heart J. 2007;28(4):492–8.
Macera CA, Ham SA, Yore MM, Jones DA, Ainsworth BE, Kimsey CD, et al. Prevalence of physical activity in the United States: behavioral risk factor surveillance system, 2001. Prev Chronic Dis. 2005;2(2):A17.
U. S. Bureau of the Census. Alphabetical index of occupations and industries (Report). 1980.
King GA, Fitzhugh EC, Bassett Jr DR, McLaughlin JE, Strath SJ, Swartz AM, et al. Relationship of leisure-time physical activity and occupational activity to the prevalence of obesity. Int J Obes Relat Metab Disord. 2001;25(5):606–12.
Brownson RC, Boehmer TK, Luke DA. Declining rates of physical activity in the United States: what are the contributors? Annu Rev Public Health. 2005;26:421–43.
Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey (NHANES) Data In: (NCHS) National Center for Health Statistics, 2003–2006.
Bureau of Labor Statistics, U. S. Department of Labor. Labor force characteristics. Washington, DC: U.S. Bureau of Labor Statistics, Division of Labor Force Statistics; 2014.
Steeves JA, Murphy RA, Zipunnikov V, Strath SJ, Harris TB. Women workers and women at home are equally inactive: NHANES 2003–2006. Med Sci Sports Exerc. 2014.
Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40(1):181–8.
Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey, Examination Components Manual.
Mâsse LC, Fuemmeler BF, Anderson CB, Matthews CE, Trost SG, Catellier DJ, et al. Accelerometer data reduction: a comparison of four reduction algorithms on select outcome variables. Med Sci Sports Exerc. 2005;37(11S):S544–54.
Wolff DL, Fitzhugh EC, Bassett DR, Churilla JR. Waist-worn actigraphy: population-referenced percentiles for total activity counts in U.S. adults. J Phys Act Health. 2014.
Hagstromer M, Troiano RP, Sjostrom M, Berrigan D. Levels and patterns of objectively assessed physical activity—a comparison between Sweden and the U.S. Am J Epidemiol. 2010;171(10):1055–64.
VanEenwyk J, Macdonald SC. Guidelines for working with small numbers. 2012.
LaPorte RE, Montoye HJ, Caspersen CJ. Assessment of physical activity in epidemiologic research: problems and prospects. Public Health Rep. 1985;100(2):131–46.
Vaz M, Bharathi AV. How sedentary are people in “sedentary” occupations? The physical activity of teachers in urban South India. Occup Med (Lond). 2004;54(6):369–72.
Brownson RC, Eyler AA, King AC, Brown DR, Shyu YL, Sallis JF. Patterns and correlates of physical activity among US women 40 years and older. Am J Public Health. 2000;90:264–70.
Kruger J, Yore MM, Ainsworth BE, Macera CA. Is participation in occupational physical activity associated with lifestyle physical activity levels? J Occup Environ Med. 2006;48(11):1143–8.
Kauppinen TP, Mutanen PO, Seitsamo JT. Magnitude of misclassification bias when using a job-exposure matrix. Scand J Work Environ Health. 1992;18(2):105–12.
Schneider S, Becker S. Prevalence of physical activity among the working population and correlation with work-related factors: results from the first German National Health Survey. J Occup Health. 2005;47(5):414–23.
Bonauto DK, Lu D, Fan ZJ. Obesity prevalence by occupation in Washington State, behavioral risk factor surveillance system. Prev Chronic Dis. 2014;11:130219.
Hawkins MS, Storti KL, Richardson CR, King WC, Strath SJ SJ, Holleman RG, et al. Objectively measured physical activity of USA adults by sex, age, and racial/ethnic groups: a cross-sectional study. Int J Behav Nutr Phys Act. 2009;6:31.
Van Domelen DR, Caserotti P, Brychta RJ, Harris TB, Patel KV, Chen KY, et al. Is there a sex difference in accelerometer counts during walking in older adults? J Phys Act Health. 2014;11(3):626–37.
New York State Department of Health. Rates based on small numbers-statistics teaching tools. 1999.
Schrack JA, Zipunnikov V, Goldsmith J, Bai J, Simonsick EM, Crainiceanu C, et al. Assessing the “physical cliff”: detailed quantification of age-related differences in daily patterns of physical activity. J Gerontol A Biol Sci Med Sci. 2014;69(8):973–9.
Crouter SE, DellaValle DM, Haas JD, Frongillo EA, Bassett DR. Validity of ActiGraph 2-regression model and Matthews and NHANES and cut-points for assessing free-living physical activity. J Phys Act Health. 2013;10:504–14.
Strath SJ, Bassett JDR, Swartz AM. Comparison of MTI accelerometer cut-points for predicting time spent in physical activity. Int J Sports Med. 2003;24(4):298–303.
Brage S, Wedderkopp N, Franks PW, Andersen LB, Froberg K. Reexamination of validity and reliability of the CSA monitor in walking and running. Med Sci Sports Exerc. 2003;35:1447–54.
Freedson PS, Melanson E, Sirard J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med Sci Sports Exerc. 1998;30(5):777–81.
Kozey-Keadle S, Libertine A, Lyden K, Staudenmayer J, Freedson PS. Validation of wearable monitors for assessing sedentary behavior. Med Sci Sports Exerc. 2011;43(8):1561–7.
McMahon GC, Brychta RJ, Chen KY. Validation of the Actigraph (GT3X) inclinometer function. American College of Sports Medicine Annual Meeting. 2010;42(5):489.
Oliver M, Schofield GM, Badland HM, Shepherd J. Utility of accelerometer thresholds for classifying sitting in office workers. Prev Med. 2010;51(5):357–60.
Kerr J, Marshall SJ, Godbole S, Chen J, Legge A, Doherty AR, et al. Using the SenseCam to improve classifications of sedentary behavior in free-living settings. Am J Prev Med. 2013;44(3):290–6.
Rowlands AV. Accelerometer assessment of physical activity in children: an update. Pediatr Exerc Sci. 2007;19(3):252–66.
Trost SG, Loprinzi PD, Moore R, Pfeiffer KA. Comparison of accelerometer cut points for predicting activity intensity in youth. Med Sci Sports Exerc. 2011;43(7):1360–8.
Hamilton MT, Hamilton DG, Zderic TW. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes. 2007;56(11):2655–67.
Aminian S, Hinckson EA. Examining the validity of the ActivPAL monitor in measuring posture and ambulatory movement in children. Int J Behav Nutr Phys Act. 2012;9:119-5868-9-119.
Steeves J, Bowles H, McClain J, Dodd K, Brychta R, Wang J, et al. Ability of thigh-worn actigraph and activPAL monitors to classify posture and motion. Med Sci Sports Exerc. 2014;47(5):952–9.
Skotte J, Korshøj M, Kristiansen J, Hanisch C, Holtermann A. Detection of physical activity types using triaxial accelerometers. J Phys Act Health. 2014;11(1):76–84.
Holtermann A, Jorgensen MB, Gram B, Christensen JR, Faber A, Overgaard K, et al. Worksite interventions for preventing physical deterioration among employees in job-groups with high physical work demands: background, design and conceptual model of FINALE. BMC Public Health. 2010;10:120.
Acknowledgements
This work was supported by the Intramural Research Program of the National Institute on Aging, National Institutes of Health. The authors acknowledge the editorial assistance of the NIH Fellows Editorial Board, National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
JAS is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analyses. JAS, RAM, ECF, CTL, GAK, and TBH, contributed to conception and design of the study. JAS performed statistical analyses. JAS wrote the initial draft of the paper, and all authors contributed to interpretation of the data and the writing of the paper. All authors read and approved the final paper.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Steeves, J.A., Tudor-Locke, C., Murphy, R.A. et al. Classification of occupational activity categories using accelerometry: NHANES 2003–2004. Int J Behav Nutr Phys Act 12, 89 (2015). https://doi.org/10.1186/s12966-015-0235-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-015-0235-z