
Abstract
Background
Systems science offers methods for designing population health interventions while implementation science provides specific guidance for successful implementation. Integrating systems and implementation science may strengthen implementation and enhance and sustain systemic change to achieve system-level outcomes. Little is known about the extent to which these two approaches have been integrated to date. This review aimed to identify and synthesise the peer-reviewed literature that has reported the combined use of systems thinking approaches and implementation science constructs (within the same study), to deliver population health interventions.
Methods
A systematic literature search of peer-reviewed original research was conducted across six databases from 2009 to 2021. Journal manuscripts were included if they: (1) reported on a population health study conducted in a community, (2) reported the use of a systems method in the design of the intervention, and (3) used an implementation science theory, framework or model in the delivery of the intervention. Data extracted related to the specific systems methods and definitions and implementation science constructs used. The Mixed Methods Appraisal Tool (MMAT) was used to assess study quality.
Results
Of the 9086 manuscripts returned, 320 manuscripts were included for full-text review. Of these, 17 manuscripts that reported on 14 studies were included in the final extraction. The most frequently reported systems methods were a ‘whole of community systems approach’ (n = 4/14) and ‘community-based system dynamics’ (n = 2/14). Nineteen different implementation science theories, frameworks and models were used for intervention delivery, with RE-AIM being the only framework used in more than one study.
Conclusion
There are few published peer-reviewed studies using systems thinking and implementation science for designing and delivering population health interventions. An exploration of synergies is worthwhile to operationalise alignment and improve implementation of systems thinking approaches.
Review protocol registration PROSPERO CRD42021250419.
Similar content being viewed by others

Contribution to the literature
-
Research has called for the adoption of systems approaches to tackle complex problems, however there is limited understanding of ‘how to’ implement solutions designed using systems science.
-
Multiple studies have reported the use of systems methods in the design of interventions, but few have yet incorporated implementation science into the delivery of the intervention.
-
Although we found some scientific evidence of interventions combining both implementation science and systems science, there was no clear guidance on the role implementation science could play and how these two sciences can best be utilised together.
-
These findings contribute to recognized gaps in the literature, including the potential of implementation science to contribute significantly to the implementation of systems approaches to addressing complex problems.
Background
Non-communicable diseases (NCDs) are responsible for almost 70% of all deaths worldwide [1]. Many of these deaths are preventable if causal modifiable risk factors, such as tobacco use, physical inactivity and unhealthy diets were addressed [2]. Relationships between drivers for NCDs (e.g. individual, environmental, societal, political etc.) are complex and dynamic, leading to calls for the adoption of a systems thinking approach [3, 4]. Systems thinking approaches extend socioecological model (SEM) approaches by promoting work across multiple levels of the SEM and actively engaging feedback loops, time delays and seeking effective intervention points [5].
Systems science is a broad field of study that incorporates methodologies with a common goal of understanding complexity [6]. Properties of complex systems include emergence, which is the collective behaviours of the system, outcomes that would not be produced by individual components alone [7]. Complex systems are also adaptive and change behaviour in response to their current environment, therefore changes to a system are likely to create further adaptive responses from within the system [8]. Systems utilise feedback, this circular causality leads to multiple elements within a system impacting others in a circular way, causing self-reinforcing or self-correcting system behaviours [8]. Therefore when working with systems, an emphasis is placed on the ‘whole’ and the importance interactions between components is observed and managed where possible [9, 10]. Many systems methods (e.g. stock and flow diagram, causal loop diagram, systems dynamics modelling etc.) [6], facilitate this enhanced understanding of systems components and their interrelationships, and some methods also assist in the identification of solutions [11] and where resources are best placed to facilitate systems change [12,13,14].
Systems thinking approaches are increasingly being used in population health, particularly in community health and wellbeing [10, 15]. These efforts have targeted outcomes including determinants of obesity [16], initiatives related to school health [17], fruit and vegetable intake in children [18], policy options for tobacco control [19], and mental health [20]. There are over 25 different systems methods that may be relevant to population health interventions [21, 22]. A recent review of system dynamics and agent-based models describes the expansion of modelling into population health over the last 10 years [23], but only four of these models mentioned the term ‘implementation’, and, in each case, this related to policy implementation [23]. There is emerging recognition of the potential of systems-oriented implementation research [24].
Implementation science, as the study of methods to promote the systematic uptake of research into practice [27], has potential to provide guidance to the implementation of systems approaches [25, 28], through theoretical constructs that provide into successful implementation [27]. Historically, an implementation science ‘evidence to practice’ journey has been depicted as a linear process; however this does not align with the theory and practice of systems approaches to address complex problems [29]. To enhance the alignment between implementation science and systems science, the dynamic properties inherent within complex systems need to be considered [29]. Some implementation science theories, frameworks and models (TFMs) may more easily facilitate such adaptation. Overall TFMs have three broad aims: to describe and/or guide the process of translating research into practice; to understand the determinants that influence implementation; and to evaluate implementation outcomes [27]. A systems intervention, like any intervention, may require one or more types of these TFMs to guide the evidence to full implementation.
Within implementation science, over 150 TFMs exist, with less than a quarter being utilised within ‘system’ change interventions [28]. Historically, an implementation science ‘evidence to practice’ journey has been depicted as a linear process, however this does not align with the theory and practice of systems approaches to address complex problems [29]. To enhance the alignment between implementation science and systems science, the dynamic properties inherent within complex systems need to be considered [29]. The potential for combining the two sciences of implementation and systems has previously been identified [30]. Northridge [30] sought to enhance implementation science through the addition of best principles from systems science, e.g. problem modelling, important elements vs quantifiable elements, boundaries and a multi-component approach. Some TFMs may more easily facilitate such adaptation. Overall TFMs have three broad aims: to describe and/or guide the process of translating research into practice (process frameworks); to understand the determinants that influence implementation (determinants frameworks); and to evaluate implementation outcomes (evaluation frameworks) [26]. A systems intervention, like any intervention, may require one or more types of frameworks to guide the evidence to full implementation.
Interventions have reported a disconnect between systems thinking and implementation science in practice. Gerritsen reported on the use of Group Model Building (a method within community-based system dynamics) [31] to promote fruit and vegetable consumption in a multi-cultural low-income community in West Auckland, New Zealand. GMB helped the community identify community-led (e.g., bottom up) actions for implementation, but did not report on how that implementation would occur [18]. Gerritsen et al. have reported that more work needs to be done to ensure that the implementation aspects are given due consideration in the design phase of GMB research [32]. This difficulty in implementing interventions designed using various systems methods has been echoed by several authors [33, 34]. The Lancet Commission on Obesity noted that poor implementation limits the effectiveness of community interventions, ‘and a greater application of implementation science might help overcome these barriers’ [4].
This review aimed to identify and synthesise the peer-reviewed literature that has reported the combined use of systems thinking approaches and implementation science constructs within the same study, to deliver population health interventions. The purpose was to inform enhanced intervention planning and research through combining the strengths of both implementation and systems science together in real-world applications. This review asks: What systems thinking and implementation science approaches have been used in combination to deliver population health interventions?
Methods
This review was prospectively registered with PROSPERO (CRD42021250419) and follows the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [35].
Search strategy
A systematic search was conducted of the online databases of Ovid Medline, Embase, Cochrane Central; and within the EBSCO Host platform: ERIC, PsycInfo and CINAHL for peer-reviewed studies published in English. The search included articles from 1 January 2009 to date of search–15 March 2021. The year 2009 was chosen as the starting point to align with the initial work of the intervention-level framework [36], the first published attempt to operationalise the systems science work by Donella Meadows on places to act in a system for public health interventions [13]. A research librarian assisted with the development, testing and subsequent translation of the search terms across the multiple databases used. Search terms explored concepts of: health promotion, obesity, population health, community AND systems science or complexity terms AND implementation science terminology AND frameworks, models or approaches. The full search terms can be found in Additional file 1.
Studies were included in this review if they were published in English, and the:
-
1.
study reported on primary or secondary prevention specifically related to the uptake, adoption or implementation of a health promotion intervention, innovation or initiative or evidence-based practice, process, policy (hereafter ‘intervention’) related to healthy eating, physical activity, tobacco control, alcohol and other drugs, or mental health; and
-
2.
intervention took place in one or more community settings or whole of community: e.g. school, workplace, sports club, community health or other; and
-
3.
manuscript explicitly stated that the study used a systems thinking approach; and
-
4.
manuscript described the implementation of an intervention either through an explicit implementation science framework, model or theory; or via an author’s own implementation plan or theory.
In the reporting of results, the terms ‘intervention’, ‘innovation’, ‘initiative’ or ‘evidence-based practice’ are collectively referred to as ‘interventions’.
Studies were excluded if the study:
-
1.
related to ‘treatment’ of a pre-existing medical condition that is not generally considered preventable; or
-
2.
was conducted in controlled settings, e.g., prisons or hospitals.
Study selection
All titles and abstracts were screened twice. One author (JW) screened all titles and abstracts. The second screening was shared between co-authors (PF, KB, TBR, EM, PL, CS, CB) and discrepancies on inclusion were resolved by CB. All full text articles were screened twice. JW screened all full texts and the second screening was shared between co-authors (PF, KB, EM, PL, CS). Conflicts were resolved by discussion with the two reviewers. Where agreement was not reached (n = 2), CB resolved outstanding conflicts.
Data extraction
Data extraction on the remaining 14 studies (17 manuscripts) was conducted by one author (JW) with the second review shared between co-authors (MB, TBR, KB, PF, PL, CS). PF and JW conducted consensus where disagreement arose between JW and the second data extractor.
The data extraction template collated data on the use of systems science in the design of the study and on the use of implementation science in the implementation of the study as reported by the author of each manuscript. Data extracted included the public health issue addressed, the use of systems terminology, definitions and methods used, study design, and specific implementation science TFMs applied. (Additional file 2).
Quality appraisal
The Mixed Methods Assessment Tool (MMAT) [37] was applied to all included manuscripts by two co-authors (JW (all), PF, MB, KB, CS, PL, TBR). MMAT was deemed suitable due to its versatility in appraising varying study designs, including qualitative, quantitative and mixed methods. All included studies met the two screening questions of MMAT which are: 1. Are there clear research questions? and 2. Do the collected data allow to address the research questions?, and then were appraised according to study design criteria. Unlike other quality appraisal tools, the MMAT discourages the use of an overall score (Additional file 3).
Results
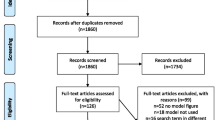
The search returned 9086 manuscripts, of which 826 were duplicates (Fig. 1). Of the remaining 8260 manuscripts, 7940 were excluded based on inclusion/exclusion criteria. Full-text review of the remaining 320 manuscripts meant 303 were excluded, leaving 17 manuscripts. The 17 manuscripts reported on 14 studies. Three studies were described in both a design manuscript and an implementation manuscript which were combined to ascertain the systems and implementation science methods utilised in the studies [38].

PRISMA diagram
Of 14 included studies, three studies were conducted in Australia, four studies in the United States, three studies in the United Kingdom, and one study each of Canada, Austria, Ghana and Mexico, and New Zealand. Of the included studies, 30% reported an intervention duration of two years or less, 50% reported between three- and five-years duration, and 20% reported on studies that lasted six years or more. Thirty percent (30%) of studies aimed to promote health in schools, 30% to prevent childhood obesity, 20% to prevent chronic diseases, and others aimed to promote breastfeeding and food security, general community health and adaptation of evidence-based health programs. Most studies (60%) targeted children (0 to 18 years), 20% targeted all ages, and one study targeted mothers who wished to breastfeed. In terms of study design, 65% utilised mixed methods and 35% were qualitative studies.
Table 1 provides a summary of the studies included in this review, the first author, title, date of publication, country within which the study was conducted, intervention duration, issue addressed, target population and study design.
The term ‘systems’ was used loosely across the studies (Table 2) which made it difficult to describe what systems approaches looked like in practice. Two studies reported on a multi-component, multi-setting intervention (The Scope Study) grounded on a systems approach [40, 41]. Four explicitly noted the importance of interconnections and relationships within the system under study [43, 44, 54, 55] for example, ….. Related terms were also used loosely. For example, three studies used ‘complexity’ to describe their systems approach [46,47,48]. Complexity was described as a self-organising system whose ‘whole is not simply a sum of its parts’ (48p.138), or a need to understand the causal mechanisms and impact pathways of policies and programmes [46] or more generally as ‘complex adaptive systems that help to explain particular problematic situations and identify ways in which they might be improved’ ([47], p. 2).
Consequently, few studies reported using specific systems methods. Three studies reported using community-based system dynamics and group model building [17, 39, 42]. Others were more generic, referring to a systems approach to strengthening community leadership [49], a community-based systems approach with an emphasis on capacity building [50], and a whole of community systems approach [47]. The Scope Study described their multi-component intervention as a ‘modest and early effort’ to incorporate systems approaches within obesity prevention [40, 41]. Contextually, some studies operated at a broad whole of community systems level [39, 47], while others considered the classroom within a school as a ‘system’ [17, 48].
A broad spread of implementation TFMs were used in the studies. Overall included studies used 11 process frameworks, 5 evaluation frameworks and 1 determinants framework (these do not add to 14 because some studies used multiple frameworks). The RE-AIM (reach, effectiveness, adoption, implementation, maintenance) evaluation framework was used in two studies [40, 47]. One of these studies adapted RE-AIM, to include reach, engagement, facilitation, resources, adaptation, mobilisation, and exchange, and re-named to RE-FRAME [40, 41]. One study paired RE-FRAME with the Knowledge-to-Action framework [40, 41]. A different study paired The Plan-Do-Study-Act with a strategy mapping exercise [54]. Other authors used frameworks developed from peak bodies, such as the Health Promoting Schools’ Framework [56], and the Building Blocks for a Strong Health System [57]. One author described a guide for implementation of a systems approach, where local communities developed their own independent methods of implementation [53]. Three of the 14 studies combined two TFMs to guide different stages of implementation. There was no single implementation science framework or set of TFMs favoured to guide the implementation of interventions designed using systems science.
Where authors described the use of both systems and implementation science constructs, these were used in collaboration, systems science was used in the design of the study, implementation science was used to guide real-world implementation of the designed study.
Discussion
This systematic review identified 14 studies (17 manuscripts) that used a combination of systems thinking approaches and implementation science TFMs to design and deliver health promotion interventions. There was no consistency in the definition of systems science, or the systems methods applied in the studies and a broad spread of TFMs was reported. CBSD was the only systems method used in more than one study [17, 39] and RE-AIM the only TFM used in more than one study, albeit in a substantially modified form in one of these two studies [40, 41, 47].
Braithwaite, in a 2018 opinion piece, stated that “the two sciences of complexity and implementation need not be mutually exclusive, though they have been largely seen and treated as such” ([29], p. 6). Our review confirms this remains the case, and aligns with the call for more systematic reporting of intervention studies that utilise systems approaches [62]. Our findings also support opportunities to build on and strengthen existing theoretical approaches, rather than invent new and untested frameworks [63]. Where Northridge [30] sought to enhance implementation science through the addition of best principles from systems science, our review sought to identify insights from published literature on ways to improve the implementation of systems science approaches to prevention through the incorporation of implementation science TFMs.
A previous review of TFMs used in prevention and/or management of cancer and other chronic diseases classified 159 TFMs against the socio-ecological model (SEM) of health: individual, organisational, community and system [28]. Of these, only 17% (n = 27) were deemed to impact the systems level of the SEM, although the term ‘system’ was not defined in the review. Highly cited implementation science TFMs were included such as Social Cognitive Theory [64], Social Leaning Theory [65], Transtheoretical Model of Behaviour Change [66], PRECEDE-PROCEED [67] and Plan-Do-Study-Act [68]. Other TFMs were also included that were less well known or were specifically designed to fit an intervention. Of these, the Plan-Do-Study-Act was the only framework that also appeared in both the SEM review [28] and our review. This limited overlap is likely due to the evolution of systems science, with earlier iterations of the SEM referring to this outer layer as ‘policy’ or ‘social’, rather than ‘systems’. Additionally, most TFMs have historically been applied to either individual behaviour change programs or settings [28], leaving it unclear which TFMs are best suited to a systems approach for community-based prevention intervention.
Many of the included manuscripts did not clearly define ‘systems’ nor clearly articulate the system method used in the study. This observation aligns with a systematic review of whole systems approaches to complex public health problems that found few programs had utilised systems approaches in the study design, implementation and evaluation; and rarely conceptualised implementation from a systems perspective [70]. We concur with Foster-Fishman that systems change requires adopting systems beyond a general definition and adopting a change framework is critical to guide true systems change systemically, rather than within a specific part of the system. For example, there remains tension that ‘policy’ can be misinterpreted as a systems approach, when policy alone may impact only one area of the system and should usually be partnered with other systemic actions [69], such as appropriate resourcing, enabling infrastructure, appropriate skills and knowledge. Without such wrap-around support, a policy is unlikely to have the reach required for a whole of system change. Inadequate framing of ‘systems’ may complicate the choice of appropriate implementation science guidance.
When implementing systems interventions, implementation requires more than just effectiveness planning, but also the anticipation of, and engagement with, a range of contexts, stakeholders and potential consequences [29]. Northridge [30] provided insights from systems science that could enhance implementation science, concepts such as, e.g. problem modelling, the inclusion of important elements rather than quantifiable elements, boundary identification and a multi-component approach. A positive signpost for future integration of the fields of implementation science and systems science is reported modification of TFMs to enhance their applications to complex intervention and systems approaches. In a recent 20-year review of RE-AIM, Glasgow et al. identified one of the future directions for the RE-AIM framework was to incorporate system concepts such as unintended consequences [71]. Such extension of a widely used framework to overtly embrace systems concepts is encouraging. Other wholistic frameworks are constantly evolving to specifically address systems change, such as the Active Implementation Frameworks developed by Fixsen and colleagues [72]. This overarching framework aligns with the interactive nature of systems through its non-linear approach to implementation and inclusion of improvement cycles. These advances in implementation science articulate promise for enhanced guidance for the implementation of systems interventions, aligns with multiple calls to integrate implementation and system science approaches [32, 53], and acknowledges the potential within the field of implementation science as noted in the Lancet’s Commission on Obesity [4].
Future research
Future studies that utilise systems thinking approaches should more clearly define terminology and specify the systems method employed within the study. Recent innovative trial designs such as stepped wedge designs [73] and hybrid Type II designs [74] may assist in the combination of systems and implementation sciences by enabling efficacy testing of both the systems intervention and the implementation strategies. Future trials, using various combinations of systems thinking and implementation science methods, would assist in identifying a ‘preferred’ combination of these approaches for population health prevention interventions.
Although GMB and RE-AIM were the most identified methods and frameworks within this review, there were too few studies to recommend these methods either alone or in combination to close this gap. Instead, there exists great potential for future research to interrogate the use of clearly defined systems methodologies and implementation science theoretical approaches to enable cyclical implementation. Such a combination has potential to optimise the intrinsic overlap in these two scientific disciplines and identify aligned theories and practice.
Strengths and limitations
To our knowledge, this is the first systematic review to explore the use of an integrated systems and implementation science approach in public health prevention intervention design and delivery. This review demonstrates there is little practical guidance to date on how best to implement systems approaches for population health. The review included all manuscripts that identified the use of systems—therefore avoiding bias for any preferred systems methodology and including studies where systems thinking was emerging. Similarly, we defined implementation science theoretical approaches broadly to maximise the capture of all manuscripts using any theoretically informed approach to implementation.
Heterogeneity of definitions of both systems science and implementation science means it was difficult to draw conclusions from existing manuscripts as to what the ‘best’ combination of these sciences might be. We limited our review to peer-reviewed literature therefore case studies may exist in the grey literature that were not captured by this review.
The heterogeneity of ‘systems’ terminology means it is possible that some work that draws from principles of systems thinking without using explicit terminology may have not been included in our review. Consequently we were unable to obtain practical guidance on how to apply these dual approaches of systems and implementation sciences.
Conclusions
To date there is limited alignment between systems thinking and implementation science approaches in the design and delivery of public health prevention interventions. Based on this review, we are unable to recommend the most promising combination of systems thinking methods and implementation science TFMs as the combination of these fields remains underdeveloped. We join the call for consistency of language, definition and guidance on the use and reporting of an integrated systems and implementation science approach for public health prevention interventions.
Availability of data and materials
All search terms are provided in Additional information, for any further information please contact the corresponding author.
References
Habib SH, Saha S. Burden of non-communicable disease: global overview. Diabetes Metab Syndr. 2010;4(1):41–7.
Murray CJL, Abbafati C, Abbas KM, Abbasi M, Abbasi-Kangevari M, Abd-Allah F, et al. Five insights from the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1135–59.
Brown T, Moore THM, Hooper L, Gao Y, Zayegh A, Ijaz S, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev. 2019(7). https://doi.org/10.1002/14651858.CD001871.pub4
Swinburn BA, Kraak VI, Allender S, Atkins VJ, Baker PI, Bogard JR, et al. The global syndemic of obesity, undernutrition, and climate change: The Lancet Commission report. Lancet. 2019;393(10173):791–846.
Bozsik F, Shook R, Wilson E, Carlson J, Markenson D, Meissen-Sebelius E, et al. Characterization of a regional childhood obesity prevention and treatment system. Child Obes. 2021;17(4):291–7.
Sterman J. System dynamics: systems thinking and modeling for a complex world. 2002.
Frank M. Systems thinking: foundation, uses and challenges. New York: Nova Science Publishers, Inc; 2016.
Haines SG. Systems thinking and learning: from chaos and complexity to elegant simplicity. Annual-San Diego-Pfeiffer Company. 2002;2:173–92.
Rutter H, Savona N, Glonti K, Bibby J, Cummins S, Finegood DT, et al. The need for a complex systems model of evidence for public health. Lancet. 2017;390(10112):2602–4.
Savigny Dd, Adam T, Alliance for Health P, Systems R, World Health O. Systems thinking for health systems strengthening / edited by Don de Savigny and Taghreed Adam. Geneva: World Health Organization; 2009.
Stroh DP. Systems thinking for social change : a practical guide to solving complex problems, avoiding unintended consequences, and achieving lasting results. White River Junction, Vermont, United States: Chelsea Green Publishing; 2015.
Bolton KA, Whelan J, Fraser P, Bell C, Allender S, Brown AD. The Public Health 12 framework: interpreting the “Meadows 12 places to act in a system” for use in public health. Arch Public Health. 2022;80(1):72.
Meadows D. Leverage points. Places to intervene in a system. The Sustainability Institute, Hartland Four Corners, Vermont, USA; 1999.
Boelsen-Robinson T, Blake MR, Brown AD, Huse O, Palermo C, George NA, et al. Mapping factors associated with a successful shift towards healthier food retail in community-based organisations: a systems approach. Food Policy. 2021;101: 102032.
Carey G, Crammond B. Systems change for the social determinants of health. BMC Public Health. 2015;15:662.
Allender S, Owen B, Kuhlberg J, Lowe J, Nagorcka-Smith P, Whelan J, et al. A community based systems diagram of obesity causes. PLoS ONE. 2015;10(7):e0129683. https://doi.org/10.1371/journal.pone.0129683
Ballard E, Farrell A, Long M. Community-based system dynamics for mobilizing communities to advance school health. J Sch Health. 2020;90(12):964–75.
Gerritsen S, Renker-Darby A, Harre S, Rees D, Raroa DA, Eickstaedt M, et al. Improving low fruit and vegetable intake in children: findings from a system dynamics, community group model building study. PLoS ONE [Electronic Resource]. 2019;14(8): e0221107.
Cavana RY, Tobias M. Integrative system dynamics: analysis of policy options for tobacco control in New Zealand. Syst Res Behav Sci. 2008;25(5):675–94.
Atkinson J-A, Page A, Heffernan M, McDonnell G, Prodan A, Campos B, et al. The impact of strengthening mental health services to prevent suicidal behaviour. Aust N Z J Psychiatry. 2019;53(7):642–50.
Ison R. Systems practice: how to act in a climate change world. Berlin: Springer Science & Business Media; 2010.
Luke DA, Stamatakis KA. Systems science methods in public health: dynamics, networks, and agents. Annu Rev Public Health. 2012;33:357–76.
Morshed AB, Kasman M, Heuberger B, Hammond RA, Hovmand PS. A systematic review of system dynamics and agent-based obesity models: evaluating obesity as part of the global syndemic. Obes Rev. 2019;20(S2):161–78.
Riley B, Willis C, Holmes B, Finegood D, Best A, McIsaac J. Systems thinking and dissemination and implementation research. Dissemination and implementation research in health. Transl Sci Pract. 2017;143.
Lobb R, Colditz GA. Implementation science and its application to population health. Annu Rev Public Health. 2013;34:235–51.
Nilsen P. Making sense of implementation theories, models, and frameworks. Implement Sci. 2020;30:53–79.
Swinburn B, Dietz W, Kleinert S. A Lancet Commission on obesity. Lancet. 2015;386(10005):1716–7.
Strifler L, Cardoso R, McGowan J, Cogo E, Nincic V, Khan PA, et al. Scoping review identifies significant number of knowledge translation theories, models, and frameworks with limited use. J Clin Epidemiol. 2018;100:92–102.
Braithwaite J, Churruca K, Long JC, Ellis LA, Herkes J. When complexity science meets implementation science: a theoretical and empirical analysis of systems change. BMC Med. 2018. https://doi.org/10.1186/s12916-018-1057-z.
Northridge ME, Metcalf SS. Enhancing implementation science by applying best principles of systems science. Health Res Policy Syst. 2016;14(1):74.
Hovmand P. Community based system dynamics. Berlin: Springer; 2014.
Gerritsen S, Harre S, Rees D, Renker-Darby A, Bartos AE, Waterlander WE, et al. Community group model building as a method for engaging participants and mobilising action in public health. Int J Environ Res Public Health [Electronic Resource]. 2020;17(10):15.
Kania A, Patel AB, Roy A, Yelland GS, Nguyen DTK, Verhoef MJ. Capturing the complexity of evaluations of health promotion interventions: a scoping review. Can J Program Eval. 2012;27(1):65–91.
Hennessy E, Economos CD, Hammond RA. Integrating complex systems methods to advance obesity prevention intervention research. Health Educ Behav. 2020;47(2):213–23.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9.
Malhi L, Karanfil O, Merth T, Acheson M, Palmer A, Finegood DT. Places to intervene to make complex food systems more healthy, green, fair, and affordable. J Hunger Environ Nutr. 2009;4(3–4):466–76.
Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018;34(4):285–91.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):1–11.
Allender S, Brown AD, Bolton KA, Fraser P, Lowe J, Hovmand P. Translating systems thinking into practice for community action on childhood obesity. Obes Rev. 2019;20(Suppl 2):179–84.
Amed S, Shea S, Pinkney S, Higgins JW, Naylor PJ. Wayfinding the live 5-2-1-0 initiative—at the intersection between systems thinking and community-based childhood obesity prevention. Int J Environ Res Public Health. 2016;13(6):1–16.
Kennedy L, Pinkney S, Suleman S, Mâsse LC, Naylor P-J, Amed S. Propagating change: using RE-FRAME to scale and sustain a community-based childhood obesity prevention initiative. Int J Environ Res Public Health. 2019;16(5):736.
Purnell JQ, Lobb Dougherty N, Kryzer EK, Bajracharya S, Chaitan VL, Combs T, et al. Research to translation: the healthy schools toolkit and new approaches to the whole school, whole community, whole child model. J Sch Health. 2020;90(12):948–63.
Bensberg M. Developing a systems mindset in community-based prevention. Health Promot Pract. 2021;22(1):82–90.
Bensberg M, Allender S, Sacks G. Building a systems thinking prevention workforce. Health Promot J Austr. 2020;31(3):436–46.
Brimblecombe J, Van Den Boogaard C, Wood B, Liberato SC, Brown J, Barnes A, et al. Development of the good food planning tool: a food system approach to food security in Indigenous Australian remote communities. Health Place. 2015;34:54–62.
Buccini G, Harding KL, Hromi-Fiedler A, Perez-Escamilla R. How does “Becoming Breastfeeding Friendly” work? A programme impact pathways analysis. Matern Child Nutr. 2019;15(3): e12766.
Gadsby EW, Hotham S, Eida T, Lawrence C, Merritt R. Impact of a community-based pilot intervention to tackle childhood obesity: a “whole-system approach” case study. BMC Public Health. 2020. https://doi.org/10.1186/s12889-020-09694-2.
Kremser W. Phases of school health promotion implementation through the lens of complexity theory: lessons learnt from an Austrian case study. Health Promot Int. 2011;26(2):136–47.
Matheson A, Walton M, Gray R, Wehipeihana N, Wistow J. Strengthening prevention in communities through systems change: lessons from the evaluation of Healthy Families NZ. Health Promot Int. 2020;35(5):947–57.
Ramanadhan S, Minsky S, Martinez-Dominguez V, Viswanath K. Building practitioner networks to support dissemination and implementation of evidence-based programs in community settings. Transl Behav Med. 2017;7(3):532–41.
Rosas S, Knight E. Evaluating a complex health promotion intervention: case application of three systems methods. Crit Public Health. 2019;29(3):337–52.
Rothwell H, Shepherd M, Murphy S, Burgess S, Townsend N, Pimm C. Implementing a social-ecological model of health in Wales. Health Educ. 2010;110(6):471–89.
Sautkina E, Goodwin D, Jones A, Ogilvie D, Petticrew M, White M, et al. Lost in translation? Theory, policy and practice in systems-based environmental approaches to obesity prevention in the Healthy Towns programme in England. Health Place. 2014;29:60–6.
Serpas S, Brandstein K, McKennett M, Hillidge S, Zive M, Nader PR. San Diego Healthy Weight Collaborative: a systems approach to address childhood obesity. J Health Care Poor Underserved. 2013;24(2):80–96.
Rosas SR. Systems thinking and complexity: considerations for health promoting schools. Health Promot Int. 2017;32(2):301–11.
Langford R, Bonell C, Jones H, Pouliou T, Murphy S, Waters E, et al. The World Health Organization’s Health Promoting Schools framework: a Cochrane systematic review and meta-analysis. BMC Public Health. 2015;15(1):130.
Organization WH. Monitoring the building blocks of health systems: a handbook of indicators and their measurement strategies. World Health Organization; 2010.
Mabry PL, Olster DH, Morgan GD, Abrams DB. Interdisciplinarity and systems science to improve population health: a view from the NIH Office of Behavioral and Social Sciences Research. Am J Prev Med. 2008;35(2):S211–24.
Strugnell C, Millar L, Churchill A, Jacka F, Bell C, Malakellis M, et al. Healthy together Victoria and childhood obesity—a methodology for measuring changes in childhood obesity in response to a community-based, whole of system cluster randomized control trial. Arch Public Health. 2016;74(1):1–16.
Leischow SJ, Milstein B. Systems thinking and modeling for public health practice. American Public Health Association; 2006. p. 403–5.
Butland B, Jebb S, Kopelman P, McPherson K, Thomas S, Mardell J, et al. Tackling obesities: future choices-project report: Citeseer; 2007.
Li B, Allender S, Swinburn B, Alharbi M, Foster C. Improving the reporting of intervention studies underpinned by a systems approach to address obesity or other public health challenges. Front Public Health. 2022;10.
Wensing M, Grol R. Knowledge translation in health: how implementation science could contribute more. BMC Med. 2019;17(1):88.
Bandura A. Social-cognitive theory. An introduction to theories of personality. 2014:341–60.
Bandura A, Walters RH. Social learning theory. Englewood Cliffs: Prentice Hall; 1977.
Sutton S, French D, Hennings S. Transtheoretical model of behaviour change. Curr Psychol. 1997;22:234–51.
Gielen AC, McDonald EM, Gary TL, Bone LR. Using the precede-proceed model to apply health behavior theories. Health Behav Health Educ Theory, Res Pract. 2008;4:407–29.
Taylor MJ, McNicholas C, Nicolay C, Darzi A, Bell D, Reed JE. Systematic review of the application of the plan–do–study–act method to improve quality in healthcare. BMJ Qual Saf. 2014;23(4):290–8.
Foster-Fishman PG, Nowell B, Yang H. Putting the system back into systems change: a framework for understanding and changing organizational and community systems. Am J Community Psychol. 2007;39(3):197–215.
Bagnall A-M, Radley D, Jones R, Gately P, Nobles J, Van Dijk M, et al. Whole systems approaches to obesity and other complex public health challenges: a systematic review. BMC Public Health. 2019;19(1):8.
Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, et al. RE-AIM planning and evaluation framework: adapting to new science and practice with a 20-year review. Front Public Health. 2019;7:64.
Fixsen DL, Blase KA. Active implementation frameworks. Handbook on implementation science. Cheltenham: Edward Elgar Publishing; 2020. p. 62–87.
Brown CA, Lilford RJ. The stepped wedge trial design: a systematic review. BMC Med Res Methodol. 2006;6(1):54.
Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217–26.
Acknowledgements
No acknowledgements.
Funding
The authors acknowledge Dean’s postdoctoral research fellowship funding received by Jillian Whelan; and Australian Government National Health and Medical Research Council funding awards: 1152968 and 1151572 that supported this work.
Author information
Authors and Affiliations
Contributions
JW and CB determined the research questions and search strategy. JW led the study and undertook the search, screening, article selection, data extraction, quality assessment, and data synthesis. PF, KAB, PL, CS, TBR, MB, EM, CB undertook the screening, article selection, data extraction, and quality assessment. JW drafted the manuscript in collaboration with all authors. All authors critically revised the manuscript, provided detail editing, and approved the manuscript submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors provide consent for publication.
Competing interests
All authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Search terms.
Additional file 2:
Details of included studies.
Additional file 3:
Quality appraisal of included studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Whelan, J., Fraser, P., Bolton, K.A. et al. Combining systems thinking approaches and implementation science constructs within community-based prevention: a systematic review. Health Res Policy Sys 21, 85 (2023). https://doi.org/10.1186/s12961-023-01023-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12961-023-01023-4